note to users - mcgill universitydigitool.library.mcgill.ca/thesisfile80114.pdf · les paramètres...
TRANSCRIPT

NOTE TO USERS
This reproduction is the best copy available.
®
UMI

Microencapsulated Genetically Engineered
Lactobacillus plantarum 80 (pCBHl) for Bile Acid
Deconjugation and its Implication in Lowering
Cholesterol
Mitchell Lawrence J anes
Department of Biomedical Engineering
McGill University, Montreal,
Quebec, Canada
A thesis submitted to McGill University in partial fulfilment of the
requirements of the degree of
Master's of Engineering (Biomedical Engineering).
Octaber, 2003
~M Gil·l \~~i c . © Mitchell Lawrence Jones, 2003
1+1 Library and Archives Canada
Bibliothèque et Archives Canada
Published Heritage Branch
Direction du Patrimoine de l'édition
395 Wellington Street Ottawa ON K1A ON4 Canada
395, rue Wellington Ottawa ON K1A ON4 Canada
NOTICE: The author has granted a nonexclusive license allowing Library and Archives Canada to reproduce, publish, archive, preserve, conserve, communicate to the public by telecommunication or on the Internet, loan, distribute and sell th es es worldwide, for commercial or noncommercial purposes, in microform, paper, electronic and/or any other formats.
The author retains copyright ownership and moral rights in this thesis. Neither the thesis nor substantial extracts from it may be printed or otherwise reproduced without the author's permission.
ln compliance with the Canadian Privacy Act some supporting forms may have been removed from this thesis.
While these forms may be included in the document page count, their removal does not represent any loss of content from the thesis.
• •• Canada
AVIS:
Your file Votre référence ISBN: 0-612-98537-7 Our file Notre référence ISBN: 0-612-98537-7
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque et Archives Canada de reproduire, publier, archiver, sauvegarder, conserver, transmettre au public par télécommunication ou par l'Internet, prêter, distribuer et vendre des thèses partout dans le monde, à des fins commerciales ou autres, sur support microforme, papier, électronique et/ou autres formats.
L'auteur conserve la propriété du droit d'auteur et des droits moraux qui protège cette thèse. Ni la thèse ni des extraits substantiels de celle-ci ne doivent être imprimés ou autrement reproduits sans son autorisation.
Conformément à la loi canadienne sur la protection de la vie privée, quelques formulaires secondaires ont été enlevés de cette thèse.
Bien que ces formulaires aient inclus dans la pagination, il n'y aura aucun contenu manquant.

ABSTRACT
A novel approach whereby one can use genetically engineered cells for the
purpose of deconjugating bile acids and lowering cholesterol is presented in this thesis.
The concept of oral administration of artificial cells has been used for this purpose. In
concurrence to these requirements, several in-vitro methods are designed and discussed in
this report. For these studies, alginate-polylysine-alginate microcapsules were used.
Process parameters for Lactobaci/lus plantarum 80 (PCBHl) cell microencapsulation
have been presented. Results show the possibility ofusing these artificial cells for various
applications. For in-vitro experiments, immobilized bacteria and artificial cells containing
the genetically engineered organism were challenged with physiologically relevant levels
of bile acids. Results show that immobilized and microencapsulated genetically
engineered bacterial cells are capable of lowering physiological levels of bile acids in
vitro. Further, tbis report summarizes the physiological interrelationship between bile
acids and cholesterol and predicts oral doses of microencapsulated cells required for
lowering cholesterol.
1
RÉSUMÉ
Une nouvelle approche basée sur l'utilisation des cellules génétiquement modifiées pour
dissocier les acides biliaires et diminuer le cholestérol est présentée dans cette thèse. Le
concept de l'administration orale des cellules artificielles a été utilisé à cette fin. Pour
réaliser l'étude, plusieurs méthodes in-vitro furent développées et sont discutées dans ce
rapport. Pour ce projet, des microcapsules d'alginate-polylysine-alginate furent utilisées.
Les paramètres du procédé pour l' encapsulation des cellules Lactobacillus plantarum 80
(pCBHl) sont présentés. Les résultats démontrent l'utilisation potentielle des cellules
artificielles pour diverses applications. Lors des expériences in-vitro, les bactéries
génétiquement modifiées immobilisées et celles encapsulées furent soumises à
d'importants taux physiologiques des acides biliaires. Les résultats démontrent que, sous
forme immobilisée et encapsulée, elles peuvent diminuer ces taux. Aussi, ce rapport
résume la relation physiologique existant entre les acides biliaires et le cholestérol, puis
présente les prédictions ~es doses orales de cellules microencapsulées requises pour
diminuer le cholestérol.
II

ACKNOWLEDGMENTS AND CONTRIBUTION OF AUTHORS
l would like to acknowledge intermittent laboratory assistance and advice given
by Terrence Metz (Graduate Student, M.Eng.), Hongmei Chen (Graduate Student, Ph.D.),
Wei Ouyang (Graduate Student, Ph.D.), and Christopher Martoni (Graduate Student,
M.Eng.). As weIl, l would like to recognize the advice and direction given by my
supervisor, Dr. Satya Prakash.
For the co-authored original paper Method for Bile Acid Determination by High
Pressure Liquid Chromatography, co-authored by Hongmei Chen, Wei Ouyang, Terrence
Metz, and Dr. Satya Prakash and in press in the Medical Journal of Science, l would like
to acknowledge intermittent laboratory assistance and advice given by my co-authors.
For the co-authored original paper Deconjugation of Bile Acids with Immobilized
Genetically Engineered Lactobacillus plantarum 80 (PCBH1), co-authored by Hongmei
Chen, Wei Ouyang, Terrence Metz, and Dr. Satya Prakash and submitted to the Cell
Transplantation Journal, l would like to acknowledge intermittent laboratory assistance
and advice given by my co-authors.
For the co-authored original paper Microencapsulated Genetically Engineered
Lactobacillus plantarum 80 (PCBH1) for Bile A cid Deconjugation and Implication in
Lowering Cholesterol, co-authored by Hongmei Chen, Wei Ouyang, Terrence Metz, and
Dr. Satya Prakash and submitted to the Journal of Biomedicine and Biotechnology, l
would like to acknowledge intermittent laboratory assistance and advice given by my co
authors.
l gratefully acknowledge financial support from the Natural Sciences and
Engineering Research Council (NSERC) of Canada in the form of a PGSA scholarship.
III

PREFACE
In accordance with the thesis preparation and submission guidelines, I have taken the
option of writing the experimental portion of this thesis in the form of original papers
suitable for publication. This option is provided by Section J-C in the Thesis
Preparation and Submission Guidelines, which reads as follows:
As an alternative to the traditional thesis format, the dissertation can consist of a collection of papers of which the student is an author or co-author. These papers must have a cohesive, unitary character making them a report of a single pro gram of research.
In this thesis, manuscripts of original papers are presented in Chapters 3-5. Each
experiment based paper has its own Abstract, Introduction, Materials and Methods,
Results, Discussion, and References. A common Abstract, Introduction, a final overall
Conclusion, Summary, Clams to Original Contributions to Knowledge, and
Recommendations are also included.
IV

TABLE OF CONTENTS
ABSTRACT
RESUME
ACKNOWLEDGMENTS AND CONTRIBUTION OF AUTHORS
PREFACE
TABLE OF CONTENTS
TABLE OF FIGURES AND TABLES
CHAPTER 1: GENERAL INTRODUCTION
1.1 Cholesterol metabolism and risk for CHD
1.2 Artificial cell microencapsulation
1.3 Presently available treatment modalities for lowering cholesterol and associated
limitations
1.4 Use oflive bacteria to reduce serum cholesterol
1.5 Research objectives
CHAPTER 2: LITERATURE REvlEW
2.1 Cholesterol metabolism and risk for CHD
2.2 Presently available treatment modalities for lowering cholesterol and associated
limitations
2.3 Potential use of therapy based on artificial cell microencapsulation
2.3.1 Artificial cells
2.3.2 Methods for preparing artificial cells
2.3.3 The c1assic method (APA microcapsules)
2.4 Use of live orally delivered bacterial cells for lowering cholesterol
2.5 Potential of artificial cells for oral delivery of live bacterial cells for therapy
2.5.1 Principle of orally delivered artificial cells for oral therapy
2.5.2 Microencapsulation: A solution to the limitations of free live bacterial cell therapy
2.5.3 Membranes used for artificial cells for oral delivery ofbacterial cells
PREFACE FOR CHAPTERS 3 TO 5
CHAPTER 3: ORIGINAL PAPER: METHOD FOR BILE ACID DETERMINATION BY
HIGH PRESSURE LIQUID CHROMATOGRAPHY
3.1 Introduction
3.2 Background
3.2 Materials and methods
v
1
II
III
IV
V
VII
1
2
3
3
4
5
7
8
9
10
10 12
13
14
18
18
19
22
27
30
31
31
32
3.3 Results and Discussion
3.4 Acknowledgments
CHAPTER 4: ORIGINAL PAPER: DECONJUGA TION OF BILE ACIDS WlTH
IMMOBILIZEDGENETICALLY ENGINEERED LA CTOBA CILL US
PLANTARUM 80 (pCBHl)
4.1 Abstract
4.2 Introduction
4.3 Materials and methods
4.4 Results
4.5 Discussion
4.6 Acknowledgments
CHAPTER 5: ORIGINAL PAPER: MICROENCAPSULATED GENETICALLY
ENGINEERED LA CTOBACILLUS PLANT ARUM 80 (pCBHl) FOR BILE ACID
32
35
36
37
37
39
41
43
45
DECONJUGATION AND IMPLICATION IN LOWERJNG CHOLESTEROL 52
5.1 Abstract 53
5.2 Introduction 53
5.3 Materials and methods 55
5.4 Results 57
5.5 Discussion 59
5.6 Acknow1edgments 61
CHAPTER 6: CONCLUSIONS, SUMMARY AND CLAIM TO THE CONTRIBUTION OF
KNOWLEDGE 69
6.1 Summary of observations and recommendations 70
6.2 Conclusions 72
REFERENCES 74
VI

Figure 2.1:
Figure 2.2:
Table 2.1:
Figure 2.3:
Table 2.2:
Figure 2.4:
Table 2.3:
Figure 3.1:
Figure 3.2:
Table 4.1:
Figure 4.1:
Figure 4.2:
Figure 4.3:
Figure 4.4:
Figure 4.5:
Figure 4.6:
LIST OF FIGURES AND TABLES
Molecular cut-off of different types of microcapsule membranes. 13
Artificial cells for bacterial cell therapy. 14
Potential therapies based on the oral delivery of free live bacteria cells. 17
The principle of orally administered artificial cells containing bacterial cells for therapy. 19
Potential therapies based on the oral delivery of microencapsulated bacterial cells. 21
Electrostatic interactions ofpolymer layers in Alginate-Poly-L-Lysine-Alginate (AP A) Membrane. 24
Established/promising polymers for live cell encapsulation. 26
Chromatogram of standards of each of GCA, TDCA, and GDCA in methanol. Inlayed are the calibration curves. 34
Chromatogram of samples of each of TDCA and GDCA with GCA internaI standard. Inlayed are the calibration curves. 34
Bile salt hydrolase (BSH) activity (/lmol DCA/mg CDW-h) of immobilized Lactobacillus plantarum 80 (PCBH1) towards glyco- and tauro- bile acids. 46
Photomicrograph of alginate beads containing immobilized Lactobacillus plantarum 80 (pCBH1) cells at 175 x magnifications. 47
HPLC calibration curves for GDCA and TDCA measurements. 47
Overlaid HPLC chromatograms ofbile acids in reaction media over time. Decreasing peak areas of TDCA and GDCA indicate BSH activity of immobilized Lactobacillus plantarum 80 (PCBH1). 48
BSH activity and GDCA and TDCA depletion efficiency of immobilized Lactobacillus plantarum 80 (PCBHl) in in-vitro experiment. 49
(A) Overlaid HPCL chromatograms from an experiment in which immobilized LP80 (pCBHl) was used to deconjugate 10 mM GDCA and 5 mM TCDA in MRS reaction media. (B) Overlaid HPLC chromatograms from a calibration with increasing concentrations of TDCA GDCA and DCA.
Hydrolysis of conjugated bile salts by the Bile Salt Hydrolase (BSH) enzyme overproduced by genetically engineered Lactobacillus
VII
50
51

Table 5.1:
Figure 5.1:
Figure 5.2:
Figure 5.3:
Figure 5.4:
Figure 5.5:
plantarum 80 (PCBHl).
Bile salt hydrolase (BSH) activity Ütmol DCA/mg CDW-h) of microencapsulated Lactobacil!us plantarum 80 (pCBH 1) towards glyco- and tauro- bile acids.
(A) Photomicrograph of Lactobacillus plantarum 80 (PCBH1) microcapsules at 77 x magnification and (B) at 112 x magnification.
(A) Overlaid HPLC chromatograms ofbile acids over time. (B) BSH activity and GDCA and TDCA depleting efficiency of Lactobacil!us plantarum 80 (PCBH1) microcapsules in in-vitro experiment.
(A) Overlaid HPLC chromatograms from experiment in which microencapsulated LP80 (PCBH1) was used to deconjugate 10 mM GDCA and 5 mM TCDA. (B) Overlaid HPCL chromatograms from experiment in which immobilized LP80 (PCBH1) was used to deconjugate 10 mM GDCA and 5 mM TCDA.
(A) Hydrolysis of conjugated bile salts by the Bile Salt Hydrolase (BSH) enzyme overproduced by genetically engineered Lactobacillus plantarum 80 (PCBH1). (B) Enterohepatic circulation of bile (EHC).
Predicted removal of cholesterol from blood serum in humans.
62
63
64
65
66
67
Supplement 5.1: HPLC calibration curves for GDCA and TDCA measurements. 68
VIII

CHAPTER 1
GENERAL INTRODUCTION
1

1.1 Cholesterol metabolism and risk for CHD
Although, cholesterol is an important basic building block for body tissues,
elevated blood cholesterol is a well known major risk factor for CHD1,2. Cholesterol,
along with triglycerides, circulates in the bloodstream as part oflipoprotein complexes.
These complexes can be separated by density ultracentrifugation into high (HDL),
intermediate (lDL), low (LDL), and very low (VLDL) density lipoprotein fractions. The
involvement oflow-density lipoprotein cholesterol (LDL-C) in CHD has been weIl
documented. Epidemiological studies have established that increased levels ofLDL-C,
plasma triglycerides (TG), and decreased levels ofhigh-density lipoprotein cholesterol
(HDL-C) are major risk factors for CHD. Cholesterol-enriched TG-rich lipoproteins,
including very-Iow-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL),
and remnants, can also promote atherosclerosis. Elevated plasma TGs are frequently
found in a triad with low HDL-C and small LDL partic1es, as weIl as in association with
non-lipid metabolic risk factors for CHD3.
Elevated blood cholesterolleads to plaque build up in the arteries, impeding blood
flow to the brain, kidneys, genitals, and heart causing CHD and other diseases. An
estimated 102 million American adults have total blood cholesterollevels of 200 mg/dL
and higher. Ofthese, about 41 million have levels of240 mg/dL or above. For adults,
total cholesterollevels of 240 mg/dL or higher are considered high risk, and levels from
200 to 239 mg/dL are considered borderline high risk4,4. According to the
recommendations of the National Cholesterol Education Program's (NCEP) the primary
objective of any therapy is the lowering ofLDL-C levels. New guidelines now consider
other risk factors such as age, family history, smoking, hypertension, low HDL, and
diabetes mellitus, in estimating cut-offlevels of cholesterol requiring intervention. Under
these guidelines patients with LDL levels above 160 mg/dL may also be considered
eligible for pharmacological therapy ifthey have additional risk factors5,6. Currently,
according to the recently revamped recommendations ofthe National Cholesterol
Education Program (NCEP) about 36 million US citizens be should treated for high
cholesteroI3,5,7.
2

1.2 Artificial cell microencapsulation
Artificial cell microencapsulation8 is a technique used to encapsulate biologically
active materials in a specialized ultra thin semi-permeable pol ymer membranes9•
Microcapsules proteet encapsulated materials from harsh extemal environments, at the
same time allowing for metabolism of selected solutes capable of passing into and out of
the microcapsules. In this manner, the enclosed material (in this case live bacteria) can be
retained and separated from the extemal environment. Mierocapsules are known to
protect live ceIls, enzymes, and DNA from immune rejection and other extreme
environments and have a number ofbiomedical and clinieal applications10-14.
It has recently been shown that artifieial cell microcapsules can be used for oral
administration oflive genetically engineered cells for therapyI5,16. Although the live cells
remain immobilized inside the microeapsules, microencapsulation has been shown not to
hinder their growth kinetics17• The microcapsules remain intact during passage through
the intestinal tract and are excreted intact with the stool in about 24 hours. The cells are
retained within the microcapsule, addressing many of the major safety eoncems
associated with the use oflive bacterial cells for clinical applications. However, as the
membranes of the mieroeapsules are permeable to smaller molecules, the cells inside the
microcapsules metabolize small molecules found within the gut during passage through
the intestine. It has been demonstrated that this can result in significant decreased
systemic metabolite levels of certain moleeules, including creatinine and uric acid, in rats.
Thus, oral delivery oflive microencapsulated cells could have applications in the
treatment of renal failure, liver disease, metabolic disorders and in the treatment of many
other diseasesI5,18-20.
1.3 Presently available treatment modalities for lowering cholesterol and associated
limitations
Methods for lowering blood cholesterollevels in man involve dietary
management, behaviour modification, exereise and drug therapy. Dietary intervention,
whereby lipid intake is restricted is generally the first line oftreatment21 -23• Studies show
that complete elimination of dietary cholesterol and limiting fat content to less than ten
3
percent of the daily caloric intake can effect a mere four percent regression of
atherosclerotic plaques after five years when combined with stress management and
aerobic exercise24• However, the combined restricted vegetarian diet (free ofmeat, fish,
chicken, vegetable oils and aIl dairy fat products) and aerobic approach, is unrealistic for
aIl but the most dedicated individuals.
A variety of dietary supplements or specific foods e.g. brans, psylliums, guar gum,
lecithins, whey, red win es, fish oils and ginseng root extract have been reported to reduce
high blood cholesterol or its consequences. The mechanisms are varied and include
cholesterol sequestering, chelating, entrapment and oxidation inhibition. Such regimens
generally lower the blood cholesterolleve1 by ten percent or less. In addition, none of
these dietary interventions have been shown to arrest or cure atherosclerosis or other high
blood cholesterol associated diseases.
Pharmacologic agents such as fibric acid derivatives (fibrates), nicotinic acid, bile
acid sequestrants (BAS), estrogen replacement therapy, and hydroxymethyl glutaryl
coenzyme A (HMG-CoA) reductase inhibitors (statins) are also available for the
treatment ofhigh cholesterol. From among the agents listed above, the statins are
considered to have the most potential for treatment. Currently, lovastatin (Mevacor),
pravastatin (Pravachol), zocor (Zocor), fluvastatin (Lescol) and atorvastatin (Lipitor) are
been used for clinicallowering of cholesterol. Although effective at reducing cholesterol
leve1s, they are nevertheless extreme1y expensive25-28
, aIl are known to have severe side
effects and are associated with extensive morbidity and/or mortality.
1.4 Use of live bacteria to reduce serum cholesterol
A less weIl known approach to reducing blood cholesterol, oral live bacterial cell
therapy, is based on the demonstration that bacteria such as Lactobacillus acidophilus,
Bifidobacteria bifidum, and Lactobaci/lus bulgaricus, which are part of the normal
intestinal flora, can lower cholesterollevels significantlY9-31. Indeed a number of studies
have confirmed this capacity, and it has been found that oral daily intake of live
lactobacillus cells in particular (found in yogurt) can lead to significant reduction in
cholesterollevels30,31. It has been reported that using these and related methods,
cholesterollevels can be reduced by 22% to 33%32. Although the mechanisms by which
4

these bacteria lower cholesterol is not entirely understood, it has been proposed that this
could be the result of enhanced Bile Salt Hydrolase (BSH) activitr9 or suppressed re
absorption of cholesterol carrying bile acids33.
Unfortunately, the therapeutic potential oflive bacterial cells has been hampered
by inherent limitations in their use. For example, a nonnal daily intake of250 ml of
yogurt would only correspond to 500 milligram of cell dry weight (CDW) ofbacteria, and
of those bacteria ingested only 1 % would survive gastric transit limiting the overall
therapeutic effect29. There are also sorne practical concems regarding the production,
cost, and storage of such a product29. Further, oral administration oflive bacterial cells
can pose problems. For example, when given orally, large amounts oflive bacterial cells
can stimulate host immune response34,35, they can be retained in the intestine, and
repeated large doses could result in their replacing the nonnal intestinal flora36,37. In
addition, risk of systemic infections, deleterious metabolic activities, adjuvant side
effects, immuno-modulation and risk of gene transfer has limited their use35,38. Concems
of safety has thus, prevented regular use of this promising therapy in c1inical practice.
1.5 Research Objectives
In the present project a treatment modality based on the use of artificial cell
microcapsules (ACM) is proposed. This method will take advantage ofthe inherent
cholesterol-Iowering properties oflive non-pathogenic genetically engineered bacteria
and at the same time circumvent to a large extent associated problems related with their
use. The research objectives are:
1. Design and test an assay for bile acid identification and quantification from
aqueous solutions using high pressure liquid chromatography (HPLC).
2. Design immobilized alginate beads containing live Lactobacil/us plantarum 80
(PCBH1) cells and study their ability to hydrolyze bile salts in-vitro in flask.
3. Design artificial cell microcapsule fonnulations containing live Lactobacil/us
plantarum 80 (pCBHl) cells and study their ability to hydrolyze bile salts in-vitro
in flask.
5

4. Evaluate the potential for microencapsulated LP80 (pCBHl) to lower serum
cholesterollevels through interruption ofthe EHC ofbile salts.
6
CHAPTER2
LITERATURE REVIEW
7

2.1 Cholesterol metabolism and risk for CHD
Although, cholesterol is an important basic building block for body tissues,
elevated blood cholesterol is a weIl known major risk factor for CHD1 • Cholesterol, along
with triglycerides, circulates in the bloodstream as part oflipoprotein complexes. These
complexes can be separated by density ultracentrifugation into high (HDL), intermediate
(IDL), low (LDL), and very low (VLDL) density lipoprotein fractions. The involvement
oflow-density lipoprotein cholesterol (LDL-C) in CHD has been weIl documented.
Epidemiological studies have established that increased levels ofLDL-C, plasma
triglycerides (TG), and decreased levels ofhigh-density lipoprotein cholesterol (HDL-C)
are major risk factors for CHD. Cholesterol-enriched TG-rich lipoproteins, including
very-low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), and
remnants, can also promote atherosclerosis. Elevated plasma TGs are frequently found in
a triad with low HDL-C and small LDL particles, as weIl as in association with non-lipid
metabolic risk factors for CHD2,39.
Elevated blood cholesterolleads to plaque build up in the arteries, impeding blood
flow to the brain, kidneys, genitals, and heart causing CHD and other related diseases. An
estimated 102 million American adults have total blood cholesterollevels of200 mg/dL
and higher. Ofthese, about 41 million have levels of240 mg/dL or above. For adults,
total cholesterollevels of 240 mg/dL or higher are considered high risk, and levels from
200 to 239 mg/dL are considered borderline high risk40• According to the
recommendations of the National Cholesterol Education Program's (NCEP) the primary
objective of any therapy is the lowering of LDL-C levels. New guidelines now consider
other risk factors such as age, family history, smoking, hypertension, low HDL, and
diabetes mellitus, in estimating cut-offlevels of cholesterol requiring intervention. Under
these guidelines patients with LDL levels above 160 mg/dL may also be considered
eligible for pharmacological therapy if they have additional risk factors5. Currently,
according to the recently revamped recommendations of the National Cholesterol
Education Program (NCEP), about 36 million US citizens be should treated for high
cholesterols.
8

2.2 Presently available treatment modalities for lowering cholesterol and associated
limitations
Methods for lowering blood cholesterollevels in man involve dietary
management, behaviour modification, exercise and drug therapy41,42. Dietary intervention,
whereby lipid intake is restricted is generaIly the first line of treatrnent. Studies show that
complete elimination of dietary cholesterol and limiting fat content to less than ten
percent of the daily caloric intake can effect a mere four percent regression of
atherosclerotic plaques after five years when combined with stress management and
aerobic exercise. However, the combined restricted vegetarian diet (free ofmeat, fish,
chicken, vegetable oils and aIl dairy fat products) and aerobic approach, is unrealistic for
aIl but the most dedicated individuals.
A variety of dietary supplements or specific foods e.g. brans, psylliums, guar gurn,
lecithins, whey, red wines, fish oils and ginseng root extract have been reported to reduce
high blood cholesterol or its consequences. The mechanisms are varied and include
cholesterol sequestering, chelating, entrapment and oxidation inhibition. Such regimens
generaIly lower the blood cholesterollevel by ten percent or less. In addition, none of
these dietary interventions have been shown to arrest or cure atherosclerosis or other high
blood cholesterol associated diseases.
Pharmacologic agents such as fibric acid derivatives (fibrates), nicotinic acid, bile
acid sequestrants (BAS), estrogens replacement therapy, and hydroxymethyl glutaryl
coenzyme A (HMG-CoA) reductase inhibitors (statins) are also available for the
treatment ofhigh cholesterol. From arnong the agents listed above, the statins are
considered to have the most potential for treatrnent. Currently, lovastatin (Mevacor),
pravastatin (Pravachol), zocor (Zocor), fluvastatin (Lescol) and atorvastatin (Lipitor) are
been used for clinicallowering of cholesterol. Although effective at reducing cholesterol
levels, they are aIl expensive and known to have severe side effects including association
to extensive morbidity and or mortalitl3-46.
Another approach to reducing blood cholesterol is through the interruption of the
enterohepatic circulation (EHC) ofbile salts. Bile salts are the water-soluble end products
9

of cholesterol, and are synthesized in the liver. During nonnal (EHC), the average bile
salt pool of 4.0 gis secreted into the duodenum twice during each meal, or an average of
6-8 times per day47,48, for the purpose offonning mixed micelles with the products of
lipid digestion. During intestinal transit, 90-95% of secreted bile salts are absorbed in the
tenninal ileum and is retumed to the liver via the portal vein48 . The bile salt pool is
approximately constant and is replenished by hepatic synthesis of new bile from serum
cholesterol. It has been shown that upon surgical, pharmacological or pathological
interruption of the EHC bile salt synthesis is increased, up to 15-fold48, leading to an
increased demand for cholesterol in the liver. Thus, if during intestinal transit bile salts
are removed or rendered incapable of reabsorption, they may not re-enter the EHC and
are lost in the faeces. To replace the bile which is lost from the EHC, bile acids are then
made in the liver de-nova with cholesterol taken from the blood stream. In this way, the
EHC bile salt pool is replenished and kept 'topped up' by bile salts derived from blood
serum cholesterot29,49.
To take advantage of this method for lowering cholesterol, bile acid sequestrants
(BAS) have been developed that interrupt the EHC and cause lowering ofblood serum
cholesterol through de nova synthesis ofbile acids in the liver, from blood serum
cholesterol. BAS bind with bile acids in the intestine and fonn insoluble complexes that
are excreted in the feces. It has been weIl demonstrated over the last 20 years that BAS
alone can reduce cholesterol concentrations by 10% to 30%7,50. However, the common
BAS Cholestyramine resin (Locholest, Questran), Colesevelam (WeIChol), and
Colestipol (Colestid) are weIl documented to exhibit major adverse effects such as
nausea, bloating, constipation, and flatulence51 . Furthennore, there have been problems
with gaining over-the-counter (OTC) status for BAS, as they interrupt the EHC using
adsorbents and binders which are found to be unacceptable for this classification by the
U.S. Food and Drug Administration (FDA). In fact, in 1995 Bristol-Myers Squibb's
application to change Questran, the company's BAS cholesterol-Iowering medication, to
OTC status was denied by the FDA51 .
2.3 Potential use of therapy based on artificial cell microencapsulation
2.3.1 Artificial cells
10

The design of artificial cells began in 1957 as T.M.S Chang, then an
undergraduate student at McGill University, conceived of and fashioned artificial cells of
approximately a millimetre in diameter8• Chang's first artificial cell made use of
microencapsulation to trap the contents ofbiological cells, namely proteins and enzymes,
that were previously extracted from existing cells in ultra thin polymer membranes. Since
the innovation of artificial ceIls, the possibilities for both their contents and membrane
design have expanded greatly. Currently there are many substances that can be
encapsulated into artificial cells, sorne ofwhich include: oxygen, drugs, enzymes,
antibodies, cell extracts, polymers, proteins, and even whole cells themselves. The
therapeutic applications of artificial cells have also expanded to include applications in
live cell therapyl5.
Artificial cell microencapsulation is a technique used to encapsulate biologically
active materials in specialized ultra-thin semi-permeable pol ymer membranes8,52. They
are, therefore, valuable as they can protect the encapsulated materials from the external
environment while at the same time permitting selected materials to pass into and out of
the microcapsules. In this manner, the enclosed material can be retained and separated
from the undesirable external environment. Microcapsules are known to protect live cells,
enzymes, DNA etc. from immune rejection and other extreme environments and have a
number ofbiomedical and clinical applications9,53,54. We have recently shown that
artificial cell microcapsules can be used for oral administration oflive genetically
engineered bacterial cells that can be effective for therapy 15. This was based on the
following hypothesis: when given orally, the live cells remain immobilized inside the
microcapsules. The microcapsules remain intact as they pass down through the GI tract
and are excreted intact with the stool in about 24 hours. The membranes of the
microcapsules are permeable to smaller molecules; thus, during passage through the
intestine, small mo1ecu1es diffuse into and out of them, enab1ing the cells inside to
metabolize them resulting in a decreased systemic metabolite level. During passage
through the intestinal tract, the cells are retained inside the intact microcapsules and
therefore do not enter into the circulation. This latter property limits the major safety
concerns associated with the use oflive bacterial cells for various clinical
applicationsI5,55.
11
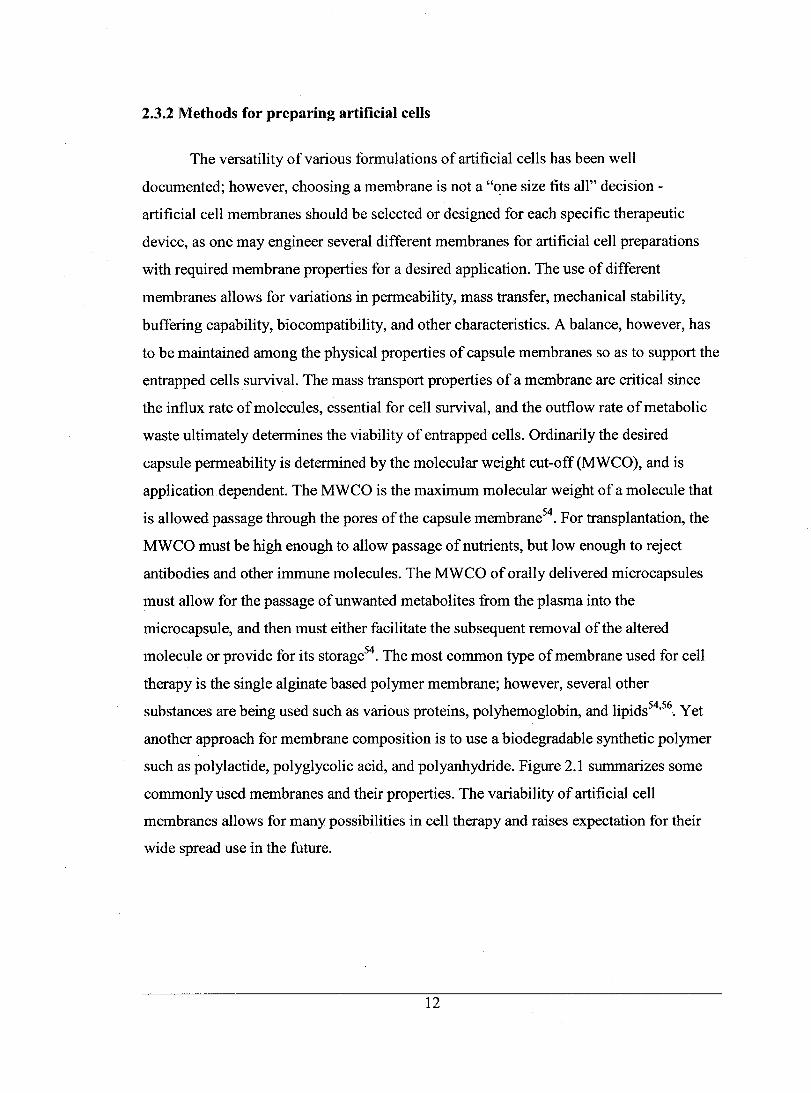
2.3.2 Methods for preparing artificial cells
The versatility of various formulations of artificial cells has been well
documented; however, choosing a membrane is not a "~ne size fits all" decision -
artificial cell membranes should be selected or designed for each specifie therapeutic
device, as one may engineer several different membranes for artificial cell preparations
with required membrane properties for a desired application. The use of different
membranes allows for variations in permeability, mass transfer, mechanical stability,
buffering capability, biocompatibility, and other characteristics. A balance, however, has
to be maintained among the physical properties of capsule membranes so as to support the
entrapped cells survival. The mass transport properties of a membrane are critical since
the influx rate of molecules, essential for cell survival, and the outflow rate of metabolic
waste ultimately determines the viability of entrapped cells. Ordinarily the desired
capsule permeability is determined by the molecular weight eut-off (MWCO), and is
application dependent. The MWCO is the maximum molecular weight of a molecule that
is allowed passage through the pores ofthe capsule membrane54. For transplantation, the
MWCO must be high enough to allow passage of nutrients, but low enough to reject
antibodies and other immune molecules. The MWCO of orally delivered microcapsules
must allow for the passage ofunwanted metabolites from the plasma into the
microcapsule, and then must either facilitate the subsequent removal of the altered
molecule or provide for its storage54. The most common type of membrane used for cell
therapy is the single alginate based polymer membrane; however, several other
substances are being used such as various proteins, polyhemoglobin, and lipids54,56. Yet
another approach for membrane composition is to use a biodegradable synthetic polymer
such as polylactide, polyglycolic acid, and polyanhydride. Figure 2.1 summarizes sorne
commonly used membranes and their properties. The variability of artificial cell
membranes allows for many possibilities in cell therapy and raises expectation for their
wide spread use in the future.
12

Membrane (Molecular Weight eut-off)
Hollow Fiber Membrane (>200KD)
IgM (95OKDl Urease (482.7KD} C19(410KD} fltll"lflogen (339t<O) Phel1Ylalanine NHS Iy.a~ (320KD) Calame (247KO) C4(210K0}
Molecule
Figure 2.1: Molecular cut-off of different types ofmicrocapsule membranes18• The
molecular weights of various cens, enzymes, antibodies, complement
components, proteins, peptides and metabolites are listed on the right.
Abbreviations: C2-9 and C19, various components of the complement
cascade; Ig, immunoglobulin; IL-l, interleukin 1; NGF, nerve growth factor.
2.3.3 The classic method (APA microcapsules)
There are various methods available for preparing artificial cens containing live
bacterial cells for therapy. For example, for preparation ofthe c1assic alginate-polylysine
alginate (AP A) membrane, the live bacterial cens are suspended in a matrix of the natural
pol ymer alginate (1.5%). The viscous polymer-bacterial suspension is passed through a
23-gauge needle using a syringe pump. Sterile compressed air, passed through a 16-gauge
13

coaxial needle, is then used to shear the droplets coming out ofthe tip of the 23-gauge
needle. The droplets are allowed to gel for 15 minutes in a gently stirred ice-cold solution
of solidifying chemicals, such as CaCh (1.4 %). After gelation in the CaCh, the beads are
then washed with HEPES (0.05 % in HEPES, pH 7.20), coated with polylysine (0.1 % for
10 min) and washed again in HEPES (0.05 % in HEPES, pH 7.20). The resultant capsules
are then coated by reaction with alginate (0.1 % for 10 min) and washed with appropriate
chemicals to dissolve their inner core content. For this step a 3.00 % citrate bath (3.00 %
in 1: 1 HEPES-buffer saline, pH 7.20) is often used. The microcapsules formed can then
be stored at 4°C in minimal solution (10% cell nutrient to 90% water).
Figure 2.2: (A) Empty APA artificial cells. (B) APA membrane artificial cells
containing thousands of genetically engineered Lactobacillus plantarum 80
(pCBH 1) cells.
2.4 Use of live orally delivered bacterial cells for lowering cholesterol
14

A less known approach to reducing blood cholesterol, oral live bacterial cell
therapy, is based on the demonstration that bacteria such as Lactobaci/lus acidophilus,
Lactobaci/lus ruteri, Escherichia coli, Bifidobacteria bifidum, Eubacterium
coprostanoligenes and Lactobaci/lus bulgaricus, which are part of the normal intestinal
flora, can lower cholesterollevels significantl!O,31,57,58. Lactobaci/lus casei fermented
skim milk (FSM) has been shown to lower levels ofplasma triglycerides 10% to 30%59.
Indeed a number of studies have confirmed tbis capacity and it has been found that oral
daily intake oflive Lactobaci/lus cells in particular (found in yogurt) can lead to
significant reduction in cholesterollevels30,6o-63.
Although the mechanisms by which these bacteria lower cholesterol is not entirely
understood, it has been proposed that this could be the result of enhanced Bile Salt
Hydrolase (BSH) activity29,64 or suppressed re-absorption of cholesterol carrying bile
acids33. A recent study at the Shinshu University in J apan has found that Lactobacil/us
acidophilus bacteria suppressed the reabsorption of bile acids carrying cholesterol and
improved the removal of cholesterol from blood through stool excretion33. In another
study in Argentina, Lactobacil/us bacteria lowered total blood cholesterol by 22% percent
and triglycerides by 33% percene2. A research report from Denmark noted that
Lactobacil/us bacteria significantly lowered blood pressure in men and women 18 to 55
years of age after eight weeks of supplementation65. Those in the control group who did
not receive the selected strains of Lactobaci/lus bacteria did not experience a drop in their
high blood pressure. Thus, there is significant evidence that specific kinds of
Lactobaci/lus bacteria can lower the three major risk factors for coronary heart disease
and stroke, excessive cholesterol, high blood pressure, and high triglyceride levels.
Unfortunately, the therapeutic potential oflive bacterial cells has been hampered
by inherent limitations in their use. For example, a normal daily intake of 250 ml of
yogurt would only correspond to 500 milligram of cell dry weight (CDW) ofbacteria, and
of those bacteria ingested only 1 % would survive gastric transit limiting the overall
therapeutic effect29. There are also sorne practical concerns regarding the production,
cost, and storage of such a product29. Furthermore, oral administration of live bacterial
cells can pose problems. For example, large amounts oflive bacterial cells can stimulate
a host immune response, they can be retained in the intestine, and repeated large doses
15

could result in their replacing the nonnal intestinal flora34,35. In addition, risk of systemic
infections, deleterious metabolic activities, adjuvant side-effects, immuno-modulation and
risk of gene transfer has limited their use34,35. Even so, therapeutic applications oflive
nonnal or genetically engineered bacterial cells delivered orally are quite diverse,
highlighting their importance and potential for therapy. Table 2.1 is a comprehensive list
of the potential therapies based on the oral delivery offree live bacterial cells for therapy.
16

DiseaselTherapy Diarrhea
Colorectal Cancer
Inflammatory Bowel Disease
Ulceration
Steatorrhea of Lipids (malabsorption of lipids) Enhance Immunity
Lower Cholesterol
Chronic Kidney Failure
Kidney Stones
Table 2.1. Potential therapies based on the oral deliyeIY of free live bacterial ceUs Culture Mode of Action! Action L. rhamnosus, L. casei L. reuteri, L. GG B.lactis B. Bifidum, B. Bb12 Lactobacillus B. breve B.longum
L. lactis L. GG
L. acidophilus
B. plantarii
L. acidophilus L. casei (LeS) L. GG B. lactis, B. Bifidum
L. acidopilus L. bulgaricus L. reuteri
L. acidophilus Lactic Acid Bacteria
(L. acidophilus, L. plantarum, L. brevis, S. thermophilus, B. infantis) O·faecalis
Reduction of antibiotic-associated diarrhea in children and adults, treatment and prevention ofrotavirus and acute diarrhea in children and adults, prevention oftraveler's diarrhea. Certain strains of lactic acid bacteria promote serum and intestinal immune responses to rotavirus, and thus may be important in establishing immunity against rotavirus infections. Mechanisms may include: enhancing the host's immune response; binding and degrading potential carcinogens; alterations in the intestinal microflora incriminated in producing recognized carcinogens (e.g. bile acid-degrading bacteria); producing anticarcinogenic or antimutagenic compounds in the colon; alteration of the metabolic activities of the resident microflora;alteration ofphysicochemical conditions; effects on general physiology. Could provide an adjunct nutritional therapy for Crohn's disease, as the bacteria increase gut IgA immune response promoting the gut immunological barrier.
Down regulation of H pylori infection by inhibition of intestinal cell adhesion and invasion. Bacteria express lipolytic activity with substantial enzyme stability in human gastric juice leading to the increased absorption of lipids in the small intestine.
By one mechanism, innate immunity is enhanced by stimulating the activity of splenic NK cells. While antigen feeding alone was shown to prime for an immune response, cofeeding antigen and probiotic bacteria suppressed both antibody and cellular immune responses and may have the potential to attenuate autoimmune diseases (e.g. encephalomyelitis - by jointly dosing with myelill)asic protein and probiotic bacteria). 1. Bacteria may bind or incorporate cholesterol directly into the bell membrane. 2. Bile salt hydrolase (BSH) enzyme deconjugates intraluminal bile acids making them less likely to be reabsorbed into the enterohepatic circulation (ECH), causing de nova synthesis ofbile acids from blood serum cholesterol. Small bowel bacterial overgrowth is weIl known to occur in end-stage kidney failure and is responsible for producing uremic toxins and contributing to decreased nutritional wellbeing. Certain bacteria are shown to reduce blood levels ofuremic toxins produced in the intestine as bacterial putrefactive metabolites, especially that of indican, dimethylamine, and Nitrosodimethylamine (a carcinogen) by inhibiting bacterial production by means of correcting the intestinal microflora. Urinary excretion of oxalate, a major risk factor for renal stone formation and growth in patients with idiopathic calcium-oxalate urolithiasis, can be greatly reduced with treatment using a high concentration of freeze-dried lactic acid bacteria. Oxalate-degrading enzymes produced by these microorganisms or by Oxalobacter-type bacteria, breaks down the unwanted oxalate and can be used to prevent the subsequent evolution of kidney stones.
17
Ref. 66-81
U.S. Patent 5,443,826
82-85
66,86
U.S. Patent 5,443,826 87
88,89
lJO~93
30-32
94,95
'16,97

2.5 Potential of artificial ceUs for oral delivery of live bacterial cells for therapy
2.5.1 Principle of orally delivered artificial cells for oral therapy
Artificial cell microencapsulation is a technique used to encapsulate biologically
active materials in specialized ultra thin semi-penneable polymer membranes8,9. The
pol ymer membrane can protect encapsulated materials from harsh external environments,
while at the same time allowing for the metabolism of selected solutes capable of passing
into and out ofthe microcapsule. In this manner, the enclosed material (in this case live
bacteria) can be retained inside and be separated from the external environment, making
microencapsulation particularly useful for biomedical and clinical applications1o,12,98.
Studies show that artificial cell microcapsules can be used for oral administration of live
genetically engineered cells that can be useful for therapeutic functions 1S,16. Although the
live cells remain immobilized inside the microcapsules, microencapsulation do es not
appear to hinder their growth kinetics17• The microcapsules remain intact during passage
through the intestinal tract and are excreted intact with the stool in about 24 hours. The
cells are retained inside, and excreted with, the intact microcapsules addressing many of
the major safety concerns associated with the use oflive bacterial cells for various clinical
applications. The membranes of the microcapsules are penneable to smaller molecules,
and thus the cells inside the microcapsules metabolize small molecules found within the
gut during passage through the intestine9,IS-17,20,99. Figure 2.3 summarizes the basic
concept of artificial cells for oral delivery ofbacterial cells for therapy.
/
18

Substrates Metabolites
Figure 2.3: The principle of orally administered artificial cells containing bacterial cells
for therapy. The semipenneable membrane excludes antibodies, tryptic
enzymes and other external materials, but allows smaller molecules (amino
acids, bile acids, ammonia, gasses) to enter and be acted on by the enclosed
microorganisms. AIso, small molecules (including sorne peptides) produced
by the enclosed bacterial cells can be designed to diffuse out as part of the
therapeutic.
2.5.2 Microencapsulation: A solution to the limitations of free live bacterial cell
therapy
The advancement of recombinant technology has introduced a wide range of non
pathogenic genetically engineered bacterial cells, and other genetically engineered cells,
that pro duce potentially therapeutic products such as enzymes, cytokines, vaccines,
receptor proteins, honnones, growth factors, monoclonal antibodies, and other gene
therapy products. These methods show great promise, but to date have not had a great
19
impact on health care because of inherent difficulties in delivering these engineered
products to the relevant sites. Thus, of the obstacles that still remain, difficulty in the
efficient delivery of non-pathogenic genetically engineered cells in-vivo for therapy is of
major importance. Recently, Prakash and Chang proposed a new artificial cell therapy
concept and demonstrated its feasibility and efficacy for delivery of live genetically
engineered cells into the intestine for various clinical applicationsl5. This was based on
the following hypothesis: when given oraIly, live cells remain immobilized inside
microcapsules. The microcapsules remain intact as they pass down through the GI tract
and are excreted intact with the stool about 24 hours later. The membranes of the
microcapsules are permeable to smaller molecules often required for cell growth and
proliferation. Thus, during the passage through the intestine, small molecules such as
urea, ammonia, uric acid etc. can diffuse through the membrane enabling the cells inside
the microcapsules to utilize them. This results in a decreased systemic metabolite level.
Furthermore, through the intestinal tract, cells are retained inside the intact microcapsules
and therefore do not enter into the body circulation. This latter property, potentially limits
the major safety concems associated with the use of live bacterial cells for various clinical
applicationsl8. This novel concept has immediate application for microencapsulation
based oral therapy in renal failure and liver failure l5, physiologically responsive gene
therapy'IOO, and somatic gene therapylOI. Table 2.2 is a comprehensive list of the
potential therapies based on the oral delivery of microencapsulated bacterial cells for
therapy.
20
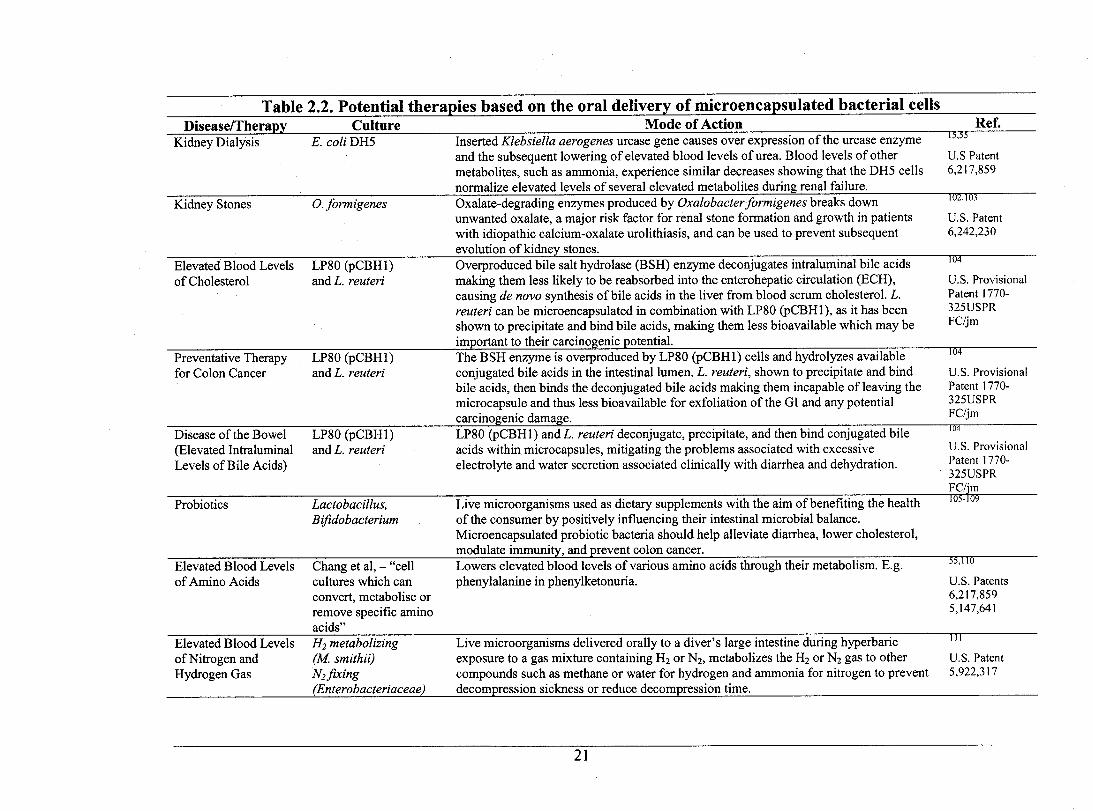
Table 2.2. Potential therapies based on tlle_ oral deliyery of microencapsulated bacterial cells Disease/Therapy
Kidney Dialysis
Kidney Stones
Elevated Blood Levels of Cholesterol
Preventative Therapy for Colon Cancer
Disease of the Bowel (Elevated Intraluminal Leve1s of Bile Acids)
Probiotics
Elevated Blood Levels of Amino Acids
Elevated Blood Levels ofNitrogen and Hydrogen Gas
Culture E. coliDH5
0. formigenes
LP80 (pCBHI) and L. reuteri
LP80 (pCBHI) and L. reuteri
LP80 (pCBHI) and L. reuteri
Lactobacillus, Bifidobacterium
Chang et al, - "ceU cultures which can convert, metabolise or remove specific amino acids" H2 metabolizing (U smithii) N2 flXing (Enterobacteriaceae)
Mode of Action Ref. Inserted K/ebsiella aerogenes urease gene causes over expression of the ureaseenzyme -î3;5S
and the subsequent lowering of elevated blood leve1s ofurea. Blood levels of other metabolites, such as ammonia, experience similar decreases showing that the DH5 ceUs normalize elevated leve1s of several elevated metabolites during renal failure. Oxalate-degrading enzymes produced by Oxa/obacter formigenes breaks down unwanted oxalate, a major risk factor for renal stone formation and growth in patients with idiopathic calcium-oxalate urolithiasis, and can be used to prevent subsequent evolution ofkidney stones. Overproduced bile salt hydrolase (BSH) enzyme deconjugates intraluminal bile acids making them less likely to be reabsorbed into the enterohepatic circulation (ECH), causing de nova synthesis of bile acids in the liver from blood serum cholesterol. L. reuteri can be microencapsulated in combination with LP80 (pCBHl), as it has been shown to precipitate and bind bile acids, making them less bioavailable which may be important to their carcinogenic potential. The BSH enzyme is overproduced by LP80 (pCBHI) ceUs and hydrolyzes available conjugated bile acids in the intestinal lumen. L. reuteri, shown to precipitate and bind bile acids, then binds the deconjugated bile acids making them incapable of leaving the microcapsule and thus less bioavailable for exfoliation of the GI and any potential carcinogenic damage. LP80 (pCBH 1) and L. reuteri deconjugate, precipitate, and then bind conjugated bile acids within microcapsules, mitigating the problems associated with excessive electrolyte and water secretion associated c1inicaUy with diarrhea and dehydration.
Live microorganisms used as dietary supplements with the aim ofbenefiting the health of the consumer by positively influencing their intestinal microbial balance. Microencapsulated probiotic bacteria should he1p aUeviate diarrhea, lower cholesterol, modulate immunity, and prevent colon cancer. Lowers elevated blood levels of various amino acids through their metabolism. E.g. phenylalanine in phenylketonuria.
Live microorganisms delivered oraUy to a diver's large intestine during hyperbaric exposure to a gas mixture containing H2 or N2, metabolizes the H2 or N2 gas to other compounds such as methane or water for hydrogen and ammonia for nitrogen to prevent decompression sickness or reduce decompression time.
21
V.S Patent 6,217,859
102,103
V.S. Patent 6,242,230
104
V.S. Provisiona1 Patent 1770-325VSPR FC/jm
104
V.S. Provisiona1 Patent 1770-325VSPR FC/jm J()4
V.S. Provisiona1 Patent 1770-325VSPR FC/jm 105:109
55,110
V.S. Patents 6,217,859 5,147,641
III
V.S. Patent 5,922,317
2.5.3 Membranes used for artificial ceUs for oral delivery of bacterial ceUs
The design of a membrane, intended for use in oral live bacterial cell therapy,
must take into consideration several primary factors so as to minimize microbial death
and maximize therapeutic effectiveness. To assure their efficacy, artificial cells intended
for oral administration, must be designed to proteet their living cargo against both the
acidic environrnent of the stomach and immunoglobulin released by the intestinal
immune response. For this reason research has historieally focused on the buffering
capability of mierocapsule membranes in simulated human gastrie environments and the
ability of various membranes to oppose immunoglobulin penetration. Several examples of
artificial cell design follow with ernphasis on research related to these core and essential
characteristics.
Rao et al., 1989, described a method to encapsulate freeze-dried B. pseudolongum
using cellulose acetate phthalate (CAP) coated with beeswax, showing that encapsulated
B. pseudolongum is able to survive the simulated gastric environrnent in larger numbers
than non-encapsulated cellsI12;113. A Brazi1ian group recently prepared probiotic
microorganisms inc1uding Lactobacillus and Bifidobacteria by spray drying, again using
CAP as the wall material, and have evaluated the resistance of these microorganisms to
drying at three temperatures and have evaluated in-vitro tolerance to pH values and
simulated human bile concentrationsJOs. They found that the CAP prepared
microorganisms were better able to protect the microorganisms from an acidic
environrnent and were resistant to conditions of a simulated human bile environrnent1os.
In another study, encapsulation of Bifidobacteria in a butter oil and whey based medium
was proposed, but was shown to be ineffective in preventing acid in jury to bacteria in
both low acid and high acid environrnentsl14.
Overall, calcium alginate and k-carrageenan-Iocust bean gurn gel beads have been
the two most commonly used polymers for immobilizing viable cellslls,116. Alginate
beads, however, have displayed the undesirable property oflimited acid resistance, and it
has been reported that alginate beads undergo shrinkage and decreased mechanical
strength in acidic conditionsll7,1l8. In order to overcome this challenge, coating the
bacteria by cross linking with a carboxyvinyl pol ymer carrier has been suggested and was
22
shown to be effective for intestinal delivery1l9. K-carrageenan-Iocust bean gum gel beads
are less sensitive to acidic conditions than alginate beads and hence have been used for
lactic fermentation. The formation ofk-carrageenan-Iocust bean gum beads, however,
requires a high concentration of potassium ions and for this reason two major limitations
preclude their widespread use: Firstly, high concentrations of potassium ions could
potentially damage the cells of B. longum during lactic fermentationI2o,121; and secondly,
it has been pointed out that, as potassium ions are important in maintaining electrolyte
equilibrium their inclusion in the diet in large amounts would not be recommended 122,123.
Gellan-xanthan beads, on the other hand, are not only acid resistant, but are also
stabilized by calcium ionsl24, suggesting that they could be a good candidates for
immobilizing bacterial cells and protecting them against acid injuryl25; however, gellan
xanthan beads do not pro vide adequate immune protection.
Similarly, agarose microcapsules prepared by emulsification/internal
gelationization for oral delivery of Bacillus Calmette-Guerin (BCG) cells, although stable
for up to 12 months in-vitro, have not yet been shown suitable for oral delivery, as
agarose membranes do not provide sufficient immunoprotectionI24,126. Thus, agarose
microspheres with the addition ofvarious polymer coatings have been proposedl27.
Among other formulations, gelatin and polymer coated gelatin capsules have been studied
for oral delivery oflive bacterial cells106,128. Although gelatin (with 20% w/v ofthe
pol ymer) has shown promising results in vitro, a radiological study among human
volunteers has shown that uncoated gelatin capsules disintegrate within 15 minutes of
ingestionI29,130.
Although a host of other formulations have been studied to date (including using
gum arabic, milk derived whey proteins, soluble starch, and others34,107,108,128,131-134) the
most promising formulation is the encapsulation of calcium alginate beads with poly-L
lysine (PLL) forming alginate-poly-L-Iysine-alginate (APA) microcapsules. In the APA
membrane microcapsule, alginate forms the core and matrix for the cell and PLL binds to
the alginate core. Binding ofPLL to alginate is the result ofnumerous long-chain alkyl
amino groups within PLL that extend from the polyamide backbone in a number of
directions and interact with various alginate molecules, through electrostatic interactions.
The resulting cross-linkage produces a stable complex membrane that reduces the
23
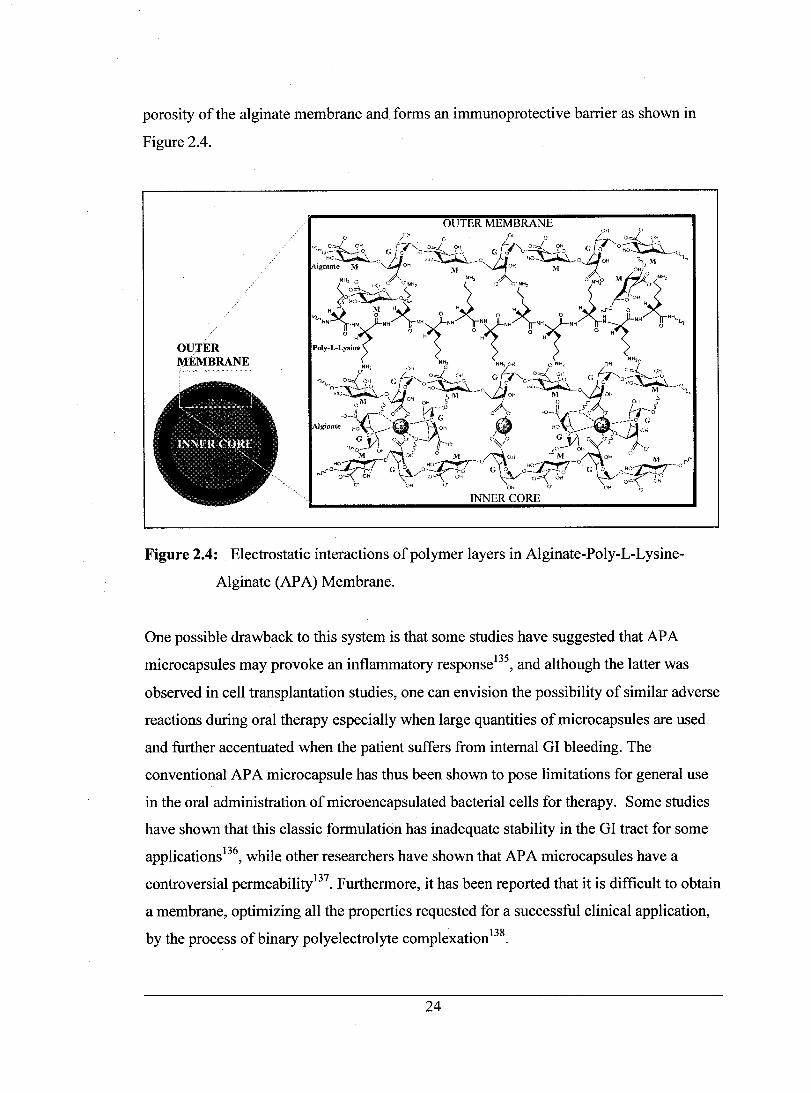
porosity of the alginate membrane and forms an immunoprotective barrier as shown in
Figure 2.4.
OUTER MEMBRANE
Figure 2.4: Electrostatic interactions ofpolymer layers in Aiginate-Poly-L-Lysine
Alginate (APA) Membrane.
One possible drawback to this system is that sorne studies have suggested that AP A
microcapsules may provoke an inflammatory response135, and although the latter was
observed in cell transplantation studies, one can envi sion the possibility of similar adverse
reactions during oral therapy especially when large quantities of microcapsules are used
and further accentuated when the patient suffers from internaI GI bleeding. The
conventional AP A microcapsule has thus been shown to pose limitations for general use
in the oral administration of microencapsulated bacterial cells for therapy. Sorne studies
have shown that this classic formulation has inadequate stability in the GI tract for sorne
applicationsl36, while other researchers have shown that APA microcapsules have a
controversial permeability137. Furthermore, it has been reported that it is difficult to obtain
a membrane, optimizing ail the properties requested for a successful clinical application,
by the process ofbinary polyelectrolyte complexation138•
24

A potential solution to these problems is the use of multi-Iayer membrane formation
based on the electrostatic attraction of oppositely charged macromolecules with a charge
reversaI at each step of the macro-ion adsorption. This technique makes it possible to
modulate the MWCO and retain high mechanical stability at the same time. SpecificaIly,
AIginate/Poly-I-lysinelPectinIPoly-I-lysine/ Alginate (APPPA), AIginatelPoly-l
lysinelPectinlPoly-I-lysinelPectin (APPPP), and AIginatelPoly-L-lysine/ChitosanlPoly-l
lysine/Alginate (APCP A) membranes have been prepared and tested for their strength and
GI stability139,140. It has been shown that these multi-Iayer membrane formulations
perform weIl in GI stability tests, providing for increased resistance to complete
dissolution in water, dilute acids and base, as weIl as in the presence of ion chelators,
while allowing for more precise control over membrane permeability. While this is
emerging and prospective technology, many formulations for the encapsulation oflive
cells have been attempted by various research groups. Table 2.3 is a non-inclusive list of
promising polymers used for live cell encapsulation (with permission from Satya Prakash
and Hahn Soe-Lin, unpublished work).
25

Table 2.3 Established/promising polymers for live cell encapsulation. Polymer Features AP A Strengths: ShortlMedium-tenn Mechanical Stability, [Alginate-Poly(l-Lysine)- flexible pennselectivity, established synthesis Alginate] protocols, low immunogenicity when PEGylated + Variants (IPEG, lBa+2, /Ca+2) Weaknesses: Susceptible to long-tenn Ca+210ss,
consequent mechanical instability, structurally rigid,
A-PMCG-A [ Alginate-poly(methylene-coguanidine)-Alginate]
HEMA-MMA (HydroxymethylacrylateMethyl Methacrylate)
Multi-Iayered HEMA-MMAMAA
PAN-PVC [poly( acrylonitrilevinylchloride)]
AN-69 (Acrylonitrile/Sodium Methallylsulfonate)
PEGIPDsfPDMS [poly( ethylene glycol) / poly(pentamethylcyclopentasilo xaQe) /poly( dimethylsiloxane)] PDMAAm [Poly (N,N-dimethyl acrylamide)]
Siliceous Encapsulates
CS/AlPMCG [Cellulose Sulphate/Sodium AIginatelPoly(Methylene-CoGuanidine)]
must be PEGylated to prevent fibrotic overgrowth Strengths: Better mechanical stability than Ca +2 / A, Ba +2/ A, BAP A, PMCG cheaper than PLL, capsule size / penneability independently adjustable Weaknesses: Immunogenicity, long-tenn mechanical stability yet to be detennined
Strengths: Insolubility in aqueous solutions conf ers greater mechanical stability Weaknesses: non-adherent membrane properties requires co-encapsulation with matrix to facilitate anchorage-dependent cell adhesionlgrowth Strengths: Exceptional design flexibility, independent adjustment of mechanical stability, p~nnselectivity, promising compatibility with blood-contact applications Weaknesses: Single-layered capsules possess insufficient mechanical stability, immunogenicity yet to be detennined, synthesis protocol more complex than other designs Strengths: established mechanical stability, pennselectivity, good biocompatibility Weaknesses: Molecular-weight cut-offs currently in question, long-tenn immunogenicity not yet established Strengths: good mechanical stability, pennselectivity, amitogenic, large-scale encapsulation (-50 million cells/minute) now possible Weaknesses: Immunogenicity not well established Strengths: good mechanical stability, PDMS conf ers excellent oxygen penneability Weaknesses: long-tenn fibrogenicity not ideal
Strengths: improved mechanical stability when crosslinked with telechelic stars Weaknesses: oxygen penneability inferior to copolymers with PDMS Strengths: Simple synthesis mechanism confers high design flexibility Weaknesses: Questionable toxicity, immunogenicity Strengths: Short-tenn applications negate long-tenn mechanical stability and biocompatibility concems Weaknesses: Encapsulated cells sensitive to alginate purity
26
References 141-156
15/
158-164
165
166-171
172
173,174
l7S
174,176-178
179-184
PREFACE FOR CHAPTER 3 TO 5
To evaluate the feasibility ofthe novel approach ofusing immobilized and/or
microencapsulated genetically engineered Lactobacillus plantarum 80 (pCBH 1) bacterial
cells for lowering blood serum cholesterol, both immobilized and microencapsulated
Lactobacillus plantarum 80 (pCBH 1) were prepared using a laminar liquid jet frequency
superimposition method. The preparation of immobilized beads containing the genetically
engineered organism is described in Chapter 4 and the preparation of alginate
polylysine-alginate microcapsules containing the bacteria cells is described in Chapter 5.
The determination of an appropriate HPLC assay for the in-vitro measurement of
bile acids, chosen for their relation to cholesterol in the enterohepatic circulation ofbile,
and the modification and calibration ofthat assay is presented in Chapter 3.
Based on the assay described in Chapter 3, 1 proposed and developed two in-vitro
experiments for determining the efficacy and suitability, ofboth immobilized beads and
microcapsules congaing Lactobacil/us plantarum 80 (pCBH 1), for various potential
applications.
Chapter 4 describes the specific details of the removal of physiologically relevant
levels ofbile acid, by the immobilized bacteria, and describes sorne potential
applications. Chapter 5 describes the specific details of the removal ofphysiologically
relevant levels of bile acid by the microencapsulated bacteria, provides a summary of the
physiological interrelationship between bile acids and cholesterol, and predicts the oral
doses of microencapsulated Lactobacil/us plantarum 80 (pCBH 1) cells required for
lowering cholesterol.
27

The results obtained in my research have been presented in the following papers:
Research articles:
1. Mitchell Lawrence Jones, Hongmei Chen, Wei Ouyang, Terrence Metz, and Satya
Prakash (2003). Method for Bile Acid Determination by High Performance Liquid
Chromatography. Journal of Medical Sciences; 23(5):277-280.
2. Mitchell Lawrence Jones, Christopher Martoni, Hongmei Chen, Wei Ouyang,
Terrence Metz, Satya Prakash (2003). Deconjugation of Bile Acids with Immobilized
Genetically Engineered Lactobacillus plantarum 80 (PCBH1). Manuscript (in press).
Applied Bionics and Biomechanics.
3. M.L. Jones, H. Chen, W. Ouyang, T. Metz, and S. Prakash (2003). Microencapsulated
genetically engineered Lactobacillus plantarum 80 (PCBH1) for bile acid
deconjugation and its implication in lowering cholesterol. Manuscript (in press).
Journal ofBiomedicine and Biotechnology.
Proceedings and Abstracts:
1. Jones, M.L., Chen, H., Ouyang, W., Metz, T., and Prakash, S (2003). Deconjugation
of Bile Acids with Immobilized Genetically Engineered Lactobacillus Plantarum 80
(PCBHl). Abstract. The 6th International Congress of the Cell Transplant Society.
Atlanta, Georgia.
2. Prakash S., Jones M. (2002). Engineering Artificial Cells for Therapy. Proceedings.
2nd World Engineering Congress 2002. Sarawark, Malaysia, pp. 91-93.
3. Prakash S., Jones M. (2002). Engineering Artificial Cells for Therapy. Abstract. 2nd
World Engineering Congress 2002. Sarawark, Malaysia.
Patent:
1. Prakash S., and Jones M.L. (2003). Immobilized bacteria to lower bile acids and/or
cholesterol. U.S. Provisional Patent [1770-325USPR FC].
28

In accordance with McGill University regulations, three of the above manuscripts
(the major publications 1 to 3) are reported in their original form in full as individual
chapters (Chapters 3 to 5).
29

CHAPTER3
ORIGINAL PAPER: METHOD FOR BILE ACID DETERMINATION BY HIGH
PRESSURE LIQUID CHROMATOGRAPHY
Mitchell Lawrence Jones, Hongmei Chen, Wei Ouyang, Terrence Metz, and Satya Prakash *
Journal of Medical Sciences 2003;
23(5):277-280.
* Corresponding Author
30

3.1 Introduction:
The accurate identification and quantitative measurement of various bile acids by
high-performance liquid chromatography (HPLC) has been described for determining and
measuring the major conjugated bile acids in human bile185,186. Traditionally, methods to
separate such mixtures have required a lengthy workup, and while producing accurate
results, the extraction and evaporation processes have not been practical for experiments
with high sample volumes. The method for bile acid separation identified here has several
operational advantages and dearly outweighs the available alternatives for the purpose,
by allowing for efficient and accurate identification and quantitative measurement of
various bile acids, while preserving the quality of bile acid separation.
3.2 Background: Several high-performance liquid chromatographic (HPLC) methods
have been described for determining and measuring the major conjugated bile acids in
human bile185,186. Traditionally, in-vitro bile acid experimentation has involved the use of
HPLC to determine the quantity ofvarious tauro- and glycol- conjugates in complex
mixtures ofbile acids in aqueous media187,188. Methods to separate such mixtures used in
in-vitro human bile experiments have required a lengthy workup involving a (1 :4; v:v)
sample: isopropanol extraction followed by an evaporation and re_suspension29,187,188.
While these methods can produce accurate results, the extraction and evaporation
processes are labor intensive, time consuming and not practical for experiments requiring
intensive sampling. Methods: To generate a standard set of results, standard solutions of
glycholic acid (GCA), taurodeoxycholic acid (TDCA), and glycodeoxycholic acid
(GDCA) were prepared and concentrations were determined by a reversed-phase C18
HPLC column, running acetate buffer and methanol (30:70). The flow rate was 1.0
ml/min and detection was performed at 205 nm. Results: The chromatograms show
adequate resolution and normal retenti on times and the calibration curves have correlation
of determinants factors (R2) ranging from 0.9920 to 0.9895. Conclusions: The method
for bile acid separation identified here eliminates the time intensive and labor intensive
workup step of evaporation, allowing for an efficient workup while preserving the quality
of bile acid separation and quantification.
Key words: bile acid, conjugated, chromatography
31

3.3 Materials and Methods:
Reagents: The sodium salts of glycocholic acid (GCA), taurodeoxycholic (TDCA), and
glycodeoxycholic acid (GDCA) were supplied by SIGMA (St. Louis MO, USA). The
water was purified with an EASYpure™ RO Reverse Osmosis System and a
NANOpure® Diarnond™ Life Science (UV /UF) ultrapure water system from
Barnstead/Therrnoline (Dubuque, lA, USA). Methanol was HPLC-gradient from Fisher
Scientific (Fair Lawn, NJ, USA). AlI other chemicals were of anal yti cal grade.
Apparatus: The HPLC system was made up of two ProStar 210/215 solvent delivery
modules, a ProStar 320 UVNis Detector, a Pro Star 410 Auto S arnpler, and Star LC
Workstatin Version 6.0 software was used.
Operating conditions: The HPLC method was perforrned under isocratic conditions at
room temperature. Analyses were perforrned on a reversed-phase C-18 colurnn:
LiChrosorb RP-18, 5 !lm, 250 x 4.6 mm from HiChrom (Novato, CA, USA). Acetate
buffer was prepared daily with 0.5 M sodium acetate, adjusted to pH 4.3 with 0-
phosphoric acid, and filtered through a 0.22 /lm filter (Whatman®, England). The flow
was 1.0 ml/min and the detection was perforrned at 205 nrn. The injection loop was set to
20/l1.
Sample Preparation:
i.) Standard solutions of GCA, TDCA, and GD CA were prepared in HPLC-grade
methanol and then filtered through a 0.22 /lm syringe driven HPLC-filter (Millipore,
Japan).
ii) Complex mixtures of TDCA, and GD CA bile acids were dissolved in MRS bacterial
growth medium (Difco, Sparks, MD, USA). Half mL sarnples were withdrawn and
acidified by 5 /lI of 6 N HCI to stop any further enzyrnatic activity. From the 0.5 ml
sarnple, bile salts were then extracted using methanol (1: 1; v:v) with 4.0 mM of GCA
dissolved and used as the internaI standard. Sarnples were mixed vigorously for 10 min
and centrifuged at 1000 g for 15 min. The supematant was then filtered through a 0.22 /lL
syringe driven HPLC-filter (Millipore, Japan).
3.4 Results and Discussion:
32

To generate a standard set of results, representing perfect runs at different
concentrations of bile acids, we prepared standard solutions of GCA, TDCA, and GDCA
in HPLC-grade methanol and determined their concentration by HPLC. Figure 3.1 shows
the superimposed chromatograms of standard solutions of varying, but equal,
concentrations of GCA, TDCA, and GDCA, and the corresponding calibration curves.
The chromatograms show adequate resolution and normal retenti on times and the
calibration curves have correlation of determinants factors (R2) ranging from 0.9920 to
0.9895.
To test our method for preparing aqueous samples containing bile acids, several
complex mixtures of TDCA and GD CA, conjugated bile acids, were dissolved in MRS
bacterial growth medium and extracted using methanol (l: 1; v:v). Extraction with
isopropanol was attempted (1: 1, 1 :2, and 1 :4; v:v); however, the results proved to produce
unacceptable variations in peak times, hence methanol proved to be the extraction solvent
of choice. Figure 3.2 shows the superimposed chromatograms ofvarying sampI es of each
of TDCA and GDCA and the corresponding calibration curves with correlation of
determinants factors (R2) ranging from 0.9984 to 0.9986. A 4 mM GCA internaI standard
was added to the sampI es at the beginning of sample preparation to mitigate any
quantitative changes to the sample during preparation. The chromatograms show
adequate resolution and normal, if not slightly shorter, retenti on times; however, the
TDCA and GDCA peaks in figure 3.2 experience fronting and change in retenti on times.
This may be due to overloading or reduced attraction of bile acid molecules for the
stationary phase causing them to move through the column faster.
33

00.
00'
.00 l GCA(8.960)
;; 300 --:
,§. 1 " = 200-1 e ...
j : J
i 1
l .1
TDCA (12.697)
10 1 15 1
Retention Time (min)
18000-
16000-
_14000~ !" 1
~12000~
!.10000 -
:: : :.8000-,
~~-: : 4000 ~
;; 2000 ~
IOmM ?; m\~
7111:\1
201
'. GDC -LI'*I,(GOCj
~~L
10 12
Figure 3.1: Chromatogram of standards ofeach of GCA, TDCA, and GDCA in methanol. Inlayed are the
calibration curves with the correlation of determinants factors: rTDCA: 0.9895 and rGDCA: 0.992.
60.
• TOC 1
HOC -L .... {GOC}
1 00.
40.
;; ConcenttltlonlmM)
,§. 30.
~ = e ... Il ~
i 20. GDCA (15.777)
TDCA (11.535)
<=l
100
" Retention Time (min)
Figure 3.2: Chromatogram of samples of each of TDCA and GDCA with GCA internaI standard. Inlayed
are the calibration curves with the correlation of determinants factors: rTDCA: 0.9976 and rGDCA:
0.9984.
34
The accurate identification and quantitative measurement of various bile acids is
clearly possible using this method. This method for preparing aqueous bile acid sampI es
could also be applied to more complex mixtures of bile acids, including mixtures of both
conjugated and free bile acids that require more sensitive HPLC detection columns and
solventsl86, eliminating the presently used labor intensive and time consuming two-step
sample preparation procedures. The speci fi cit y of determining conjugated from free bile
acids should prove to depend upon the separation conditions, as it appears that the above
outlined method of sample preparations is satisfactory. Hence, interference from related
compounds like deoxycholic acid and cholic acid, both free bile acids, should prove
minimal using the outlined preparatory method and an adequate separation technique 186.
Thus, this method has several operational advantages and clearly outweighs the available
alternatives for the purpose 29,187,188. Presently used methods are expensive, wasteful, and
labor intensive, whereas the method identified here is accurate, relatively inexpensive,
quick, and easy to perform. This would, therefore, provide an efficient and productive
mode for future bile acid research.
3.5 Acknowledgements
We gratefully acknowledge financial support from the Natural Sciences and
Engineering Research Council (NSERC) of Canada.
35

CHAPTER4
ORIGINAL P APER: DECONJUGATION OF BILE ACIDS WITH IMMOBILIZED
GENETICALLY ENGINEERED LA CTOBA CILL US PLANTARUM 80 (pCBHl)
MANUSCRIPT IN PREss IN ApPLIED BIONICS AND BIOMECHANICS
Mitchell Lawrence Jones, Hongmei Chen, Wei Ouyang, Terrence Metz, and Satya Prakash *
* Corresponding Author
36
4.1 Abstract
Bile acids are important to nonnal human physiology. However, bile acids can be
toxic when produced in pathologically high concentrations in hepatobileary and other
diseases. This study shows that immobilized genetically engineered Lactobacillus
plantarum 80 (pCBHl) (LP80 (PCBHl» can efficiently hydrolyze bile acids and
establishes a basis for their use. Results show that immobilized LP80 (pCBH 1) is able to
effectively break down the conjugated bile acids glycodeoxycholic acid (GD CA) and
taurodeoxycholic acid (TDCA) with bile salt hydrolase (BSH) activities of 0.17 and 0.07
Ilmol DCA/mg CDW /h respectively. The deconjugation product, deoxycholic acid
(DCA), was diminished by LP80 (PCBH1) within 4 h ofinitial BSH activity. This in-vitro
study suggests that immobilized genetically engineered bacterial cells has important
potential for deconjugation of bile acids for lowering ofhigh levels of bile acids for
therapy.
Key words: Immobilization, bile acid, bile salt hydrolase, glycodeoxycholic acid,
taurodeoxycholic acid, genetically engineered Lactobacillus plantarum cells.
4.2 Introduction
Bile acids are important physiological agents that are required for the disposaI of
cholesterol and the absorption of dietary lipids and lipid soluble vitamins. Bile salts are
the water-soluble end products of cholesterol, and are synthesized in the liver. During
nonnal enterohepatic circulation (EHC), the average bile salt pool of 4.0 g is secreted into
the duodenum twice during each meal, or an average of 6-8 times per day 47,48. During
intestinal transit, 90-95% of secreted bile salts are absorbed in the tenninal ileum and are
retumed to the liver via the portal vein 49. The bile salt pool is held approximately
constant and is replenished by hepatic synthesis of new bile from serum cholesterol. Daily
bile acid secretions approach 20-30 g 47,48 or 20-60 mmol 189 sustaining an intestinal bile
salt concentration of 5-20 mM 49. During intestinal transit, 90-95% of secreted bile salts
are reabsorbed in the tenninal ileum and are retumed to the liver via the portal vein 190.
37
About 75 per cent ofthe bile acid secretion is reabsorbed in the conjugated form in an
active sodium-dependent way 49. The remaining 25 per cent is hydrolyzed during
intestinal transit and only 15 per cent is reabsorbed in a passive way 190. Thus, only 60 per
cent of deconjugated bile acids are reabsorbed and one mmol of deconjugated bile salt is
responsible for a 0.4 mmol faecal excretion 48.
Although bile acids are important to normal human physiology, bile acids can be
cytotoxic agents when produced in pathologically high concentrations. Increased blood
bile acid levels is a known symptom ofhepatobileary disease and increased blood levels
can be measured in the urine by sulphated bile acid concentrations 191-193. As weIl, when
ileal transport of bile acids is defective due to a congenital defect, resection of the ileum,
or disease, a compensatory increase in bile biosynthesis occurs and an increased amount
of bile acids pass into the colon 194. An elevated intraluminal concentration of bile acids
induces the secretion of electrolytes and water causing diarrhea, loss of electrolytes, and
dehydration. Furthermore, deconjugated bile acids are believed to be associated with diet
related colon carcinogenesis 195-197.
Bile acid sequestrants (BAS) have been shown to lower elevated intraluminal
concentrations of bile acids and can provided sorne symptomatic benefit 194. BAS bind
bile acids in the intestine and form insoluble complexes that are excreted in the feces. It
has been weIl demonstrated over the last 20 years that BAS alone can diminish
intraluminallevels of bile acids, and through interruption of the ECH even reduce blood
serum cholesterollevels 7,50. However, the common BAS Cholestyramine resin
(Locholest, Questran), Colesevelam (WelChol), and Colestipol (Colestid) are weIl
documented to exhibit major adverse effects such as nausea, bloating, constipation, and
flatulence 51. Furthermore, there have been problems with gaining over-the-counter
(OTC) status for BAS, as it uses adsorbents and binders which are found to be
unacceptable for this classification by the V.S. Food and Drug Administration (FDA). In
fact, in 1995 Bristol-Myers Squibb's application to change Questran, the company's BAS
cholesterol-Iowering medication, to OTC status was denied by the FDA 51.
Removal ofbile salts from the gastrointestinal tract, through the enzymatic action
of the Bile Salt Hydrolase (BSH) enzyme, has been proposed and it has been shown that
Lactobaci/li bacteria have the ability to hydrolyze bile salts in the intestinal tract 29,30,195.
38

However, much work needs to be done to establish that lowering luminallevels ofbile
salts by this approach can be both effective and safe.
Immobilization is a technique used to surround and irnrnobilize biologically active
materials in specialized polymer beads 9,198,199. The pol ymer bead can protect biological
materials from harsh extemal environrnents, while at the same time allowing for the
metabolism of selected solutes capable of passing into and out of the polymer
surrounding. In this manner, the enclosed material (in this case live bacteria) can be
retained inside and be separated from the extemal environrnent, making immobilization
particularly useful for biomedical, clinical, and industrial applications 10,12,98,198,199.
Studies show that the irnrnobilization of cells can be used for both cell implantation and
oral administration oflive genetically engineered cells that can be useful for therapeutic
functions 15,16,200,201. In this article we study the potential of irnrnobilized genetically
engineered Lactobacillus plantarum 80 (pCBH 1) for assimilating a complex mixture of
hurnan bile acids in-vitro to develop a method for the deconjugation of bile acids and
potentially an effective therapy method to lower pathologically high levels of bile acids in
clinical conditions.
4.3 Materials and Methods
Media and chemicals
The sodium salts of glycocholic acid (GCA), taurodeoxycholic (TDCA),
glycodeoxycholic acid (GDCA), and deoxycolic acid (DCA) were supplied by SIGMA
(St. Louis MO, USA). De Man-Rogosa-Sharpe (MRS) broth was obtained from Difco
(Sparks, MD, USA). The water was purified with an EASYpure™ RO Reverse Osmosis
System and a NANOpure® Diarnond™ Life Science (UVIUF) ultrapure water system
from Bamstead/Therrnoline (Dubuque, lA, USA). Methanol was HPLC-gradient from
Fisher Scientific (Fair Lawn, NJ, USA). AlI other chemicals were of analytical grade.
Bacterial strains and growth conditions
The bacterial strain used in this study was the bile salt hydrolytic (BSH) isogenic
Lactobacillus plantarum 80 (PCBHl) strain. Overproduction of the BSH enzyme in LP80
39

(pCBH1) was obtained as described by Christiaens et al 202. The BSH overproducing
LP80 (pCBH 1) strain carries the multicopy plasmid pCBH 1 carrying the LP80 (pCBH 1)
chromosomal bsh gene and an erythromycin resistance gene. The Lactobacillus strains
were grown in MRS broth at 37°C in a Sanyo MIR-162 bench top incubator. The MRS
broth was supplemented with 1 00 ~g/ml erythromycin from Fisher Biotech (Fair Lawn,
NJ, USA) to select for bacteria carrying the multicopy plasmid pCBH1.
Immobilization ofLactobacillus plantarum 80 (PCBHl)
Low viscosity alginate, 1.5%,50 ml (Kelco, Chicago, IL), solution was prepared
and filtered through a 0.22 ~m Sterivex-GS filter (Millipore, Bedford, MA) into a sterile
60 ml syringe. LP80 (pCBH 1) was grown at 37°C in MRS broth and prepared as a
concentrated microorganism suspension by re-suspension of microorganism in 10 ml of
sterilized physiologic solution. The 10 ml concentrated microorganism suspension was
added to the 50 mllow viscosity alginate solution and mixed weIl. The
alginate/microorganism mixture was immobilized, through a 300 ~m nozzle, into a
filtered solution ofCaCh with an Inotech Encapsulator 1ER-20 (Inotech Biosystems
International Inc., Rockville, MD). This procedure was performed in a Microzone
Biological Containment Hood (Microzone Corporation, ON, Canada) to assure sterility.
The immobilized LP80 (pCBH1) was stored in 1.0 L minimal solution (10% MRS and
90% Physiologic Solution) at 4°C.
BSH activity ofimmobilized Lactobacillus plantarum 80 (PCBHl) alginate beads.
To investigate the BSH activity ofthe immobilized BSH overproducing LP80
(PCBH1), batch experiments were performed. Five grams cell dry weight (CDW) of
immobilized LP80 (PCBH1) was added to fresh MRS broth to which 10.0 mM GD CA
and 5.0 mM TDCA were added. Samples were taken at regular time intervals during the
24 h incubation to determine the bile salt concentration in the reaction vessels. The
experiment was performed in triplicate.
Bile salt hydrolase assay
40
A modification ofthe HPLC-procedure described by Scalia 188 was used to
determine BSH activity. Traditionally, in-vitro bile acid experimentation has involved the
use ofHPLC to determine the quantity ofvarious tauro- and glycol- bile acids in complex
mixtures ofadded bile acids in complex aqueous media 187,188,203. Methods to separate
such mixtures have required a lengthy workup involving a (1 :4; v:v) sample:isopropanol
extraction followed by evaporation and resuspension steps 187,203,204. While this method
can produce accurate results, we eliminated the time consuming and labor intensive
workup step of evaporation, allowing for an efficient workup while preserving the quality
ofbile acid separation and quantification.
Analyses were performed on a reversed-phase C-18 column: LiChrosorb RP-18, 5
~m, 250 x 4.6 mm from HiChrom (Novato, CA, USA). The HPLC system was made up
oftwo Pro Star 210/215 solvent delivery modules, a Pro Star 320 UVNis Detector, a
Pro Star 410 AutoSampler, and Star LC Workstation Version 6.0 software was used. The
solvents used were HPLC-grade methanol (solvent A), and solvent B, which was acetate
buffer prepared daily with 0.5 M sodium acetate, adjusted to pH 4.3 with o-phosphoric
acid, and filtered through a 0.22 ~m filter (Whatman®, England). An isocratic elution of
70 per cent solvent A and 30 per cent solvent B was used at a flow rate of 1.0 ml/min at
room temperature. An injection loop of 20 ~l was used, and the detection occurred at 205
nm within 25 min after injection of the bile salt extract.
Quarter milliliter sampI es to be analyzed were acidified by the addition of2.5 ~l
of6 N HCI to stop any further enzymatic activity. A modification of the extraction
procedure described by Cantafora was used 29,187. From the 0.25 ml sample, bile salts
were extracted using a solution of methanol (1: 1; v:v). GCA was added as an internaI
standard at 4.0 mM. The sampI es were mixed vigorously for 10 min and centrifuged at
1000 g for 15 min. The supernatant was then filtered through a 0.22 ~L syringe driven
HPLC-filter (Millipore, Japan) and the samples were analyzed directly after filtration.
4.4 Results
Preparation of alginate beads containing immobilized genetically engineered
Lactobacillus plantarum 80 (PCBH1) cells
41
Alginate beads containing immobilized genetically engineered Lactobacil/us
plantarum 80 (PCBH1) cells (Figure 4.1) were prepared using the methods described
above and were stored at stored at 4 0 C for use in experiments. Sterile conditions and
procedures were strictly adhered to during the process of immobilization.
Determination of Bile Acids by HPLC
We prepare a calibration curve to quantifying the HPLC sample results. For this
known quantities of GDCA and TDCA were added to MRS broth and 0.25 mL sampI es
and analyzed using the modified HPLC bile salt hydrolase assay outlined above. Figure
4.2 shows the calibration curves for TDCA and GDCA with a 4.0 mM GCA internaI
standard and correlation ofdeterminants factors (R2) of 0.997829 and 0.993246
respectively. Result shows (Figure 4.2) that this modified method allows accurate
identification and quantitative measurements ofvarious bile acids.
BSH activity of alginate beads containing immobilized Lactobacillus plantarum 80
(PCBHl)
To investigate the BSH activity of alginate beads containing immobilized LP80
(PCBH1), previously stored at 4°C, 5 g CDW ofimmobilized LP80 (pCBHl) was
incubated in MRS broth supplemented with 10.0 mM GDCA and 5.0 mM TDCA. The
concentration of bile acids was monitored by analyzing media samples at regular intervals
over 24 hours. Figure 4.3 shows superimposed HPLC chromatograms ofbile acids in
reaction media taken from one ofthe experiments at Oh, 1h, 2h, 3h, 4h, 5h, and 6h. The
internaI standard was GCA and was the first peak eluted.
Decreasing peak areas ofTDCA and GDCA bile acids indicate BSH activityof
alginate beads containing immobilized LP80 (pCBH1). At time zero an unidentified peak
was detected, just before the measured TDCA peak, and was diminished totally within
four hours (Figure 4.3).
The BSH activity of 0.25 g CDW ofimmobilized LP80 (PCBH1), previously
stored at 4°C, was determined and is shown in Table 4.1. The" BSH activity of 0.26 g
CDW ofimmobilized LP80 (pCBH1) was calculated based on the depletion of 0.2 mmol
of GDCA in a 5h period, and the BSH activity towards TDCA based on the breakdown of
42
0.1 mmol ofTDCA in a 6h period. This calculation was also based on the in-vitro
depletion ofbile acids with 0.25 g CDW LP80 (pCBHl) in 5.0 g alginate beads in a
complex mixture of the bile acids.
Figure 4.4 shows the BSH activity ofimmobilized LP80 (pCBHl) in alginate in
an in-vitro bile acid experiment over a 12 h period. The concentration of GD CA and
TDCA bile acids are shown to decrease over time. Results from Figure 4.4 show that the
BSH activity of immobilized LP80 (pCBH 1) began immediately and depleted GDCA at a
greater initial rate. While TDCA began to breakdown immediately, it did so at a slower
rate than GDCA. The removal of GDCA, however, experienced concentration effects as it
depleted and thus the breakdown of GDCA slowed as the experiment progressed (Fig.
4.4).
To investigate the fate of the products of deconjugation, the above experiment was
performed with a calibration of increasing concentrations ofTDCA, GDCA, and DCA.
Figure 4.5 shows superimposed HPLC chromatograms ofbile acids in MRS reaction
media taken from one of the experiments at Oh, lh, 2h, 3h, 4h, 5h, and 6h. Decreasing
peak areas ofTDCA and GDCA bile acids indicate BSH activity of alginate beads
containing immobilized LP80 (pCBH 1). The peak detected, just before the measured
TDCA peak, was diminished totally within 4 h and corresponds to the calibration peak of
DCA. The internaI standard was GCA and was the first peak eluted. The experiment was
performed in triplicate and the results were averaged.
4.5 Discussion
Bile salt hydrolase (BSH) activity is a common phenomenon in the human gut;
however, Lactobacil/us plantarum 80 (LP80) (pCBHl) used in this study has been
genetically engineered to overproduce the BSH enzyme. Although it has earlier been
shown that the free bacteria was able to break down bile acids in-vitro 29, we intended on
proving the efficacy ofimmobilized LP80 (PCBHl) at breaking down tauro- and glycol
bile acids, and hence establish a basis for their use in deconjugating pathologically high
levels ofbile acids.
43

Results clearly show that immobilized LP80 (PCBH1) was able to effectively
break down the bile acids within six hours (Fig. 4.3) (Fig. 4.4). The BSH activityof
immobilized LP80 (PCBH1) began immediately and depleted GDCA at a greater initial
rate. While TDCA also began to breakdown immediately, it did so at a slower rate than
GDCA. The removal of GDCA, however, experienced concentration effects as it was
depleted. Thus, the breakdown of GDCA slowed as the experiment progressed.
The BSH activity results show that 0.25 g CDW of immobilized LP80 can
breakdown 0.2 mmol of GDCA in a 5h period and 0.1 mmol ofTDCA in a 6h period.
This calculation is based on the in-vitro depletion of bile acids with 0.25 g CDW LP80
(pCBH1) in 5.0 g of alginate beads.
At time zero an unidentified peak was detected (Fig. 4.5), just before the measured
TDCA peak, and was diminished totally within four hours. As depicted in Figure 5.6, the
deconjugation ofTDCA and GDCA lead to the formation of deoxycholic acid (DCA);
thus, it was probable that the unidentified peak was a measure of DCA. To confirm this,
we designed the experiment using a calibration ofincreasing concentrations ofTDCA,
GDCA, and DCA (Fig. 4.5). Results show that indeed the unidentified peak was DCA,
and that DCA was diminished totally within 4 h of the onset of the experiment (Fig. 4.5).
That raised several questions regarding the fate of DCA, the most important of which was
where was the DCA going and why was it not doing so immediately? It is our assumption
that DCA is being consumed or altered by the LP80 (PCBH1) cells and is either bound to
the bacterial membrane or precipitated within the bead. This is based on previous findings
that Lactobacil/us bacteria are able to remove deconjugated bile acids from reaction
media and make them less bioavailable 205.
This in-vitro study shows that immobilized Lactobacil/us plantarum 80 (pCBH 1
can actively break down tauro- and glycol- conjugated bile acids in complex mixtures and
at similar concentrations to human physiological values. The results have shown the
potential for alginate beads, containing immobilized genetically engineered Lactobacillus
plantarum 80 (PCBH1), to mitigate pathologically high levels of bile acids. AIso, is has
given evidence that LP80 (pCBH 1) cells may remove deconjugated bile acids once they
have been produced through BSH activity. However, it should be stated that this in-vitro
study is only suggestive of the values for the in-vivo deconjugation ofbile acids by
44

immobilized LP80 (pCBH 1). Even so, this study has established a basis for the
investigation of the bile acid deconjugation potential of immobilized LP80 (pCBH 1)
when transplanted or administered orally allowing for the safe and effective control of
bile acid levels. The potential uses of immobilized beads containing LP80 (pCBH 1) are
many and inc1ude the removal of unwanted and pathologically high levels of bile acids, in
patients with fulminant hepatic failure (FHF).
4.6 Acknowledgements:
We gratefully acknowledge tinancial support from the Natural Sciences and
Engineering Research Council (NSERC) of Canada.
45

TABLES:
Table 4.1:
Strain
Bile salt hydrolase (BSH) activity (Ilmol DCA/mg CDW-h) of immobilized Lactobacillus plantarum 80 (PCBHl), previously stored at 4 oC, towards glyco- and tauro- bile acids.
BSH activity (Ilmol DCA/mg CDW-h) towards
GDCA TDCA DCA
Immobilized LP80 (pCBHl) 0.17 0.07 0.24
46

FIGURES:
Figure 4.1: Photomicrograph of alginate beads containing immobilized Lactobacillus
plantarum 80 (pCBH1) cells at 175 x magnifications.
1 Coeff. Oet.("'): 0.997829 '" i Coeff. Oet.("'): 0.993246
'" 3.5 -l l 1
1
'" 1 4-0 3.0
1 2.5
'" 3.0
2.0
1.5 2.0
0
1.0
1.0
0.5
0.0
1
2.5 5.0 1.5 10.0 2.5 5.0 1.5 10.0 1
Amoun! 1 Amt. S!d. (mM) Amoun! 1 AmI. S!d. (mM)
Figure 4.2: HPLC calibration curves for GDCA and TDCA measurements.
47

600-
GCA (8.2) GDCA (14.9)
Retention Time (min)
Figure 4.3: Overlaid HPLC chromatograms ofbile acids in reaction media over time
(Oh, lh, 2h, 3h, 4h, 5h, and 6h). Decreasing peak areas ofTDCA and
GDCA indicate BSH activity of immobilized Lactobacillus plantarum 80
(PCBHl).
48

7.00
6.00
~ 5.00
.s "0 4.00 ë::; l'CI
.li! :ë 3.00 .... +--!-_----'\---"-________________ ...........,I __ [GOCA] (mM)
0 r::: 0
-- [TOCA] (mM) ;:;
2.00 i!! ... r::: CIl (,) r::: 1.00 0 0
0.00 0 2 3 4 5 6 7 8 9 10 11 12
Retention Time (h)
Figure 4.4: BSH activity and GDCA and TDCA depletion efficiency of immobilized
Lactobacillus plantarum 80 (PCBHl) in in-vitro experiment. The
concentration of GDCA and TDCA bile acids are shown over time. The
experiment was performed in triplicate: error bars indicate standard
deviations.
49

400 -
i ~ 300 -,
.§. 1
Q) 1/1 C
&. 200
~ ... .s (,,) .2! 100 Q)
C
400
- 300 J!l
1 g: 200 c o Cl. 1/1 Q)
D:: ... 100 .s (,,)
~ c
A
B
Figure 4.5:
GOCA (13.8)
TOCA (11.0) GCA (7.6)
2.5 5.0 7.5 10.0 12.5
Retention Time (Minutes)
GCA (7.7) GOCA (13.6)
TOCA (10.5)
2.5 5.0 7.5 10.0 12.5 15.0
Retention Time (Minutes)
(A) Overlaid HPCL chromatograms of samples (Oh, lh, 2h, 3h, 4h, 5h, 6h)
from an experiment in which immobilized LP80 (pCBH 1) was used to
deconjugate 10 mM GDCA and 5 mM TCDA in MRS reaction media. (D)
Overlaid HPLC chromatograms from a calibration with increasing
concentrations (2 mM, 3 mM, 4 mM, 6 mM, 7 mM, 8 mM, 10 mM) of
TDCA GDCA and DCA. A 4 mM internaI standard was used for the
preparation of aU samples.
50

Taurine
r~ BiI, ,"h H,dml=(BSH)
o + H20 • hydrolysis
o~ 01
A ~/ NH; '\../ ~ o C-OH
Il o + OR
NH,)l OH
H
Glycine
Figure 4.6: Hydrolysis of conjugated bile salts by the Bile Salt Hydrolase (BSH)
enzyme overproduced by genetically engineered Lactobaci/lus plantarum
80 (PCBHl)195. R indicates the amino acid glycine or taurine. RDCA:
glyco- or tauro- deoxycholic acid, DCA: deoxycholic acid.
51
CHAPTER5
ORIGINAL P APER: MICROENCAPSULATED GENETICALLY ENGINEERED
LACTOBACILLUS PLANTARUM 80 (pCBHl) FOR BILE ACID DECONJUGATION
AND IMPLICATION IN LOWERING CHOLESTEROL
MANUSCRIPT SUBMITTED TO JOURNAL OF BIOMEDICINE AND
BIOTECHNOLOGY
Mitchell Lawrence Jones, Hongmei Chen, Wei Ouyang, Terrence Metz, and Satya Prakash *
* Corresponding Author
52
5.1 Abstract
Cholesterol is known to be a major risk factor for coronary heart disease (CHD).
Current treatments for elevated blood cholesterol include dietary management, regular
exercise, and drug therapy with fibrates, bile acid sequestrants, and statins. Such
therapies, however, are often sub-optimal and carry a risk for serious side effects. This
study shows that microencapsulated Lactobacillus plantarum 80 (pCBH 1) can efficiently
break down and remove bile acids and establishes a basis for their use in lowering blood
serum cholesterol. Results show that microencapsulated LP80 (pCBH 1) is able to
effectively break down the conjugated bile acids glycodeoxycholic acid (GDCA) and
taurodeoxycholic acid (TDCA) with bile salt hydrolase (BSH) activities of 0.19 and 0.08
Jlmol DCA/mg CDW lb respectively. This article also summarizes the physiological
interrelationship between bile acids and cholesterol and predicts the oral doses of
microencapsulated Lactobacillus plantarum 80 (pCBH 1) cells required for lowering
cholesterol.
Key words: Artificial cell, microcapsule, cholesterol, coronary heart disease, bile acid,
glycodeoxycholic acid, taurodeoxycholic acid.
5.2 Introduction
Coronary heart disease (CHD) is the main cause of death in Canada, the US and
many other countries around the world6,206. The World Health Organization (WHO)
predicts that by the year 2020, up to 40% of all deaths will be related to cardiovascular
diseases or disease of the heart207. Although cholesterol is an important basic building
block for body tissues, elevated blood cholesterol is a well known major risk factor for
CHD1,2. Recent modalities for lowering blood cholesterollevels involve dietary
management, behavior modification, regular exercise, and drug therapYl,22,22,24.
Pharmacologic agents such as fibrates, nicotinic acid, bile acid sequestrants, and statins
are also available for the treatment ofhigh cholesterol. Although these drugs effectively
53

reduce cholesterol Ievels, they are expensive and are known to have severe side effects20S-
210
Bile salts are the water-soluble end products of cholesterol, and are synthesized in
the liver. During nonnal enterohepatic circulation (EHC), the average bile salt pool of 4.0
g is secreted into the duodenum twice during each meal, or an average of 6-8 times per
day for the purpose offonning mixed micelles with the products oflipid digestion47,4S.
During intestinal transit, 90-95% of secreted bile salts are absorbed in the tenninal ileum
and are retumed to the liver via the portal vein190. The bile salt pool is replenished by
hepatic synthesis of new bile from serum cholesterol. It has been shown that upon
surgical, phannacological or pathological interruption of the EHC, bile salt synthesis is
increased up to 15-fold, leading to an increased demand for cholesterol in the live?9,4s.
Bile acid sequestrants (BAS) are a type of cholesterollowering therapy that
interrupt the ECH and cause lowering ofblood serum cholesterol through de-novo
synthesis of bile acids in the liver. BAS bind bile acids in the intestine and fonn insoluble
complexes that are excreted in the feces. It has been shown that BAS alone can reduce
cholesterol concentrations by 10% to 30%7,50. However, the common BAS
Cholestyramine resin (Locholest, Questran), Colesevelam (We1Chol), and CoIestipoI
(Colestid) are known to exhibit major adverse effects51 .
Certain strains ofbacteria act directly on bile acids in the gastrointestinal (GI)
tract and are beneficial in reducing serum cholesterollevels29,30,32. Control of cholesterol
through oral live bacterial cell therapy, is based on the demonstration that naturally
occurring bacteria such as Lactobacillus acidophilus, Lactobacil/us bulgaricus, and
Lactobacil/us reuteri can significantly lower serum cholesterollevels due BSH
activities29,30,32. De Smet et al. calculated that a daily intake of a realistic amount of
highly BSH active Lactobacil/us cells, in the fonn ofyogurt, might lead to a significant
reduction of cholesterof9. It has also been reported that the oral administration ofthis and
other free bacteria'can reduce serum cholesterolleve1s by 22% to 33%29,30,32. While this
was very promising, severallimiting factors to the oral administration of free bacteria
have been identified. For example, ofthose free bacteria ingested only 1 % survive GI
transit limiting the overall therapeutic effect29. Also, oral administration oflive bacterial
cells can cause a host immune response and can be retained in the intestine replacing the
54

natural intestinal flora32,34. Thus, concems of safety and practicality have prevented the
regular use of this promising therapy in c1inical practice.
Artificial cell microencapsulation is a technique used to encapsulate biologically
active materials in specialized ultra-thin semi-permeable polymer membranes9. The
pol ymer membrane protects encapsulated materials from harsh extemal environments,
while at the same time allowing for the metabolism of selected solutes capable of passing
into and out of the microcapsule. In this manner, the enc10sed material can be retained
insid,e and be separated from the extemal environment, making microencapsulation
particularly useful for biomedical and c1inical applicationsI5-17
,20,99. In the present study
we examine the potential of artificial cell microencapsulated genetically engineered
Lactobacillus plantarum 80 (pCBH 1) cells for bile acids deconjugation to lower
cholesterol.
5.3 Materials and Methods
Media and chemicals
The sodium salts of glycocholic acid (GCA), taurodeoxycholic (TDCA),·
glycodeoxycholic acid (GDCA), and deoxycolic acid (DCA) were supplied by SIGMA
(St. Louis, MO). De Man-Rogosa-Sharpe (MRS) broth was obtained from Difco (Sparks,
MD). The water was purified with an EASYpure™ Reverse Osmosis System and a
NANOpure® Diamond™ Life Science (UVIUF) ultrapure water system from
Bamstead/Thermoline (Dubuque, lA). Methanol was HPLC-gradient from Fisher
Scientific (Fair Lawn, NJ). AlI other chemicals were of analytical grade.
Bacterial strains and growth conditions
The bacterial strain used in this study was the bile salt hydrolytic (BSH) isogenic
Lactobacillus plantarum 80 (pCBHl) strain. Overproduction of the BSH enzyme in LP80
(PCBHl) was obtained as described by Christiaens et aP02. The BSH overproducing
LP80 (PCBHl) strain carries the multicopy plasmid pCBHl carrying the LP80 (PCBHl)
chromosomal bsh gene and an erythromycin resistance gene.
55

The Lactobaci/lus strains were grown in MRS broth at 37°C in a Sanyo MIR -162
bench top incubator. The MRS broth was supplemented with 100 Ilg/ml erythromycin
from FisherBiotech (Fair Lawn, NJ) to select for bacteria carrying the multicopy plasmid
pCBH1.
Microencapsulation of Lactobacillus plantarum 80 (pCBH 1)
50 ml of 1.5% low viscosity alginate (Kelco, Chicago, IL) solution was prepared
and filtered through a 0.22 Ilm Sterivex-GS filter (Millipore, Bedford, MA) into a sterile
60 ml syringe. LP80 (pCBH 1) was grown at 37°C in MRS broth and prepared as a
concentrated microorganism suspension by re-suspension of mi croorgani sm in 10 ml of
sterilized physiologie solution. The 10 ml concentrated microorganism suspension was
added to the 50 mllow viscosity alginate solution and mixed weIl. The
alginate/microorganism mixture was immobilized, through a 300 Ilm nozzle, into a
filtered solution ofCaCh with an Inotech Encapsulator IER-20 (Inotech Biosystems
International Inc., Rockville, MD). The immobilized LP80 (pCBH1) alginate beads were
washed in sterilized physiological solution (8.5 g NaCI/L), placed in a 1 % solution of
poly-L-Iysine from Sigma (St. Louis, MO) for 10 min., washed in physiological solution,
placed in 1 % solution oflow-viscosity alginate for 10 min., and washedin physiological
solution a final time. This procedure was performed in a Microzone Biological
Containment Hood (Microzone Corporation ON, Canada) to assure sterility. The
microencapsulated LP80 (PCBH1) (Figure 5.1) was stored in 1.0 L minimal solution
(10% MRS and 90% physiologic solution) at 4°C to mimic pre sale product storage.
BSH activity of Lactobaci/lus plantarum 80 (PCBH1) microcapsules
To investigate the BSH activity of the microeneapsulated BSH overproducing
LP80 (PCBH1) batch experiments were performed. Five grams ofmicroencapsulated
LP80 (PCBH1) was added to fresh MRS broth to which 10.0 mM GDCA and 5.0 mM
TDCA were added. Samples were taken at regular time intervals during the 12 h
incubation to determine the bile salt concentration in the reaction vessels. The experiment
was performed in triplicate.
56
Bile salt hydrolase assay
A modification of the HPLC-procedure described by Scalial88 was used to
determine BSH activity. Analyses were performed on a reversed-phase C-18 column:
LiChrosorb RP-18, 5 Ilm, 250 x 4.6 mm from HiChrom (Novato, CA). The HPLC system
was made up of two Pro Star 210/215 solvent delivery modules, a Pro Star 320 UV Nis
Detector, a Pro Star 410 AutoSampler, and Star LC Workstation Version 6.0 software was
used. The solvents used were HPLC-grade methanol (solvent A), and solvent B, which
was acetate buffer prepared daily with 0.5 M sodium acetate, adjusted to pH 4.3 with 0-
phosphoric acid, and filtered through a 0.22 Ilm filter (Whatman®, England). An isocratic
elution of 70 per cent solvent A and 30 per cent solvent B was used at a flow rate of 1.0
ml/min at room temperature. An injection loop of 20 III was used, and the detection
occurred at 205 nm within 25 min after injection ofthe bile salt extract.
Quarter ml samples to be analyzed were acidified by the addition of 2.5 III of 6 N
HCI to stop any further enzymatic activity. A modification ofthe extraction procedure
described by Cantafora was used29,187. From the 0.25 ml sample, bile salts were extracted
using a solution of methanol (1: 1; v:v). GCA was added as an internaI standard at 4.0
mM. The samples were mixed vigorously for 10 min and centrifuged at 1000 g for 15
min. The supernatant was then filtered through a 0.22 ilL syringe driven HPLC-filter
(Millipore, Japan) and the sampI es were analyzed directly after filtration.
5.4 Results
Preparation of artificial cell microcapsules containing genetically engineered
Lactobacillus plantarum 80 (PCBBl) cells and determination ofbile acids by BPLC:
Artificial cell microcapsules containing genetically engineered Lactobacillus
plantarum 80 (pCBH1) cells (Fig. 5.1) were prepared using the methods described above
and were stored at 4°C for use in experiments. Sterile conditions and procedures were
strictly adhered to during the process of microencapsulation.
Known quantities of GD CA and TDCA were added to MRS broth and 0.25 mL
sampI es were analyzed using the modified HPLC bile salt hydrolase assay (Fig. 5.2).
57

Using 4.0 mM GCA internaI standard, correlation of detenninant factors (R2) of 0.987599
for GDCA and 0.991610 for TDCA were obtained and used in all experiments.
BSH activity of Lactobaci/lus plantarum 80 (pCBH 1) microcapsules
The BSH activity of microencapsulated LP80 (pCBH 1) cells was detennined to
evaluate the potential for depleting high concentrations ofbile acids. Five grams of
microencapsulated LP80 (pCBH1) was incubated in MRS broth supplemented with 10.0
mM GDCA and 5.0 mM TDCA and sample were analyzed. The concentration ofbile
acids was monitored by analyzing media samples at regular intervals over 12 hours.
Figure 5.2A shows superimposed HPLC chromatograms ofbile acids in reaction media at
Oh, 1h, 2h, 3h, 4h, 5h, and 6h. Decreasing peak areas ofTDCA and GDCA bile acids
indicate BSH activity of LP80 (pCBH1) microcapsules. The BSH activity of
microencapsulated LP80 (PCBH1) towards glyco- and tauro- bile acids was also analyzed
(Table 5.1).
The BSH activity of 0.26 g CDW ofmicroencapsulated LP80 (PCBH1) was
calculated based on the depletion of 0.2 mmol of GDCA in a 4 h period, and the BSH
activity towards TDCA was based on the breakdown of 0.1 mmol ofTDCA in a 5 h
period. AIso, this calculation was based on the in-vitro depletion of bile acids with 0.26 g
CDW LP80 (pCBH1) in 5.0 g alginate microcapsules in a complex mixture ofthe bile
acids. Figure 5.2B shows the BSH activity ofLP80 (PCBH1) microcapsules in the in
vitro bile acid experiment over a 12 h period. The concentration ofGDCA and TDCA
bile acids were found to decrease over time.
Figure 5.2B shows that the BSH activity ofLP80 (PCBH1) began immediately
and depleted GD CA at a greater initial rate. While TDCA also began to breakdown
immediately, it did so at a slower rate than GDCA. The removal of GDCA, however,
experienced concentration effects as it was depleted early and thus the breakdown of
GDCA slowed as the experiment progressed and the BSH activity towards TDCA
increased.
To investigate the fate ofthe products of deconjugation, experiment was
perfonned using a calibration ofincreasing concentrations ofTDCA, GDCA, and DCA.
Figure 5.3A shows superimposed HPLC chromatograms of sampI es at Oh, 1h, 2h, 3h, 4h,
58
5h, and 6h. Decreasing peak areas ofTDCA and GD CA bile acids indicate BSH activity
of microencapsulated LP80 (pCBH 1). We compared these results to earlier studies using
immobilized beads containing LP80 (pCBH1) (Fig. 5.3B). Decreasing peak areas of
TDCA and GDCA bile acids indicate BSH activity of alginate beads containing
immobilized LP80 (PCBH1). The peak detectedjust before the measured TDCA peak
was diminished totally within 4 h and corresponds to the calibration peak of DCA. The
absence of a corresponding peak in the encapsulation results shows the clear advantage of
using encapsulated cells.
5.5 Discussion
Earlier studies have shown that free LP80 (pCBH1) cells can be use to break
down bile acids in-vitro29• We intended on proving the efficacy of the microencapsulated
bacteria at breaking down tauro- and glycol- bile acids, and hence establish a basis for
their use in lowering blood serum cholesterol when administered orally. Results obtained
in this study clearly show that microencapsulated LP80 (PCBH1) was able to effectively
break down physiologically relevant concentrations ofbile acids in-vitro. The BSH
activity results show that 0.26 g CDW ofmicroencapsulated LP80 (pCBH1) can
breakdown 0.2 mmol of GD CA in a 4 h period and 0.1 mmol ofTDCA in a 5 h period
against an average hepatic bile salt secretion of2.0 mmol/4h48,2l1. Thus, an oral
administration ofmicrocapsules, containing 1.85 g CDW ofLP80 (pCBH1), would have
the capacity to completely breakdown the total bile salt secretion in the average human
during a 4 h intestinal transit period. However, breaking down aIl secreted bile salts may
not be the goal oftherapy with microencapsulated LP80 (PCBH1), as sorne bile acids are
required for intestinal absorption of fat through formation of mixed micelles. Even so,
enzymatic breakdown of the bile salt pool in this way would have an impact on serum
cholesterol due to the deconjugation of tauro- and glydo- bile acids and their resulting de
novo synthesis, from serum cholesterol, in the liver (Fig. 5.4A).
In the average human, conjugated bile salts are produced from cholesterol and
taruine or glycine at a rate of 0.02 mmol/h in the liver mmol/h194• During normal EHC,
the average bile salt pool of 4.0 gis secreted into the duodenum twice during each meal,
59
or an average of 6-8 times per day47,48 for lipid digestion (Fig. 5.4B). Daily bile acid
secretions approach 20-30 g47,48 or 20-60 mmol189 sustaining an intestinal bile salt
concentration of 5-20 mM190. During intestinal transit, 90-95% of secreted bile salts are
reabsorbed in the terminal ileum and are retumed to the liver via the portal vein190 (Fig.
5.4B). About 75 per cent of the bile acid secretion is reabsorbed in the conjugated form in
an active sodium-dependent way190. The remaining 25 per cent is hydrolyzed during
intestinal transit and only 15 per cent is reabsorbed in a passive way190 (Fig. 5.4B). Thus,
about 60 per cent of deconjugated bile acids are reabsorbed. Thus, one mmol of
deconjugated bile salt, formed through breakdown by microencapsulated LP80 (pCBH 1),
is responsible for a 0.4 mmol faecal excretion48. It is consequently required for this
amount to be replaced by newly synthesised bile salts from blood serum cholesterol. In
this way, interruption of the ECH can result in an increased bile acid biosynthesis of up to
15-fold, from 0.02 mmol/h to 0.3 mmol/hl94. One may calculate the effects different
dosages of microencapsulated LP80 (pCBH 1) can have on blood serum cholesterollevels
through interruption of the ECH in this way (Fig. 5.5).
Microencapsulated LP80 (PCBH1) was able to deconjugate GDCA and TDCA
completely within 4 h and 5 h respectively (Fig. 5.3A). Earlier, immobilized LP80
(pCBHl) was able to effectivelybreak down GDCA and TDCA bile acids within 5 h and
6 h respectively (Fig. 5.3B). However, the deconjugation product, deoxycholic acid
(DCA), was detected (Fig. 5.3B). This suggests that unlike immobilized cells,
microencapsulated cells diminish the bioavailability ofBSH deconjugated bile acids
totally (Fig 5.4). This finding may improve the therapeutic properties of
microencapsulated LP80 (PCBHI) in several ways. For example, it addresses concems
over the production oflarge amounts of deconjugated bile salts and their association with
an increased risk of developing colon cancer. AIso, if bile salts are actually being
deconjugated, precipitated, and then bound within the microcapsule, microencapsulated
LP80 (PCBH1) maybe capable ofremoving all bile acid from the GI lumen. This effect
contrasts previous results, using free bacteria, where the authors predicted only an
improved clearance (from 95% for conjugated to 60% for deconjugated) ofbile acids
from the ECH and not total clearance29. Further, elevated intraluminal concentrations of
deconjugated bile acids in the colon, normally resulting in an increased secretion of
60

electrolytes and water and causing diarrhea, would cease to present difficulty, as the
deconjugated bile acids would be entirely precipitated and bound within the
microcapsules themselves.
This study has shown that microcapsules containing LP80 (pCBH 1) have several
advantages to the free or immobilized bacteria. Microencapsulation renders the
potentially harmful products of BSH deconjugation, namely DCA, less bioavailable while
at the same time avoiding the problems with oral administration of free bacterial cells.
However, further research is required to substantiate these results, in particular in-vivo
affirmation of the cholesterollowering capacity ofLP80 (pCBH1) is required before
complete potential of this research can be comprehended.
5.6 Acknowledgements:
We gratefully acknowledge financial support from the Natural Sciences and
Engineering Research Council (NSERC) of Canada.
61

TABLES:
Table 5.1: Bile salt hydrolase (BSH) activity (Jlmol DCA/mg CDW-h) of microencapsulated Lactobaci/lus plantarum 80 (pCBH 1) towards glycoand tauro- bile acids.
Strain
Microencapsulated LP80 (pCBH1)
BSH activity (Jlmol DCA/mg CDW-h) towards
GDCA TDCA
0.19 0.08
62
DCA
0.27

FIGURES:
Figure 5.1: (A) Photomicrograph of Lactobacil/us plantarum 80 (PCBH1)
microcapsules at 77 x magnification and (B) at 112 x magnification.
63

600 -
s-C 500-> E -; 400-ln C o Il. ln CI)
0::::
300 -
12.00
GOCA (14.4)
m mm~O~~(11.~) .. :/~ ..
1
i" ,r-~~------------------------------------------~~ 10.00
§. '0 ë:; 8.00 Ils
~ :ci 6.00 .... 0 c 0 .. 4.00 l! -c CI) CJ c 2.00 0 0
0.00
B
1
-[GDCAJ ImM)~ +---~~~-\-~~~~~~~~~~~~~~~~~--I-- rrOCA] (mM) 1
0 2 3 4 5 6 7
Sam pie Time (h)
8 9 10 11 12
Figure 5.2: (A) Overlaid HPLC chromatograms of bile acids over time (Oh, lh, 2h, 3h,
4h, Sh, and 6h). Decreasing peak areas ofTDCA and GDCA indicate BSH
activity of Lactobaci/lus plantarum 80 (pCBHI) microcapsules. (B) BSH
activity and GDCA and TDCA depleting efficiency of Lactobaci/lus
plantarum 80 (PCBHI) microcapsules in in-vitro experiment. The
concentration of GDCA and TDCA bile acids are shown over time.
64

400- 400-
~ 301T ~ 300-'0 '0 > > .§. GDC (14.3) .s GDCA (13.6) CI) CI) : GCA (7.7) t/) t/)
200-; !: 201T1 !: 0 GC (7.9KDC (11.4)
0 Q. i c. t/) t/)
CI) CI)
Q: Q:
... ... 0 0
1001 ... ... 1001 Il Il
1
.! 1 CI)
1 ... CI) CI)
C c
2.5 5.0 7.5 10.0 12.5 15.0 2.5 5.0 7.5 10.0 '12.5 ~~,
15.0
A Peak Time (Minutes) B Peak Time (Minutes)
Figure 5.3: (A) Overlaid HPLC chromatograms ofsamples (Oh, lh, 2h, 3h, 4h, 5h, 6h)
from experiment in which microencapsulated LP80 (pCBHl) was used to
deconjugate 10 mM GDCA and 5 mM TC DA. (B) Overlaid HPCL
chromatograms of samples (Oh, Ih, 2h, 3h, 4h,5h, 6h) from experiment in
which immobilized LP80 (PCBHl) was used to deconjugate 10 mM
GDCA and 5 mM TCDA.
65

A
B
Figure 5.4:
~ Bile Salt Hydrolase (BSH)
c- -NH-R
Il o + H20 ..
hydrolysis
H
20-30 g/day
Taurine
C-OH
Il o + OR
N~ " ~OH Glycine
Bile Salt Pool (4.0 g) Circulated (6 - 8 x/day)
........ ...;::==:;:::::::::~~ 1 10% Fecal Excretion .. (5 g/day)
(A) Hydrolysis of conjugated bile salts by the Bile Salt Hydrolase (BSH)
enzyme overproduced by genetically engineered Lactobacil/us plantarum
80 (PCBHI) 195. R indicates the amino aèid glycine or taurine. RDCA:
glyco- or tauro- deoxycholic acid, DCA: deoxycholic acid. (B)
Enterohepatic circulation ofbile (EHC) 47,48,190,194,211.
66
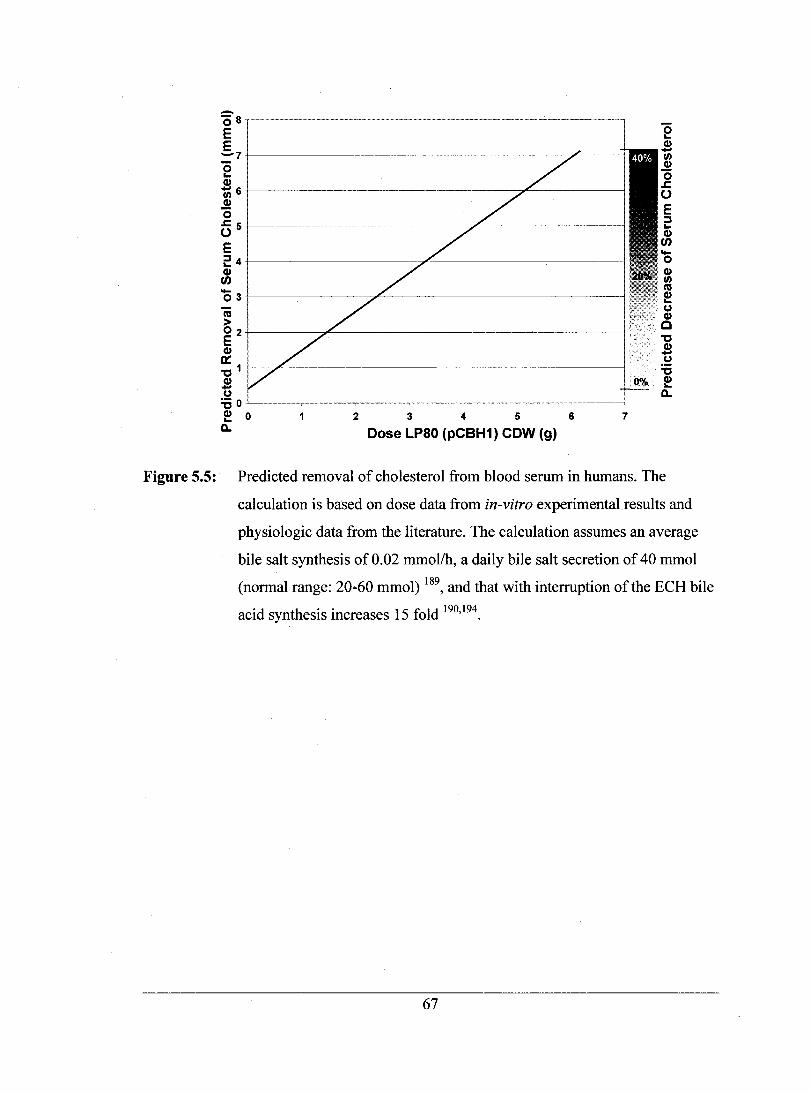
~8,~---···~---_··-~--------·-_·-- ------ -------------------E E ~7~----------------~-------
e CI) 06~------------------~~----------~~--------~ CI)
"0 ~5~------------------------~--------------~
E 24~------------------~---------------------~ CI) en 03~------------~--------------------------~ cu > 02~------~~------------------------------~ E CI)
a: ~1~~~------------------------------------~
S (.)
~o~----~----~----~----~----~----~----~
~ 0 D..
2 3 4 5
Dose LP80 (pCBH1) CDW (9) 6 7
"0 "-CI) -fi) CI)
"0 .r. 0 E ::s "-CI) en 00-0 CI) fi) CU
~ (.) CI)
··0 ~
S .~ ~
0% CI) "-a..
Figure 5.5: Predicted removal of cholesterol from blood serum in humans. The
calculation is based on dose data from in-vitro experimental results and
physiologic data from the literature. The calculation assumes an average
bile salt synthesis of 0.02 mmol/h, a daily bile salt secretion of 40 mmol
(normal range: 20-60 mmol) 189, and that with interruption of the ECH bile
acid synthesis increases 15 fold 190,194.
67

SUPPLIMENTAL INFORMATION:
GDCA TDCA Coeff. Det.(r'): 0.987599 Coeff. Det.(r'): 0.991610
/ 35-'
" / "-, i
/ /
// .J (') 30
1 // ,.j /
/
'" / 3,
,01
i 0
"J '" 21
1 (')
1.0~ 1
1-i
o.sJ
i
li ----_._-, 1 , ,=-_=---"1 1 '2 '3 '4 5 :
Amount 1 AmI. Std. (mmol) Amoun! 1 AmI. S!d. (mmol)
Supplement 5.1: HPLC calibration curves for GD CA and TDCA measurements.
68

CHAPTER6
CONCLUSIONS, SUMMARY, CLAIMS TO THE CONTRIBUTION OF
KNOWLEDGE, AND RECOMMENDATIONS
69

6.1 Summary of observations and recommendations
1. Alginate beads containing genetically engineered Lactobacillus plantarum 80
(PCBH1) cells were found effective in deconjugating glyco- and tauro- conjugated
bile salts in-vitro. The immobilized bacteria had a bile salt hydrolase (BSH) activity
(J..lmol DCA/mg CDW·h) of 0.17 towards glycodeoxycholic acid, 0.07 towards
taurodeoxycholic acid, and 0.24 towards deoxycholic acids overall (Table 4.1).
2. The results c1early show that immobilized LP80 (PCBH1) was able to effectively
break down the bile acids within six hours (Fig. 4.3) (Fig. 4.4). The BSH activity of
immobilized LP80 (pCBH 1) began immediately and depleted ODCA at a greater
initial rate. While TDCA also began to breakdown immediately, it did so at a slower
rate than ODCA. The removal of ODCA, however, experienced concentration effects
as it was depleted. Thus, the breakdown of ODCA slowed as the experiment
progressed.
3. With immobilized LP80 (PCBH1) an unidentified peak was detected (Fig. 4.5), just
before the measured TDCA peak, and was diminished totally within four hours. As
depicted in Figure 4.6, the deconjugation ofTDCA and ODCA lead to the formation
of deoxycholic acid (DCA); thus, it was probable that the unidentified peak was a
measure of DCA. To confirm this, we designed the experiment using a calibration of
increasing concentrations ofTDCA, ODCA, and DCA (Fig. 4.5). Results showed that
indeed the unidentified peak was DCA, and that DCA was diminished totally within 4
h ofthe onset of the experiment (Fig. 4.5).
4. Aiginate-polylysine-aiginate microcapsules containing genetically engineered
Lactobacillus plantarum 80 (pCBH1) cells were found effective in deconjugating
glyco- and tauro- conjugated bile salts in-vitro. The artificial cells had a bile salt
hydrolase (BSH) activity (J..lmol DCA/mg CDW·h) 0.19 towards glycodeoxycholic
acids, 0.08 towards taurodeoxycholic acids, and 0.27 towards deoxycholic acid
overall (Table 5.1).
70
5. Microencapsulated LP80 (pCBH1) was able to deconjugate ODCA and TDCA
completely within 4 h and 5 h respectively (Fig. 5.3A). Earlier, immobilized LP80
(PCBH1) was able to effectivelybreak down ODCA and TDCA bile acids within 5 h
and 6 h respectively (Fig. 5.3B). However, the deconjugation product, deoxycholic
acid (DCA), was detected (Fig. 5.3B). This suggests that unlike immobilized cells,
microencapsulated cells diminish the bioavailability of BSH deconjugated bile acids
totally (Fig 5.4).
6. The predicted removal of cholesterol from blood serum in humans was calculated
based on dose data from in-vitro experimental results and physiologic data from the
literature and the results were charted. The calculation assumes an average bile salt
synthesis of 0.02 mmol/h, a daily bile salt secretion of 40 mmol (normal range: 20-60
mmol), and that with interruption of the ECH bile acid synthesis increases 15 fold
(Fig. 5.5).
7. Patients would benefit from an effective and safe system for the removal of excess
bile aicds, as elevated intraluminal concentrations of deconjugated bile acids in the
colon normally result in an increased secretion of electrolytes and water causing
diarrhea194• The oral administration ofmicroencapsulated LP80 (PCBH1) bacteria
would deconjugate, precipitate, and then bind conjugated bile acids within the
microcapsules thus mitigating problems associated with excessive electrolyte and
water secretion and the resulting diarrhea.
8. It is believed that thirty percent of all colon cancer deaths can be linked to diet212. One
proposed mechanism for this close association is that a high fat diet leads to an
increased secretion of primary bile salts into the small intestine, where the indigenous
microflora deconjugates the primary bile acids. The increased bileary secretion leads
to the formation ofhigher levels of deconjugated bile acids that may then exert their
cytotoxic and mutagenic effect on the gastrointestinal mucosa197. It is these
conjugated bile salts which have been incriminated in colonie carcinogenesis and thus
71

a system for their removal would be a valuable tool for the prevention of colon
cancer. Treatment with microencapsulated LP80 (PCBH1) would allow for the
removal ofunwanted and potentially harmful deconjugated bile acids and provide a
safe and effective means for patients and public to prevent this deadly disease.
9. Urinary levels of sulfated bile acids are known to be significantly elevated in liver
disease and hepatobiliary disease213 . Several research groups have directed their
efforts towards detection of these levels because urinary analysis is noninvasive, and
urinary levels of sulfated bile acids are thought to be useful as an index ofliver
function and an indicator ofhepatobilary disease191 . A diagnostic strip containing
immobilized beads and/or microcapsules containing LP80 (pCBH 1), as weIl as a
coloured detector molecule, could be used as a novel noninvasive diagnostic tool for
liver function and hepatobiliary diseases in urine.
10. It is weIl known that the bioartificialliver (BAL) must provide both synthetic and
detoxifying functions 192,193 normally performed by the liver. Several groups have
developed a BAL consisting of isolated porcine214,21 5 or bovine hepatocytes in a
hoIlow-fiber bioreactor. Recently, researchers have focused on the use of BAL to
support patients with fulminant hepatic failure (FHF), in which impaired liver
function is associated with pathologically elevated levels of bile acids. In this case an
effective BAL requires the ability to remove and process a significant quantity of
deconjugated bile acid. Incorporation of immobilized beads and/or microcapsules
containing LP80 (PCBH1) could be used for the removal ofunwanted and
pathologically high levels of bile acids if incorporated into a bioartificialliver.
6.2 Conclusions
In the present project we proposed a treatment modality based on the use of
artificial cell microcapsules containing Lactobacillus plantarum 80 (pCBH 1) and planned
to test the efficacy of such microcapsules in-vitro. Our hypothesis was that a therapeutic
of alginate-polylysine-alginate artificial cells, containing the genetically engineered
72
organism, would take advantage of inherent cholesterol-Iowering properties ofthe
bacteria and at the same time circumvent to a large extent associated problems related
with their use. The project was undertaken, therefore, to prove the above hypothesis
through our proposed research objectives. Our research objectives were to design a
reliable assay for bile acid identification and quantification, design immobilized beads
and artificial cell microcapsules containing live Lactobacil/us plantarum 80 (pCBH 1)
cells and study their ability to hydrolyze bile salts in-vitro in flask, and ca1culate the
potential for microencapsulated LP80 (PCBH1) to lower serum cholesterollevels through
interruption ofthe EHC of bile salts.
After reviewing the results obtained the following conclusions can be made:
1. A novel formulation of alginate beads or alginate-polylysine-alginate microcapsules,
containing Lactobacillus plantarum 80 (pCBH 1), has been proposed and its potential
efficacy for several biomedical applications has been demonstrated.
2. Microcapsules containing LP80 (pCBH 1) have several advantages to the free or
immobilized bacteria. Microencapsulation renders the potentially harmful products of
BSH deconjugation, namely DCA, less bioavailable while at the same time avoiding
the problems with oral administration of free bacterial cells. Further research is,
however, required to substantiate these results, in particular in-vivo affirmation of the
cholesterollowering capacity ofLP80 (pCBH1) is required before complete potential
of this research can be comprehended.
3. This study confirms the lab scale feasibility of the approach in-vitro and provides a
starting point for future simulated gastrointestinal in-vitro work and in-vivo studies
aimed at proving the efficacy of this potential therapeutic.
73

References
1. Ridker,P .M. Evaluating novel cardiovascular risk factors: can we better predict heart attacks? Ann. Intern. Med. 130, 933-937 (1999).
2. Tall,A.R. Plasma high density lipoproteins. Metabolism and relationship to atherogenesis. J. Clin. Invest 86,379-384 (1990).
3. Executive Summary of The Third Report of The National Cholesterol Education Pro gram (NCEP) Expert Panel on Detection, Evaluation, And Treatment ofHigh Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 285, 2486-2497 (2001).
4. Lousberg,T.R., Denham,A.M., & Rasmussen,J.R. A comparison of clinical outcome studies among cholesterol-Iowering agents. Ann. Pharmacother. 35, 1599-1607 (2001).
5. National Cholesterol Education Program. Second Report of the Expert Panel on Detection, Evaluation, and Treatment ofHigh Blood Cholesterol in Adults (Adult Treatment Panel II). Circulation 89, 1333-1445 (1994).
6. The Heart and Stroke Foundation of Canada. The Changing Face of Heart Disease and Stroke in Canada. 2000.
Ref Type: Report
7. The Lipid Research Clinics Coronary Primary Prevention Trial results. 1. Reduction in incidence of coronary heart disease. JAMA 251, 351-364 (1984).
8. Chang,T.M.S. Semipermeable microcapsules. Science 146, 524-525 (1964).
9. Chang,T.M. & Prakash,S. Artificial cells for bioencapsulation of cells and genetically engineered E. coli. For cell therapy, gene therapy, and removal ofurea and ammonia. Methods Mol. Biol. 63,343-358 (1997).
10. Sefton,M.V., May,M.H., Lahooti,S., & Babensee,J.E. Making microencapsulation work: conformaI coating, immobilization gels and in vivo performance. J. Control Release 65, 173-186 (2000).
11. Chang,P.L., Van Raamsdonk,J.M., Hortelano,G., Barsoum,S.C., MacDonald,N.C., & Stockley,T.L. The in vivo delivery ofheterologous proteins by microencapsulated recombinant cells. Trends Biotechnol. 17, 78-83 (1999).
12. Chang,P.L. Encapsulation for somatic gene therapy. Ann. N. Y. Acad. Sei. 875, 146-158 (1999).
13. Quong,D. & Neufeld,RJ. DNA encapsulation within co-guanidine membrane coated alginate beads and protection from extracapsular nuclease. J. Microencapsul. 16, 573-585 (1999).
74
14. Siebers,U., Horcher,A., Bretze1,R.G., Federlin,K., & Zekom,T. Aiginate-based microcapsules for immunoprotected islet transplantation. Ann. N. Y. Acad. Sei. 831,304-312 (1997).
15. Prakash,S. & Chang,T.M. Microencapsulated genetically engineered live E. coli DH5 cells administered orally to maintain normal plasma urea leve1 in uremic rats. Nat. Med. 2, 883-887 (1996).
16. Prakash,S. & Chang,T.M. In vitro and in vivo uric acid lowering by artificial cells containing microencapsulated genetically engineered E. coli DH5 cells. Int. J. Artif. Organs 23, 429-435 (2000).
17. Prakash,S. & Chang,T.M. Growth kinetics of genetically engineered E. coli DH 5 cells in artificial cell AP A membrane microcapsules: preliminary report. Artif. CeUs Blood Substit. Immobil. Biotechnol. 27,291-301 (1999).
18. Chang,T.M. & Prakash,S. Therapeutic uses ofmicroencapsulated genetically engineered cells. Mol. Med. Today 4,221-227 (1998).
19. Chang,T.M. & Prakash,S. Procedures for microencapsulation of enzymes, cells and genetically engineered microorganisms. Mol. Biotechnol. 17,249-260 (2001).
20. Prakash,S. & Chang,T.M. Artificial cell microcapsules containing genetically engineered E. coli DH5 cells for in-vitro lowering of plasma potassium, phosphate, magnesium, sodium, chloride, uric acid, cholesterol, and creatinine: a pre1iminary report. Artif. CeUs Blood Substit. Immobil. Biotechnol. 27,475-481 (1999).
21. Lichtenstein,A.H. Effects of diet and exercise on cholesterollevels. N. Engl. J. Med. 339, 1552-1553 (1998).
22. Omish,D. & Denke,M. Dietary treatment ofhyperlipidemia. J. Cardiovasc. Risk 1,283-286 (1994).
23. Omish,D., Scherwitz,L.W., Billings,J.H., Brown,S.E., Gould,K.L., Merritt,T.A., Sparler,S., Armstrong,W.T., Ports,T.A., Kirkeeide,R.L., Hogeboom,C., & Brand,R.J. Intensive lifestyle changes for reversaI of coronary heart disease. JAMA 280, 2001-2007 (1998).
24. Dunn-Emke,S., Weidner,G., & Omish,D. Benefits of a low-fat plant-based diet. Obes. Res. 9, 731 (2001).
25. Attanasio,E., Russo,P., & Allen,S.E. Cost-minimization analysis of simvastatin versus atorvastatin for maintenance therapy in patients with coronary or peripheral vascular disease. Clin. Ther. 23,276-283 (2001).
75

26. Hodgson,T.A. & Cohen,AJ. Medical care expenditures for selected circulatory diseases: opportunities for reducing national health expenditures. Med. Care 37, 994-1012 (1999).
27. Prosser,L.A., Stinnett,A.A., Goldman,P.A., Williams,L.W., Hunink,M.G., Goldman,L., & Weinstein,M.C. Cost-effectiveness of cholesterol-Iowering therapies according to selected patient characteristics. Ann. Intern. Med. 132, 769-779 (2000).
28. Reckless,J.P. Economic issues in coronary heart disease prevention. Curr. Opin. Lipidol. 7,356-362 (1996).
29. De,S., l, Van Hoorde,L., De Saeyer,M., Vande,W.M.,& Verstraete,W. In vitro study ofbile salt hydrolase (bsh) activity ofbsh isogenic lactobacillus plantarum 80 strains an destimation of cholesterollowering through enhanced bsh activity. Microbial ecology in health and disease 7, 315-329 (1994).
30. Anderson,J.W. & Gilliland,S.E. Effect offermented milk (yogurt) containing Lactobacillus acidophilus LIon serum cholesterol in hypercholesterolemic humans. J. Am. Coll. Nutr. 18, 43-50 (1999).
31. Schaafsma,G., Meuling,WJ., van Dokkum,W., & Bouley,C. Effects ofa milk product, fermented by Lactobacillus acidophilus and with fructo-oligosaccharides added, on blood lipids in male volunteers. Eur. J. Clin. Nutr. 52, 436-440 (1998).
32. Taranto,M.P., Medici,M., Perdigon,G., Ruiz Holgado,A.P., & Valdez,G.F. Effect of Lactobacillus reuteri on the prevention ofhypercholesterolemia in mice. J. Dairy Sei. 83,401-403 (2000).
33. Usman & Hosono,A. Effect of administration of Lactobacillus gasseri on serum lipids and fecal steroids in hypercholesterolemic rats. J. Dairy Sei. 83, 1705-1711 (2000).
34. Chin,J., Tumer,B., Barchia,L, & Mullbacher,A. Immune response to orally consumed antigens and probiotic bacteria. Immunol. Cell Biol. 78, 55-66 (2000).
35. Ishibashi,N. & Yamazaki,S. Probiotics and safety. Am. J. Clin. Nutr. 73, 465S-470S (2001).
36. Oggioni,M.R., Manganelli,R., Contomi,M., Tommasino,M., & Pozzi,G. Immunization ofMice by Oral Colonization with Live Recombinant Commensal Streptococci. Vaceine 13, 775-779 (1995).
37. Wadolkowski,E.A., Laux,D.C., & Cohen,P.S. Colonization of the StreptomycinTreated Mouse Large-Intestine by A Human Fecal Escherichia-Coli Strain - Role of Adhesion to Mucosai Receptors. Infection and Immunity 56, 1036-1043 (1988).
76

38. Salminen,S., von Wright,A., Morelli,L., Marteau,P., Brassart,D., de Vos,W.M., Fonden,R., Saxelin,M., Collins,K., Mogensen,G., Birkeland,S.E., & MattilaSandholm,T. Demonstration ofsafety ofprobiotics -- a review. Int. J. Food Microbiol. 44, 93-106 (1998).
39. Tanne,D., Koren-Morag,N., Graff,E., & Goldbourt,U. Blood lipids and first-ever ischemic stroke/transient ischemic attack in the Bezafibrate Infarction Prevention (BIP) Registry: high triglycerides constitute an independent risk factor. Circulation 104,2892-2897 (2001).
40. American Heart Association. Heart Disease and Stroke Statistics - 2002 Update. 2002. Dalas Texas.
Ref Type: Report
41. Criqui,M.H. Very low cholesterol and cholesterollowering. A statement for healthcare professionals from the American Heart Association Task Force on Cholesterol Issues. Circulation 90, 2591 (1994).
42. Hulley,S.B., Newman,T.B., & Jacobs,D.R. Toward a more balanced cholesterol policy. Circulation 90, 2570-2572 (1994).
43. Grundy,S.M. United States Cholesterol Guidelines 2001: expanded scope of intensive low-density lipoprotein-Iowering therapy. Am. J. Cardiol. 88, 23J-27J (2001).
44. Rosenson,R.S. The rationale for combination therapy. Am. J. Cardiol. 90,2K-7K (2002).
45. Grundy,S.M. Approach to lipoprotein management in 2001 National Cholesterol Guidelines. Am. J. Cardiol. 90, l1i-21i (2002).
46. Talbert,R.L. New therapeutic options in the National Cholesterol Education Program Adult Treatment Panel III. Am. J. Manag. Care 8, S301-S307 (2002).
47. Binder Henry J. in Principles of Intemal Medicine, Edn. 15th. eds. Braunwald, Fauchi, Kasper, Hauser, Longo, & Jameson 1667-1678 (McGraw-Hill,2001).
48. Hofinann,A.F. CUITent concepts ofbiliary secretion. Dig. Dis. Sei. 34, 16S-20S (1989).
49. Hofinann,A.F. in Handbook ofPhysiology. Gastrointestinal system, Vol. IV 567-596 (American Physiological Society, Bethesda; 1989).
50. Levine,G.N., Keaney,J.F., Jr., & Vita,J.A. Cholesterol reduction in cardiovascular disease. Clinical benefits and possible mechanisms. N Engl. J. Med. 332,512-521 (1995).
77
51. Bristol-Myers Squibb. 1995 In Review: Worldwide Consumer Medicines. 1995. Company Annual Report. Online: http://www.bms.comlstatic/annual/95annuldata/cp95me.html.
Ref Type: Report
52. Chang,T.M.S. in Encyclopedia of Human Biology 457-463 (1997).
53. Quong,D. & Neufeld,RJ. DNA protection from extracapsular nucleases, within chitosan- or poly-L-lysine-coated alginate beads. Biotechnol. Bioeng. 60, 124-134 (1998).
54. Uludag,H., De Vos,P., & Tresco,P.A. Technology ofmammalian cell encapsulation. Adv. Drug Deliv. Rev. 42, 29-64 (2000).
55. Chang, T. M. S. and Prakash, S. Microencapsulated genetically engineered microorganisms for clinical application. [6,217,859].4-17-2001. U.S. 7-31-1997.
RefType: Patent
56. Prakash, S. and Jones M.L. Engineering Artificial Cells for Therapy. 7-22-2002. Sarawak, Malaysia, 2nd World Engineering Congress.
Ref Type: Conference Proceeding
57. Hara,H., Haga,S., Kasai,T., & Kiriyama,S. Fermentation products ofsugar-beet fiber by cecal bacteria lower plasma cholesterol concentration in rats. J. Nutr. 128, 688-693 (1998).
58. Li,L., Baumann,C.A., Meling,D.D., Sell,J.L., & Beitz,D.C. Effect oforally administered Eubacterium coprostanoligenes A TCC 51222 on plasma cholesterol concentration in laying hens. Pou/t. Sei. 75, 743-745 (1996).
59. Kikuchi-Hayakawa,H., Shibahara-Sone,H., Osada,K., Onodera-Masuoka,N., Ishikawa,F., & Watanuki,M. Lowerplasma triglyceride level in Syrian hamsters fed on skim milk fermented with Lactobacillus casei strain Shirota. Biosei. Biotechnol. Biochem. 64,466-475 (2000).
60. De Rodas,B.Z., Gilliland,S.E., & Maxwell,C.V. Hypocholesterolemic action of Lactobacillus acidophilus ATCC 43121 and calcium in swine with hypercholesterolemia induced by diet. J. Dairy Sei. 79,2121-2128 (1996).
61. Fukushima,M., Yamada,A., Endo,T., & Nakano,M. Effects of a mixture of organisms, Lactobacillus acidophilus or Streptococcus faecalis on delta6-desaturase activity in the livers ofrats fed a fat- and cholesterol-enriched diet. Nutrition 15, 373-378 (1999).
62. Fukushima,M. & Nakano,M. Effects of a mixture of organisms, Lactobacillus acidophilus or Streptococcus faecalis on cholesterol metabolism in rats fed on a fat- and cholesterol-enriched diet. Br. J. Nutr. 76,857-867 (1996).
78
63. Molin,G., Andersson,R., Ahrne,S., Lonner,C., Marklinder,l., Johansson,M.L., Jeppsson,B., & Bengmark,S. Effect of fennented oatmeal soup on the cholesterol level and the Lactobacillus colonization of rat intestinal mucosa. Antonie Van Leeuwenhoek 61, 167-173 (1992).
64. De,S., I, De Boever,P., & Verstraete,W. Cholesterollowering in pigs through enhanced bacterial bile salt hydrolase activity. Br. J Nutr. 79, 185-194 (1998).
65. Agerholm-Larsen,L., Bell,M.L., Grunwald,G.K., & Astrup,A. The effect of a probiotic milk product on plasma cholesterol: a meta-analysis of short-tenn intervention studies. Eur. J Clin. Nutr. 54, 856-860 (2000).
66. Borody, D. a. T. J. Treatment of gastro-intestinal disorders with a fecal composition or a composition ofbacteroides and E. coli. [5,443,826].1995. U.S.
Ref Type: Patent
67. Hilton,E., Kolakowski,P., Singer,C., & Smith,M. Efficacy of Lactobacillus GG as a Diarrheal Preventive in Travelers. J. Travel. Med. 4, 41-43 (1997).
68. Kaila,M., Isolauri,E., Soppi,E., Virtanen,E., Laine,S., & Arvilommi,H. Enhancement of the circulating antibody secreting cell response in human diarrhea by a human Lactobacillus strain. Pediatr. Res. 32, 141-144 (1992).
69. Majamaa,H., Isolauri,E., Saxelin,M., & Vesikari,T. Lactic acid bacteria in the treatment of acute rotavirus gastroenteritis. J. Pediatr. Gastroenterol. Nutr. 20, 333-338 (1995).
70. Oberhelman,R.A., Gilman,R.H., Sheen,P., Taylor,D.N., Black,R.E., Cabrera,L., Lescano,A.G., Meza,R., & Madico,G. A placebo-controlled trial of Lactobacillus GG to prevent diarrhea in undernourished Peruvian children. J. Pediatr. 134, 15-20 (1999).
71. Phuapradit,P., Varavithya,W., Vathanophas,K., Sangchai,R., Podhipak,A., Suthutvoravut,U., Nopchinda,S., Chantraruksa,V., & Haschke,F. Reduction of rotavirus infection in children receiving bifidobacteria-supplemented fonnula. J Med. Assoc. Thai. 82 Suppl 1, S43-S48 (1999).
72. Raza,S., Graham,S.M., Allen,S.J., Sultana,S., Cuevas,L., & Hart,C.A. Lactobacillus GG promotes recovery from acute nonbloody diarrhea in Pakistan. Pediatr. Infect. Dis. J. 14, 107-111 (1995).
73. Raza,S., Graham,S.M., Allen,S.J., Sultana,S., Cuevas,L., Hart,C.A., Kaila,M., Isolauri,E., Saxelin,M., Arvilommi,H., & . Lactobacillus GG in acute diarrhea. Indian Pediatr. 32, 1140-1142 (1995).
74. Saavedra,J.M., Bauman,N.A., Oung,l., Pennan,J.A., & Yolken,R.H. Feeding of Bifidobacterium bifidum and Streptococcus thennophilus to infants in hospital for prevention of di arrhoea and shedding of rotavirus. Lancet 344, 1046-1049 (1994).
79
75. Saavedra,J.M. Microbes to fight microbes: a not so novel approach to controlling diarrheal disease. J. Pediatr. Gastroenterol. Nutr. 21, 125-129 (1995).
76. Shomikova,A.V., Casas,I.A., Mykkanen,H., Salo,E., & Vesikari,T. Bacteriotherapy with Lactobacillus reuteri in rotavirus gastroenteritis. Pediatr. Infeet. Dis. J. 16, 1103-1107 (1997).
77. Shomikova,A.V., Isolauri,E., Burkanova,L., Lukovnikova,S., & Vesikari,T. A trial in the Karelian Republic of oral rehydration and Lactobacillus GG for treatment of acute diarrhoea. Aeta Paediatr. 86, 460-465 (1997).
78. Siitonen,S., Vapaatalo,H., Salminen,S., Gordin,A., Saxelin,M., Wikberg,R., & Kirkkola,A.L. Effect of Lactobacillus GG yoghurt in prevention of antibiotic associated diarrhoea. Ann. Med. 22, 57-59 (1990).
79. Arvola,T., Laiho,K., Torkkeli,S., Mykkanen,H., Salminen,S., Maunula,L., & Isolauri,E. Prophylactic Lactobacillus GG reduces antibiotic-associated diarrhea in children with respiratory infections: a randomized study. Pediatries 104, 'e64 (1999).
80. Bellomo,G., Mangiagle,A., Nicastro,L., & Frigerio,G. A controlled double-blind study of SF68 strain as a new biological preparation for the treatment of diarrhea in pediatrics. Curr. Therap. Res. 28, 927-936 (1980).
81. Isolauri,E., Juntunen,M., Rautanen,T., Sillanaukee,P., & Koivula,T. A Human Lactobacillus Strain (Lactobacillus-Casei Sp Strain Gg) Promotes Recovery from Acute Diarrhea in Children. Pediatries 88, 90-97 (1991).
82. Akiyama,K.e.a. Effects of oral administration of Bifidobaeterium breve on development of intestinal microflora in extremely premature infants. Aeta Neonatol. Japan 30, 130-137 (1994).
83. Hirayama,K. & Rafter,J. The role oflactic acid bacteria in colon cancer prevention: mechanistic considerations. Antonie Van Leeuwenhoek 76, 391-394 (1999).
84. McIntosh,G.H., Royle,P.1., & Playne,M.J. A probiotic strain of 1. acidophilus reduces DMH-induced large intestinal tumors in male Sprague-Dawley rats. Nutr. Cancer 35, 153-159 (1999).
85. Singh,J., Rivenson,A., Tomita,M., Shimamura,S., Ishibashi,N., & Reddy,B.S. Bifidobacterium longum, a lactic acid-producing intestinal bacterium inhibits colon cancer and modulates the intermediate biomarkers of colon carcinogenesis. Careinogenesis 18, 833-841 (1997).
86. Malin,M., Isolauri,E., Pikkarainen,P., Karikoski,R., & Isolauri,J. Enhanced absorption of macromolecules. A secondary factor in Crohn's disease. Dig. Dis. Sei. 41, 1423-1428 (1996).
80

87. Michetti,P., Dorta,G., Wiesel,P.H., Brassart,D., Verdu,E., Herranz,M., Felley,C., Porta,N., Rouvet,M., Blum,A.L., & Corthesy-Theulaz,1. Effect ofwhey-based culture supernatant of Lactobacillus acidophilus (johnsonii) LaI on Helicobacter pylori infection in humans. Digestion 60, 203-209 (1999).
88. Layer,P. & Keller,J. Lipase supplementation therapy: standards, alternatives, and perspectives. Pancreas 26, 1-7 (2003).
89. Raimondo,M. & DiMagno,E.P. Lipolytic activity ofbacteriallipase survives better than that of porcine lipase in human gastric and duodenal content. Gastroenterology 107, 231-235 (1994).
90. Matsuzaki,T. & Chin,J. Modulating immune responses with probiotic bacteria. lmmunol. Cel! Biol. 78, 67-73 (2000).
91. Pelto,L., Isolauri,E., Lilius,E.M., Nuutila,J., & Salminen,S. Probiotic bacteria down-regulate the milk-induced inflammatory response in milk-hypersensitive subjects but have an immunostimulatory effect in healthy subjects. Clin. Exp. Al!ergy 28, 1474-1479 (1998).
92. Link-Amster,H., Rochat,F., Saudan,K.Y., Mignot,O., & Aeschlimann,J.M. Modulation of a specific humoral immune response and changes in intestinal flora mediated through fermented milk intake. FEMS lmmunol. Med. Microbiol. 10,55-63 (1994).
93. Schiffrin,E.J., Rochat,F., Link-Amster,H., Aeschlimann,J.M., & DonnetHughes,A. Immunomodulation ofhuman blood cells following the ingestion of lactic acid bacteria. J. Dairy Sei. 78,491-497 (1995).
94. Simenhoff,M.L., Dunn,S.R., Zollner,G.P., Fitzpatrick,M.E., Emery,S.M., Sandine,W.E., & Ayres,J.W. Biomodulation ofthe toxic and nutritional effects of small bowel bacterial overgrowth in end-stage kidney disease using freeze-dried Lactobacillus acidophilus. Miner. Electrolyte Metab 22,92-96 (1996).
95. Hida,M., Aiba,Y., Sawamura,S., Suzuki,N., Satoh,T., & Koga,Y. Inhibition ofthe accumulation ofuremic toxins in the blood and their precursors in the feces after oral administration of Lebenin, a lactic acid bacteria preparation, to uremic patients undergoing hemodialysis. Nephron 74, 349-355 (1996).
96. Campieri,C., Campieri,M., Bertuzzi,V., Swennen,E., Matteuzzi,D., Stefoni,S., Pirovano,F., Centi,C., Ulisse,S., Famularo,G., & De Simone,C. Reduction of oxaluria after an oral course of lactic acid bacteria at high concentration. Kidney lnt. 60, 1097-1105 (2001).
97. Hokama,S., Honma,Y., Toma,C., & Ogawa,Y. Oxalate-degrading Enterococcus faecalis. Microbiol.lmmunol. 44,235-240 (2000).
81

98. Lim,F. & Sun;A.M. Microencapsulated islets as bioartificial endocrine pancreas. Science 210, 908-910 (1980).
99. Prakash,S. & Chang,T.M. Microencapsulated genetically engineered E. coli DH5 cells for plasma urea and ammonia removal based on: 1. Column bioreactor and 2. Oral administration in uremic rats. Artif. Cells Blood Substit. Immobil. Biotechnol. 24,201-218 (1996).
100. Chang,T.M. Future prospects for artificial blood. Trends Biotechnol. 17,61-67 (1999).
101. Ross,C.J., Ralph,M., & Chang,P.L. Delivery of recombinant gene products to the central nervous system with nonautologous cells in alginate microcapsules. Hum. Gene Ther. 10,49-59 (1999).
102. Batich, C. and Vaghefi, F. Process for microencapsulating cells. [6,242,230].6-5-2001. D.S. 11-18-1999.
RefType: Patent
103. Duncan,S.H., Richardson,A.J., Kaul,P., Holmes,R.P., Allison,M.J., & Stewart,C.S. Oxalobacter formigenes and its potential role in human health. Appl. Environ. Microbiol. 68,3841-3847 (2002).
104. Jones, M. L., Chen, H., Ouyang, W., Metz, T., and Prakash, S. Deconjugation of Bile Acids with Immobilized Genetically Engineered Lactobacillus Plantarum 80 (PCBH1). Cell Transplantation. 3-2-2003.
Ref Type: Abstract
105. Favaro-Trindade,C.S. & Grosso,C.R. Microencapsulation of L. acidophilus (La-05) and B. lactis (Bb-12) and evaluation of their survival at the pH values of the stomach and in bile. J. Microencapsul. 19,485-494 (2002).
106. Kailasapathy,K. Microencapsulation of probiotic bacteria: technology and potential applications. Curr. Issues Intest. Microbiol. 3,39-48 (2002).
107. O'Riordan,K., Andrews,D., Buckle,K., & Conway,P. Evaluation of microencapsulation of a Bifidobacterium strain with starch as an approach to prolonging viability during storage. J. Appl. Microbiol. 91, 1059-1066 (2001).
108. Sultana,K., Godward,G., Reynolds,N., Arumugaswamy,R., Peiris,P., & Kailasapathy,K. Encapsulation of probiotic bacteria with alginate-starch and evaluation of survival in simulated gastrointestinal conditions and in yoghurt. Int. J. Food Microbiol. 62,47-55 (2000).
109. Saarela,M., Mogensen,G., Fonden,R., Matto,J., & Mattila-Sandholm,T. Probiotic bacteria: safety, functional and technological properties. J. Biotechnol. 84, 197-215 (2000).
82
110. Chang, T. M. S, Bourget, L., and Lister, C. Mierocapsule for the removal of specifie ami no acids through the entero-portal recirculation. [5,147,641].10-15-1991. U.S. 6-24-1991.
Ref Type: Patent
111. Kayar, S. R. and Axley, M. J. Accelerated gas removal from divers' tissues utilizing gas metabolizing baeteria. [5,922,317]. 7-13-1997. U.S. 5-6-1997.
RefType: Patent
112. Rao,A.V., Shiwnarain,N., & Maharaj,I. SurvivalofMicroencapsulated Bifidobaeterium-Pseudolongum in Simulated Gastric and Intestinal Juiees. Canadian Institute of Food Science and Technology Journal 22, 345-349 (1989).
113. Sun,W. & Griffiths,M.W. Survival ofbifidobacteria in yogurt and simulated gastric juice following immobilization in gellan-xanthan beads. Int. J Food Microbiol. 61, 17-25 (2000).
114. Modler,H.W. & Vila-Gracia,L. The growth ofBifidobacterium longum in wheybased medium and viability ofthis organism in frozen yogurt with ow and high levels of developed acidity. Cult. Dairy Prod. 28, 4-8 (1993).
115. Audet,P., Paguin,C., & Lacroix,C. Effect of Medium and Temperature ofStorage on Viability of Lactic-Acid Bacteria Immobilized in Kappa-Carrageenan-Loeust Bean Gum Gel Beads. Biotechnology Techniques 5, 307-312 (1991).
116. Truelstrup,H.L., Allan-Wojtas,P.M., Jin,Y.L., & Paulson,A.T. Survival of Caalginate microencapsulated Bifidobacterium spp. in milk and simulated gastrointestinal conditions. Food Microbiology 19, 35-45 (2002).
117. Eikmeier,H., Westmeier,F., & Rehm,H.J. Morphological Development of Aspergillus-Niger Immobilized in Ca-Alginate and K-Carrageenan. Applied Microbiology and Biotechnology 53-57 (1984).
118. Hansen T.L., Allan-Wojtas,P.M., Jin,Y.L., & Paulson,A.T. SurvivalofCaalginate microencapsulated Bifidobacterium spp. in milk and simulated gastrointestinal conditions. Food Microbiology 19, 35-45 (2002).
119. Baichwal, Staniforth, and John, N. Agglomerated hydrophilic complexes with multi-phasie release characteristics. [5,670,168]. 1997.
Ref Type: Patent
120. Audet,P., Paguin,C., & Lacroix,C. Immobilized Growing Lactic-Acid Bacteria with K-Carrageenan-Locust Bean Gum Gel. Applied Microbiology and Biotechnology 29, 11-18 (1988).
121. Audet,P., Paguin,C., & Lacroix,C. Batch Fermentations with A Mixed Culture of Lactic-Acid Bacteria Immobilized Separately in Kappa-Carrageenan Locust Bean Gum Gel Beads. Applied Microbiology and Biotechnology 32, 662-668 (1990).
83

122. Stacia,M. in Human Physiology. ed. Deborah,ed. 526-527 (1990).
123. Weisz,R.R. Hypokalemia-Induced Clinical Neurophysiological Changes in the Human Neuromuscular-Junction. Clinical Research 28, A 752 (1980).
124. Norton,S., Lacroix,C" & Vuillemard,J.C. Effect ofpH on the Morphology of Lactobacillus helveticus in Free-Cell Batch and Immobilized-Cell Continuous Fermentation. Food Biotechnology 7,235-251 (1993).
125. Sanderson,G.R. in Food Gels. ed. Elsevier 201-233 (New York; 1990).
126. Esquisabel,A., Hemandez,R.M., Igartua,M., Gascon,A.R., Calvo,B., & Pedraz,J.L. Preparation and stability of agarose microcapsules containing BCG. J. Microencapsul. 19,237-244 (2002).
127. Losgen,H., Brunner,G., Holloway,C.J., Buttelmann,B., Husmann,S., Scharff,P., & Siehoff,A. Large agarose beads for extracorporeal detoxification systems. Biomater. Med. Deviees Artif. Organs 6, 151-173 (1978).
128. Lian,W.C., Hsiao,H.C., & Chou,C.C. Survival ofbifidobacteria after spraydrying. Int. J. Food Microbiol. 74, 79-86 (2002).
129. Narayani,R. & Rao,K.P. Gelatin microsphere cocktails of different sizes for the controlled release of anticancer drugs. International Journal of Pharmaeeutics 143,255-258 (1996).
130. Winzer,A. & Lutze,V. Radiochemical Studies of the Influence of Photographically Active Substances on the Kinetics of the Mass-Transfer of Silver-Halide Crystals .9. Activation Parameters for the Mass-Transfer in the Course of the Ostwald-Ripening in the Presence ofUnfolded Gelatin. Journal of Information Recording Materials 22, 65-77 (1994).
131. Crittenden,R., Laitila,A., Forssell,P., Matto,J., Saare1a,M., Mattila-Sandholm,T., & Myllarinen,P. Adhesion ofbifidobacteria to granular starch and its implications in probiotic technologies. Appl. Environ. Microbiol. 67,3469-3475 (2001).
132. Carr, M. E., Doane, W. M., Wing, R. E., and Bagley, E. B. Starch encapsulation ofbiologically active agents by a continuous process. [5,183,690].2-2-1993. United States. 6-25-1990.
RefType: Patent
133. Rosenberg, M. Milk derived whey protein-based microencapsulating agents and a method of use. [5,601,760].2-11-1997. United States. 9-1-1994.
RefType: Patent
134. Shasha, B. S. and Dunkle, R. L. Starch encapsulation of entomopathogens. [4,859,377].8-22-1989. United States. 7-10-1987.
RefType: Patent
84

135. Kulseng,B., Skjak-Braek,G., Ryan,L., Andersson,A., King,A., Faxvaag,A., & Espevik,T. Transplantation of alginate microcapsules: generation of antibodies against alginates and encapsulated porcine islet-like cell c1usters. Transplantation 67, 978-984 (1999).
136. Prakash,S. & Chang,T.M.S. Preparation and In-Vitro Analysis of Microencapsulated Genetically-Engineered Escherichia-Coli Dh5 Cells for Urea and Ammonia Removal. Biotechnology and Bioengineering 46, 621-626 (1995).
137. Awrey,D.E., Tse,M., Hortelano,G., & Chang,P.L. Permeability of alginate microcapsules to secretory recombinant gene products. Biotechnology and Bioengineering 52,472-484 (1996).
138. Schneider,S., Feilen,P.1., Slotty,V., Kampfner,D., Preuss,S., Berger,S., Beyer,J., & Pommersheim,R. Multilayer capsules: a promising microencapsulation system for transplantation of pancreatic islets. Biomaterials 22, 1961-1970 (2001).
139. Wei Ouyang, Chen, Hongmei, Jones M.L., Metz, Terrence, and Satya Prakash. Novel artificial cell forinulation: design, preparation and morphology studies. Polymers in Medicine and Biology . 11-13-0002.
Ref Type: Abstract
140. Chen, Hongmei, Ouyang, Wei, Jones, Mitchell, Metz, Terrence, and Prakash, Satya. Preparation of new multi-layer alginate-chitosan based microcapsules for biomedical applications. Polymers in Medicine and Biology. 11-13-2002.
Ref Type: Abstract
141. Smidsrod,O. & Skjak-Braek,G. Alginate as immobilization matrix for cells. Trends Biotechnol. 8, 71-78 (1990).
, 142. Thu,B., Bruheim,P., Espevik,T., Smidsrod,O., Soon-Shiong,P., & Skjak-Braek,G.
Alginate polycation microcapsules. I. Interaction between alginate and polycation. Biomaterials 17, 1031-1040 (1996).
143. Kulseng,B., Thu,B., Espevik,T., & Skjak-Braek,G. Alginate polylysine microcapsules as immune barrier: permeability of cytokines and immunoglobulins over the capsule membrane. Cell Transplant 6, 387-394 (1997).
144. Hasse,C., Zielke,A., Klock,G., Schlosser,A., Barth,P., Zimmermann,U., Sitter,H., Lorenz,W., & Rothmund,M. Amitogenic alginates: key to first c1inical application of microencapsulation technology. World J. Surg. 22, 659-665 (1998).
145. Orive,G., Ponce,S., Hemandez,R.M., Gascon,A.R., Igartua,M., & Pedraz,J.L. Biocompatibility of microcapsules for cell immobilization elaborated with different type of alginates. Biomaterials 23, 3825-3831 (2002).
85
146. Stokke,B.T., Smidsrod,O., Bruheim,P., & Skjak-Braek,G. Distribution ofuronate residues in alginate chains in relation to alginate gelling properties. Macromolecules 24, 4637-4645 (1991).
147. De Vos,P., De Haan,B., & Van Schilfgaarde,R. Effect of the alginate composition on the biocompatibility of alginate-polylysine microcapsules. Biomaterials 18, 273-278 (1997).
148. Zhang,W.J., Marx,S.K., Laue,C., Hyder,A., Juergensen,A., Bickel,M., & Schrezenmeir,J. HOE 077 reduces fibrotic overgrowth around the barium alginate microcapsules. Transplant Proc. 32,206-209 (2000).
149. Chen,J.P., Chu,I.M., Shiao,M.Y., Hsu,B.R.S., & Fu,S.H. Microencapsulation of islets in PEG-amine modified alginate-poly(L-lysine)-alginate microcapsules for constructing bioartificial pancreas. JOURNAL OF FERMENTATION AND BIOENGINEERING 86, 185-190 (1998).
150. Strand,B.L., Ryan,T.L., In't,V.P., Kulseng,B., Rokstad,A.M., Skjak-Brek,G., & Espevik,T. Poly-L-Lysine induces fibrosis on alginate microcapsules via the induction of cytokines. Cel! Transplant 10, 263-275 (2001).
151. De,S. & Robinson,D. Polymer relationships during preparation of chitosanalginate and poly-l-lysine-alginate nanospheres. J. Control Release 89, 101-112 (2003).
152. Wee,S. & Gombotz,W.R. Protein release from alginate matrices. Adv. Drug Deliv. Rev 31,267-285 (1998).
153. De Vos, P., De Haan, B., Wolters, G. H., Strubbe, J., and Van Schilfgaarde, R. Purification of alginate for microencapsulation of pancreatic islets: effect on biocompatibilityand graft function. 2003.
RefType: Unpublished Work
154. Zhang,W.J., Laue,C., Hyder,A., & Schrezenmeir,J. Purity of alginate affects the viability and fibrotic overgrowth of encapsulated porcine islet xenografts. Transplant Proc. 33,3517-3519 (2001).
155. Cui,J.H., Goh,J.S., Kim,P.H., Choi,S.H., & Lee,B.J. Survival and stability of bifidobacteria loaded in alginate poly-l-lysine microparticles. Int. J. Pharm. 210, 51-59 (2000).
156. O'Shea,G.M. & Sun,A.M. Encapsulation ofrat islets of Langerhans prolongs xenograft survival in diabetic mice. Diabetes 35,943-946 (1986).
157. Orive,G., Ponce,S., Hemandez,R.M., Gascon,A.R., Igartua,M., & Pedraz,J.L. Biocompatibility of microcapsules for cell immobilization elaborated with different type of alginates. Biomaterials 23, 3825-3831 (2002).
86

158. Babensee,J.E. & Sefton,M.V. AlIogeneic and xenogeneic transplantation of HEMA-MMA microencapsulated hepatoma celIs into rats. Cel! Transplantation 5, 56 (1996).
159. Roberts,T., De Boni,U., & Sefton,M.V. Dopamine secretion by PC12 celIs microencapsulated in a hydroxyethyl methacrylate--methyl methacrylate copolymer. Biomaterials 17,267-275 (1996).
160. Lahooti,S. & Sefton,M.V. Effect of an immobilization matrix and capsule membrane permeability on the viability of encapsulated HEK cells. Biomaterials 21, 987-995 (2000).
161. Babensee,J .E., Comelius,R.M., Brash,J .L., & Sefton,M. V. Immunoblot analysis of proteins associated with HEMA-MMA microcapsules: human serum proteins in vitro and rat proteins folIowing implantation. Biomaterials 19, 839-849 (1998).
162. Sefton,M.V., May,M.H., Lahooti,S., & Babensee,J.E. Making microencapsulation work: conformaI coating, immobilization gels and in vivo performance. J. Control Release 65, 173-186 (2000).
163. Dawson,R.M., Broughton,R.L., Stevenson,W.T., & Sefton,M.V. Microencapsulation of CHû celIs in a hydroxyethyl methacrylate-methyl methacrylate copolymer. Biomaterials 8, 360-366 (1987).
164. Lahooti,S~ & Sefton,M.V. Effect ofan immobilization matrix and capsule membrane permeability on the viability of encapsulated HEK cells. Biomaterials 21, 987-995 (2000).
165. Chia,S.M., Wan,A.C., Quek,C.H., Mao,H.Q., Xu,x., Shen,L., Ng,M.L., Leong,K.W., & Yu,H. Multi-Iayered microcapsules for celI encapsulation. Biomaterials 23, 849-856 (2002).
166. Broadhead,K.W. & Tresco,P.A. Effects of fabrication conditions on the structure and function of membranes formed from poly (acrylonitrile-vinylchloride). JOURNAL OF MEMBRANE SCIENCE 147, 235-245 (1998).
167. Bridge,M.J., Broadhead,K.W., Hlady,V., & Tresco,P.A. Ethanol treatment alters the uitrastructure and permeability ofPAN-PVC hollow fiber cell encapsulation membranes. JOURNAL OF MEMBRANE SCIENCE 195,51-64 (2002).
168. CIark,H., Barbari,T.A., Stump,K., & Rao,G. Histologie evaluation ofthe inflammatory response around implanted hollow fiber membranes. J. Biomed. Mater Res. 52, 183-192 (2000).
169. Broadhead,K. W., Biran,R., & Tresco,P .A. Hollow fiber membrane diffusive permeability regulates encapsulated cellline biomass, proliferation, and small molecule release. Biomaterials 23, 4689-4699 (2002).
87
170. Shoiehet,M.S. & Rein,D.H. In vivo biostability of a polymerie hollow fibre membrane for cell eneapsulation. Biomaterials 17,285-290 (1996).
171. Sehneider,B.L., Sehwenter,F., Pralong,W.F., & Aebiseher,P. Prevention of the initial host immuno-inflammatory response determines the long-term survival of encapsulated myoblasts genetically engineered for erythropoietin delivery. Mol. Ther. 7,506-514 (2003).
172. Honiger,J., Sarkis,R., Baudrimont,M., Delelo,R., Chafai,N., Benoist,S., Sarkis,K., Balladur,P., Capeau,J., & Nordlinger,B. Semiautomatic macroencapsulation of large numbers of porcine hepatocytes by coextrusion with a solution of AN69 polymer. Biomaterials 21, 1269-1274 (2000).
173. Kurian,P., Kasibhatla,B., Daum,J., Burns,C.A., Moosa,M., Rosenthal,K.S., & Kennedy,J.P. Synthesis, permeability and biocompatibility oftricomponent membranes containing polyethylene glycol, polydimethylsiloxane and polypentamethylcyclopentasiloxane domains. Biomaterials 24,3493-3503 (2003).
174. Premkumar,J.R., Rosen,R., Belkin,S., & Lev,O. Sol-gel luminescence biosensors: Encapsulation of recombinant E. coli reporters in thick silicate films. Analytica Chimica Acta 462, 11-23 (2002).
175. Isayeva,I.S., Kasibhatla,B.T., Rosenthal,K.S., & Kennedy,J.P. Characterization and performance of membranes designed for macroencapsulationlimplantation of pancreatic islet cells. Biomaterials 24, 3483-3491 (2003).
176. Boninsegna,S., Bosetti,P., Carturan,G., Dellagiacoma,G., DaI Monte,R., & Rossi,M. Eneapsulation of individual panereatic islets by sol-gel Si02: a novel procedure for perspective cellular grafts. J. Biotechnol. 100,277-286 (2003).
177. Carturan, G., Muraca, M., and DaI Monte, R. Encapsulation of supported animal cells using gas-phase inorganic alkoxides. [6,214,593]. 2001. USA.
RefType: Patent
178. Sglavo,V.M., Carturan,G., DaI Monte,R., & Muraca,M. Si02 entrapment of animal cells - Part l - mechanical features of sol-gel Si02 coatings. JOURNAL OF MATERIALS SCIENCE 34,3587-3590 (1999).
179. Wang,T., Lacik,l., Brissova,M., Anilkumar,A.V., Prokop,A., Hunkeler,D., Green,R., Shahrokhi,K., & Powers,A.C. An encapsulation system for the immunoisolation of pancreatic islets. Nat. Biotechnol. 15, 358-362 (1997).
180. Risbud,M.V., Bhargava,S., & Bhonde,R.R. In vivo biocompatibility evaluation of cellulose macrocapsules for islet immunoisolation: Implications oflow molecular weight cut-off. J. Biomed. Mater Res. 66A, 86-92 (2003).
181. Lohr,M., Hoffmeyer,A., Kroger,J., Freund,M., Hain,J., Holle,A., Karle,P., Knofel,W.T., Liebe,S., Muller,P., Nizze,H., Renner,M., Saller,R.M., Wagner,T.,
88
Hauenstein,K., Gunzburg,W.H., & Salmons,B. Microencapsulated cell-mediated treatment of inoperable pancreatic carcinoma. Lancet 357, 1591-1592 (2001).
182. Kino,Y., Sawa,M., Kasai,S., & Mito,M. Multiporous cellulose microcarrier for the development of a hybrid artificialliver using isolated hepatocytes. J. Surg. Res. 79, 71-76 (1998).
183. Dautzenberg,H., Schuldt,U., Lerche,D., Woehlecke,H., & Ehwald,R. Size exclusion properties of polyelectrolyte complex microcapsules prepared from sodium cellulose sulphate and poly[diallyldimethylammonium chloride]. J. Membr. Sei. 162, 165-171 (1999).
184. Risbud,M.V. & Bhonde,R.R. Suitability of cellulose molecular dialysis membrane for bioartificial pancreas: in vitro biocompatibility studies. J. Biomed. Mater Res. 54,436-444 (2001).
185. Coca,E., Ribas,B., & Trigueros,G. A method for quick determination of bile acids in bile of patients with biliary lithiasis. J. of Liquid Chromatogr. 17, 1349-1363 (1994).
186. Rossi,S.S., Converse,J.L., & Hofinann,A.F. High pressure liquid chromatographic analysis of conjugated bile acids in human bile: simultaneous resolution of sulfated and unsulfated lithocholyl amidates and the common conjugated bile acids. J. Lipid Res. 28, 589-595 (1987).
187. Cantafora,A., Di Biase,A., Alvaro,D., & Angelico,M. Improved method for measuring the glycine and taurine conjugates ofbile salts by high-performance liquid chromatography with tauro-7 alpha,12 alpha-dihydroxy-5 beta-cholanic acid as internaI standard. J. Chromatogr. 386,367-370 (1987).
188. Scalia,S. Simultaneous determination of free and conjugated bile acids in hum an gastric juice by high-performance liquid chromatography. J. Chromatogr. 431, 259-269 (1988).
189. Bongaerts,G.P., Severijnen,R.S., Tangerman,A., Verrips,A., & Tolboom,J.J. Bile acid deconjugation by Lactobacilli and its effects in patients with a short small bowel. J. Gastroenterol. 35,801-804 (2000).
190. Hofinann,A.F. in Handbook ofPhysiology. Gastrointestinal system, Vol. IV 567-596 (American Physiological Society, Bethesda; 1989).
191. Kobayashi,N., Katsumata,H., Uto,Y., Goto,J., Niwa,T., Kobayashi,K., & Mizuuchi,Y. A monoclonal antibody-based enzyme-linked immunosorbent assay of glycolithocholic acid sulfate in human urine for liver function test. Steroids 67, 827-833 (2002).
192. Rozga,J., Williams,F., Ro,M.S., Neuzil,D.F., Giorgio,T.D., Backfisch,G., Moscioni,A.D., Hakim,R., & Demetriou,A.A. Development of a bioartificialliver:
89

properties and function of a hollow-fiber module inoculated with liver cells. Hepatology 17, 258-265 (1993).
193. Schafer,D.F. & Shaw,B.W., Jr. Fulminant hepatic failure and orthotopic liver transplantation. Sernin. Liver Dis. 9, 189-194 (1989).
194. Hofrnann,A.F. Bile Acids: The Good, the Bad, and the Ugly. News Physiol Sei. 14,24-29 (1999).
195. De Boever,P. & Verstraete,W. Bile salt deconjugation by lactobacillus plantarum 80 and its implication for bacterial toxicity. J. Appl. Microbiol. 87,345-352 (1999).
196. De Boever,P., Wouters,R., Verschaeve,L., Berckmans,P., Schoeters,G., & Verstraete,W. Protective effect of the bile salt hydrolase-active Lactobacillus reuteri against bile salt cytotoxicity. Appl. Microbiol. Biotechnol. 53, 709-714 (2000).
197. Oumi,M. & Yarnarnoto,T. A scanning electron microscope study on the effects of different bile salts on the epitheliallining of jejunal mucosa. Med. Electron Microsc. 33, 11-15 (2000).
198. Jankovsky,M. & Vasakova,L. [Irnrnobilization in alginate gels]. Veto Med. (Praha) 41, 159-164 (1996).
199. Sirnrnonds,W.J., Hofrnann,A.F., & Theodor,E. Absorption of cholesterol from a micellar solution: intestinal perfusion studies in man. J. Clin. Invest 46,874-890 (1967).
200. Mullen,Y., Maruyarna,M., & Smith,C.V. CUITent progress and perspectives in immunoisolated islet transplantation. J. Hepatobiliary. Pancreat. Surg. 7,347-357 (2000).
201. Tatarkiewicz,K., Garcia,M., Lopez-Avalos,M., Bonner-Weir,S., & Weir,G.C. Porcine neonatal pancreatic cell clusters in tissue culture: benefits of serum and irnrnobilization in alginate hydrogel. Transplantation 71, 1518-1526 (2001).
202. Christiaens,H., Leer,RJ., Pouwels,P.H., & Verstraete,W. Cloning and expression of a conjugated bile acid hydrolase gene from Lactobacillus plantarum by using a direct plate assay. Appl. Environ. Microbiol. 58, 3792-3798 (1992).
203. Coca,E., Ribas,B., & Trigueros,G. A method for quick deterrnination of bile acids in bile of patients with biliary lithiasis. J. of Liquid Chrornatogr. 17, 1349-1363 (1994).
204. Scalia,S. Simultaneous deterrnination offree and conjugated bile acids in human gastric juice by high-perforrnance liquid chromatography. J. Chrornatogr. 431, 259-269 (1988).
90
205. De Boever,P., Wouters,R., Verschaeve,L., Berckmans,P., Schoeters,G., & Verstraete,W. Protective effect ofthe bile salt hydrolase-active Lactobacillus reuteri against bile salt cytotoxicity. Appl. Microbiol. Biotechnol. 53, 709-714 (2000).
206. American Heart Association. Heart Disease and Stroke Statistics - 2002 Update. 2002. Dalas Texas.
RefType: Report
207. Aboderin, L, Kalache, A., Ben-Shlomo, Y., Lynch, J. W., Yajnik, C. S., Kuh, D., and Yach, D. Life Course Perspectives on Coronary Heart Disease, Stroke and Diabetes: Key Issues and Implications for Policy and Research. 2002. Geneva, World Health Organization.
Ref Type: Report
208. Bliznakov,E.G. Lipid-Iowering drugs (statins), cholesterol, and coenzyme QI0. The Baycol case--a modern Pandora's box. Biomed. Pharmacother. 56, 56-59 (2002).
209. Kolata G and Andrews EL. Anticholesterol Drug pulled after link to 31 deaths. New York Times Online. 9-9-2001.
RefType: Newspaper
210. Willman D. A gigantic headache for Bayer. New York Times Online. 9-14-2001. RefType: Newspaper
211. McGilvery RW in Biochemistry. A functional approach. 555-571 (W.B. Saunders, Company, Tokio; 1983).
212. Stone,W.L. & Papas,A.M. Tocopherols and the etiology of colon cancer. J. Natl. Cancer Inst. 89, 1006-1014 (1997).
213. Back P in The bile acids: chemistry, physiology, and metabolism. vol 4. Methods and applications, Vol. 4. eds. Setchell KDR, Kritchevski D, & Nair PP 405-440 (Plenum Press, New York; 1988).
214. Abouna,G.M., Ganguly,P.K., Hamdy,H.M., Jabur,S.S., Tweed,W.A., & Costa,G. Extracorporealliver perfusion system for successful hepatic support pending liver regeneration or liver transplantation: a pre-clinical controlled trial. Transplantation 67, 1576-1583 (1999).
215. Morsiani,E., Pazzi,P., Moscioni,A.D., Rozga,J., Azzena,G., & Demetriou,A.A. In vitro morphological and functional characterization of isolated porcine hepatocytes for extracorporealliver support: bile acid uptake and conjugation. J. Surg. Res. 79, 54-60 (1998).
91