nose ring application. diseases of the forestomachs m. s. gill, d.v.m., m.s
TRANSCRIPT

Nose Ring Application

Nose Ring Application

Nose Ring Application

Nose Ring Application

Nose Ring Application

Diseases of the Forestomachs
M. S. Gill, D.V.M., M.S.

Ruminant Carbohydrate Engorgement
• Grain overload
• Lactic acidosis
• Carbohydrate intoxication
• Grain engorgement
• Founder

History• Access to highly fermentable feedstuffs
– by unaccustomed animals, or– in larger than normal amounts
• May involve several animals in herd
• Rapid clinical course
Clinical findings• Abdominal pain
• Dehydration (6-12 %)
• Diarrhea – fluid, fetid
• Splashy rumen, bloat
• Depression
• Lameness
• Scleral injection

Clinical findings• Elevated temp initially, may be
subnormal when presented
• HR = 80-140 bpm
• RR elevated (blow off CO2)
• Rumen fluid analysis– pH < 5– sour odor– protozoa dead, predominance of gram +

Clinical findings• Metabolic acidosis
• PCV
• protein
• Elevated BUN, creatinine, phosphorous
• Increased anion gap
• Decreased calcium

Pathogenesis
• Excess CHO ingestion, VFAs, rumen pH, rumen motility, Strep bovis proliferates producing lactic acid, further pH (4-5)
• Acid resistant Lactobacillus spp. proliferate producing lactic acid

Pathogenesis
• Lactic acid accumulation in the rumen osmolarity of the rumen fluid drawing more body water into the rumen (creates the “splashy rumen”)
• Loss of body water causes dehydration contributing to acidosis
• Lactic acid is absorbed from rumen as well as from small intestine & profound lactic acidosis develops

Pathogenesis
• Acidic rumen pH damages mucosal surfaces in the forestomachs & intestine
• Blood vessels thrombose & sections of rumen mucosa & submucosa slough allowing bacteria to invade
• Bacteria travel to liver via portal circulation & cause liver abscesses
• Mycotic ruminitis may develop

Pathogenesis
• Histamine levels increase
• Ethanol, methanol, tyramine, tryptamine production contribute to CNS depression
• Thiaminase production may result in development of polio
• Death of Gram – bacteria can cause endotoxin release
What feeds can cause carbohydrate engorgement?
• Cereal grains
• Industrial byproducts (brewers grains, sugars)
• Fruits
• Tubers (potatoes, sugar beets)

What feeds can cause carbohydrate engorgement?
• Finely ground feeds with large surface area promote rapid fermentation
• Hay and grass are are not highly fermentable due to cellulose and large particle size
• Corn silage usually not a problem because much of CHO already reduced to VFAs in ensiling process and also due to large particle size

Diagnosis
• History
• Clinical signs and clinical findings
• Rumen fluid analysis
• CBC, chem panel, blood gas
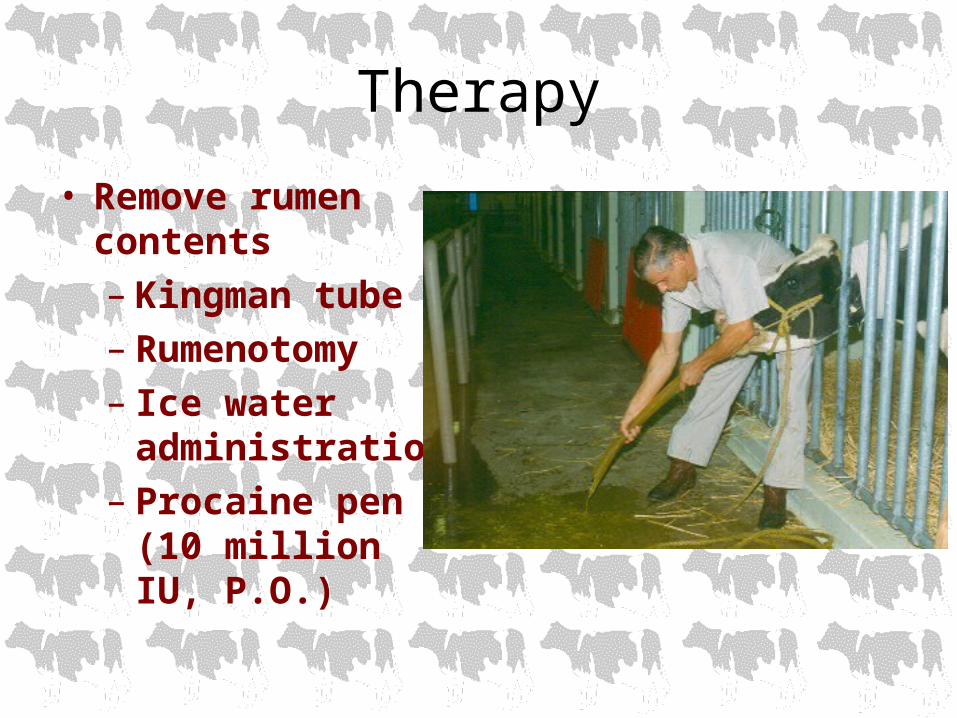
Therapy
• Remove rumen contents– Kingman tube– Rumenotomy– Ice water
administration– Procaine pen G
(10 million IU, P.O.)

Therapy
• Fluid and electrolyte replacement IV• Anti-inflammatory agents –flunixin
meglumine (Banamine)• Antibiotics• Antimycotic therapy• Rumen transfaunation• Thiamine• B-complex vitamins

Client education
• Make dietary changes very gradually– Addition of antibiotics, HCO3-, and
ionophore antibiotics to the feed have been beneficial but do not replace good management
• Rumen adaptation may take 6 weeks

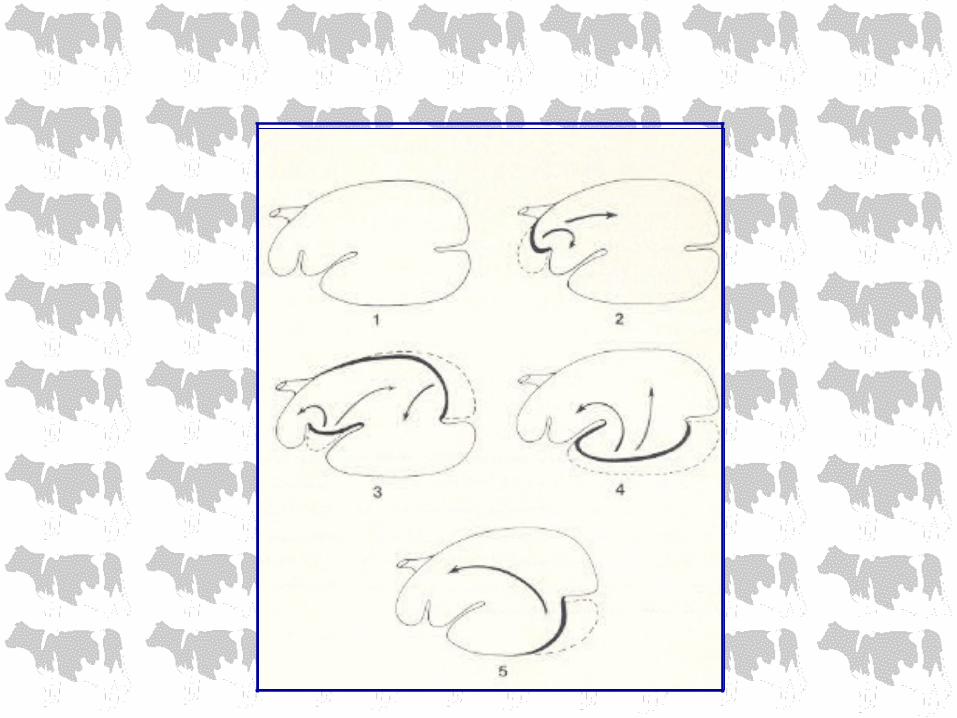
Rumenotomy

Rumenotomy

Rumenotomy

Rumenotomy

Rumenotomy

Rumenotomy

Rumenotomy

Rumen tympany (bloat)
• Gas production is a normal occurrence during rumen fermentation
• Bloat occurs if eructation is prevented for any reason

Clinical findings
• Distended left paralumbar fossa• Discomfort (grunting, colic)• Open-mouth breathing• Anorexia• Salivation• Anxious• Depressed terminally• Sudden death

Types of bloat
• Primary– Eructation normal but gas cannot be expelled
• frothy bloat – legumes or grain (Strep bovis)
• Secondary– Failure of eructation
• esophageal FB’s• vagus indigestion• positional• hypocalcemia• pharyngitis
Diagnosis
• History
• Clinical findings

THERAPY
• Free gas bloat– Pass a stomach tube (carefully) either
nasogastric or orogastric– If positional, roll cow into sternal recumbency– Force exercise– If hypocalcemia, administer calcium – Rumen stimulents– Rumen trocharization for emergencies only

THERAPY
• Frothy bloat– Reduce surface tension
• Poloxalene – 2 oz.• Household detergent (Tide 2-3 oz.)• Mineral oil• Dioctyl sodium sulfosuccinate (DSS)
*All of the above reduce surface tension allowing consolidation of tiny bubbles into a free gas bloat which can be eructated or relieved via tube

THERAPY
• Chronic bloat – typically free gas bloat associated with high grain diets that may cause a permanent shift in microflora– Increase fiber in diet & reduce grain– Rumen transfaunation– Temporary rumenostomy in severe cases
• May be 2° to another problem such as vagus indigestion
Rumen tympany (bloat)

Rumen tympany (bloat)

Rumenostomy

Client education
• Slow adaptation to grain
• Limit legume grazing
• Poloxalene in feed, molasses, salt or block
• Maintain sufficient long stem hay (fiber) in ration to stimulate good rumen motility

Rumenitis, rumen parakeratosis, chronic rumen acidosis
• Long-term ingestion of high grain, low roughage diet
• Poor appetite
• Poor weight gain
• Chronic laminitis

Rumenitis, rumen parakeratosis, chronic rumen acidosis
• Clinical findings– Hypomotile rumen– Elevated liver enzymes– Rumen protozoa, gram + bacteria

Rumenitis, rumen parakeratosis, chronic rumen acidosis
• Chronic exposure to high grain diet• Low rumen pH (5.0-5.5)• Increased propionic & butyric acid which
stimulates proliferation of rumen papillae epithelium and even parakeratosis
• Fine particle size, less cud chewing, less saliva buffering rumen contents
• Damage to rumen leads to liver abscesses

Rumenitis, rumen parakeratosis, chronic rumen acidosis
• Treatment includes increasing proportion of long stem hay in the diet

Vagus indigestion syndrome
• Motor disturbances which impair passage of ingesta from the reticulorumen and/or abomasum into the lower GI tract

Vagus indigestion syndrome
• “Vague” signs• Slow loss of production• Slow weight loss• Poor appetite• Scant, pasty feces• Abdominal enlargement - “papple”
shape• Rumen hyper motility, bradycardia

Vagus indigestion syndrome

Vagus indigestion syndrome
• Classification:– Lesions anterior to cardia– Lesions at the cardia– Lesions at the reticulum– Lesions distal to the reticulum
Vagus indigestion syndrome
• Treatment involves correction of underlying problem
• Lymphosarcoma hopeless
• Rumen lavage
• Rumenotomy to remove contents & ‘shrink’ rumen or to treat reticular abscesses

Vagus indigestion syndrome
Traumatic reticuloperitonitis (TRP, hardware disease)
• Sudden decrease in appetite & milk production
• Anterior abdominal pain
• Kyphosis
• Low grade fever (103°)
• Mild leukocytosis with neutrophilia
• Hyperfibrinogenemia

Traumatic reticuloperitonitis (TRP, hardware disease)
• Diagnostics– History– Clinical findings– Paracentesis– Reticular radiography– ultrasound

Traumatic reticuloperitonitis (TRP, hardware disease)
• Medical treatment– Antibiotics– Magnet
• Surgical treatment– Rumenotomy to approach reticulum

Traumatic reticuloperitonitis (TRP, hardware disease)

Traumatic reticuloperitonitis (TRP, hardware disease)

Abomasal ulcers
• Occur in all ages of cattle• Associated with stress & high concentrate
diets and lymphosarcoma in older animals• Four categories
– Non-perforating– Non-perforating with severe blood loss*– Perforating with localized peritonitis– Perforating with diffuse peritonitis*
*life threatening

Abomasal ulcers
• Diagnostics– Fecal occult blood– Abdominocentesis– WBC – leukocytosis with neutrophilia, high
fibrinogen– Serology for BLV

Abomasal ulcers
• Calves– Usually see perforation with peritonitis– May be associated with copper deficiency
• Adults– 1/3 significant hemorrhage– 1/3 perforating with localized peritonitis– 1/3 perforating with diffuse peritonitis

Abomasal ulcers
• Treatment– Dietary changes– Decrease stress– Avoid steroid & NSAID use– Treat concurrent problems– Blood transfusions– Antibiotics– GI protectants– H2 antagonists
Clinical case
• History:– Yearling BFM show heifer– History of mild abdominal pain– Mild bloat– Off feed– Change in feed in last week

• Clinical findings:– T – 103°– Leukocytosis, neutrophilia– Increased fibrinogen– Abdominocentesis
• Protein > 3.5• WBC > 10,000• Neutrophilic inflammation
• Treatment:– Antibiotics– Decrease stress– Dietary change – hay, ryegrass, no grain– Rumen transfaunation– Avoid NSAIDS & steroids

Abomasal impaction
• Causes:– Poor quality roughage for overwintering beef
cows– Calves fed poor quality milk replacers– Animals on low fiber diets– Abomasal volvulus– Lymphosarcoma

Abomasal impaction
• Clinical signs:– Takes weeks to develop– Decreased appetite– Firm, dry feces– Rumen enlargement, stasis– Poor BCS– Abomasal rupture may occur

Abomasal impaction
• Differentials– Hydrops– Chronic peritonitis– Vagus indigestion– Omasal impaction

Abomasal impaction
• Poor quality roughage is poorly digested so fibrous material passes to the abomasum creating accumulation of fibrous material in the abomasum which can not pass through
• May develop post abomasal volvulus due to vagus nerve dysfunction

Abomasal impaction
• Prognosis poor if advanced (slaughter)• Fluid therapy*, laxatives, metaclopramide to early cases• Terminate pregnancy• Rumenotomy, backflush abomasal contents into rumen • Place NG tube directly into abomasum for post-op
medication
*usually don’t develop metabolic alkalosis & hypochloremia

Abomasal emptying defect (AED)
• Suffolk sheep• Anorexia, weight loss, abdominal enlargement• Abomasum is enlarged and palpable• DDx:
– Malnutrition– Parasitism– Dental attrition– Johne’s– Caseous lymphadenitis– Neoplasia– Chronic pneumonia

Abomasal emptying defect (AED)
• Diagnostics– Increased rumen chloride (normal = 8-15
mEq/L)– Ultrasound abomasum – normal diameter is
2-3”, with AED may see abomasal diameter of 6-10”
• Pathophysiology remains unknown

Abomasal emptying defect (AED)
• Treatment:– Surgery – rumenotomy & backflush rumen– Metaclopramide – facilitates abomasal
emptying