nonpenetrating traumaticinjury the aorta - semantic scholar · and the walter reed army hospital,...
TRANSCRIPT

Nonpenetrating Traumatic Injury of the AortaBy LOREN F. PARMLEY, LT. COLONEL, MC, THOMAS W. MATTINGLY, BRIG. GEN., MC,
WILLIAM C. MANION, M.D., AND EDWARD J. JAHNKE, JR., MAJ., MC
Rupture or laceration of the aorta is a more common result of nonpenetrating traumaticinjury than is generally appreciated. Approximately 15 per cent of individuals withtraumatic rupture survive temporarily. If the lesion is promptly diagnosed appropriatesurgical treatment may be life-saving. Diagnosis may be difficult and at times therupture may remain clinically silent for variable periods. The natural course fromaortic rupture to false aneurysm formation with secondary rupture of the aneurysmmay be brief or extend over many years. Surgical treatment of a false aneurysm thathas remained stable for a prolonged period has been successful, but in some instancesconservative management may be the treatment of choice.
O F ALL the cardiovascular lesions thatresult from nonpenetrating traumatic
injury none demonstrates the need forprompt recognition and surgical therapy asemphatically as rupture of the aorta that isnot immediately fatal. That anyone survivescomplete transection of this major artery isalmost unbelievable; nonetheless, an appre-ciable number have survived.The medical literature contains many case
reports of aortic rupture caused by trauma.According to Sailer' one of the first cases ofaortic aneurysm, presumably the result oftrauma, was reported in 1557 by Vesalius.Two of the larger series were reported byKuhn,2 who collected 75 cases published be-tween 1895 and 1925, and Strassmann,3 whoreviewed the literature in 1947 in connectionwith his report on 72 cases of his own. Pa-tients who have survived aortic rupture, in-cluding those in whom post-traumatic aorticaneurysms developed, have been less fre-quently reported. The English literaturelists at least 57 cases2-30 of aortic rupturecaused by nonpenetrating trauma which thepatients have survived for varying lengths oftime. The lesion in all these cases was con-firmed by postmortem or surgical examina-tion. Other cases of aortic rupture with sur-vival have been reported, but the diagnoseswere made clinically. The 5 cases of traumatic
From the Armed Forces Institute of Pathology,and the Walter Reed Army Hospital, Washington,D. C.
aortic aneurysm recently reported by Stein-berg36 are well documented despite lack ofsurgical or postmortem confirmation in 4.Although an individual with an apparenttraumatic aneurysm of the abdominal aortahas been reported to have survived 27 yearsafter injury,10 the relationship to trauma inthis case may be questioned. However, the27-year survival of an individual with a trau-matic aneurysm of the thoracic aorta was alsoreported by Steinberg,36 and 4 others in hisseries had survived for periods of from 2 to21 years. One patient with a traumaticaneurysm of the thoracic aorta survived 8years before surgical repair,23 but most pa-tients have lived for periods of from 15 min-utes to 3 weeks before surgical interventionor death.
It is the purpose of this paper to presentthe salient clinical and pathologic featuresobserved in our series of 296 cases of aorticinjury caused by nonpenetrating trauma andto discuss the diagnosis and management ofaortic rupture in those who survive the im-mediate effects of the injury. Of the 1,174necropsy cases of traumatic injury of theheart and aorta we have studied from the filesof the Armed Forces Institute of Pathology,275 were cases of aortic rupture, 104 com-bined with cardiac injury (table 1). In-cluded in the series are 2 living patients inwhom traumatic aortic aneurysm has beencorrected surgically. In addition to the 275cases of aortic rupture, 21 cases of laceration
Circulation, Volume XVII, June 19581086)
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from
NONPENETRATING INJURY OF THE AORTA
involving only 1 or 2 layers of the aorta werestudied, for a total of 296. In all but 1 of the21 there was associated cardiac injury. Thir-ty-eight of the patients with aortic rupturesurvived the injury for a time.
Injuries other than cardiovascular werefrequently sufficient to cause death. In an an-alysis of the cause of death in this series itwas found that approximately 80 per centof patients with combined cardiac and aorticinjury and at least half of those with aorticrupture only would have died from theirother injuries had there been no cardiovascu-lar lesion.The majority of patients were young men,
only 4 of the 275 being women. This distri-bution does not reflect a true sex incidence,but only the sex distribution of the materialat the Armed Forces Institute of Pathology,which is drawn from a predominantly malepopulation. The average age in this serieswas 27 years, 18 and 85 years being the ex-tremes.The forces that produce aortic rupture are
the same as for other nonpenetrating cardio-vascular injuries; namely, direct and indirectforces, deceleration, compression, and blast.Often a combination of 2 or more of theseforces is responsible.The mechanism whereby aortie injury or
rupture is produced varies with the type offorce. A direct force that results in fractureor displacement of one of the dorsolumbarvertebrae may cause rupture of the aorta byshearing action.
Indirect force apparently acts throughproduction of increased intravascular pres-sure. It has been demonstrated experiment-ally37 that such a pressure may exceed 1,000mm. Hg without causing rupture. An ap-parently normal human aorta has been rup-tured by an aortic pressure of 2,070 mm.Hg.38 Zehnder29 tested the tensile strengthof strips of aorta and calculated that pres-sure sufficient to cause rupture is equivalentto an intravascular pressure of 2,500 min. Hg.Our series includes an instance of rupture ofthe arch of the aorta by indirect force result-ing from a cave-in accident that suddenly
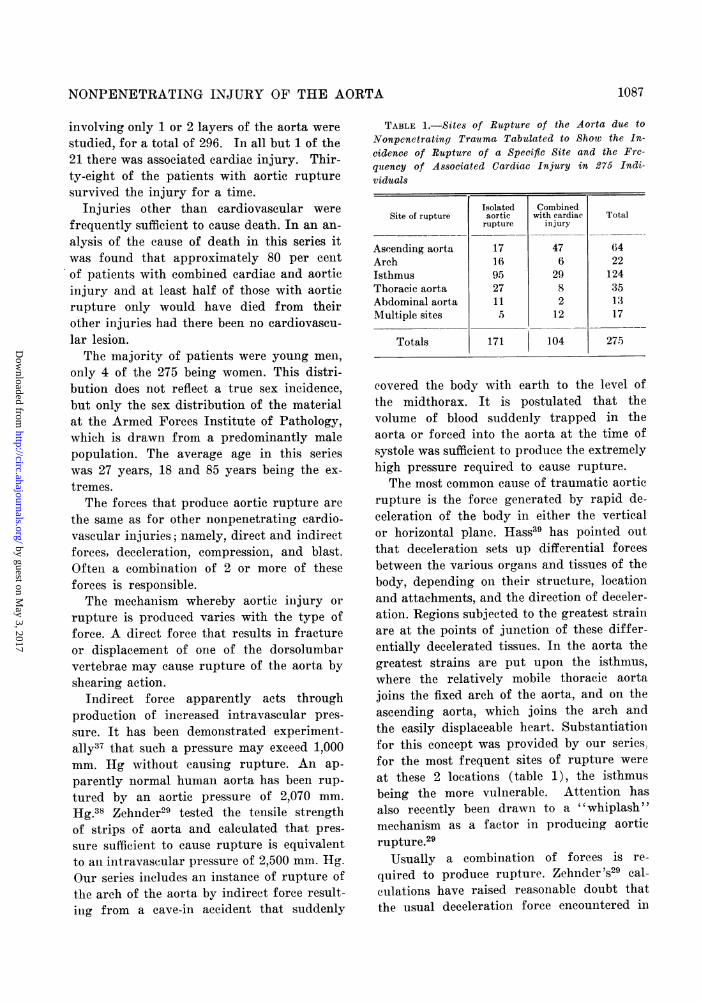
TABLE 1.-Sites of Rupture of the Aorta due toNonpenetrating Trauma Tabulated to Show the In-cidence of Rupture of a Specific Site and the Fre-quency of Associated Cardiac Injury in 275 Indi-viduals
Isolated CombinedSite of rupture aortic with cardiac Total
rupture injury
Ascending aorta 17 47 (A4Arch 16 6 22Isthmus 95 29 124Thoracic aorta 27 8 35Abdominal aorta 11 2 13Multiple sites 5 12 17
Totals 171 104 275
covered the body with earth to the level ofthe midthorax. It is postulated that thevolume of blood suddenly trapped in theaorta or forced into the aorta at the time ofsystole was sufficient to produce the extremelyhigh pressure required to cause rupture.
The most common cause of traumatic aorticrupture is the force generated by rapid de-celeration of the body in either the verticalor horizontal plane. Hass39 has pointed outthat deceleration sets up differential forcesbetween the various organs and tissues of thebody, depending on their structure, locationand attachments, and the direction of deceler-ation. Regions subjected to the greatest strainare at the points of junction of these differ-entially decelerated tissues. In the aorta thegreatest strains are put upon the isthmus,where the relatively mobile thoracic aortajoins the fixed arch of the aorta, and on theascending aorta, which joins the arch andthe easily displaceable heart. Substantiationfor this concept was provided by our series,for the most frequent sites of rupture were
at these 2 locations (table 1), the isthmusbeing the more vulnerable. Attention hasalso recently been drawn to a "whiplash "mechanism as a factor in producing aorticrupture.29
Usually a combination of forces is re-
quired to produce rupture. Zehnder 's29 cal-culations have raised reasonable doubt thatthe usual deceleration force encountered in
1087
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from
PARMLEY, MATTINGLY, MIANION, AND JAHNKE
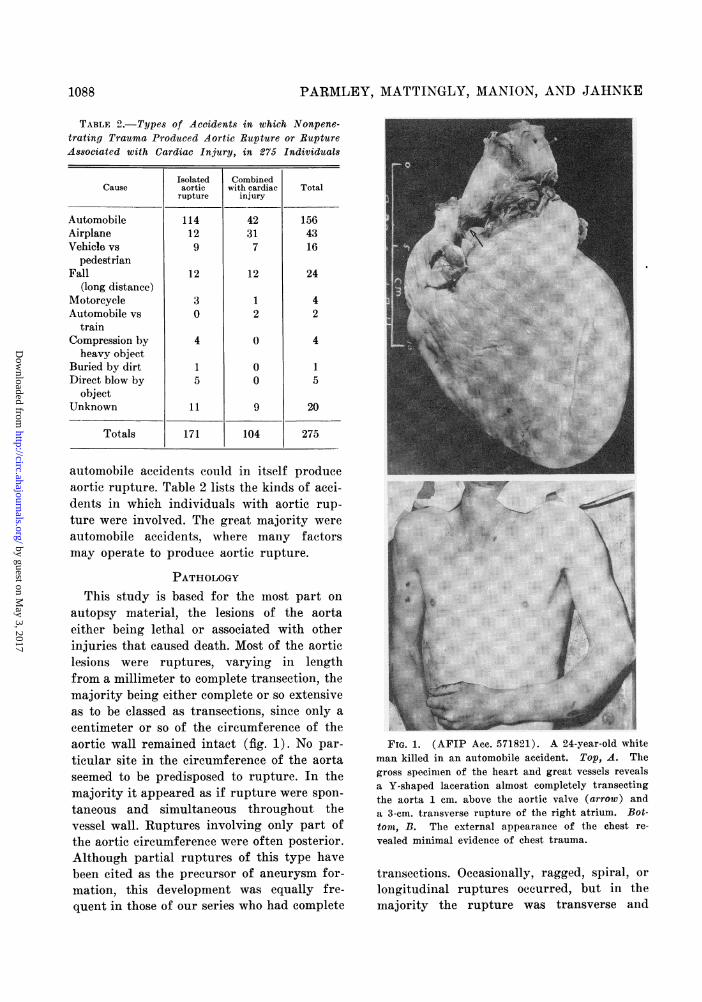
TABLE 2. Types of Accidents in which Nonpene-tratiny Trauma Produced Aortic Rupture or RuiptureAssociated with Cardiac Injury, in 275 Individuals
Cause
AutomobileAirplaneVehicle vs
pedestrianFall
(long distance)MotorcycleAutomobile vs
trainCompression byheavy object
Buried by dirtDirect blow by
objectUnknown
Totals
automobile accidents could in itself produceaortic rupture. Table 2 lists the kinds of acei-dents in which individuals with aortic rup-
ture were involved. The great majority were
automobile accidents, where many factorsmay operate to produce aortic rupture.
PATHOLOGYThis study is based for the most part on
autopsy material, the lesions of the aortaeither being lethal or associated with otherinjuries that caused death. Most of the aorticlesions were ruptures, varying in lengthfrom a millimeter to complete transection, themajority being either complete or so extensiveas to be classed as transections, since only a
centimeter or so of the eircumference of theaortic wall remained intact (fig. 1). No par-
ticular site in the circumference of the aortaseemed to be predisposed to rupture. In themajority it appeared as if rupture were spon-
taneous and simultaneous throughout thevessel wall. Ruptures involving only part ofthe aortic cireumference were often posterior.Although partial ruptures of this type havebeen cited as the precursor of aneurysm for-
mation, this development was equally fre-
quent in those of our series who had complete
FIG. 1. (AFIP Acc. 571821). A 24-year-old white
man killed in an automobile accident. Top, A. The
gross specimen of the heart and great vessels reveals
a Y-shaped laceration almost completely trainsectiiigthe aorta 1 cm. above the aortic valve (arrow) and
a 3-em. transverse rupture of the right atrium. Bot-
toutR, B. The external appeal-ance of the chest re-
vealed minimal evidence of chest trauma.
transections. Occasionally, ragged spiral or
longitudinal ruptures occurred, but in themajority the rupture was transverse and
Isolatedaorticrupture
114129
12
30
4
15
11
171
Combinedwith cardiac
injury
42317
12
12
0
00
9
104
Total
1564316
24
42
4
151
20
275
1088
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
FIG. 2. (AFIP Ae. 639151). (A) Stained section showing a small area of intimal heinor-rhage with an intact endothelial surface. There are extravasated red blood cells in thesubintimal tissue. The lhemorrhage is limited to the intinia of the aorta. X70. (B). (AFIPAcc. 652262). Laceration of the aorta at the junction of the intima and media along theinternal elastic membrane. In this region the integrity of the intimal surface is still pre-served. There is a small amount of hemiorrhage in the lacerated area. X 50. (C) (Same caseas fig. 2B). Elastic stained section from another region of the aorta showing an aortic lacera-tion with tearing and partial dissection of the intimia from the media. The internal elasticmembrane is visualized in this section. Note the small amount of intimal hemorrhage and thetear through the media. X 50 (D) (AFIP Ace. 639151). A section from the aorta showing amedial laceration with tearing and separation of the elastic lamella and hemorrhage into theadjacent media. Disruption of the media is evident. X 35.
smooth. In a few instances dissectinganeurysm resulted from intimal and mediallacerations with subsequent rupture throughthe adventitia after dissections of the arterialwall for varying distances. Surprisingly, veryfew (21) lacerations of the aorta were foundin which the trauma involved only 1 or 2layers of the aortic wall. In these instancesthey were usually small horizontal or longi-tudinal tears involving the intima and occa-sionally extending into the media. Thus in
our series the extent of involvement of theaortic wall varied from a simple subintimalhemorrhage to complete laceration of theaorta. The lesions may be classified as fol-lows: (1) intimal hemorrhage; (2) intimalhemorrhage with laceration; (3) mediallaceration; (4) complete laceration of theaorta; (5) false aneurysm formation; (6)periaortic hemorrhage.An evaluation of the gross and histopatho-
logic features of trauma to the aorta requires
1089
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

PARMLEY, MATTINGLY, MANION, AND JAHNKE
an appreciation not only of the normal micro-scopic structure of the aorta, but also of thepossible pathologic alterations that mighthave preceded the wound. It would be falla-cious to assume that all aortas were free frompathologic change at the time of injury.Indeed, our experience with a large series ofautopsies in a similar age group in whichtrauma was not the cause of death indicatesthat pathologic changes in the aorta, par-ticularly atherosclerosis, are common.
Atherosclerosis was found in our series,but in only 1 instance was it considered to haveadded significantly to the traumatic lesion.However, medial cystic necrosis of minimalto moderate degree in 3 instances probablymade the aorta more vulnerable to unusualstress. Syphilitic involvement of the aortawas noted twice but was not considered afactor in production of the rupture. Inneither of these cases was there aneurysmaldilatation of the aorta. Congenital cardio-vascular defects were not demonstrated inour series.
LESIONS OF THE INTIMAThe lesions involving the intimal layer in
our series may be grouped as (1) intimalhemorrhage and (2) intimal hemorrhage as-sociated with laceration.Intimal HemorrhageAreas of intimal hemorrhage were de-
scribed occasionally in association with fatallesions. They varied in size and often werenoted only on microscopic examination (fig.2A). It is probable that lesions of this typeoccur frequently but are not recognized.
Intimal Laceration with HemorrhageThis lesion differs in that the endothelial
surface of the aorta is broken and the col-lagenous and elastic fibers of the "subendo-thelial layer" of the intima are more severelydisrupted and separated by hemorrhage (figs.2B and 2C). The limiting effect of the internalelastic lamina on the extent of the lacerationof the wall is illustrated in both figures. It islesions of this type that could serve as thenidus of thrombus formation, either bland or
septic, with possible peripheral embolization.The break in the endothelial lining might alsolead to further dissection.
LESIONS OF THE MEDIAThe tunica media forms the bulk of the
aortic wall. The elastic fibers of the mediawith their great tensile strength and theirconcentric lamellar arrangement providemuch of the resiliency of the arterial wall.The smooth muscle fibers provide the con-tractile properties and serve to maintain the"vascular tone," but probably contributerelatively little to the over-all strength ofthe arterial wall. The elastic lamina may befrayed, split, or even destroyed in variousdiseases, such as advanced atherosclerosis orsyphilitic aortitis, and such changes may ren-der it more susceptible to traumatic lacera-tion. The importance of the amorphous inter-cellular substance of the intima and mediahas recently been recognized. It is increasedin amount in atherosclerosis, and accumula-tions of this material, often with focal pool-ing and vacuolization, characterize the lesionsof idiopathic cystic medial necrosis of theaorta. Thus, it would appear that an abnor-mal accumulation of the amorphous intercel-lular substance must be considered in theevaluation of the effect of trauma on theaorta.
Traumatic Medial LacerationsLacerations extending into, but not
through, the tunica media (fig. 2D) were ob-served occasionally in this series. Such lesionswere described at autopsy, usually in associa-tion with other aortic lesions, but sometimesalone. The possibility that a medial lacerationmight lead to further dissection, rupture, orformation of an aneurysm should not beoverlooked.
LESIONS OF THE ADVENTITIAThe tunica adventitia provides a portion
of the tensile strength necessary for the main-tenance of the normal caliber of the aorta, andthrough the medium of the vasa vasorum con-
tributes to the sustenance of the arterial wall.It is vulnerable to systemic and local disease.
1090
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
FIG. 3. (AFIP Ace. 147826). (A) A recent thrombus superimposed on the site of post-traumatic laceration of the aorta. Note the small fragment of aorta on the surface of thethrombus. The laeeratioii extends through the aorta. X 21/2. (B) (AFIP Ace. 714264).Elastic stained section showing a healed false aneurysm of the aorta. Note the abrupttermination of the elastic fibers of the aorta at the site of the traumatic laceration. Thewall of the aneurysmal sac is composed of fibrous and collagenous connective tissue in whichonly a rare degenerating elastic fiber is seen. X 2.
Thus, pathologic processes of the adjacentstructures, particularly benign or malignantlesions affecting lymph nodes and involvingthe adventitia secondarily, should be con-sidered in evaluating any traumatic ruptureof the aorta.The traumatic lesions that involved the
adventitia of the aorta were of 3 types: (1)traumatic false aneurysm formation; (2)complete aortic laceration; (3) periaortichemorrhage.
Traumatic AneurysmsIncluded under this type are all cases in
which aneurysmal bulging of the aortic wallfollowed complete laceration of the intimaand media, and also those in which falseaneurysm formed after rupture of all 3layers. In some instances a distinction be-tween the 2 could not be made with certainty,even on microscopic examination of the wallof the aneurysm.
In cases in which circumferential lacerationof the intima and media was complete, a fusi-form aneurysmal bulging of the wall of theaorta developed, while in those in which onlya portion of the wall was lacerated the bulg-ing appeared as a localized diverticulum orpouch-like formation. The structure variedwith the age or duration of the aneurysm.When a repair operation or postmortem ex-amination was performed soon after injury,the pouch of the aneurysm contained a throm-
bus consisting of fibrin with many enmeshedred blood cells, and usually there was hemor-rhage into adjacent tissue. If the patientsurvived for a few days, the thrombus wassoft and fibroblastic proliferation and earlyvascularization were observed in the wall ofthe aorta. It is at this stage, when the throm-bus is of recent origin, that peripheral em-bolization is likely. With longer survival, thethrombus may become organized and the wallof the pouch lined with endothelial cells.
Complete Laceration of the AortaComplete rupture of the aorta, including
the adventitia and the attached connectivetissue, was the most common lesion found.Usually death was immediate. However, falseaneurysm formation or occlusion of the siteof rupture by thrombus (fig. 3) may permittemporary survival.Periaortic Hemorrhage
Periaortic hemorrhage often accompaniedcomplete rupture or other traumatic lesionsof the aorta, but occasionally occurred in-dependently.
AORTIC RUPTURE WITH SURVIVALIn our series of 275 cases of aortic rup-
ture caused by nonpenetrating trauma theinitial survival rate was 13.8 per cent (table3). Of the 38 patients who survived for vari-ous periods, 2 on whom surgical resection ofa post-traumatic aneurysm was performed are
1091
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from
PARMLEY, MATTINGLY, MANION, AND JAHNKE
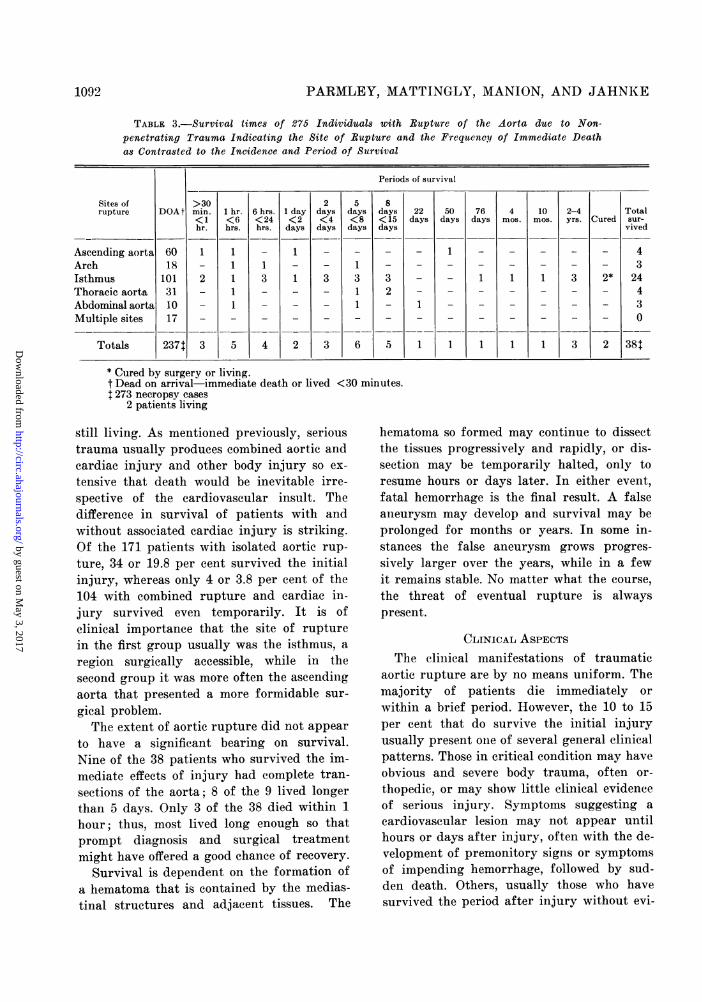
TABLE 3.-Survival times of 275 Individuals with Rupture of the Aorta due to Non-penetrating Trauma Indicating the Site of Rupture and the Frequency of Immediate Deathas Contrasted to the Incidence and Period of Survival
Sites ofrupture
Ascending aortaArchIsthmusThoracic aortaAbdominal aortaMultiple sites
Totals
DOA t
6018
101311017
2371
Periods of survival
>30min.<1hr.
1
2
3
1 hr.<6hrs.
11111
5
6 hrs.<24hrs.
13
4
1 day<2days
1
1
2
2days<4days
3
3
5days<8days
1311
6
8days<15days
32
5
* Cured by surgery or living.t Dead on arrival immediate death or lived <30 minutes.t 273 necropsy cases
2 patients living
22days
1
50days
1
1
still living. As mentioned previously, serioustrauma usually produces combined aortic andcardiac injury and other body injury so ex-
tensive that death would be inevitable irre-spective of the cardiovascular insult. Thedifference in survival of patients with andwithout associated cardiac injury is striking.Of the 171 patients with isolated aortic rup-
ture, 34 or 19.8 per cent survived the initialinjury, whereas only 4 or 3.8 per cent of the104 with combined rupture and cardiac in-jury survived even temporarily. It is ofclinical importance that the site of rupturein the first group usually was the isthmus, a
region surgically accessible, while in thesecond group it was more often the ascendingaorta that presented a more formidable sur-
gical problem.The extent of aortic rupture did not appear
to have a significant bearing on survival.Nine of the 38 patients who survived the im-mediate effects of injury had complete tran-
sections of the aorta; 8 of the 9 lived longerthan 5 days. Only 3 of the 38 died within 1
hour; thus, most lived long enough so that
prompt diagnosis and surgical treatment
might have offered a good chance of recovery.Survival is dependent on the formation of
a hematoma that is contained by the medias-
tinal structures and adjacent tissues. The
hematoma so formed may continue to dissectthe tissues progressively and rapidly, or dis-section may be temporarily halted, only toresume hours or days later. In either event,fatal hemorrhage is the final result. A falseaneurysm may develop and survival may beprolonged for months or years. In some in-stances the false aneurysm grows progres-
sively larger over the years, while in a fewit remains stable. No matter what the course,
the threat of eventual rupture is alwayspresent.
CLINICAL ASPECTSThe clinical manifestations of traumatic
aortic rupture are by no means uniform. Themajority of patients die immediately or
within a brief period. However, the 10 to 15per cent that do survive the initial injuryusually present one of several general clinicalpatterns. Those in critical condition may haveobvious and severe body trauma, often or-
thopedic, or may show little clinical evidenceof serious injury. Symptoms suggesting a
cardiovascular lesion may not appear untilhours or days after injury, often with the de-velopment of premonitory signs or symptomsof impending hemorrhage, followed by sud-den death. Others, usually those who havesurvived the period after injury without evi-
1092
76days
1
4mos.
1
1
10mos.
1
1
2-4yrs.
3
3
Cured
2*
2
Totalsur-vived
4324430
38t
1 1 A A~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
dence to suggest aortic injury, may exhibitthe signs and symptoms of aortic aneurysmwith impending rupture weeks or monthslater; or, in the absence of significant symp-toms, aortic aneurysm formation may be re-vealed by a routine chest roentgenogram.Rarely, aneurysm with dissection may followtraumatic aortic injury of this type. 17 Anunusual complication is subacute bacterialendaortitis, which has been reported byStryker.13
Failure to diagnose the aortic rupturewhile the patient is still alive is the chiefobstacle to proper treatment. In 12 of the 38cases in this series, the correct diagnosis wasconsidered before death, in 9 because anaortic aneurysm was demonstrable by roent-genogram. This diagnosis is seldom consideredin the early postinjury period because of themistaken concept that a patient could rarely,if ever, survive such a lesion. The realizationthat this concept is false will remove themajor impediment to diagnosis.
Unfortunately, there are no clear-cut earlydiagnostic features of aortic rupture. Thepatient 's vascular injury is usually over-looked and the more obvious injuries areproblems for the orthopedic or neurologic sur-geon. Eighteen, or 47 per cent of the 38patients, had a history of unconsciousness forvarying periods of time. Twenty-seven hadfractures other than of the ribs, usually ofan extremity, and many died from unsus-pected aortic rupture during or soon afterorthopedic treatment. Fractures of the dorso-lumbar vertebrae were found in 34 of theentire series of patients, and in 29 the rupturewas definitely related to the site of fracture.Possible aortic rupture should be consideredin every patient incurring a dorsolumbarvertebral fracture in a serious accident.
External evidence of chest injury was help-ful in arousing suspicion of possible cardio-vascular damage, but was often absent evenwhen cardiovascular damage was extensive(fig. 1B). In a review of all cases of aorticrupture from this standpoint it was foundthat 101, or 36 per cent of the 275, had mini-mal or no external evidence of chest injury,
FIG. 4. (AFIP Acc. 709699). (Case 3). Postero-anterior chest roentgenogram demonstrating widen-ing of the mediastinum in a patient who had incurredan almost complete transection of the ascending aorta.
despite the high incidence of rib fracture.Although many patients were in shock
initially, blood pressure was within normalrange in 10 and became normal in an addi-tional 19 soon after measures to combat shockwere instituted. Rarely were there any spe-cific symptoms or signs of cardiovascular in-jury. Chest or abdominal pain, dyspnea,tachycardia, hemoptysis, and cyanosis werethe more common clinical manifestations.These signs and symptoms were most oftenattributed to other injuries, frequently toassociated pulmonary lesions.Unexplained hemorrhage and hemothorax
with roentgenographic evidence of wideningof the mediastinum are the early manifes-tations of diagnostic importance. The earlyroentgen signs of rupture of the aorta haverecently been described.19 The most importantis widening of the mediastinum (fig. 4). Usu-ally there is associated hemothorax that maybe present early or may be delayed. Fracturesof the thoracic cage are common, despite a
lack of external evidence of injury. Clinicaland laboratory evidence of unexplained
1093
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

PARMLEY, MATTINGLY, MANION, AND JAHNKE
hemorrhage has in several instances led to ex-
ploratory laparotomy on the assumption thatcontinuing blood loss was due to hepatic or
splenic laceration. The possibility of aorticrupture must always be considered in suchcircumstances.
After the first 24 hours have passed andthe patient 's condition becomes stable, theprobabilities for diagnosis are greatly im-proved. The signs and symptoms of aorticrupture then resolve into those produced bya mediastinal mass, the hematoma or falseaneurysm, and the tendency of this aneurysm
to leak blood. This often produces a delayedor recurrent hemothorax, which is the one
most important diagnostic feature. Failureto recognize its importance is disastrous, sincefatal rupture soon follows. Frequently asso-
ciated with this finding, although it may
occur independently, is the recurrence or ag-
gravation of chest pain caused by furtherdissection of mediastinal structures andpleura by the enlarging hematoma. The ap-
pearance of dysphagia, evidence of trachealor bronchial obstruction, vena caval obstruc-tion, or the development of hoarseness havebeen encountered in patients of this series.Impending rupture of the aneurysm into a
bronchus may be heralded by hemoptysiswith or without associated hemothorax.Roentgenographic examination of the chest
at this time may demonstrate that a pre-
viously nonspecific widening of the media-
stinum now appears as a mass. In one patientof this series, enlargement of the aneurysm
was delayed sufficiently long after the acci-
dent to suggest a rapidly growing lymphomaor abscess. In other instances, the false
aneurysm may remain relatively stable for a
prolonged period before evidence of second-
ary rupture appears. In some cases ruptureoccurs without prior warning and is cata-
strophic in extent.Diagnosis of aortic rupture is easiest in
those instances in which a false aneurysmdevelops and then remains stable and asymp-tomatic. Routine x-ray examination of the
chest is almost always the means wherebydiagnosis is made. This was the circumstance
in 9 of the patients of this series. The etiologyof the aneurysm is suggested when the pasthistory is evaluated in the light of the roent-gen finding.
Three cases of the series emphasize theclinical and pathologic features most com-monly encountered.
Case 1. AFIP Aeo. 128610: This 20-year-oldwhite man sustained a comminuted fracture of theclavicle and an acromioclavicular separation onthe right when the truck in which he was ridingoverturned. There was no other obvious injuryand the orthopedic injuries were repaired. Roent-gen examination of the chest 1 month later revealedconsiderable widening of the upper mediastinum,primarily to the right. Repeated roentgen studiesdemonstrated progressive increase of this widen-ing. Forty-eight days after the injury, evidenceof superior vena caval and respiratory obstructiondeveloped with increasingly severe chest pain.Within 24 hours the signs of superior vena cavalobstruction were pronounced and the patient wasorthopneic with an audible stridor. Within thenext 24 hours asphyxia was imminent. Bronchos-copy revealed marked compression of the lowertrachea. An emergency thoracotomy was per-formed, and the aneurysm of the aortic arch thatwas found ruptured spontaneously during opera-tion. Death occurred 50 days after injury. Atnecropsy a defect large enough to admit the indexfinger was noted in the right posterior aortic walljust proximal to the innominate artery. Themargins of the defect were smooth and coveredwith endothelium and communicated with a "false"aneurysmal sac approximately 7 em. in diameterlying to the right of the superior mediastinum.The sac was filled with partially organizedthrombus and was surrounded by considerablefibrosis and edema. The underlying superior venacava and lower end of the trachea were compressedby the aneurysm. In the right lateral wall of theaneurysmal sac a large tear communicated withthe right pleural cavity, which was filled withblood.Comment. This patient is typical of those
in whom orthopedic injuries dominate theclinical picture and vascular injury is notsuggested. As in this patient, progressivewidening of the mediastinum may be seen
in the roentgenograms days after the injury.The rapid development of obstructive symp-toms signals the rupture of the aneurysmalsac.
Case 2. AFIP Ace. 639151: This 23-year-oldwhite man was pinned under a wrecked automobile.
1094
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
FIG. 5. (AFIP Acc. 639151). (Case 2). Left, A. Gross specimen of heart and lungsdemonstrating complete transverse horizontal rupture of the aorta 8 mm. below the left sub-clavian artery in the anterior view (sections for study removed just below site of rupture);and a 6 by 5 by 4 cm. false aneurysm contained by pleura, most clearly seen in the posteriorview. Right, B. The aneurysm incorporated the recurrent laryngeal nerve. The site ofrupture of the aneurysm through a 1.5 cm. rent in the pleura may be seen.
On admission to the hospital, he complained ofpain in the right side of the chest and the leftthigh. Blood pressure was 105/65, pulse 90 permain., and respiration 20 per min. A few raleswere heard in the right lung. There were abra-sions of the chest, fractures of the sixth andseventh ribs on the left, and the third, fourth,and fifth on the right, and a compound comminutedfracture of the left femur. The patient wasgiven a whole-blood transfusion and the compoundfracture was treated surgically. Postoperativelyand until 6 days later the patient did well. Thenhis temperature rose to 101F., and tachycardiaand dyspnea appeared. Because of dulness andabsence of breath sounds on the right, thoracentesiswas performed with recovery of 500 ml. of blood.The patient became cyanotic, but oxygen therapybrought relief. Hoarseness developed. During thecourse of the next 24 hours he was given 1,500ml. of whole blood and by the end of this periodthe temperature returned to normal and his breath-ing was normal. Blood pressure was normal andthere were no physical signs of hemiothorax. How-ever, on the eighth day after injury he suddenlydied. Review of chest x-rays taken during hospitali-zation revealed no definite abnormalities excepthemothorax. At necropsy a complete horizontaltransverse rupture of the aorta, 8 mm. below theorigin of the left subelavian artery, was surroundedby a large hematoma forming a false aneurysm6 by 5 by 4 cm. that was contained by the pleura
(fig. 5). The recurrent laryngeal nerve was in-corporated in this hematoma. A rent 1.5 cmn.long in the parietal pleura that contained theaneurysm accounted for the massive hemorrhage,which produced left hemothorax of 4,200 mil.Comment. This is an example of the patient
who has no obvious signs or symptoms ofaortic rupture when seen initially. The pres-ence of other injury, usually orthopedic, isthe obvious and immediate problem. Hoursor days later the sudden development ofIhemothorax is the sign that there is impend-hlg rupture of a heretofore silent falseaneurysm. Delayed hemothorax appearingsuddenly after injury and for no apparentreason should always suggest the presence ofa traumatic false aneurysm of the aorta.
Case 3. AFIP Ace. 709699: This 24-year-oldwhite man was the driver of a car involved in ahead-on collision. On admission to the hospital,2 hours later, he was alert and stated that heh1ad not been unconscious. The blood pressurewas 55,/40 but rose to 150/70 after administrationof 1,000 miil. of dextran. Whole-blood transfu-sion of 500 mil. was then given. Physical exam-
ination revealed abrasions of the face, anteriorchest, and lacerations of the extremities. Breathsounds were diminished on the right and the
1095
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from
PARMLEY, MATTINGLY, MANION, AND JAHNKE
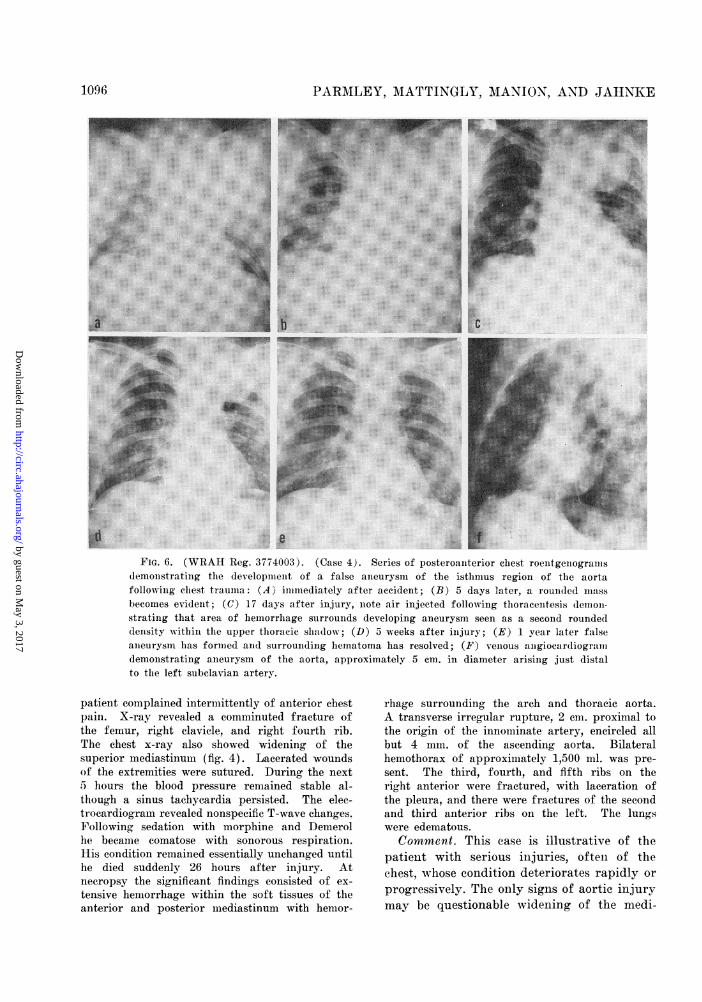
FIG. 6. (WRAH Reg. 3774003). (Case 4). Series of posteroanterior chest roentgenogranisdemonstrating the development of a false aneurysm of the isthmus region of the aortafollowing chest trauma: (A' immediately after accident; (B) 5 days later, a rounded massbecomes evident; (C) 17 days after injury, note air injected following thoracentesis demoni-strating that area of hemorrhage surrounds developing aneurysm seen as a second roundeddensity within the upper thoracic shadow; (D) 5 weeks after injury; (E) 1 year later falseaneurysm has formed and surrounding hematoma has resolved; (F) venous ammgiocardiogralndemonstrating aneurysm of the aorta, approximately 5 cm. in diameter arising just distalto the left subclavian artery.
patient complained intermittently of anterior chestpain. X-ray revealed a comminuted fracture ofthe femur, right clavicle, and right fourth rib.The chest x-ray also showed widening of thesuperior mediastinum (fig. 4). Lacerated woundsof the extremities were sutured. During the next5 hours the blood pressure remained stable al-though a sinus tachycardia persisted. The elee-trocardiogram revealed nonspecific T-wave changes.Following sedation with morphine and Demerolhe became comatose with sonorous respiration.His condition remained essentially unchanged untilhe died suddenly 26 hours after injury. Atneeropsy the significant findings consisted of ex-tensive hemorrhage within the soft tissues of theanterior and posterior mediastinum with hemor-
rhage surrounding the arch and thoracic aorta.A transverse irregular rupture, 2 cm. proximal tothe origin of the innominate artery, encircled allbut 4 mm. of the ascending aorta. Bilateralhemothorax of approximately 1,500 ml. was pre-sent. The third, fourth, and fifth ribs on theright anterior were fractured, with laceration ofthe pleura, and there were fractures of the secondand third anterior ribs on the left. The lungswere edematous.Comment. This case is illustrative of the
patient with serious injuries, often of thechest, whose condition deteriorates rapidly orprogressively. The only signs of aortic injurymay be questionable widening of the medi-
1096
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

X\'ONPENETRATING INJURY OF THE AORTA
astinunni roentgeilologically and shock or otherevidence of hemlorrhage.
MANAGEMENT01e the diagnosis of rupture of the aorta
is uiade, surgical treatment must be con-sidered. The surgical technics employed havebeen well established.33' 40, 41 Review of theavailable literature reveals 8 reportedcases23' 26-28, 30, 31, 3 of traumatic aorticaneurysm successfully treated by resection.Two additional cases treated by resction andhomograft replacement are included in ourseries. The progression of aortic rupture froma massive hematoma to the formation of awell-defined false aneurysm is well illustratedin these 2 cases.
Case 4. WIRAH Reg. No. 3774003: This 27-year-old white soldier incurred a steering wheelinjury to the chest and a fracture of the rightpatella in an automobile accident on December 6,1953. He was hospitalized immediately and placedin an oxygen tent because of dyspnea. Multiplerib fractures were found on the left side. Trans-fusions were required because of blood loss dueto the development of a left hemnothorax, whichwas considered to be an extrapleural hemlorrhage(fig. 6A-D). This was treated by thoracentesis.Following operation for the patellar fractureperformed on December 17, hoarseness developedbut cleared after 3 weeks. The patient was re-turned to duty but because of repeated symptomsreferable to his knee was rehospitalized in Novem-ber 1954. On direct questioning the patientadmitted to slight exertional dyspnea, a mildnonproductive cough, and a pulling sensation inthe chest, which he had ignored. A routine chestroentgenogram revealed a left superior mediastinalmass considered to be an aneurysm of the aorta,presumably traumatic (fig. 6E). Chest x-raystaken before the automobile accident were reviewedand found normal. Physical examination revealedan increased pulsation of the suprasternal notchand widening of the cardiac base on percussionbut no other cardiovascular abnormalities. Bloodpressures were 130/90 in the right arm, 134/94in the left arm, and 144/110 in the left leg.Laboratory studies including the serologic testsfor syphilis were normal. The electrocardiogramwas normal. A venous angiocardiographic studyrevealed an aneurysm approximately 5 cmn. indiameter involving the aorta just below the sub-elavian artery (fig. 6F). On May 31, 1955, thepatient was operated on by one of us (E.J.).The aneurysm arose just distal to the left sub-
FIG. 7. (WRAH Reg. 3774003) (Case 4). Falseaneurysmn as it appearedl at time of surgery (Top, A);and (Bottom, B) aorta follow-ing resection and llomno-graft replacement.
clavian cartery and was approximately S cmii. inlength and 7 cmi. in width. Under en(dlotrahelealanesthesia, and hv potheleiai the canieurv\'smmi was
resected and the defect w'as repaired with a 6-cm.homologous aortic graft (fig. 7). The patientdid well postoperativrely and was later dischargedfroml amilitary service in good condition.
Case 5). WVRAtH Re-. No. 4017011: This 20-year-old white man fell asleep at the wheel ofhis automobile in October 1955 and the car raninto a tree. He remiailed unconscious an(l inshock for 3 hours. Later he complained of head-ache, pain in the left side of the chest and back,and paimi and numbness below the left knee.Epistaxis and vomiting of bloody immaterial oe-curred. Chest roentgenograms -revealed a left
109,1
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

PARMLEY, MATTINGLY, MANION, AND JATINKE
FIG. 8. (WRAH Reg. 4017011) (Case 5). Postero-anterior chest roentgenogram prior to surgery demon-strating the aortic aneurysm of the isthmus regionand associated fibrothorax.
pneumothorax and a small right pneumothoraxwith atelectasis and fractures of the fourth leftand sixth right ribs. X-ray evidence of consolida-tion of the left lower lobe appeared later andthe patient continued to run a low-grade fever.It was believed that an organizing fibrothorax(fig. 8) had developed on the left, and on Novemi-ber 9, 1955, a left thoracotomy was performed
and decortication was accomplished. An aneurysmof the isthmus region was noted, but at that timesurgical correction was not considered feasible.The patient was transferred to Walter Reed ArmyHospital. Physical examination there revealedblood pressure of 128/90 in the upper extremitiesand 130/90 in the lower extremity. Expansionof the left hemithorax was reduced and breathsounds in the lower lung field posteriorly weredecreased. At a site just medial to the left scap-ular border a systolic bruit was heard. A similarbruit was heard anteriorly only with the patientsitting and leaning forward in full expiration.Results of laboratory studies were normal. OnJanuary 24, 1956, under general oxygen-etherendotracheal anesthesia with hypothermia, theaneurysm was identified just distal to the leftsubelavian artery. It was 7 em. in length and5 to 6 em. in width. Resection of the aneurysmwas completed and a 7-cm. fresh aortic homograftwas used to bridge the resulting defect (fig. 9).The postoperative course was uneventful, and thepatient was discharged from the hospital inexcellent condition.
Ten other patients in this series wereoperated upon for various reasons. Some wereknown to have an aortic aneurysm, othersunderwent thoraeotomy because of unex-plained and persistent thoracoabdominal
FIG. 9. (WRAH Reg. 4017011). (Case 5). Left, A. Photographs obtained at time ofthoracotomy demonstrating false aneurysm of the aorta just below the left subclavian artery.Right, B. The homograft in place following resection of the aneurysm.
1098
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
hemorrhage or an enlarging mediastinal massof unknown nature. In only 3 instances wasoperation performed soon after the injury.In the other 7 cases treated surgically thepatients had survived from 10 weeks to 4years, and definite aneurysm formation de-monstrable by x-ray made the diagnosis cer-tain. In 1 case that has been reported indetail,23 the postoperative course was com-plicated by an esophageal pleural fistula andthe aortic homograft ruptured at its proximalanastomosis 3 days postoperatively. One pa-tient, whose case is also reported elsewhere,14underwent exploratory thoracotomy only tohave the aneurysm declared inoperable. Fourother patients died during or after thoraco-tomy from complications of a prolonged sur-gical procedure. The seventh patient (case 1)underwent late exploratory thoracotomy withrupture of the aneurysm.
If the patient is in extremis when firstseen, even a reasonable certainty of diagnosiswould rarely justify exploratory thoracotomy.However, in a traumatized patient who isconsidered to be in relatively good conditionand who demonstrates a widened mediastinumon roentgen study, delayed or recurrent he-mothorax, or other evidence of unexplainedhemorrhage, the diagnosis of aortic ruptureand the need for thoracotomy must beseriously considered.
Those individuals in whom a traumaticaortic aneurysm may be demonstrated to bepresent late in the period after injury andwho are otherwise in good condition should,with present day surgical technics, be con-
sidered candidates for surgical correction ofthe aneurysm. However, it has recently beenemphasized36 that the natural course of trau-matic aortic aneurysms may be prolongedand before surgical treatment is decided uponits risks must be carefully evaluated.
SUMMARY AND CONCLUSIONS
A review of 296 cases of nonpenetratingtraumatic injury resulting in aortic lacera-tion in 21 and rupture in 275, indicates thatthis lesion should be suspected more frequent-ly in the traumatized individual.
Study of the causation and the pathologyof this aortic injury demonstrates that thecommonest site of rupture in this series is atthe aortic isthmus, just distal to the left sub-clavian artery; 45 per cent or 124 occurredat this site.Almost one fifth of all individuals who
sustain traumatic aortic rupture withoutassociated cardiac lesions may be expected tosurvive at least temporarily. The over-allsurvival rate in our series was 13.8 per cent(38 of 275 cases) but this figure includedthose with associated cardiac injury.A review of the clinical features of the
survivors emphasizes that external evidenceof trauma may be minimal and initial evi-dence of definite cardiovascular injury maybe lacking. Roentgen signs of a widenedmediastinum, evidence of persistent thoraco-abdominal hemorrhage, and the appearanceof delayed hemothorax are shown to be earlydiagnostic criteria of aortic rupture.Prompt diagnosis of traumatic aortic rup-
ture is essential if surgical treatment is to beperformed before fatal sequelae develop. Sur-gical treatment of a traumatic aortic aneu-rysm that is producing no symptoms and hasbeen demonstrated to have remained un-changed over a period of years should be ap-proached only after careful consideration.Successful surgical resection of a traumaticaortic aneurysm in 2 patients is reported.
ADDENDUM
Since the preparation of this paper 3 additionalpatients with thoracic aorta aneurysms due tononpenetrating trauma have been evaluated atWalter Reed Army Hospital. Retrograde aortog-raphy was demonstrated to be the most effectiveroentgenographic means of delineating the extentof these lesions. Two of these patients under-went surgical treatment. In the one the aneurysmcould not be resected because it involved the archof the aorta and its major vessels; the patientdied at the time of operation. In the other, whosefalse aneurysm was a result of almost completetransection of the aorta at the isthmus region,resection with homograft replacement was success-ful. The operation was performed by means ofpartial bypass from left atrium to femoral arterywith sigmamotor pump.
1099
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

PARMLEY, MATTINGLY, MANION, AND JAHNKE
SUMMARIO IN INTERLINGUA
Un revista de 296 casos de non-penetrante
traumatisation que resultava in lacerationaortic in 21 e in ruptura aortic in 275 casos
indica que iste lesion deberea esser suspiciteplus frequentemente in individuos tramma-
tisate.lie studio del causas e del pathologia de
iste typo de vulneration del aorta demonstraque in le serie presente le plus commun sitodel ruptura es le isthmo aortic, justo distal alarteria sinistro-subelavian. Isto valeva in 124o 45 pro cento del casos.
On pote expectar que quasi un quinto deomne individuos que suffre un traumatic rup-
tura aortic sin associate lesiones cardias va
superviver al minus temporarimente. In nostreserie le superviventia total amontava a 13.8pro cento (i.e. 38 ex 275 casos), sed iste cifraincludeva le casos con associate lesiones car-
diac.Un revista del aspectos clinic del super-
viventes indica que le evidentia externe detrauma pote esser minimal e que al initioomne evidentia de un lesion cardiovasculardefinite pote esser absente. Es monstrate qu2
signos roentgenographic de allargamentomediastinal, manifestationes de persistentehemorrhagia thoraco-abdominal, e le appari-tion de un retardate hemothorace es precoce
criterios diagnostic de ruptura aortic.5. Le prompte diagnose de un traumatic
ruptura del aorta es essential si on vole que
le intervention chirurgic pote esser effectuateante le disveloppamento de sequellas mortal.lie tractamento chirurgic de un traumaticaneurysmo aortie que produce nulle symp-
tomas e que es demonstratemente inalteratedepost plure annos es un interprisa que re-
quire le plus circumspecte consideration de
omne factores involvite. Es reportate 2 casos
de successo in resection chirurgic de trau-
matic aneurysmos aortic.
REFERENCES
1. SAILER, S.: Dissecting aneurysm of the aorta.Arch. Path. 23: 704, 1942.
2. KUHN, L. P.: Traumatic rupture of thoracicaorta with review of fifty-five abdominalinjuries. Illinois M. J. 47: 420, 1925.
3. STRASSMANN, G.: Traumatic rupture of theaorta. Am. Heart J. 33: 508, 1947.
4. SHENNAN, T.: Traumatic (false) aneurysmof the aorta. J. Path. & Bact. 32: 795, 1929.
5. SAMSON, P. C.: Dissecting aneurysms of theaorta, including traumatic type: Three casereports. Ann. Int. Med. 5: 117, 1931.
6. WILSON, H., AND ROOME, N. W.: Traumaticshock syndrome following rupture of aortaand multiple fractures. Am. J. Surg. 22:333, 1933.
7. HAWKES, S. Z.: Traumatic rupture of heartand intrapericardial structures. Am. J.Surg. 27: 503, 1935.
8. CORBITT, R. W., AND MATTHEWS, A. R. K.:Rupture of the aorta. West Virginia M. J.33: 372, 1937.
9. COLLINS, J. 0., AND D'ALESSIO, C. M.: Trau-matic rupture of the thoracic aorta. NewEngland J. Med. 219: 229, 1938.
10. RICEN, E., AND DICKENS, P. F., JR.: Trau-matic aneurysm of the abdominal aorta of27 years duration: Case report. U. S. Nav.M. Bull. 40: 692, 1942.
11. FORBES, G.: Traumatic rupture of aorta. Brit.M. J. 2: 400, 1944.
12. TANNENBAUM, I., AND FERGUSON, J. A.: Rapiddeceleration and rupture of the aorta. Arch.Path. 45: 503, 1948.
13. STRYKER, W. A.: Traumatic saccular aneu-rysm of the thoracic aorta. Am. J. Clin.Path. 18: 152, 1948.
14. HENNING, B. H., AND AGMAR, A. R.: Trau-matic rupture of thoracic aorta: Report ofcase. Mil. Surgeon 103: 260, 1948.
15. BRADFORD, B. JR., AND JOHNSTON, F. L.:Traumatic rupture of the aorta: Report ofa case in which the patient survived foreighty-one days. Surgery 28: 893, 1950.
16. RICE, W. G., AND WITTSTRUCK, K. P.: Acutehypertension and delayed traumatic rup-ture of the aorta. J.A.M.A. 147: 915, 1951.
17. LEONARD, D. W.: Dissecting aneurysm of theaorta due to trauma. Am. J. Surg. 69:344, 1951.
18. HOLLINGSWORTH, R. K., JOHNSON, W. W.,AND MCCOOEY, J. F.: Traumatic saccularaneurysm of the thoracic aorta. J. ThoracicSurg. 24: 325, 1952.
19. WYMAN, A. C.: Roentgenologic diagnosis oftraumatic rupture of the thoracic aorta.Arch. Surg. 66: 656, 1953.
20. KASTL, W. H.: Traumatic rupture of thethoracic aorta. Ann. Surg. 137: 111, 1953.
21. RODDA, R.: A case surviving six months aftertraumatic rupture of the aorta. J. Clin.Path. 6: 145, 1953.
22. JAY, J. B., AND FRENCH, S. W.: Traumaticrupture of the thoracic aorta. Arch. Surg.68: 657, 1954.
1100
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

NONPENETRATING INJURY OF THE AORTA
23.iEBAKEY, M. X,., AND COOLEY, D. A.: Suc-cessful resection of aneurysm of distalaortic arch and replacement by graft.J.A.AI.A. 155: 1398, 1954.
24. GOYETTE, E. M., BLAKE, H. A., FORSEE, J. H.,AND SWAN, H.: Traumatic aortic aneu-
rysms. Circulation 10: 824, 1954.25. WARE, P. F., ADLER, R. H., AND LYTER, C. S.:
Traumatic aneurysm of the thoracic aorta.U. S. Armed FDrces M. J. 6: 1674, 1955.
26. ADAMS, H. D.: Shunt graft with resectionfor aneurysm of arch of aorta. J.A.M.A.159: 1195, 1955.
27. STRANAHAN, A., ALLEY, R. D., SEWELL, W.H., AND KAUSEL, H. W.: Aortic arch re-section and grafting for aneurysm employ-ing an external shunt. J. Thoracic Surg. 29:54, 1955.
28. JULIAN, 0. C., GROUSE, W. J., DYE, X. S.SADOVE, M. S., JAVID, H., AND ROSE, R. F.:Hypotension and hypothermia in surgery
of the thoracic aorta. Arch. Surg. 70: 729,1955.
29. ZEHNDER, M. A.: Delayed post-traumiatic rup-
ture of the aorta in a young healthy indi-vidual after closed injury: Mechanical-etiological considerations. Angiology 7:252, 1956.
30. STOREY, C. F., NARDI, G. L., AND SEWELL, W.H.: Traumatic aneurysm of the thoracicaorta: Report of two cases, one success-fully treated by resection and graft re-placement with aid of a shunt. Ann. Surg.144: 69, 1956.
31. DEBAKEY, M. E.: Personal communication toStorey.`
32. WEISEI, W., HUTTNER, W. A., AND BECHER,I. A.: Unusual aortic arch nonluetic aneu-
rysm$; surgical treatment. Wisconsin Al. J.50: 866, 1951.
33. BAHNSON, H. T.: Definitive treatment of sac.cular aneurysms of the aorta with excisionof sac and aortic suture. Surg., Gynee. &Obst. 96: 383, 1953.
34 HOLMEs, T. W. JR., AND NETTERVILLE, R. E.:Complications of first rib fracture, includ-ing one case each of tracheoesophageal fis-tula and aortic arch aneurysm. J. ThoracicSurg. 32: 74, 1956.
35. HARDIN, C. A.: Resection and orlon graft ofmultiple aortic aneurysms due to trauma.J. Thoracic Surg. 32: 251, 1956.
36. STEINBERG, I.: Chronic traumatic aneurysmof the thoracic aorta: Report of five cases,with a plea for conservative treatment. NewEngland J. Med. 257: 913, 1957.
37. KLOTZ, 0., AND SIMPSON, W.: Spontaneousrupture of the aorta. Am. J. M. Sc. 184:455, 1932.
38. OPPENHEIM, F.: Gibt es eine spontane rupturdes gesunden aorta und wie kommt dieZustande. Miinchen. med. Wchnschr. 65:1234, 1918 cited by Zehnder."
39. HASS, G. ar.: Types of internal injuries ofpersonnel involved in aircraft accidents.J. Aviation M. 15: 77, 1944.
40. DEBAKEY, M. E., COOLEY, D. A., AND CREECH,0. JR.: Aneurysm.-s and occlusive diseasesof the aorta: Analysis of 203 cases treatedby resection and homograft replacement.Henry Ford Hospital International Symn-posium on Cardiovascular Surgery. Phila-delphia, W. B. Saunders Co., 1955, p. 468.
41. COOLEY, D. A., DEBAKEY, _M. E., AND CREECH,0. JR.: Surgical treatment of aortic aneu-rysms. Am. Surgeon 22: 1043, 1956.
'I,Gordon, R. S., Jr.: Unesterified Fatty Acid in Human Blood Plasma. II. The Trans-
port Function of Unesterified Fatty Acid. J. Clin. Invest. 36: 810 (June), 1957.A new method has been developed to determine the unesterified fatty acids in blood
pllasmna. This technic has been used in these experiments. During a fast arteriovenousdifferences were observed. These indicated a net transport of fatty acid from fat tissueto heart, voluntary muscle and viscera. Amnino acids given during a fast had a similarsmaller effect. The suggestion is made that adipose tissue releases more or lessunesterified fatty acids into the blood to preserve "caloric homiieostasis." A mechanismthat is sensitive to the availability of nonfat calories seems to exist, which controlsthe release of unesterified fatty acids.
OPPENHEIMER
1101
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from

GEN., WILLIAM C. MANION and EDWARD J. JAHNKE, JR., MAJ.LOREN F. PARMLEY, LT. COLONEL, THOMAS W. MATTINGLY, BRIG.
Nonpenetrating Traumatic Injury of the Aorta
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1958 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.17.6.10861958;17:1086-1101Circulation.
http://circ.ahajournals.org/content/17/6/1086located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 3, 2017
http://circ.ahajournals.org/D
ownloaded from