non-surgical treatments for urinary incontinence in adult women: diagnosis and comparative...
TRANSCRIPT

Non-surgical Treatments for Urinary Incontinence in Adult
Women:Diagnosis and Comparative
Effectiveness Prepared for:
Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov

Introduction to urinary incontinence (UI) diagnosis and treatment
Systematic review methods The clinical questions addressed by the comparative
effectiveness review (CER) Synthesis of results from studies of diagnostic methods
and patient goals for treatment Results of studies and evidence-based conclusions
about effectiveness and adverse effects of non-surgical treatments for UI
Gaps in knowledge and future research needs What to discuss with patients and their caregivers
Outline of Material
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

UI (the involuntary leakage of urine) affects women of all ages, but its prevalence increases with age. 25% of younger women 44–57% of women at middle-age or postmenopause 75% of older women in nursing homes
UI presents physical, psychological, and social burdens that can range from mildly bothersome to debilitating. 6% of nursing home admissions of women are directly
attributable to UI management. The costs of UI care averaged $19.5 billion in 2004.
The Burden of Urinary Incontinence
Abrams P, Anderson KE, Birder L, et al. Neurourol Urodyn 2012;29(1):213-40. PMID: 20025020.
Anger JT, Saigal CS, Madison R, et al. J Urol 2006 Jul;176(1):247-51; discussion 51. PMID: 16753411.
Boyington JE, Howard DL, Carter-Edwards L, et al. Nurs Res. 2007 Mar-Apr;56(2):97-107. PMID 17356440.
Carls C. Urol Nurs 2007 Feb;27(1):21-4, 39. PMID: 17390923.
Kinchen KS, Lee J, Fireman B, et al. J Womens Health (Larchmt) 2007 Apr;16(3):415-22. PMID: 17439386.
Morrison A, Levy R. Value Health 2006 Jul-Aug;9(4):272-4. PMID: 16903997.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The types of UI are classified based on underlying pathophysiology.
The three types are: Stress incontinence Urgency incontinence Mixed incontinence
The International Urogynecological Association (IUGA)/International Continence Society (ICS) has developed definitions of the types of UI.
Characterizing UI
Haylen BT, de Ridder D, Freeman RM, et al. Neurourol Urodyn 2010;29(1):4-20. PMID: 19941278.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Stress incontinence results from sphincter failure during increases in intra-abdominal pressure. For example, when sneezing, coughing,
or laughing or with physical exertion. Stress incontinence is the most prevalent
type. One-third of adult women (ages 19–64)
are affected
Stress Incontinence
Haylen BT, de Ridder D, Freeman RM, et al. Neurourol Urodyn 2010;29(1):4-20. PMID: 19941278.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Urgency incontinence is the involuntary loss of urine associated with a sudden, compelling urge to void that is difficult to defer.
The underlying cause is typically involuntary contractions of the detrusor muscle in the bladder wall (overactive bladder).
The prevalence of urgency UI among women increases with age: 13% of women up to 44 years of age 17% of women 45–64 years of age 25% of women older than 65
Urgency Incontinence
Haylen BT, de Ridder D, Freeman RM, et al. Neurourol Urodyn 2010;29(1):4-20. PMID :19941278.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Mixed UI: Characteristics of both stress and urgency UI are present.
33% of older women report mixed UI.
Mixed UI
Haylen BT, de Ridder D, Freeman RM, et al. Neurourol Urodyn 2010;29(1):4-20. PMID: 19941278.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Known risk factors include: Age Pregnancy Vaginal delivery, caesarian section Menopause Hysterectomy Obesity Chronic cough Constipation Urinary tract infections Functional impairment Cognitive impairment
Risk Factors for UI
Shamliyan T, Wyman J, Bliss DZ, et al. Evid Rep Technol Assess (Full Rep) 2007 Dec;(161):1-379. PMID: 18457475.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Assessment begins with exclusion of transient UI due to underlying reversible causes not related to sphincter failure or overactive bladder, including: Pelvic organ prolapse Urinary tract infection Poor bladder emptying Voiding dysfunction (e.g., urine retention) Neurogenic causes (injury, stroke)
Approaches to Diagnosis of UI (1 of 3)
Abrams P, Anderson KE, Birder L, et al. Neurourol Urodyn 2012;29(1):213-40. PMID: 20025020.
Haylen BT, de Ridder D, Freeman RM, et al. Neurourol Urodyn 2010;29(1):4-20. PMID 19941278.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Methods for clinical diagnosis include: Patient reports of symptoms Questionnaires Checklists and scales Voiding diaries Cotton swab test (“Q-Tip® ” test for urethral
hypermobility) Cough test, Valsalva maneuver Pad test (urine collection) Post-void residual volume (ultrasound or
catheter)
Approaches to Diagnosis of UI (2 of 3)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Instrumental methods: Multichannel urodynamics may help distinguish
between pure stress UI, urgency UI, and mixed UI. Urodynamic evaluation is not typically used in
primary care but is used for differential diagnosis, especially for patients considering surgical treatment.
Urodynamics are used as a reference standard for determining the diagnostic value of other methods.
Approaches to Diagnosis of UI (3 of 3)
Abrams P, Anderson KE, Birder L, et al. Neurourol Urodyn 2012;29(1):213-40. PMID: 20025020.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The treatment approach depends on the type of UI; each has different underlying pathophysiologies. Stress UI treatments include a variety of
nonpharmacological methods intended to strengthen muscles that support the bladder and urethra. Pelvic floor muscle training: PFMT, also known as
Kegel exercises Electrical stimulation of pelvic floor muscles Magnetic stimulation of pelvic floor muscles
Non-surgical Treatment of UI (1 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Urgency UI treatments include: Lifestyle changes, fluid management Bladder training Tibial nerve stimulation Drugs that reduce detrusor muscle activity: Anticholinergic drugs that are selective
antagonists of muscarinic receptors
Mixed UI may benefit from approaches meant for both stress and urgency UI.
Non-surgical Treatment of UI (2 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Monitoring UI Treatment Success
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Typical treatment outcomes in clinical studies are: Number of episodes per day Amount of urine in pad tests Urodynamic evaluation
In clinical studies, results showing a difference in number of episodes per day or changes in urodynamics may be statistically significant but not clinically meaningful. For example, a statistically significant reduction of two episodes
per day for a patient with severe UI may not provide a perception of improvement in severity or quality of life.
Meaningful differences in questionnaires or scales have not been systematically reviewed.
The minimal clinically important differences for diagnostic and treatment monitoring tools have not been systematically reviewed.

Topics are nominated through a public process, which includes submissions from health care professionals, professional organizations, the private sector, policymakers, members of the public, and others.
A systematic review of all relevant clinical studies is conducted by independent researchers, funded by AHRQ, to synthesize the evidence in a report summarizing what is known and not known about the select clinical issue. The research questions and the results of the report are subject to expert input, peer review, and public comment.
The results of these reviews are summarized into Clinician Research Summaries and Consumer Research Summaries for use in decisionmaking and in discussions with patients. The Summaries and the full report, with references for included and excluded studies, are available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Agency for Healthcare Research and Quality (AHRQ) Comparative Effectiveness Review (CER) Development
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Clinical questions addressed by the CER included: What constitutes an adequate diagnostic evaluation for
women in the ambulatory care setting on which to base treatment of UI?
What are the minimal clinically important differences in measures of severity and quality of life?
How effective is pharmacological treatment of UI in women? How effective is the nonpharmacological treatment of UI? What are the adverse effects of pharmacological and
nonpharmacological treatments for UI? What patient characteristics can modify the benefits and
adverse effects of treatments for UI?
Clinical Questions Addressed by the CER
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Continence rates Improvement in frequency or severity Quality of life Adverse effects
Clinically Significant Outcomes of InterestExamined in the CER
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Population: Adult and elderly women with symptoms of UI (for the purpose of evaluating diagnostic methods) or diagnosed with UI
Interventions: Nonpharmacological and pharmacological
Comparators: Other active interventions, placebo, or no active intervention
Outcomes: Continence, frequency, severity, improvement, quality of
life Adverse effects
Timing: typically 8 to 12 weeks for trials Setting: Primary care and specialized clinics
Summary of Study Characteristics Evaluated in the CER: The PICOTS Framework
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

95% Confidence Interval: The range of statistically valid results that will include the true population mean in 95 of 100 repeated experiments.
Mean Difference (MD): The difference between treatment and comparison group means. Standardized mean difference (SMD) is the mean difference expressed in units of
standard deviations. It is a method for normalizing results to a uniform scale for pooled analysis when different scales are used in trials.
For MD and SMD, the result is statistically significant (p < 0.05) when the 95% confidence interval does not include 0.0, which is the point of no difference between groups.
Odds Ratio (OR): The ratio of the odds of an event in the treatment group to the odds of the event in the comparison group. Odds are the number of individuals in the group having an event divided by the
number of individuals not having the event (Odds = # with/# without; with + without = total # in the group).
For OR, the result is statistically significant at p < 0.05 when the 95% confidence interval does not include 1.0, which is the point of equal odds for both groups.
Modes of Results Reporting and Statistical Analysis in the CER (1 of 2)
Higgins JPT, Green S, eds. Cochrane handbook for systematic reviews of interventions. Version 5.1.0. Available at www.cochrane-handbook.org.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Relative Risk (RR): The ratio of the rate (absolute risk, probability) of an event in the treatment group to the rate of the event in the comparison group. For RR, the result is statistically significant at p < 0.05 when the
95% confidence interval does not include 1.0, which is the point of equal risk for both groups.
Absolute Risk Difference (ARD): The absolute value of the mathematical difference between the rates (risk) of an event in the treatment (ART) and comparison (ARC) groups. ARD = | ARC–ART |
Number of Attributable Events per 1,000: The number of reported events that can be attributed to the intervention of interest per 1,000 treated patients. The attributable events value is calculated from the ARD. Number of attributable events per 1,000 = 1,000 x |ARC–ART|
Modes of Results Reporting and Statistical Analysis in the CER (2 of 2)
Higgins JPT, Green S, eds. Cochrane handbook for systematic reviews of interventions. Version 5.1.0. Available at www.cochrane-handbook.org.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
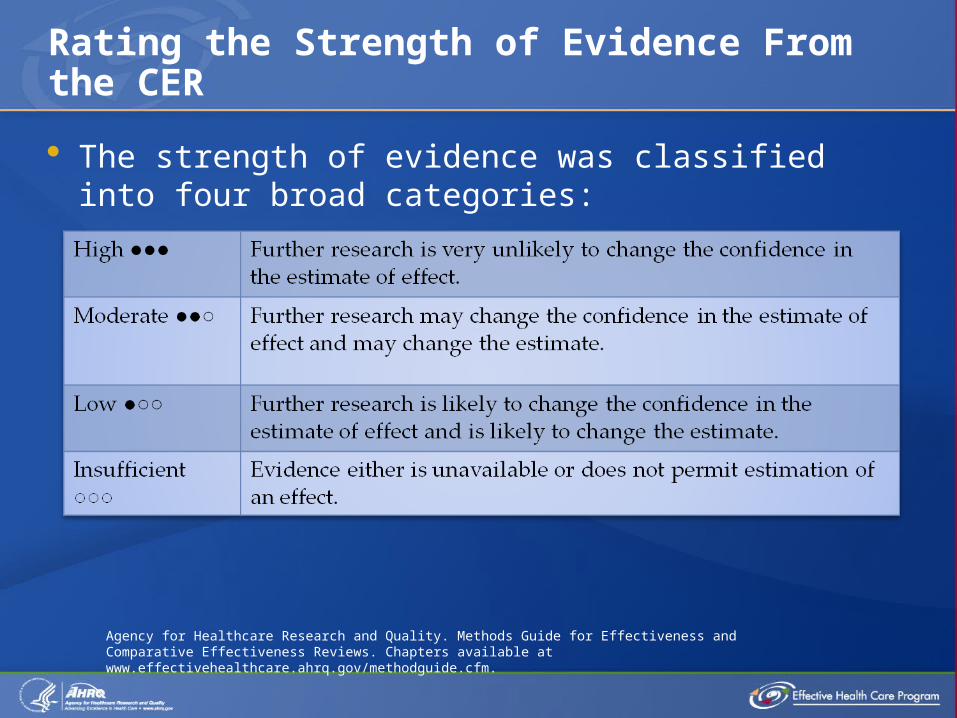
The strength of evidence was classified into four broad categories:
Rating the Strength of Evidence From the CER
Agency for Healthcare Research and Quality. Methods Guide for Effectiveness and Comparative Effectiveness Reviews. Chapters available at www.effectivehealthcare.ahrq.gov/methodguide.cfm.

Urodynamic evaluation is an objective instrumental method for diagnosing UI and is used as a reference standard for evaluating diagnostic methods.
The relative value of urodynamic evaluation when compared with other procedures for diagnosis, such as those used in primary care, is not clear.
The ability of urodynamic evaluation to improve outcomes of non-surgical treatments is not clear.
The CER evaluated the relative diagnostic values of instrumental and clinical diagnostic methods.
In all analyses, the true positive and true negative rates were determined by using the “gold standard.”
Evaluation of Diagnostic Methods (1 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Comparative analyses included: Sensitivity: The probability of a true positive result when used on an
affected population. Specificity: The probability of a true negative result when used on a
nonaffected population.
Positive Predictive Value (PPV): The ratio of the number of true positives to the total number of positive test outcomes.
Positive Likelihood Ratio: The ratio of the probability of a true positive (the sensitivity) to the probability of a false positive (1-specificity). The larger the positive likelihood ratio, the more useful the test.
1 No difference 1–2 Minimal 2–5 Small 5–10 Moderate >10 Large, conclusive
Evaluation of Diagnostic Methods (2 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Ninety-nine studies provided diagnostic values of different methods of UI diagnosis.
81,043 women were included in these studies. The methodology of urodynamic testing was very
similar across studies. Diagnostic methods included history, physical
examination, pelvic examination, urine culture, cotton swab test, diaries, cytometry, cough stress test, 48-hour home pad test, evaluation of sacral nerves 2 to 4, and postvoid residual volume.
Results of the Systematic Review:Evaluation of Diagnostic Methods (1 of 4)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The comparative value of symptoms of stress, urgency, or mixed UI for correctly diagnosing the type of UI was evaluated by comparing them with the full clinical diagnosis or the results of multichannel urodynamics.
Results of the Systematic Review:Evaluation of Diagnostic Methods (2 of 4)
Diagnosis
Diagnostic Method
Reference Standard
Sensitivity(95% CI)
Specificity(95% CI)
Positive Likelihood Ratio
Positive Predictive Value (95% CI)
Stress UI Stress UI Symptoms
Clinical Diagnosis
0.88 (0.68, 0.96)
0.67 (0.54, 0.78)
2.35Small
0.80 (0.66, 0.89)
Detrusor overactivity
Urgency UISymptoms
Clinical Diagnosis
0.82 (0.73, 0.89)
0.67 (0.53, 0.89)
2.52Small
0.79 (0.54, 0.92)
Mixed UI Stress and Urgency UI symptoms
Clinical Diagnosis
0.65 (0.36. 0.86)
0.54 (0.21, 0. 84)
1.6Small
0.80 (0.43, 0.96)
Stress UI Stress UI Symptoms
Multichannel urodynamics
0.93 (0.90, .95)
0.41 (0.34, 0.49)
1.5 4Minimal
0.74 (0.67, 0.81)
Detrusor overactivity
Urgency UISymptoms
Multichannel urodynamics
0.82 (0.76, 0.87)
0.51 (0.44, 0.59)
1.5 4Minimal
0.80 (0.73, 0.86)
Mixed UI Stress and Urgency UI symptoms
Multichannel Urodynamics
0.73 (0.61, 0.82)
0.53 (0.40, 0.66)
1.45 Minimal
0.89 (0.85, 0.92)
95% CI = 95 percent confidence interval: the range of statistically valid results for the true treatment effect Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Results of the Systematic Review:Evaluation of Diagnostic Methods (3 of 4)
Yalcin I, Versi E, Benson JT, et al. J Urol 2004;71(6 Pt 1): 2321-5. PMID: 15126813.Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
DiagnosisDiagnostic Method
Reference Standard
Sensitivity(95% CI)
Specificity(95% CI)
Positive Likelihood Ratio
Positive Predictive Value
Stress UI EPIQ –basedalgorithm
Clinical Diagnosis
0.65 (0.36, 0.86)
0.54 (0.21, 0.84)
10Large
0.88
Detrusor Overactivity
EPIQ –basedalgorithm
Clinical Diagnosis
0.82 (0.73, 0.89)
0.67 (0.53, 0.89)
7.70Large
0.77
Detrusor Overactivity
OAB-V8 –based algorithm
Clinical Diagnosis
0.65 (0.36. 0.86)
0.54 (0.21, 0. 84)
5.66Moderate
0.44
Detrusor Overactivity
BIDI Urodynamics
0.88(not available)
0.83
(not
available)
5.12Moderate
0.41
Stress UI Clinical algorithm(Yalcin et al, 2004)
Urodynamics
NR NR NR 0.90(0.85, 0.94)
Stress UI Clinical algorithm (Yalcin et al., 2004)
Clinical Diagnosis
NR NR NR 0.85(0.79, 0.90)
95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 experiments); BIDI = Bladder Instability Discriminant Index; EPIQ = Epidemiology of Incontinence Questionnaire; NR = not reported; OAB-V8 = Overactive Bladder Awareness Tool; UI = urinary incontinence
The comparative value of clinical algorithms for correctly diagnosing the type of UI was evaluated by comparing them with the full clinical diagnosis or multichannel urodynamics. Some examples of this analysis are presented here.
These questionnaires, used alone, had minimal diagnostic value for stress, urgency, or mixed UI when compared with urodynamics (positive likelihood ratio <2): UDI-6: Urogenital Distress Inventory QUID: Questionnaire for Urinary Incontinence
Diagnosis Bristol Female Lower Urinary Tract Symptoms
Questionnaire Gaudenz
Results of the Systematic Review:Evaluation of Diagnostic Methods (4 of 4)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Assuming that clinical diagnosis includes an adequate assessment of conditions that may cause UI: No statistically significant differences in continence,
improvement, or treatment failure were found between groups of women who did or did not have a baseline urodynamics diagnosis.
One large analysis of 6,276 women from the United Kingdom indicated that urodynamic evaluation is essential to predict outcomes of surgical treatment for UI.
Is Urodynamic Evaluation Essential for Predicting Who Will Benefit From Treatment?
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Patient reports of individual symptoms of stress or urgency have minimal or small diagnostic value when compared with both urodynamics and clinical diagnosis. Strength of Evidence = High
Clinical algorithms for differentiating stress, urgency, and mixed UI have high diagnostic value when compared with urodynamics. Strength of Evidence = Moderate
Diagnosis by urodynamic examination is not associated with better outcomes after non-surgical treatments. Strength of Evidence = Moderate
Summary: Comparative Value of UIDiagnostic Methods
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The CER included an analysis of treatment-monitoring tools. Validity = the ability to measure what the test intends to
measure Reliability = reproducibility
Results of the Systematic Review: Evaluation of UI Treatment-Monitoring Methods (1 of 2)
Outcome
TotalInstruments Evaluated
Number Both Valid and Reliable
Number Valid But Not Reliable
Number Not Valid or Reliable
Symptom Bother
9 6 3 NA
Screening 8 6 1 1 (3 IQ)
Quality of Life 20 17 2 1 (IBS simple visual analog scale)
Patient Satisfaction
6 2 4 NA
3 IQ = 3 Incontinence Questions; IBS = Incontinence Bothersome Scale; NA = not applicable
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Multiple validated instruments can be used to monitor UI treatment success by detecting meaningful changes in symptoms and quality of life (QoL), as identified by women with UI.
††The authors examined the clinical literature to produce definitions of minimal clinically important differences. Clinical success is perceived by women when episode
frequency is reduced by 50% or more. ††QoL improvements are perceived by women at a
70% reduction in frequency (as measured by the Incontinence Quality of Life Questionnaire and the Global Perception of Improvement and Incontinence Impact Questionnaire).
Summary of Evaluation and Treatment Monitoring

Continence and Improvement From Nonpharmacological Interventions for Stress UI
Intervention
Continence Improvement
N Studies(Participants)
RR(95% CI)
Events per 1,000*(95% CI)
N Studies(Participants)
RR(95% CI)
Events per 1,000*
(95% CI)
PFMT10 (959)
3.77 (2.09, 6.80)
299 (188, 410)
6 (510) 5.44(1.57, 18.83)
412 (174, 649)
PFMT plus biofeedback
2 (185) NSD NSD 4 (383) 3.93 (1.00, 15.49)
390 (170, 610)
Electrical stimulation 7 (420)
2.86(1.57, 5.23)
162 (64, 259)
8 (582) 2.01(1.28, 3.15)
156 (84, 228)
Magnetic stimulation
3 (171) NSD NSD 3 (153) 2.30(1.43, 3.71)
265 (112, 417)
* Events per 1,000 is calculated from the difference between treatment and control group event rates.95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 repeated experiments); Strength of Evidence:: = high; = moderate; = low; = insufficient
Nonpharmacological interventions promote continence and improve severity for patients with stress UI. Results from trials comparing interventions with placebo or no active intervention are given below.
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Nonpharmacological interventions improve severity and for patients with urgency UI, and both promote continence and improve severity for patients with mixed UI. Results from trials comparing interventions with placebo or no active intervention are given below.
Continence and Improvement From Nonpharmacological Interventions for Urgency UI or Mixed UI
Intervention
Continence Improvement
N Studies(Participants)
RR(95% CI)
Events per 1,000*(95% CI)
N Studies(Participants)
RR(95% CI)
Events per 1,000*(95% CI)
Urgency UI
Bladder Training 1 (131) 2 (283) 3.22(2.25, 4.60)
430 (275, 585)
Percutaneous Tibial Nerve Stimulation
Not Reported
Not Reported
Not Reported 3 (405) 1.9 (1.1, 3.2)
308 (40, 577)
Mixed UI
PFMT plus Bladder Training
5 (1369) 3.79 (1.55, 9.27)
166 (63, 268)
4 (1171) 4.13 (1.58, 10.78)
387(171, 603)
Maintained weight loss and exercise
1 (338) 2 (386) 2.17(1.26, 3.76)
273(57,490)
* Events per 1,000 is calculated from the difference between treatment and control group event rates.95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 repeated experiments); PFMT = pelvic floor muscle training; RR = relative risk; Strength of Evidence: = high; = moderate; = low; = insufficient
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
No statistically significant differences were found in meta-analyses of these head-to-head comparisons:
For Stress and Mixed UI: PFMT alone versus PFMT combined with either biofeedback,
bladder training, or supervision Strength of Evidence = High
PFMT alone versus PFMT combined with either intravaginal electrical stimulation or intravaginal devices Strength of Evidence = Moderate
Intravaginal and intraurethral devices and bulking agents when compared with PFMT Strength of Evidence = Low
For Urgency UI Bladder training alone versus bladder training plus PFMT
Strength of Evidence = High
Comparative Effectiveness ofNonpharmacological Interventions
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Pharmacological interventions are used for urgency UI and mixed UI.
The use of drug treatment for stress UI is rare and is considered “off-label.” In treatment of stress UI with duloxetine , the rate of
discontinuation due to adverse effects (129 per 1,000 treated patients) is greater than the rate of benefits (75 per 1,000 treated patients).
For the analysis presented here, benefits are measured as rates of continence or improvement.
The rate of discontinuation from treatment due to adverse effects and the rates of individual adverse effects are reported.
Pharmacological Interventions for UI:Benefits and Adverse Effects
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Continence and Improvement From Pharmacological Interventions for Urgency UI: Placebo Comparisons
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.
Intervention
Continence Improvement
N Studies(Participants)
Odds Ratio(95% CI)
Events per 1,000*(95% CI)
N Studies,(Participants)
Odds Ratio(95% CI)
Events per 1,000*(95% CI)
DarifenacinNot Reported
3, 1011 1.7(1.04, 2.9)
117 (57, 177)
Fesoterodine 2 (2,465) 1.7(0.9, 3.3)
130 (58, 202)
4, 3801 1.3(1.2, 1.5)
10 0 (56, 145)
Oxybutynin 4 (992) 2.1(1.2, 3.9)
114 (64, 163)
9 (1,244) 2.5(1.7, 3.7)
167 (95, 240)
Solifenacin 5 (6,304) 1.7(1.3, 2.1)
107 (58, 156)
2, 1507 2.2(1.1, 4.3)
180 (97, 263)
Tolterodine 4 (3,404) 1.5(1.0, 2.1)
85 (40, 129)
7 (6,119) 1.5(1.2, 2.0)
96 (42, 149)
Trospium 4 (2,677) 2.0(1.4, 2.9)
114 (83, 144)
2 (1,176) NSD NSD
* Events per 1,000 is calculated from the difference between treatment and control group event rates.95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 repeated experiments); Strength of Evidence:: = high; = moderate; = low; = insufficient
For all pharmacological interventions, the continence and improvement rates for groups treated with drugs differ by less than 20 percent from rates in placebo groups, with fewer than 200 attributable events per 1,000 treated patients. Events attributable to treatment range from 85 to
180 per 1,000 treated patients.
Outcomes of Pharmacological Interventionsfor Urgency UI: Summary
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Tolerability of pharmacological interventions is represented as the rate of discontinuation from treatment due to adverse effects, compared with placebo groups.
Adverse Effects of Pharmacological Interventions for Urgency UI: Placebo Comparisons (1 of 2)
Intervention
Discontinuation of Treatment Due to Adverse Effects
N Studies(Participants)
Odds Ratio(95% CI)
Events per 1,000(95% CI)
Darifenacin 7 (3,138) NSD NSD
Fesoterodine 6 (6,338) 2.1 (1.5, 2.9) 31 (10, 56 )
Oxybutynin 6 (1,662) 1.7 (1.2, 2.5) 63 (12, 127)
Solifenacin 8 (9,819) 1.4 (1.1, 1.7) 13 (1, 26)
Tolterodine 13 (7,801) NSD NSD
Trospium 6 (3,936) 1.5 (1.1, 1.9) 18 (4, 33)
* Events per 1,000 is calculated from the difference between treatment and control group event rates.95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 repeated experiments); NSD = no statistically significant difference; Strength of Evidence: = high; = moderate; = low; = insufficient
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Adverse Effects of Pharmacological Interventions for Urgency UI: Placebo Comparisons (2 of 2)
Intervention
Other Adverse Events
Dry Mouth Constipation Other
N Studies(Participants)
Reports per 1,000 Treated*(95% CI)
N Studies(Participants)
Reports per 1,000 Treated*(95% CI)
Adverse Event;N Studies(Participants)
Reports per 1,000 Treated*(95% CI)
Darifenacin
5 (2,382)158 (65, 269)
5 (2,239)80 (24, 148)
Dyspepsia 4 (1,772)
31 (7, 62)
Fesoterodine
5 (6,674) 199 (161, 239)
7 (7, 695)
41 (1, 97)
Dry Eye4 (4,145)
28 (6, 60)
Oxybutynin
9 (2,238) 347 (158, 536)
7 (1,743) NSD Dyspepsia3 (613)
85 (27, 158)
Solifenacin
7 (11,089) 175 (122, 232)
8 (11,765) 73 (49, 99)
Blurred Vision9 (12,922)
17 (10, 26)
Tolterodine
14 (7,637) 139 (104,175)
14 (9,592) 12 (3, 22)
Dyspepsia6 (3,525)
22 (1, 53)
Trospium 6 (3,490) 106 (75, 140)
5 (3,335) 70 (47, 95)
Dry Eye2 (1,590)
14 (4, 29)
* Events per 1,000 treated is calculated from the difference between treatment and control group events rates.95% CI = 95 percent confidence interval (i.e., the range of statistically valid results that contains the true population mean in 95 of 100 repeated experiments); NSD = no statistically significant difference; Strength of Evidence:: = high; = moderate; = low; = insufficient
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Tolerability of pharmacological interventions, represented by the rate of discontinuation of treatment during clinical trials due to adverse effects, includes: No statistically significant difference from placebo
(darifenacin, tolterodine) Less than 10% difference in rate from placebo
(discontinuations per 1,000: solifenacin, 10; trospium, 20; fesoterodine, 30; oxybutynin, 63).
Strength of Evidence = High Dry mouth is the most common adverse effect (106 to 347
per 1,000 treated patients), followed by constipation (12 to 80 per 1,000 treated patients).
Dry eye, blurred vision, and dyspepsia are less frequent. Fewer than 50 events per 1,000 treated patients, with the
exception of dyspepsia with oxybutynin at 80 per 1,000 treated patients
Summary of Adverse Effects ofPharmacological Interventions
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Other findings: The rate of adverse effects increases with increased doses of darifenacin, fesoterodine, oxybutynin, and solifenacin. (Dosage effects of tolterodine and trospium are not reported.) Strength of Evidence = High
„Transdermal and controlled-release forms of oxybutynin have lower rates of adverse effects, but a dose response for adverse effects is still found with these formulations. Strength of Evidence = Low
50% of women stop treatment with drugs within 1 year. Strength of Evidence = High
Other Report Findings of Adverse Effects
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Evidence about long-term safety of drug treatments for UI is insufficient to permit conclusions about the magnitude of risk.
Postmarketing surveillance has revealed increased risks of ventricular arrhythmias or sudden death when used in older people who are also using antihistamines or cytochrome inhibitors. Tolterodine is associated with an increased risk of hallucinations.
Additional Information About Adverse Effects
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

When compared with tolterodine, fesoterodine achieves higher rates of continence (a difference of 55 reports per 1,000 treated patients) and improvement (a difference of 28 events per 1,000 treated patients).
Strength of Evidence = Continence, Low
Improvement, High
No statistically significant difference in improvement rates is found in comparisons of oxybutynin and tolterodine.
Strength of Evidence = Moderate
Comparative Effectiveness of Pharmacological Interventions (1 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Discontinuation rates due to adverse effects are higher with fesoterodine (18 events per 1,000 treated patients) and oxybutynin (55 events per 1,000 treated patients) than with tolterodine. Strength of Evidence = Moderate (fesoterodine)
High (oxybutynin)
No statistically significant difference in discontinuation rate was found in comparisons of solifenacin and tolterodine. Strength of Evidence = Moderate
For most head-to-head comparisons, only a single study was available for review, and the evidence is insufficient to permit conclusions about differences in the rates of benefits or adverse events.
Comparative Effectiveness of Pharmacological Interventions (2 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Age does not modify continence or improvement outcomes of oxybutynin, trospium, or darifenacin.
Strength of Evidence = Moderate
Obesity does not modify the effect of trospium.
Strength of Evidence = High
Trospium effectiveness is not affected by concomitant medications. Adverse effects are more common in patients taking trospium and seven or more concomitant medications.
Strength of Evidence = Moderate
Modifiers of Outcomes and Safety of Pharmacological Treatment (1 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Solifenacin is effective regardless of response to previous treatment.
Strength of Evidence = High
Tolterodine and solifenacin outcomes are not affected by mixed or pure urgency types of UI.
Strength of Evidence = Moderate
Baseline frequency of UI does not influence clinical outcomes of any drug.
Strength of Evidence = Low
Modifiers of Outcomes and Safety of Pharmacological Treatment (2 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

Nonpharmacological interventions (notably, PFMT or bladder training) lessen the severity of urgency, stress, and mixed UI, and promote continence in patients with stress and mixed UI, with low risk of adverse effects.
For nonpharmacological interventions, reasons for discontinuation and methods to improve adherence are not understood or systematically investigated.
Drug treatments for urgency UI show similar small benefits but may be differentiated by their adverse effects profiles.
Withdrawal from drug treatment is typically due to adverse effects. Dry mouth and constipation are common.
Conclusions About Benefits and Adverse Effects (1 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The long-term safety of drugs for UI has not been evaluated in clinical trials, but serious adverse effects have been associated with their use (e.g., among the elderly and in combination with other commonly prescribed drugs).
Diagnosis using clinical tools available in primary care is comparable to urodynamic evaluation.
Diagnosis by urodynamic evaluation is not associated with better outcomes after non-surgical treatments.
Currently available validated tools (voiding diaries, scales measuring perception of improvement and quality of life) are effective for measuring success with treatment targets that are valued by women with UI.
Conclusions About Benefits and Adverse Effects (2 of 2)
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The systematic review revealed areas where the evidence about treatments for UI is limited or absent, including: Evidence is insufficient to permit conclusions about the
effectiveness of nonpharmacological interventions when compared with drugs or combined modalities.
The reasons for high discontinuation rates with nonpharmacological interventions and methods to improve adherence are not understood nor well investigated.
Evidence is inadequate to determine whether increasing drug dosage leads to greater improvement or likelihood of achieving continence.
Evidence about how patient characteristics influence the treatment benefits or adverse effects of treatment is incomplete and of limited value to guide decisionmaking (e.g., baseline frequency, age, race, type of UI, prior treatment, comorbidities, and obesity).
Gaps in Knowledge
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.

The roles of nonpharmacological, pharmacological, and surgical interventions for treating UI.
The trade-offs between the likelihood of benefits and the types and severity of adverse effects associated with UI drug treatments.
The importance of adherence to exercise protocols to achieve continence or improve severity of UI.
The benefits and low risk of adverse effects from nonpharmacological UI treatments, such as special exercises.
What To Discuss With Your Patients andTheir Caregivers
Shamliyan T, Wyman J, Sainfort F, et al. Comparative Effectiveness Review No. 36. Available at www.effectivehealthcare.ahrq.gov/ui.cfm.