non-small cell lung cancer state of the art -...
TRANSCRIPT

Non-Small Cell Lung Cancer
State of the Art
Rolf Stahel
University Hospital of Zürich
1 |
Cape Town, 11.2.2017
2 |

Individual patient data meta-analysis: sequential vs
concurrent chemo-radiotherapy
3 |
Aupérin, JCO 2010

Chemoradiotherapy: No evidence for advantage with
induction or consolidation chemotherapy in stage III
4 |
Carboplatin-paclitaxel induction
followed by chemoradiotherapyConcurrent PE chemoradiotherapy
followed by docetaxel consolidation
Vokes, JCO 2007 Hanna, JCO 2008

5 |
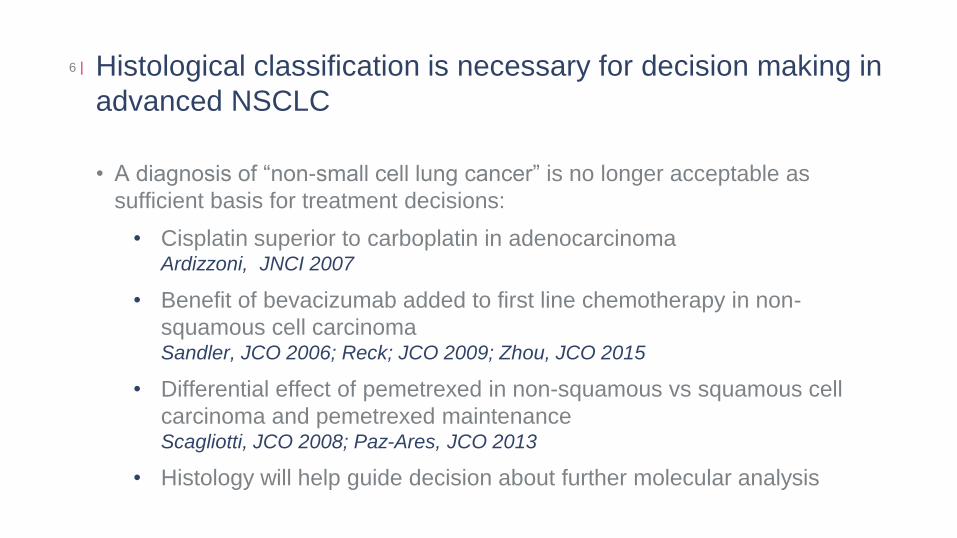
Histological classification is necessary for decision making in
advanced NSCLC
• A diagnosis of “non-small cell lung cancer” is no longer acceptable as
sufficient basis for treatment decisions:
• Cisplatin superior to carboplatin in adenocarcinomaArdizzoni, JNCI 2007
• Benefit of bevacizumab added to first line chemotherapy in non-
squamous cell carcinomaSandler, JCO 2006; Reck; JCO 2009; Zhou, JCO 2015
• Differential effect of pemetrexed in non-squamous vs squamous cell
carcinoma and pemetrexed maintenanceScagliotti, JCO 2008; Paz-Ares, JCO 2013
• Histology will help guide decision about further molecular analysis
6 |
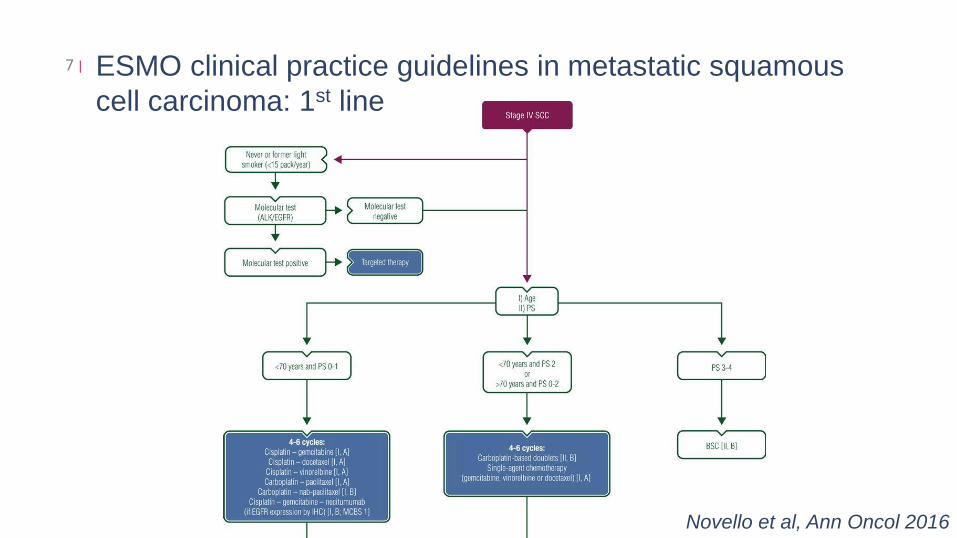
ESMO clinical practice guidelines in metastatic squamous
cell carcinoma: 1st line
7 |
Novello et al, Ann Oncol 2016

Gemcitabine and cisplatin with or without necitumumab in
squamous cell lung cancer
8 |
Thatcher, Lancet Oncol 2015

Magnitunde of Clinical Benefit Scale: Form 2a
(primary endpoint OS, OS < 1 year, non-curative)
9 |
Cherny et al, Ann Oncol 2015
54321
A
B
C
Curative Non-curative

Magnitunde of Clinical Benefit Scale: Second line squamous
cell carcinoma
10 |

ESMO clinical practice guidelines in metastatic squamous
cell carcinoma: 2nd line
11 |
Novello et al, Ann Oncol 2016

ESMO clinical practice guidelines in metastatic non-squamous
cell carcinoma: 1st line
12 |
Novello et al, Ann Oncol 2016

ESMO clinical practice guidelines in metastatic non-squamous
cell carcinoma: 1st line
13 |
Novello et al, Ann Oncol 2016

Bevacizumab in adenocarcinoma14 |
Sandler, JTO 2008
OS for E4599 all patients and
adenocarcinoma only
BEYOND: Randomized phase III
study from China
Zhou JCO 2015

PARAMOUNT: Overall survival15 |
Paz-Ares, JCO 2013
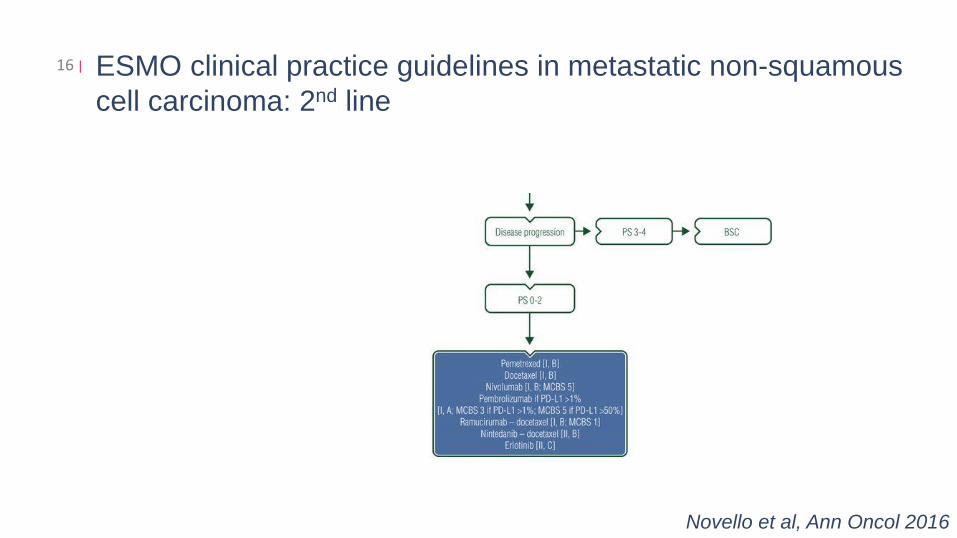
ESMO clinical practice guidelines in metastatic non-squamous
cell carcinoma: 2nd line
16 |
Novello et al, Ann Oncol 2016

2nd line NSCLC phase III: Docetaxel vs BSC17 |
MST 7.5 vs 4.7 months
D100 D75
Shepherd, JCO 2000
OS 7.5 vs 6.4 months

Docetaxel plus nintedanib (LUME-Lung 1) or docetaxel plus
ramucirumab (REVEL) versus docetaxel plus placebo for
2nd line treatment of stage IV NSCLC
18 |
LUME-Lung 1: Adenocarcinoma
OS 12.6 vs 10.3 months OS 10.5 vs 9.1 months
Reck, Lancet Oncol 2014
REVEL: all histologies
Garon, Lancet Oncol 2014

Magnitunde of Clinical Benefit Scale: Second line non-
squamous cell carcinoma
19 |

The complexity of PD-L1 diagnostics of NSCLC20 |
Nivolumab:
BMS
Pembrolizumab:
Merck
Atezolizumab:
Roche
Durvalumab:
AstraZeneca
Avelumab: Pfizer
Ab Clone 28-8 SP263 22C3 SP142 SP263 73-10
Diagnostic
PartnerDako Ventana Dako Ventana Ventana Dako
Scoring Method† % of PD-L1–expressing
tumour cells
% of PD-L1–
expressing
tumour cells
% of PD-L1–
expressing
tumour cells or
immune cells
% of PD-L1–
expressing
tumour cells
% of PD-L1–expressing tumour
cells
Diagnostic Status
Complementary: testing not required
Companion: testing required
US/EU: SQ and NSQ NSCLC
Dx not approved for NSCLC setting
Dx not approved for durvalumab in
any setting
Dx not approved for avellumab in
any settingUS/EU: NSQ NSCLC
EU: NSQ NSCLC
Approved IVD PD-L1 Threshold
US/EU:All patients
eligible
EU: All patients
eligible
US: ≥50%EU: ≥1%
NA NA NA
PD-L1 Thresholds≥1% (pos), ≥5% (strong), or
≥10%Validated
≥1% (pos)≥50% (strong)
Validated
TC / IC 3(+)TC / IC 2(+) TC / IC 1(+)TC / IC 0(−)
TCPD-L1(+): ≥ 25%
TBC, TC between all >1% and 25%
with moderate or high intensity

Analytical evaluation results: Mean TPS per case based on 3
readers: Tumor cells
21 |
22C3
28-8
SP142
SP263
100
90
80
70
60
50
40
30
20
10
0391 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37
CasesHirsch, AACR 2016
• Analytical comparison of TPS
by case for each assay
• Data points represent the
mean score from 3 pathologists
for each assay on each case
• No clinical diagnostic cutoff
applied
• Conclusion: 3 of 4 assays
are analytically similar
for tumor cell
staining
Hirsch, AACR 2016

Example of PD-L1 tumor expression22 |
22C3 28-8 SP263 SP142
Not only technical validation, also clinical validation required
Not all animals are created equalHirsch, AACR 2016

Checkmate 017 and 057: 2-years update of OAS
(no biomarker selection),
23 |
Borghael, ASCO 2016
* No biomarker selection
* *

Checkmate 057: OS by PD-L1 Expression24 |
mOS (mos)
Nivo 17.7
Doc 9.0
mOS (mos)
Nivo 19.4
Doc 8.1
mOS (mos)
Nivo 19.9
Doc 8.0
mOS (mos)
Nivo 10.5
Doc 10.1
mOS (mos)
Nivo 9.8
Doc 10.1
mOS (mos)
Nivo 9.9
Doc 10.3
≥1% PD-L1 expression level
Time (Months)
100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
OS
(%
)
NivoDoc
HR (95% CI) = 0.58 (0.43, 0.79)
≥5% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (Months)
HR (95% CI) = 0.43 (0.30, 0.62)
≥10% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (Months)
HR (95% CI) = 0.40 (0.27, 0.58)
<1% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (Months)
OS
(%
)
NivoDoc
<10% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (Months)
<5% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (Months)
HR (95% CI) = 0.87 (0.63, 1.19) HR (95% CI) = 0.96 (0.73, 1.27) HR (95% CI) = 0.96 (0.74, 1.25)
Based on a July 2, 2015 DBL. Symbols represent censored observations EMA Opdivo Product Characteristics

KEYNOTE 10: Pembrolizumab versus doxetaxel in 2nd line
NSCLC (1% of tumor cells PD-L1 positive)
25 |
Herbst, ESMO Asia 2015, Lancet
2016

Relationship between level of PD-L1 expression and
outcomes in the KEYNOTE-010 trial
26 |
Baas, ASCO 2016

Less toxicity with immune checkpoint inhibitors in second line
comparative studies
28 |
Toxicity
Gade
% of patients
Check-mate 17 Checkmate 57 KEYNOTE 10
N Doc N Doc P2 P10 Doc
All 59 87 69 88 63 66 35
3-5 8 60 10 54 13 16 79

Case study, R.M. 1952
• 06/15 Diagnosis: Pleomorphic carcinoma RUL,
clinical state stage T3N1M1 (bone)
• 07/15 – 08/15 3 cycles of cisplatin and gemcitabine
• 28.08.2015 Re-Staging: progression in bone
29 |
08/201506/2015

Case study, R.M. 1952
• 29.09.2015 Right upper lobe resection ypT3 ypN1 (1/8)
• 06.11.2015 Re-Staging: progression bone, LN
30 |
Nov 2015 RT Sacrum, paravertebral, Os
14.12.2015 Nivolumab, on the 14.12. and 28.12.2015

Case study, R.M. 195231 |
Emergency hospitalisation 05.01.2016
• PiO2 67%; no fever, ECOG 3-4
• CRP 115, LDH 680; Leucocytes 11 G/l
• Methylprednisolon 250mg iv (1d)
• Prednison 200mg (2d), 100mg (2d), 50mg (3d), 25mg (3d), 20mg (3d),
10mg (2d), 5mg (2d)
• Tazobac +Bactrim

Case study, R.M. 195232 |
2/2016, 6/2016, 11/201611/2015

Treatment effect on overall suvival in Checkmate 57 and
KEYNOTE 10
33 |
Borghaei. NEJM 2015; Herbst Lancet 2015

First line immunotherapy: Duration of therapy after response?A case of a 70-year old man with stage IV adenocarcinoma of the lung treated with
two doses of atezolizumab
34 |
April 2014:
Pretreatment
September 2014:
2 doses of therapy in
June 2014
March 2015:
Hilar progression

KEYNOTE-024: Pembrolizumab vs platinum-based
chemotherapy as first-Line therapy for advanced NSCLC with
a PD-L1 TPS ≥50%
35 |
Reck, ESMO 2016

KEYNOTE-024: Pembrolizumab vs platinum-based
chemotherapy as first-Line therapy for advanced NSCLC with
a PD-L1 TPS ≥50%
36 |
Reck, ESMO 2016

KEYNOTE-024: Treatment related side effects with
incidence >10%
37 |
0
5
10
15
20
25
30
35
40
45
50
Incid
en
ce,
%
1-2
Grade
3-4
Data cut-off: May 9, 2016.
Pembrolizumab
Chemotherapy

KEYNOTE-024: Immune-mediated adverse events38 |
0
1
2
3
4
5
6
7
8
9
10In
cid
en
ce,
%
1-2
Grade
3-4
Overall incidence
• 29.2% any grade
• 9.7% grade 3-4
• No grade 5 events

Targeted therapy in non-squamous NSCLC lung cancer:
First line TKIs: Superior progression-free survival as compared
to chemotherapy
39 |
Crizotinib
NTRK fusion
Gefitinib
Erlotinib
Afatinib

First TKI versus chemotherapy in oncogenic driver NSCLC40 |
Mok, NEJM 2014Rosell, Lancet Oncol 2012
Aktivating EGFR mutation ALK rearragnement

Targeted therapy in non-squamous NSCLC lung cancer:
Second line TKIs: Superior progression-free survival as compared
with chemotherapy
41 |
Crizotinib
NTRK fusion
Gefitinib
Erlotinib
AfatinibT790M: Osimertinib
Ceritinib / AlectinibCrizotinib

Major mechanisms of resistance to EGFR TKIs42 |
Yu, Clin Cancer Res 2013

Osimertinib or platinum-pemetrexed in EGFR T790M–positive
NSCLC
43 |
Mok, NEJM 2016

Crizotinib-resistant ALK-positive NSCLC44 |
Alectinib phase 2 trial
RR 48%
Median PFS 8.1
months
Ceritinib vs chemotherapy
(ASCEND-5)RR 45% vs 8%
Shaw, Lancet Oncol 2016 Scagliotti, ESMO 2016

Targeted therapy in non-squamous NSCLC lung cancer:
TKIs in later line beyond mutated EGFR, ALK or ROS rearrangement
45 |
Vandetanib/LevatinibAlectinib
CrizotinibTrastuzumab
Crizotinib
Afatinib
Crizotinib
Dabrafenib/Trametinib
Vermurafenib
NTRK fusion Entrectinib
Gefitinib
Erlotinib
Afatinib
Osimertinib
Ceritinib/AlectinibCrizotinib
46 |
ETOP | Name Project | Title Presentation | Zurich, July 27, 2009