non-infectious catheter/mechanical...
TRANSCRIPT

+
Non-Infectious
Catheter/Mechanical
ComplicationsZoe Parr, MD, FRCSC, FACS
ADC, February 27, 2016, Seattle, WA
+OBJECTIVES
To review common catheter complications
To review considerations for catheter salvage
To discuss the importance of surgical technique for
prevention
+Background
Work in a multi-disciplinary team
General Surgeons – UWMC and HMC
Nephrologists – UWMC and HMC
Nurses – UWMC, HMC, Northwest Kidney Center
Place PD catheters laparoscopically according to a technique
taught to us by Dr. John Crabtree (Kaiser Permanente, CA)
+Catheter complications
Many techniques to place catheters (laparoscopic, open, peritoneoscopic, percutaneous) and many differently trained providers placing them
Infectious complications
Exit site infections (2-41%)
Peritonitis (2-30%)
Non-infectious complications
Catheter-related
Abdominal-wall hernias

+Non-infectious complications
Catheter-related
Problems with flow – obstruction, migration, kinking
Peri-catheter leak
Abdominal wall hernias
Umbilical > Inguinal > Incisional, Epigastric
Peri-catheter hernias
+
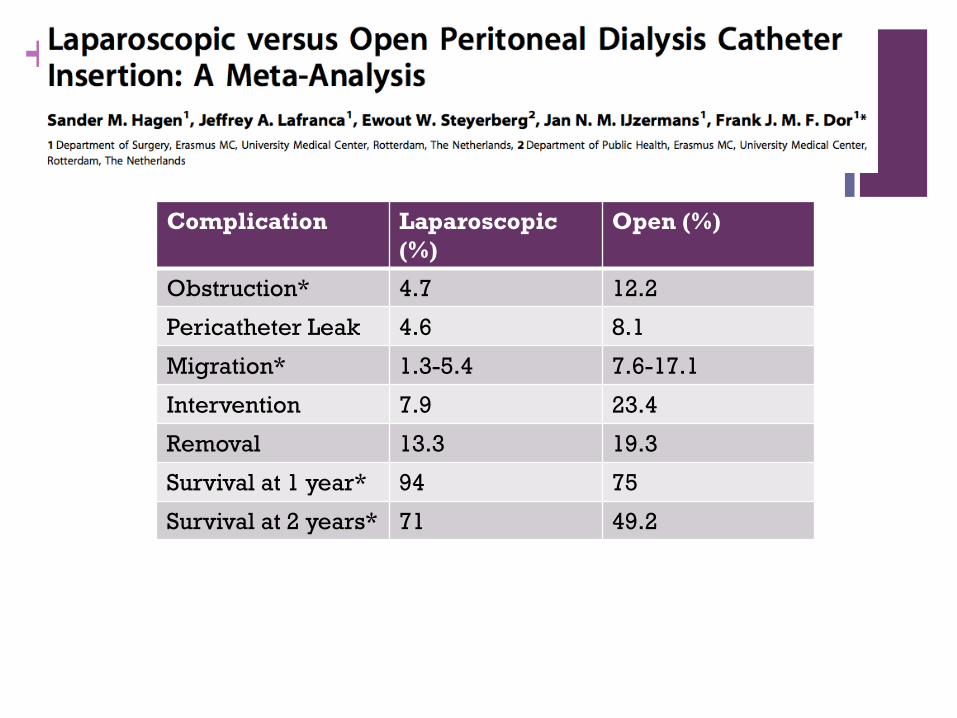
Complication Laparoscopic
(%)
Open (%)
Obstruction* 4.7 12.2
Pericatheter Leak 4.6 8.1
Migration* 1.3-5.4 7.6-17.1
Intervention 7.9 23.4
Removal 13.3 19.3
Survival at 1 year* 94 75
Survival at 2 years* 71 49.2
+Mechanical Flow
Confirm the diagnosis – Hx, PE, radiology
Consider peri-catheter leakage
Outflow >> inflow
Obstruction – extra-luminal (constipation, bladder distension,
organs) or intra-luminal (fibrin plugging, omental intrusion)
Catheter kinking
Catheter malposition – migration
+Work-up of Issues with Flow
Rule out constipation, bladder distension, fibrin plugging
Initial diagnostics – AXR, bladder scan, catheter study
AXR – constipation, tube displacement (suggestive of omental
entrapment or adhesions)
Catheter study – rule out catheter leakage, may suggest
evidence for entrapment or adhesions
Fibrin plugging – urokinase, alteplase

+Images of Malpositioned/Migrated
catheters

+

+
+Catheter salvage
Techniques utilized for de-plugging or for re-direction of
catheters
Endoluminal brushes, fogarty balloons, fluoroscopic guide wire
manipulation
Laparoscopy
Extra-luminal obstruction
Intra-luminal obstruction from omental intrusion
Catheter-tip migration
Kinking (replacement)
+My Approach to Laparoscopy
Review their pre-operative Hx, PE, imaging studies, existing
operative reports
Supine positioning with both arms tucked
Access the abdomen opposite the side the catheter was
inserted on
Achieve pneumoperitoneum via the technique one most
comfortable with/most appropriate for the case
Consider using the existing PD catheter to insufflate

+Findings
Omental wrapping +- tip migration
Perform or re-do omentopexy
Adhesions +- tip migration
Adhesions from bowel, fallopian tubes, epiploicea etc.
Try to leave the adhesions in place and reposition the catheter
Angulation through the abdominal wall or related to tube memory
May be best to replace the catheter
Fibrin plugging
Catheter stripping, use of fogarty balloons or brushes

+
40/197 pts (20.3%) evaluated for catheter malfunction and 46 laparoscopic procedures performed to attempt catheter salvage
16 pts – tip migration alone; 12 pts – tip migration + omental/bowel adhesions; 4 pts – adhesions alone; 8 pts – other
3 pts required catheter removal, 3 required replacement and the remaining were corrected laparoscopically
Catheter malfunction recurred in 12 patients of 37 patients (32.4%) at a mean time of 12.4 months.
97.2% catheter patency at 3 months for the 37 patients, 62% at 12 months.
Mean catheter survival 19.9 months.
+Pericatheter leaks
Pericatheter leakage – outflow < inflow with signs of leakage from the exit site, subQ swelling, peripheral or genital edema
Highly variable reported incidence due to varying techniques, though rates tend to be less with embedded catheters
Tends to occur early after surgery in the setting of high dialysate volumes
Late leaks are more often associated with factors predisposing to a weak abdominal wall (pericannular hernias) or are caused by occult tunnel track infections
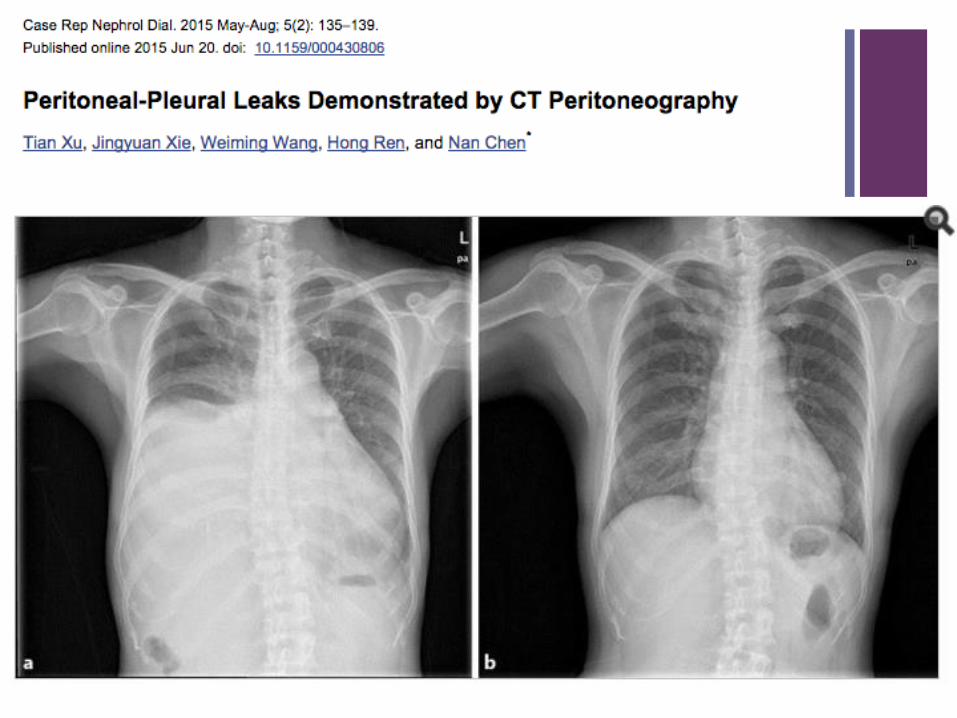
Hydrothorax – (1-2% of PD pts), less likely to resolve with disruption of PD and best success rates with thorascopic pleurodesis (3)
Diagnosis – CT peritoneography or peritoneal scintigraphy
Treatment – Typically will seal with temporary disruption of PD
+


+Hernias
PD is a known risk factor for the development of hernias, with reported incidences of 2-25% (4-6). ESRD pts will also have pre-existing hernias. This is considered a contraindication to PD and therefore must be fixed prior to starting PD.
General principles:
Reduce the peritoneal sac without entering it
Mesh repairs in a tension-free manner with mesh placed outside the peritoneal cavity and with wide overlap
Onlay, intraparietal, pre-peritoneal
Alternative?: IPOM w/ Zenapro
Hernia repairs are done at the same time as PD catheter placement (7)
If needed, can start PD immediately at low volumes w/ apparent good outcomes (8-10)
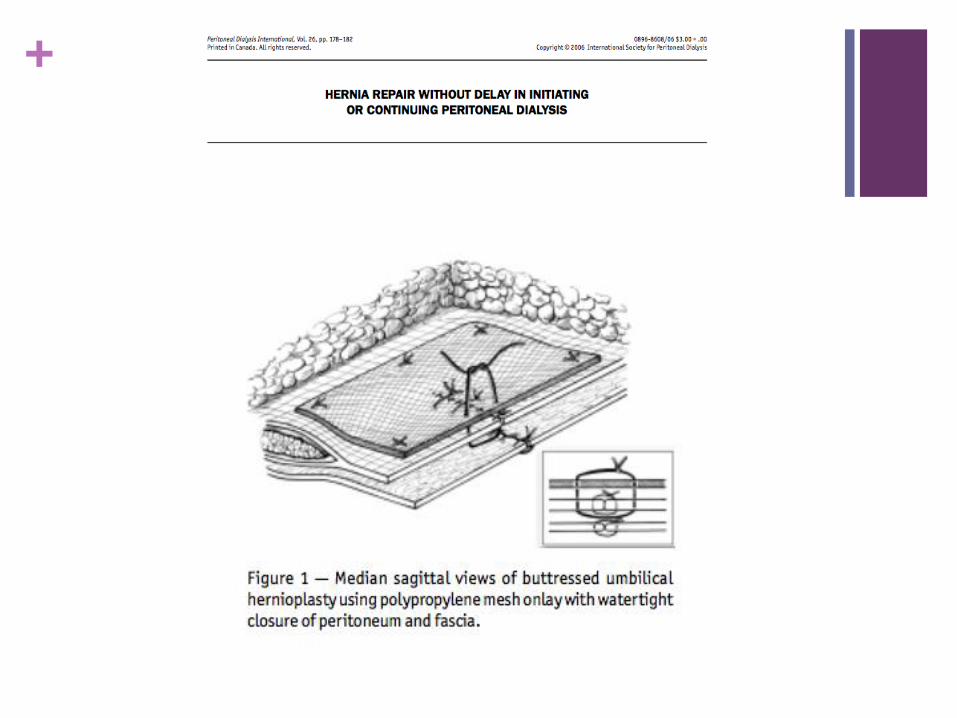
+Umbilical hernias
Most common acquired hernia in PD patients (11-16)
< 1 cm – My practice - primary repair at time of procedure
with an Endoclose
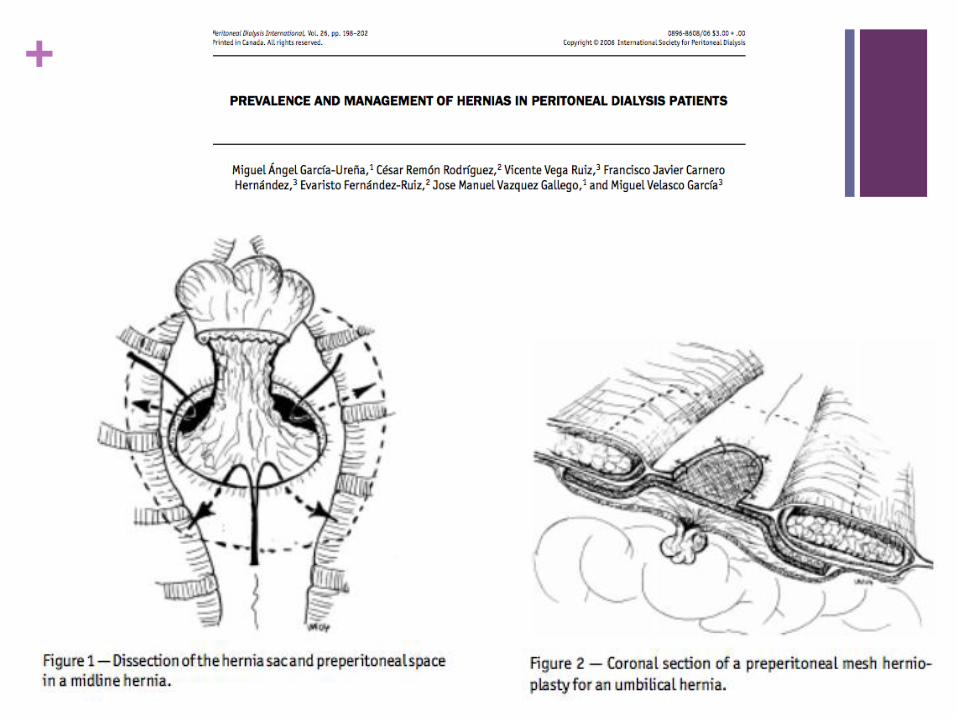
1 - 3 cm – Onlay mesh hernioplasty (17) versus pre-
peritoneal or H mesh hernioplasty (11)
> 3 cm – Retro-rectus type repair (8)
+
+
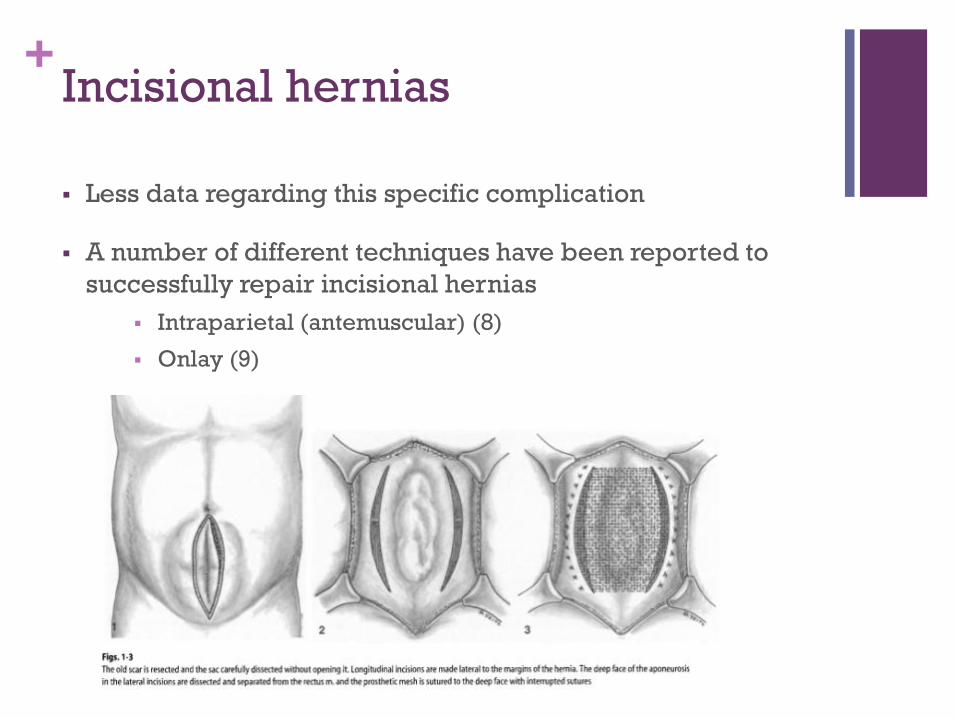
+Incisional hernias
Less data regarding this specific complication
A number of different techniques have been reported to
successfully repair incisional hernias
Intraparietal (antemuscular) (8)
Onlay (9)

+Inguinal
Open repair with mesh concurrently with PD catheter
placement
Avoid intra-parietal mesh and making rents in the
peritoneum with a TEP or TAPP
Avoid disrupting the space used for catheter tunneling
+Pericatheter hernias
These catheters must be replaced and the hernia fixed
according to the principles discussed
+Low Volume PD for Early Starts
Has been suggested by authors to wait a period of time after
hernia repair to start PD. However, in those patients currently
on PD where the decision was made not to wait, results have
been favorable without dialysate leaks using a low volume
protocol (11, 18)
“Our” protocol:
Supine, low volume PD (~1L) 3-5 times per week for 2 weeks
prior to transitioning to home
+Prevention!!!
Utilize a technique developed and taught by Dr. John Crabtree –adopted by all surgeons at UWMC/HMC
Preoperatively mark creases/pants line, check handedness
Laparoscopic approach using 5 mm camera and 2nd 5 mm port
Check for hernias initially and repair concurrently if found
Perform an omentopexy for every patient
Place the catheter with a preperitoneal tunnel using a 7/8 mm Versaport
Downward facing exit site
Check inflow/outflow and additionally flush with heparinized saline
+References
1. Hagen SM, Lafrana JA, Steyerberg EW, IJzermans JN, Dor FJ. Laparoscopic versus open
peritoneal dialysis catheter insertion: a meta-analysis. PLoS One. 2013; 8(2):e56351.
2. Yilmazlar T, Kirdak K, Bilgin S, Yavuz M, Yurtkuran M. Laparoscopic findings of
peritoneal dialysis catheter malfunction and management outcomes. Perit Dial Int.
2006; 26:374-9.
3. Xu T, Xie J, Wang W, Ren H, Chen N. Peritoneal-pleural leaks demonstrated by CT
peritoneography. Case Rep Nephrol Dial. 2015; 5(2):135-9.
4. Nelson H, Lindner M, Schuman ES, Gross GF, Hayes JF. Abdominal wall hernias as a
complication of peritoneal dialysis. Surg Gynecol Obstet. 1983; 157(6):541-4.
5. Hussain SI, Bernardini J, Piraino B. The risk of hernia with large exchange volumes. Adv
Perit Dial. 1998; 14:105-7.
6. O’Connor JP, Rigby RJ, Hardie IR. Abdominal hernias complicating continuous
ambulatory peritoneal dialysis. Am J Nephrol. 1986; 6(4):271-4.

+References
7. Sodo M, Bracale, U, Argentino G, Merola G, Russo R, Sannino, G, Strazzullo T, Russo D. Simultaneous abdominal wall defect repair and Tenckhoff catheter placement in candidates for peritoneal dialysis. J Nephrol. 2015; Nov 13, epub
8. Guzman-Valdivia G, Zaga I. Abdominal wall hernia repair in patients with chronic renal failure and a dialysis catheter. Hernia 2001; 5:9-11.
9. Imvrios G, Tsakiris D, Gakis D, Takoudas D, Koukoudis P, Papadimitriou M et a. Prosthetic mesh repair of multiple recurrent and large abdominal hernias in continuous ambulatory peritoneal dialysis patients. Perit Dial Int. 1994; 14:338-43.
10. Gianetta E, Civalleri D, Serventi A, Floris F, Marianai F, Aloisi F et al. Anterior tension-free repair under local anaesthesia of abdominal wall hernias in continuous ambulatory peritoneal dialysis patients. Hernia. 2004; 8:354-7.
11. Garcia-Urena MA, Remon Rodriguez C, Vega Ruiz V, Carnero Hernandez FJ, Fernandez-Ruiz E, Vazquez Gallego JM, et al. Prevalence and management of hernias in peritoneal dialysis patients. Perit Dial Int. 2006; 26:198-202
12. Afthentopoulos IE, Panduranga RS, Mathews R, Oreopoulos DG. Hernia development in CAPD patient and the effect of 2.5 L dialysate volume in selected patients. Clin Nephrol. 1998; 9:307-8

+References
13. Lupo A, Tarchini R, Gegoloni GP, Gentile MG, Cancarini G, Gellin G et al. Abdominal hernia in CAPD patients: incidence, risk factors and outcome. Adv Perit Dial. 1988; 4:107-9
14. Suh H, Wadhwa NK, Cabralda T, Sokunbi D, Pinard B. Abdominal wall hernias in ESRD patients receiving peritoneal dialysis. Adv Perit Dial. 1994; 10:85-5.
15. Cherney DZI, Siccion Z, Chu M, Bargman JM, Natural history and outcome of incarcerated abdominal hernias in peritoneal dialysis patients. Adv Perit Dial. 2004; 20:86-9.
16. Del Paso G, Bajo MA, Costero O, Hevia C, Gil F, Diaz C et al. Risk factors for abdominal wall complications in peritoneal dialysis patient. Peri Dial Int. 2003; 23:249-54.
17. Crabtree JH. Hernia repair without delay in initiating or continuing peritoneal dialysis. Peri Dial Int. 2006; 26:178-182.
18. Shah H, Chu M, Bargman J. Perioperative management of peritoneal dialysis patients undergoing hernia surgery without the use of interim hemodialysis. Peri Dial Int. 2006; 26:684-7.