niv vs high flow oxygen
TRANSCRIPT

NIV vs. High flow oxygen in Acute respiratory failure in Immunocompromised patients.
Tajamul hussain shah
Department of Pulmonary and sleep disordersAIIMS

Respiratory failure in Immunocompromised • Acute respiratory failure (ARF) remains the leading reason
for intensive care unit (ICU) admission of immunocompromised patients.
• Often require mechanical ventilation
• IMV in immunocompromised is associated with significant mortality.
• 60% solid malignancy, 40% Immunosupressive Rx
Crit Care 2011, 15:R91 Crit Care Med 1984;12:26-8.

Role of Non invasive ventilation • There are few Randomized control trails and
many retrospective studies that showed • Use of NIPPV in such subset of patients
results in reduced use of Mechanical ventilation and mortality.


Conclusion

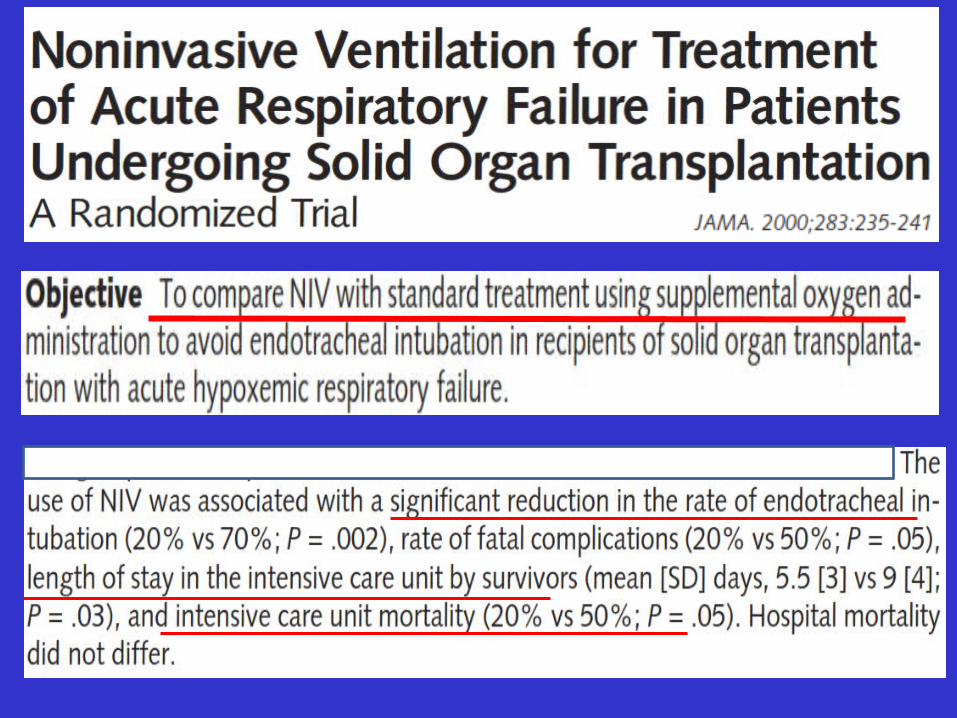
• Objective of study To compare Non invasive positive pressure ventilation vs. Invasive mechanical ventilation in AIDS patient with PCJ related Acute hypoxemic respiratory failure

• Use of NIPPV avoided intubation in 67% of pts.• Improved survival (100% vs. 38% ; p=0.003).• NPPV treated patients required fewer invasive
devices (p= <0.001)) and lower incidence of pneumothorax (8.3% vs. 37.5%; p= 0.039).
• NPPV group had lower ICU and hospital mortality.

Conclusion






Current study

Aim of the Study
• To determine whether early non-invasive ventilation improved survival in immunocompromised patients with non hypercapnic acute respiratory failure

Study design
• Study was done from AUG 2013 to JAN 2015.• Patients were recruited from 28 hospitals in
France and Belgium.
• The study protocol was approved by French Ethics committee, French health authorities' and the ethics committees of 2 Belgian hospitals.
• Informed consent was obtained from all patients.
• The study was foreseen by independent data and safety monitoring board.

Patients • Patients were recruited in 28 ICUs where the staff had
considerable experience and expertise with immunocompromised patients and noninvasive ventilation.
• Eligibility criteria1. 18 years or older 2. Acute hypoxemic respiratory failure3. Duration of respiratory symptoms < 72 hours4. Immuno-deficient patients

Contraindication of NIPPV• Those patients who fulfilled above Eligibility criteria where
assessed for contraindications of NIPPV.
• Exclusion criteria – Hyper-carbia (> 50 mmHg).– Need for immediate mechanical ventilation.– Cardiogenic acute pulmonary edema.– Acute coronary syndrome.– Requirement of inotropic support.– GCS <13– Do not intubate decision – On long term oxygen, pregnant and lactating women.

Randomization
• Enrolled patients were randomly assigned in a 1:1 ratio to receive either noninvasive ventilation or oxygen throughout the ICU stay.
Randomization was performed in • Permuted blocks of concealed variable size Stratified by • Center of recruitment• Oxygen flow at randomization ( < or > 9L/min)• Cause of immuno-supression


• The nature of the intervention precluded blinding of the Patients and Clinicians.
• All management decisions other than the use of Noninvasive ventilation or Oxygen were made by the managing physicians according to standard practice in each ICU.
• In both groups, oxygenation modalities and the use of high flow nasal oxygen were at the clinician’s discretion.

Noninvasive ventilation was not allowed for patients allocated to the oxygen group except, if needed
• For pre-oxygenation before intubation • For up 2 hours to improve the safety of Bronchoscopy and Bronchoalveolar lavage.
In the NIV group Intervention was started immediately after randomization. The PS was adjusted to obtain an TVe of 7 to 10 mL/kg Initial PEEP of 2 and 10 cm H2O. FiO2 and PEEP levels were adjusted to maintain oxygen saturation (SpO2) at 92% or greater

• NIV was provided for at least 60-minute session every 4 hours for at least 2 days.
• Was resumed if RR was more than 25 and SPO2 <92%
• Use of NIV was stopped if signs of respiratory failure disappeared between 2 sessions of NIV.
• In between NIV sessions received Oxygen

• In both groups, intubation decisions were based on the
– Therapeutic response to initial mode of ventilation
– Clinical status (SpO2, RR, signs of respiratory distress and bronchial secretion volume)
– and Patient’s adherence to noninvasive ventilation.

Study Outcomes
The primary study outcome • All-cause mortality within 28 days after
randomization.
Secondary outcomes • Oxygenation failure (defined as endotracheal
intubation)• Sequential Organ Failure Assessment score on day 3• ICU-acquired infections• Mechanical ventilation duration and • length of ICU stay.

Statistical analysis• To detect a decrease in 28 day mortality from 35%
in oxygen group and 20% in NIV group with 90 % power 187 patients per group where needed (374)
• Kaplan Miere curves were used to assess survival and endotracheal intubation from time of enrollment.
• Continuous variables were described as medians [IQRs]) and categorical variables as proportions

• The primary outcome was compared between the 2 groups using the χ2 test

Results

All patients at randomization received standard oxygen therapy• With PaO2/FiO2 suggestive of
moderate to severe respiratory failure
• There was no lost in follow up


Causes of Immuno-Supression • ACUTE LEUKEMIA and AGGRESSIVE LYMPHOMA most common hematological malignancy. (n=238, 63.6%)• LUNG CANCER was the most common Solid
tumor (n= 79, 21.1%)• Most common organ transplant was KIDNEY
(n=24, 6.4%)• 8.8% n=33 patients had Immuno-supression
related to drugs.

• .

Non-invasive ventilation group
Median durations of NIPPV were • 8 hours (IQR, 4-11) within the first 24 hours• 6 hours (IQR, 4-8) on day 2. • 5 hours (IQR, 3-7) on day 3.
14 Patients (7.3%) received only a single session of NIPPV • 5 were subsequently intubated • 9 because they could not tolerate NIPPV
Of these 9 patients, none was intubated and all survived

Oxygen group
In the oxygen group• 3 patients (1.5%) received rescue NIV
(including 2 who were eventually intubated).
High-flow nasal oxygen was given to 141 patients overall (37.7%) and was used more often in the Oxygen group (44.3%) than in the Noninvasive ventilation group (31.4%) (P = 0.01).

• Total 142 patients underwent bronchoscopy and BAL with no significant difference between the 2 groups.
• During the ICU stay, vasopressors were required by 148 patients (39.7%) and RRT by 58 patients (15.5%), with no significant difference between groups

Oxygen saturation
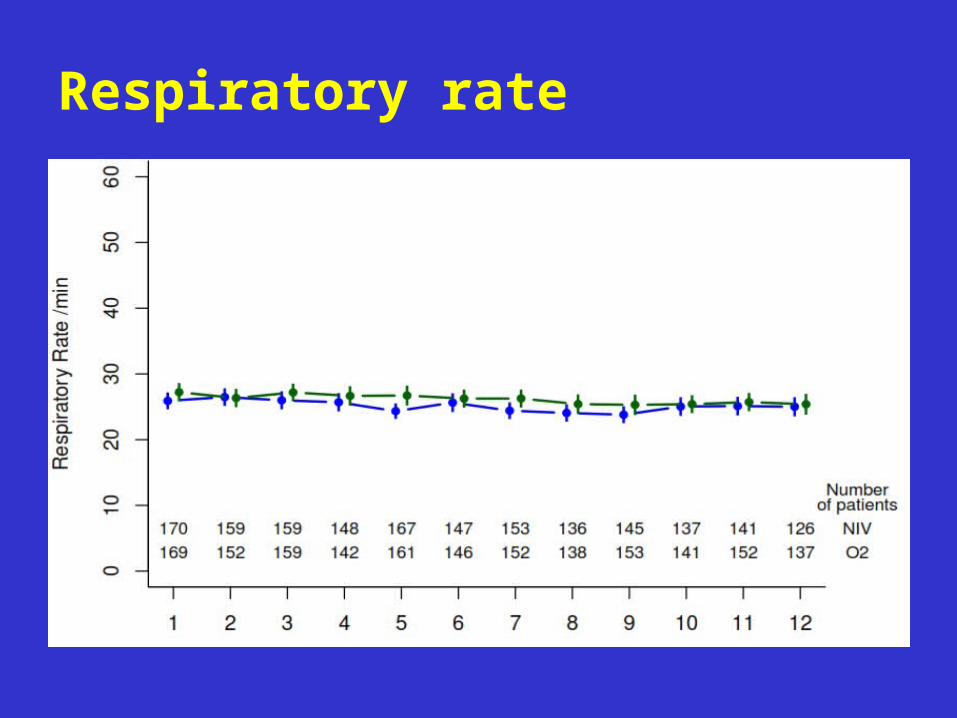
Respiratory rate

PaO2/FiO2
Median PaO2:FIO2 ratios were • 156 (IQR, 100-237) mm Hg on day 1• 169 (IQR, 108-236) mm Hg on day 2• 158 (IQR, 108-226) mm Hg on day 3 with no significant between-group difference.
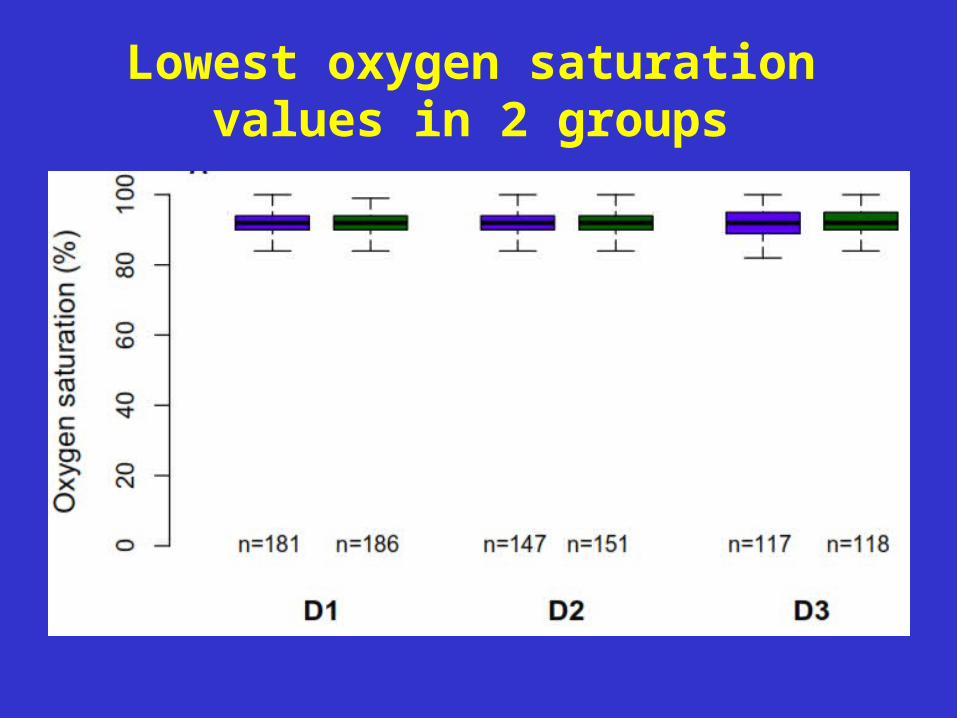
Lowest oxygen saturation values in 2 groups

Respiratory rate
Median expiratory TV were • 8.8 (IQR, 7.3-11.4) mL/kg of IBW on day 1• 9.1 (IQR, 7.20-10.7) on day 2• 9.5 (IQR,7.2-11.8) on day 3
With no significant difference according toNIV Success vs. Failure or between Survivors and Non-survivors.

Outcome

Survival at 28 days


POST HOC AnalysisNon Invasive Oxygen P value
ICU mortality 20.9% 24.6%
Hospital mortality 30.9% 34.4%
Hospital stay 24 IQR(12-43) 22 IQR(14-42) 0.99
Cancer patients Immunosuppressive treatment for OL/other
28 day mortality 27.0% 19% 0.19
< 9L /min > 9L /min
26% 31% 0.03

Cumulative incidence of Intubation in 2 groups

• Among intubated patients n= 155 With 82 (Oxygen group) 73 ( NIV group) 28 day mortality was 49.7% (77/155). 52.1% in NIV and 47.6% with O2 alone (p=0.58)
• Of the 141 patients given high-flow nasal oxygen, 15 of 60 (25.4%) died in the NIV group, vs. 26 of
81 (32.1%) in the oxygen group (P = .36).

Discussion
• In immunocompromised patients with ARF early NIV compared with oxygen therapy alone, did not reduce the primary outcome of day-28 all-cause mortality or in Subgroups
• There were no significant differences in the proportions of patients who required intubation ICU or hospital lengths of stay, or in duration of invasive mechanical ventilation.

Strength of the study• Multicenter design • Adherence to early use of NIV• In majority of the cases the etiology of ARF was
known.• There was no loss of follow up• The statistical analysis plan where published
before recruitment was completed to decrease Analytical bias.
• Primary outcome was mortality that could not be influenced by Observer bias.

Limitations
Lower than expected mortality rate with oxygen alone limited the power of our study to detect a significant between-group difference in mortality.
High-flow nasal oxygen was used in about two-fifthsof our patients and may have served to decrease the intubation and mortality rates.

Thankyou