ninth international workshop on pharmacodynamics of anticancer agents durham sept 2013
DESCRIPTION
Presentation on multi-arm, multi-stage trialsTRANSCRIPT

Adaptive Study Design Multi-Arm, Multi-Stage trials
Nicholas JamesProfessor of Clinical Oncology
University of Birmingham@Prof_Nick_James

Cancer research spending
• Half of all drugs in trials are cancer drugs• Global cancer drug market risen from $48bn
(2008) to $75bn (est 2012)• 25 drugs with sales >£1bn pa• Annual research spend:
– pharmaceutical industry $6-8 bn– NCI $3.6 bn– EU public bodies Eur 1.4 bn
• If we are to afford new drugs, we must make trials cheaper and quicker

Research environment
• New treatments usually not better than current– About 30 to 40% are positive – Both academia and industry
• Trials require huge time, effort and cost
• Must be a better way to select treatments for efficacy assessments

STAMPEDE Celecoxib -- ECCO 2011 [LBA20] – N Clarke
MAMS Trial DesignMulti-Stage:• Are there reasons why we
should continue investigating a treatment?– Require sufficiently
encouraging activity to continue assessment
• Focus away from insufficiently active regimens– Focus limited resources on
regimens that may benefit patients
• Add new treatments of interest
STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
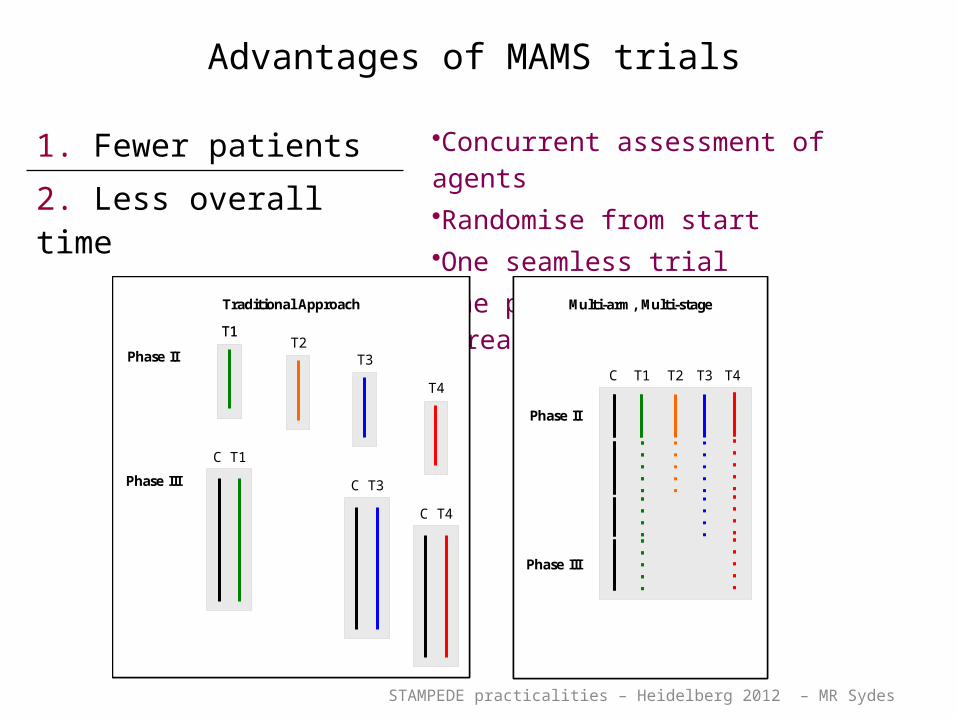
Advantages of MAMS trials
1. Fewer patients •Concurrent assessment of agents•Randomise from start•One seamless trial•One protocol Less bureaucracy
2. Less overall time
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Traditional Approach
Phase II
Phase III
T1
C T1
T2T3
C T3
T4
C T4
Traditional Approach
Phase II
Phase III
T1T1
C T1
T2T3
C T3
T4
C T4

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Advantages of MAMS trials
3. Increased flexibility •Adapts to intermediate results•Focus on more promising arms
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Traditional Approach
Phase II
Phase III
T1
C T1
T2T3
C T3
T4
C T4
Traditional Approach
Phase II
Phase III
T1T1
C T1
T2T3
C T3
T4
C T4

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Advantages of MAMS trials
4. Reduced costs •Limited resources for trials•Must use fairly and efficiently
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Multi-arm, Multi-stage
T2 T3T1C T4
Phase II
Phase III
Traditional Approach
Phase II
Phase III
T1
C T1
T2T3
C T3
T4
C T4
Traditional Approach
Phase II
Phase III
T1T1
C T1
T2T3
C T3
T4
C T4

STAMPEDE Celecoxib -- ECCO 2011 [LBA20] – N Clarke
MAMS Trial Design
Multi-Arm:• Start randomising from the outset
• Assess many promising agents simultaneously– Compared to a common control arm
Multi-stage
• Incorporate interim activity assessments– Phase II type assessments of each research arm

STAMPEDE Celecoxib -- ECCO 2011 [LBA20] – N Clarke
Clinical Setting
• Men with metastatic or high-risk non-metastatic prostate cancer
• Long-term hormone therapy (HT) alone is the standard of care
• Investigating whether early use of additional therapies can improve overall survival
• Many interesting agents demand assessment– No clear reason to choose one particular regimen– Do not want to choose arbitrarily– Want to assess all interesting agents
• Focussed on three distinct initial treatments

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
STAMPEDE outcome measuresOutcome Measure
Stage Primary Secondary
Pilot Safety Feasibility
Activity I-III Failure-free survival Overall survival
(phase II) Toxicity / safety
Skeletal events
Efficacy IV Overall survival Failure-free survival
(Phase III) Toxicity / safety
Skeletal events
Quality of life

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Trial design
Stage Type 10 OM HRA Power Sig. Critical HR
Control Events
1 Activity FFS 0.75 95% 0.500 1.00 114
2 Activity FFS 0.75 95% 0.250 0.92 215
3 Activity FFS 0.75 95% 0.100 0.89 334
4 Efficacy OS 0.75 90% 0.025 - 400
85% 0.013
FFS: failure-free survivalOM: outcome measureOS: overall survival
Overall (per comparison)
• Stop early for lack-of-benefit on intermediate primary OM
• Stop early for benefit only on definitive primary OM

FEASIBILITY ASSESSMENT

STAMPEDE trial
• Launched 2005• Initial feasibility stage:
– Would patients accept randomisation between 6 treatment arms?
– Would clinicians put the time into the study to make it work?
– Would the chosen treatments be safe?

STAMPEDE original design
RANDO
MIS
ATIO
N
AAndrogen Deprivation Therapy
B ADT + Zoledronic Acid
C ADT + Docetaxel
D ADT + Celecoxib
E ADT + ZA + Doc
F ADT + ZA + Cel
Control arm
Treatment detail
Androgen Deprivation Therapy:: Standard hormones :: Given for >3 year
Zoledronic Acid:: 3rd generation bisphosphonate:: IV for 2 years every 3 to 4 weeks
Docetaxel:: Taxane chemotherapy:: IV for 6 cycles over 18 weeks
Celecoxib :: Cox-2 inhibitor:: Oral for 1 year
Man with high-risk prostate cancer starting long-term hormone therapy
MRC PR08
CRUK/06/019
ISRCTN78818544
NCT00268476

Slides for Kim Chi and NCIC CTG: Oct-2011
Accrual: start
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
ADT-aloneA
ADT + zoledronic acidB
ADT + docetaxelC
ADT + celecoxibD
ADT + zoledronic acid + docetaxelE
ADT + zoledronic acid + celecoxibF
Past accrual
Possible future accrual Follow-up

ADT + docetaxel
ADT-alone
ADT + zoledronic acid
ADT + celecoxib
ADT + zoledronic acid + docetaxel
ADT + zoledronic acid + celecoxib
Accrual: end of Pilot Phase
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
B
C
D
E
F
Past accrual
Possible future accrual Follow-up
Feasibility and safety confirmed

STOPPING ARMS WITH INSUFFICIENT ACTIVITY

Slides for Kim Chi and NCIC CTG: Oct-2011
ADT-alone
ADT + docetaxel
ADT + zoledronic acid
ADT + celecoxib
ADT + zoledronic acid + docetaxel
ADT + zoledronic acid + celecoxib
Accrual: end of Activity Stage I
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
B
C
D
E
F
Past accrual
Possible future accrual Follow-up
All arms complete round 2 of their high jump!

Slides for Kim Chi and NCIC CTG: Oct-2011
Accrual: end of Activity Stage II
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
ADT-aloneA
ADT + zoledronic acidB
ADT + docetaxelC
ADT + celecoxibD
ADT + zoledronic acid + docetaxelE
ADT + zoledronic acid + celecoxibF
Past accrual
Possible future accrual Follow-up
Celecoxib fails round 3 of its contest

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
AS 2 analysis (original arms)
• Data frozen: 01-Feb-2011• IDMC meeting: 31-Mar-2011 • Accrual: 2043 patients total• FFS events: 209 on control arm (target 215)
• IDMC recommended changes:: Stop accrual to 2 arms due to lack-of-benefit
• Both celecoxib-containing arms (D and F)
: Remaining arms to continue accrual into their Activity Stage III
• Arms B, C and E, plus control arm A
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017

STAMPEDE Celecoxib -- ECCO 2011 [LBA20] – N Clarke
Failure-free Survival
Adjusted HR: 0.94
(95%CI 0.74-1.20)
(1-sided upper 75% upper CI 1.03)
Target HR: 0.924
Unadjusted HR = 0.98
2-year FFS 50% (As predicted)

ADDING NEW AGENTS

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Flexibility and extension
• Design adapts to include further agents– Can add new research arms during trial
• Might see as a new trial within STAMPEDE protocol
• Must be scientifically compelling case for inclusion– Proposed through Trial Management Group– Survey of participants – Peer review through original funder (Cancer Research
UK)

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Principles• First priority is to ongoing research arms
– Must not hamper accrual or maturity so must either: 1. Recruit better than predicted overall 2. Wait for arms to have “dropped out”
• Accept that new arm will mature later than original research arms
• Need to extend accrual to control arm
• Only compare patients on new arms to patients recruited contemporaneously to control arm

Criteria for new arms
• Existing or pending licence in prostate cancer• Deliverable across all (or most) trial centres• (Pharmaceutical partner willing to support with drug
and distribution costs)
Model for introduction• Draw up draft agreement with partner organisation(s)• Needs clinical leader – effectively the CI for the new
substudy• Apply to CRUK for extension of trial

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Advantages?1. Can start recruiting quicker than a new trial
– Updated protocol = simple, substantial amendment – Scientific review = amendment
2. Efficient use of volunteers– Patients contribute to more than one comparison – Reduce competing trials– Seamless accrual: no gaps between “trials”
3. Efficient use of resources– Much quicker start-up time: Start at “full speed”– Much cheaper than separate trial– Get answers more quickly

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Disadvantages?
1. Original research arms could mature whilst new assessment ongoing– Treat like data emerging from an external trial– TMG will reacts if needed– Update backbone of therapy across arms if
required
– Already done for some M0 patients in STAMPEDE: added RT to ADT following published data from SPCG-7 & MRC PR07/NCIC PR.3

STAMPEDE trial design
Composition of arms• Abiraterone added Nov
2011
R
A
N
D
O
M
I
S
E
Androgen suppression (AS)
A
B
C
D
E
Control arm
R
A
N
D
O
M
I
S
E
Hormone Therapy (HT)
A
HT + zoledronic acidB
HT + docetaxelC
D
HT + zoledronic acid + docetaxel
E
Control
HT + abirateroneG

Slides for Kim Chi and NCIC CTG: Oct-2011
Accrual: from Nov-2011
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
ADT + celecoxibD
ADT + zoledronic acid + docetaxelE
ADT + zoledronic acid + celecoxibF
ADT + abirateroneG
ADT-alone
Past accrual
Possible future accrual Follow-up

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Local approvals of new comparison
Ready on act ivat ion Suspended unt il ready
Activ
ation
day
0.0
0.2
0.4
0.6
0.8
1.0
Ppn
site
s re
ady:
R&
D a
ppro
val c
onfir
med
104 98(6) 77(21) 58(19) 47(11) 21(26) 13(8) 13(0) 12(1) 11(1) 7(4) 7(0) 7(0) 7(0) 6(1) 3(3)approval
Sit es needing
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15Time (weeks) from notifying sites
Timely R&D approval for new protocol
New arm “switched on” for whole trial on set date
Sites given ~4 wk notice to gain local approvals
80 sites ready to recruit on activation day!
Accrual nearly seamless

Accrual to new arms
Closure of original arms

Cost
• Faster set up• Lower cost as
shared between arms
• New funder needs to provide red area costs, no cost to original funder for “extra” trial
2 arms
Duration of trial
Trial 1
2 armsTrial 2
2+1 arms
Duration of trial
MAMS trial
Slides for Kim Chi and NCIC CTG: Oct-2011
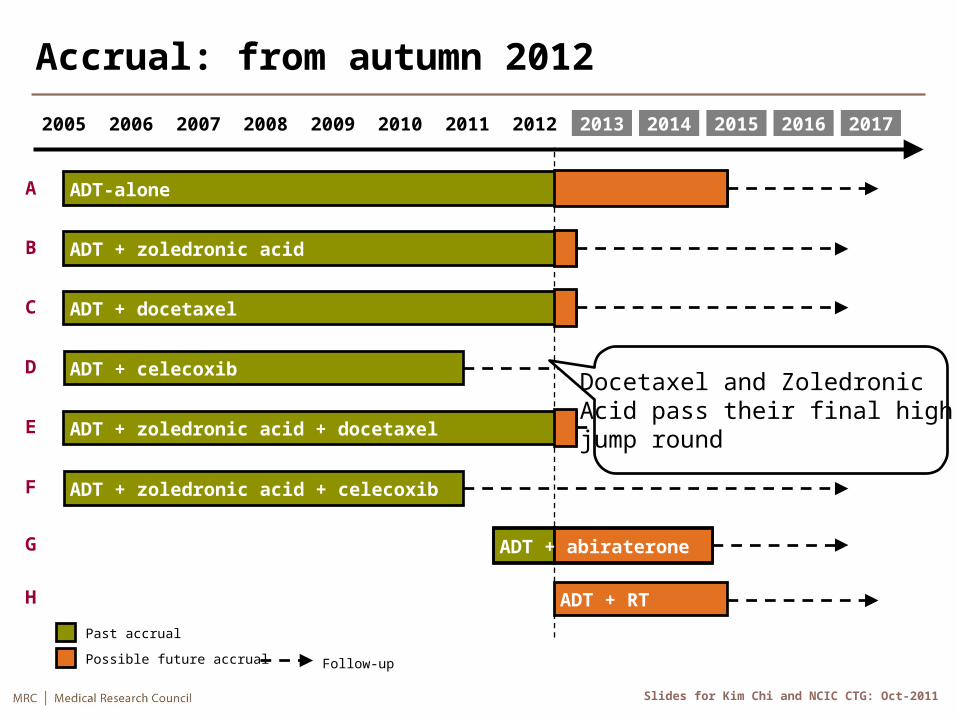
Accrual: from autumn 2012
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
ADT + celecoxibD
ADT + zoledronic acid + docetaxelE
ADT + zoledronic acid + celecoxibF
ADT + abirateroneG
ADT-alone
H ADT + RT
Past accrual
Possible future accrual Follow-up
Docetaxel and Zoledronic Acid pass their final high jump round

ADDING FURTHER NEW AGENTS

Adding a randomisation to a subgroup
• Prostate radiotherapy standard of care in locally advanced cases
• Of unproven benefit but of interest in M1 cases
NEWLY DIAGNOSED M1 PATIENTS1
A ADT
G ADT + abiraterone
ALL OTHER PATIENTS2
RANDOMISATION
A ADT
G ADT + abiraterone
H ADT + RT to prostate
RANDOMISATION
Patients eligible for STAMPEDE

WHAT’S THE CONTROL ARM?

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Analysis: ZA comparison2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
M1 only ADT + RT
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone
• Fully powered: accrued through AS4

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Analysis: Docetaxel comparison2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
ADT + RT
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone
M1 only
• Fully powered: accrued through AS4
STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
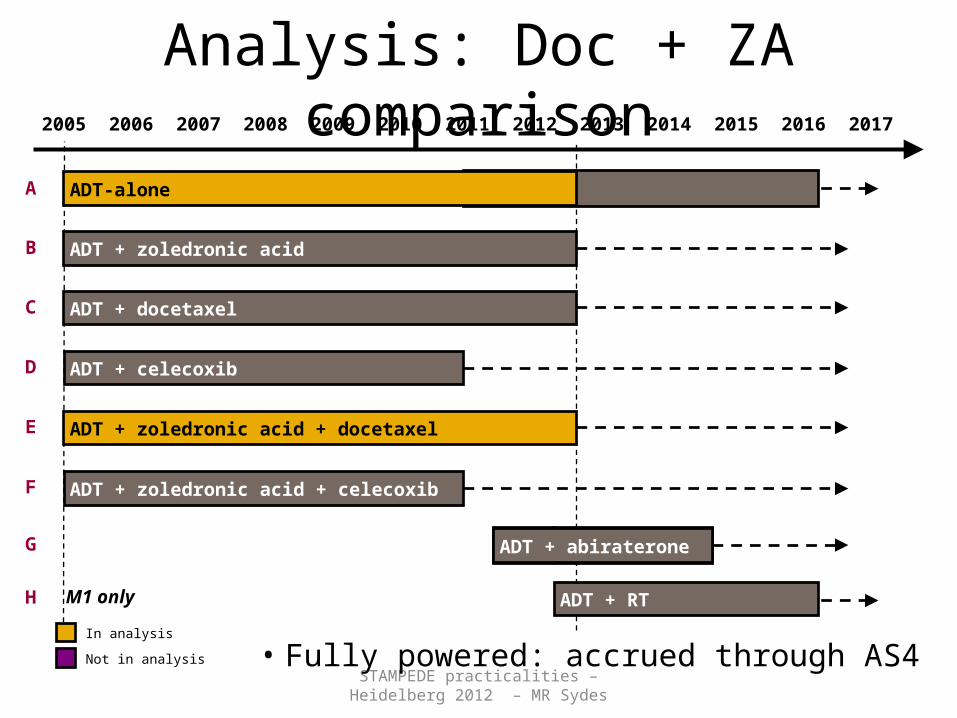
Analysis: Doc + ZA comparison2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
ADT + RT
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone
M1 only
• Fully powered: accrued through AS4

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Analysis: Celecoxib comparisons2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
ADT + RT
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone
M1 only
• Less power: stopped accrual in AS2

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Analysis: Abiraterone comparison2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
ADT + RT
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone
M1 only
• Recruitment in Efficacy Phase 2

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Analysis: M1/RT comparison2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
A
ADT + zoledronic acidB
ADT + docetaxelC
D
ADT + zoledronic acid + docetaxelE
F
ADT + abirateroneG
H
In analysis
Not in analysis
ADT + RT (M1-only)
ADT + celecoxib
ADT + zoledronic acid + celecoxib
ADT-alone (M1-only)
M1 only
• Recruitment in Feasibility Phase

STAMPEDE trial• One question answered – celecoxib probably
not of value in prostate cancer• Docetaxel and zoledronic acid completed
intermediate efficacy tests FFS and OS data are awaited
• Trial expanded twice to add abiraterone, RT in M1 disease
• Potentially can add arms indefinitely and use as a programmatic platform
STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Conclusions
• MAMS trials speed evaluation of new treatments by:1. Testing many treatments simultaneously2. Using LOB analyses to focus research efforts
• Insufficiently active arms can successfully be stopped seamlessly in a MAMS trial
• Adding new research arms to an ongoing trial is achievable and desirable
• Addition of arms to subgroups feasible and effective e.g. – Stage– Pattern of metastasis– Biomarkers – none yet tested in Stampede but possible in theory

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Refs: MAMS trials
• Royston P, Parmar MKB, Qian W Novel Designs for Multi-Arm Clinical Trials with Survival Outcomes, with an Application in Ovarian Cancer. Statistic Med 2003; 22: 2239–2256
• Barthel FMS, Royston P, Parmar MKBA menu-driven facility for sample size calculation in multi-arm, multi-stage randomised controlled trials with a survival-time outcome. The Stata Journal 2009; 9 (4): 505-523
• Parmar MKB, Barthel F, Sydes MR et alSpeeding up the Evaluation of New Agents in Cancer. J Natl Cancer Inst 2008; 100 (17):1204-1214

STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Refs: STAMPEDE methods & data• Sydes MR, Parmar MKB, James ND et al Issues in applying multi-
arm multi-stage (MAMS) methodology to a clinical trial in prostate cancer: the MRC STAMPEDE trial. Trials 2009; 10 (39)
• James ND, Sydes MR, Parmar MKB et al Celecoxib plus hormone therapy versus hormone therapy alone for hormone-sensitive prostate cancer: first results from the STAMPEDE multiarm, multistage, randomised controlled trial. The Lancet Oncology 13(5): 549-558
• Parker, C et al Prostate radiotherapy for men with metastatic disease: a new comparison in the STAMPEDE trial. BJU Int. 2013; 111(5):697-9 and Clin Onc editorial 2013; 25(5): 318-320
STAMPEDE practicalities – Heidelberg 2012 – MR Sydes
Acknowledgements• Matt Sydes and Max Parmar – MRC CTU• Noel Clark and Malcolm Mason – Study Vice Chairs
• Funding: – Cancer Research UK (CRUK/016/09)– Novartis – free drug & educational grant– Sanofi-Aventis – discounted drug & educational grant – Pfizer – free drug & educational grant– Janssen – free drug & educational grant– MRC – core funding
• All clinicians and hospital staff who have supported and continue to support the trial
• All patients who joined the trial and their families