nicola petrosillo - nadirex · 2015-11-26 · agrawal m et al. j clin gastroenterol 2015 aug 26 the...
TRANSCRIPT

L’infezione da
C difficile grave o
complicata
Nicola PetrosilloIstituto Nazionale per le Malattie Infettive
“Lazzaro Spallanzani”, IRCCS
Roma

Bagdasarian N et al. JAMA 2015; 313: 398-408

European Society of Clinical Microbiology and Infectious Diseases
(ESCMID): update of the treatment guidance document for Clostridium
difficile infection (CDI)
Debast SB et al. Clin Microb Infect 2013

Bagdasarian N et al. JAMA 2015; 313: 398-408

Surgical evaluation in CDI
• Prompt surgical evaluation should be
obtained in patients with complicated CDI
• Early intervention can reduce mortality
• Subtotal or total colectomy with end
ileostomy is often performed when surgery
is required, although there are newer colon-
preserving techniques.

Stewart DB et al. Colorectal Dis 2013;15:798-804
Fulminant CDC is defined as disease of such severity
as to require any one of the following:
1. Admission to the ICU;
2. Consideration for surgery, or
3. Death due to CDC


Burning issues:
Metro vs Vanco
Mono vs Combo

Li R et al. PLoS ONE 2015;10(10): e0137252
Metronidazole vs vancomycin for mild CDI

Li R et al. PLoS ONE 2015;10(10): e0137252
Metronidazole vs vancomycin for severe CDI

Li R et al. PLoS ONE 2015;10(10): e0137252
Metronidazole vs combination therapy

Li R et al. PLoS ONE 2015;10(10): e0137252
Metro vs vanco for
CDI recurrence

Rokas KEE et al. Clin Infect Dis 2015; 61:934-41
Vanco 125x4 os (82%)
Metro 500x3 IV (72%)

Rokas KEE et al. Clin Infect Dis 2015; 61:934-41

Louie TJ et al. Clin Infect Dis 2015;60:S91–7
Tolevamer C difficile persisted in high counts during treatment
Both vancomycin and metronidazole suppressed microbiome
components during treatment of CDI

Louie TJ et al. Clin Infect Dis 2015;60:S91–7

Louie TJ et al. Antimicrob Agents Chemother 2009; 53: 261-3

Bagdasarian N et al.
JAMA 2015; 313:
398-408.

“All disease begins in the gut”Hippocrates 460 BC – c. 370 BC

Gerding DN et al. Clin Infect Dis 2010 ;51:1306-13


Probiotics

• ~3,000 patients aged ≥65 years who were receiving antibiotics
• Probiotic capsule × 21 days
Probiotics for prevention of CDI in older inpatients
A multicentre, randomised, double-blind, placebo-controlled trial
• “No evidence that a multistrain preparation of lactobacilli and bifidobacteria was effective” in prevention of antibiotic associated diarrhoea or CDI
Allen SJ, et al. Lancet 2013; doi:10.1016/S0140-6736(13)61218-0.

Faecal microbiota transplantation (FMT)
Image reproduced with permission from Syates21, via Wikimedia Commons
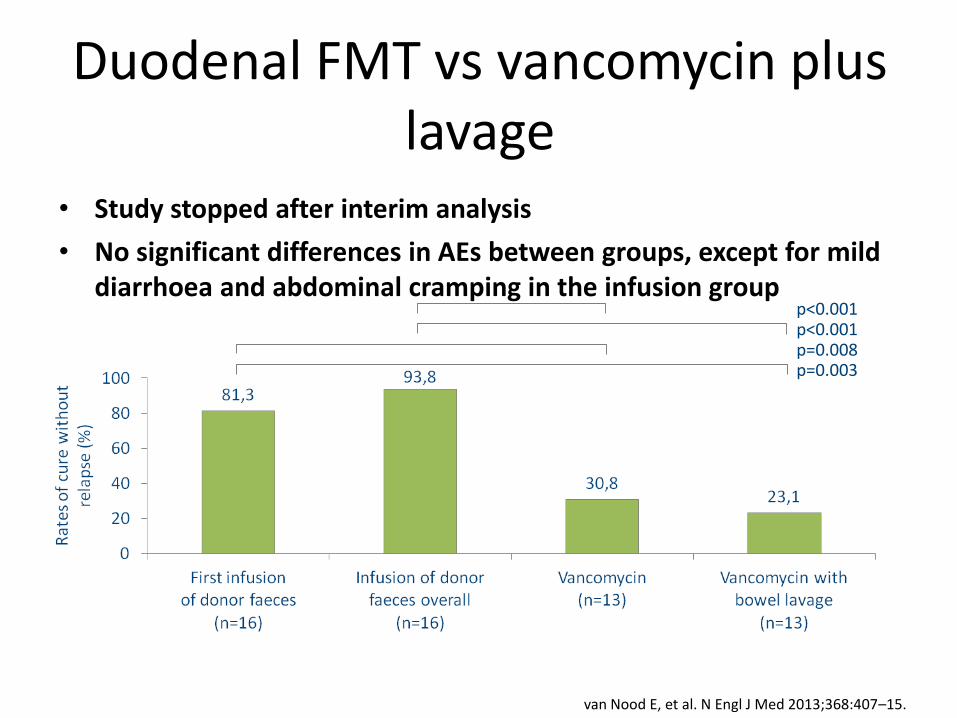
• Study stopped after interim analysis
• No significant differences in AEs between groups, except for mild diarrhoea and abdominal cramping in the infusion group
Duodenal FMT vs vancomycin plus lavage
p<0.001p<0.001p=0.008p=0.003
van Nood E, et al. N Engl J Med 2013;368:407–15.

Agrawal M et al. J Clin Gastroenterol 2015 Aug 26
The Long-term Efficacy and Safety of Fecal Microbiota
Transplant for Recurrent, Severe, and Complicated
Clostridium difficile Infection in 146 Elderly Individuals.
• A multicenter, long-term follow-up study was performed
with demographic, pre-FMT, and post-FMT data collected
from elderly patients with RCDI, SCDI, and CCDI, through
a 47-item questionnaire.
• 146 patients
• FMT was performed for RCDI in 89 (61%), SCDI in 45
(30.8%), and CCDI in 12 (8.2%) patients.
• The primary and secondary cure rates were 82.9% and
95.9%, respectively.
• Early and late recurrences occurred in 25 and 6 patients,
respectively.

Orenstein R et al.
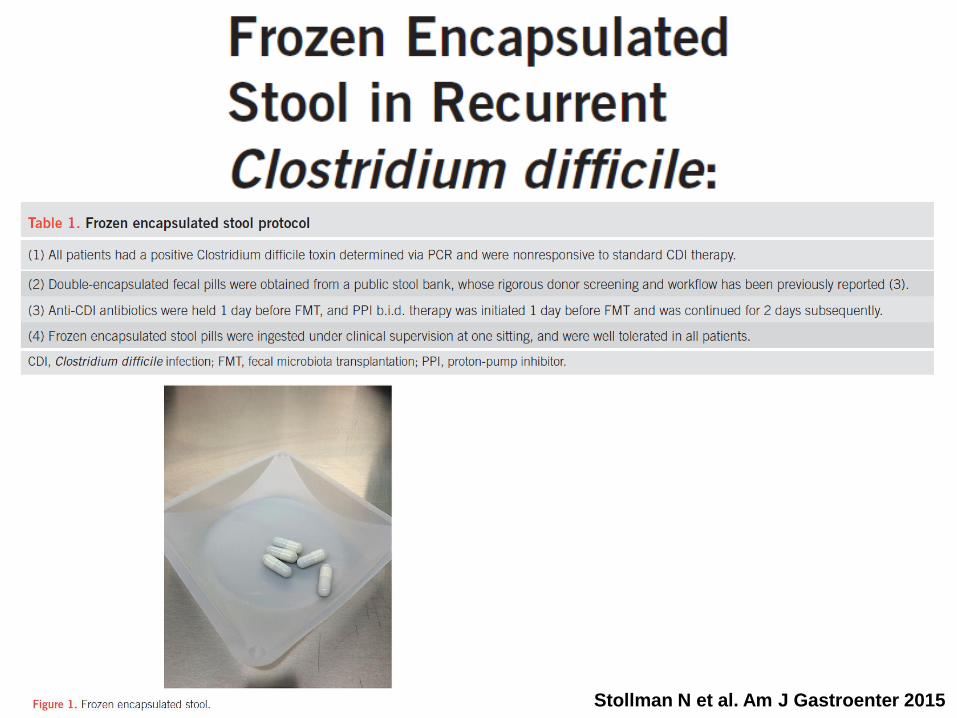
Stollman N et al. Am J Gastroenter 2015

Gerding DN et al. JAMA 2015;313(17):1719-1727
OBJECTIVE To determine the safety, fecal colonization,
recurrence rate, and optimal dosing schedule of
nontoxigenic C difficile strain M3 (VP20621; NTCD-M3)
for prevention of recurrent C difficile infection (CDI).

Gerding DN et al. JAMA 2015;313(17):1719-1727

Gerding DN et al. JAMA 2015;313(17):1719-1727

No. at riskAntibody 101 93 89 85Placebo 99 77 66 62
• Relative risk of recurrence significantly lower in the antibody group
– 0.23 (95% CI: 0.08, 0.54; p=0.01)
Monoclonal antibodies against C. difficile
Lowy I, et al. N Engl J Med 2010;362:197–205.
80
60
40
20
0Rec
urr
ence
of
infe
ctio
n (
%)
10 20Days after infusion
100
0
Placebo
40 50 60 70 80 90
Antibodyp<0.001
30


• Antibiotic inactivation is targeted at
eliminating the collateral damage associated
with the initial antibiotic exposure, thereby
potentially reducing the risk of CDI.
• As antibiotic are often necessary, the
coadministration of an agent such as SYN-
004 can inactivate the antibiotic in the large
intestine
• This approach minimize the risk of CDI and
allows the continued use of antibiotic for
prevention an treatment.

Gerding GR et al. J Antimicrob Chemother 2015 October 3
The aim of this study was to evaluate the susceptibilities of
Clostridium difficile isolates to cadazolid, a novel antibiotic
for the treatment of C. difficile infection
Patients were randomized to receive 250, 500 or 1000 mg of
cadazolid twice daily or 125 mg of vancomycin four times
daily, for 10 days.
MICs of cadazolid, vancomycin, fidaxomicin, linezolid and
moxifloxacin were determined at baseline for all patients and
post-baseline for patients with clinical failure or recurrence,
using the agar dilution method.

Bender KO et al. Sci Transl Med 2015;7:306ra148
• Cysteine protease domain (CPD) within C difficile
major virulence factor toxin B (TcdB) is a target for
experimental therapies.
• One potent CPD inhibitor, ebselen, showed a
therapeutic benefit in a mouse model of CDI

Ursodeoxycholic Acid Inhibits Clostridium difficile
Spore Germination and Vegetative Growth, and
Prevents the Recurrence of Ileal Pouchitis Associated
With the Infection.
Weingarden AR et al. J Clin Gastroenterol 2015 Oct 17
• To test whether ursodeoxycholic acid (UDCA) is
inhibitory to Clostridium difficile and can be used in the
treatment of C. difficile-associated ileal pouchitis.
• The restoration of secondary bile metabolism may be the key
mechanism for FMT in treating RCDI.
• Therefore, it is possible that exogenous administration of
inhibitory bile acids may be used directly as nonantibiotic
therapeutics for this indication.
• The need for such a treatment alternative is especially
significant in patients with refractory C. difficile-associated
pouchitis, where the efficacy of FMT may be limited.

Mizumura N et al. Intern Med 2015; 54: 1559-62