nicholson, a; kivimaki, m; aitsi-selmi, a - lshtm research online
TRANSCRIPT
Kuper, H; Nicholson, A; Kivimaki, M; Aitsi-Selmi, A; Cavalleri, G;Deanfield, JE; Heuschmann, P; Jouven, X; Malyutina, S; Mayosi,BM; Sans, S; Thomsen, T; Witteman, JC; Hingorani, AD; Lawlor,DA; Hemingway, H (2009) Evaluating the causal relevance of diverserisk markers: horizontal systematic review. BMJ, 339. b4265. ISSN1468-5833 DOI: https://doi.org/10.1136/bmj.b4265
Downloaded from: http://researchonline.lshtm.ac.uk/4552/
DOI: 10.1136/bmj.b4265
Usage Guidelines
Please refer to usage guidelines at http://researchonline.lshtm.ac.uk/policies.html or alterna-tively contact [email protected].
Available under license: http://creativecommons.org/licenses/by-nc-nd/2.5/

RESEARCH
Evaluating the causal relevance of diverse risk markers:horizontal systematic review
Hannah Kuper, senior lecturer,1 AmandaNicholson, clinical research fellow,2Mika Kivimaki, professor of socialepidemiology,2 Amina Aitsi-Selmi, academic clinical fellow in public health medicine,2 Gianpiero Cavalleri,biomedical research lecturer,3 John E Deanfield, professor of cardiology,4 Peter Heuschmann, professor,5
Xavier Jouven, professor of cardiology,6 Sofia Malyutina, professor,7 Bongani M Mayosi, professor ofmedicine,8 Susanna Sans, director of monitoring and research programme on chronic diseases,9 TroelsThomsen, consultant in preventive cardiology,10 Jacqueline C M Witteman, professor of cardiovascularepidemiology,11 Aroon D Hingorani, professor of genetic epidemiology,2 Debbie A Lawlor, professor ofepidemiology,12 Harry Hemingway, professor of clinical epidemiology2
ABSTRACT
Objectives To develop a new methodology to
systematically compare evidence across diverse risk
markers for coronary heart disease and to compare this
evidence with guideline recommendations.
Design “Horizontal” systematic review incorporating
different sources of evidence.
Data sources Electronic search of Medline and hand
search of guidelines.
Study selection Two reviewers independently determined
eligibility of studies across three sources of evidence
(observational studies, genetic association studies, and
randomised controlled trials) related to four risk markers:
depression, exercise, C reactive protein, and type 2
diabetes.
Data extraction For each risk marker, the largest meta-
analyses of observational studies and genetic
association studies, and meta-analyses or individual
randomised controlled trials were analysed.
ResultsMeta-analyses of observational studies reported
adjusted relative risks of coronary heart disease for
depression of 1.9 (95% confidence interval 1.5 to 2.4), for
top compared with bottom fourths of exercise 0.7 (0.5 to
1.0), for top compared with bottom thirds of C reactive
protein 1.6 (1.5 to 1.7), and for diabetes in women 3.0
(2.4 to 3.7) and inmen 2.0 (1.8 to 2.3). Prespecified study
limitations were more common for depression and
exercise. Meta-analyses of studies that allowed formal
Mendelian randomisation were identified for C reactive
protein (and did not support a causal effect), and were
lacking for exercise, diabetes, and depression.
Randomised controlled trials were not available for
depression, exercise, or C reactive protein in relation to
incidence of coronary heart disease, but trials in patients
with diabetes showed some preventive effect of glucose
control on risk of coronary heart disease. None of the four
randomised controlled trials of treating depression in
patients with coronary heart disease reduced the risk of
further coronary events. Comparisons of this horizontal
evidence review with two guidelines published in 2007
showed inconsistencies, with depression prioritised
more in the guidelines than in our review.
Conclusions This horizontal systematic review pinpoints
deficiencies and strengths in the evidence for depression,
exercise, C reactive protein, and diabetes as
unconfounded and unbiased causes of coronary heart
disease. This new method could be used to develop a
field synopsis and prioritise future development of
guidelines and research.
INTRODUCTION
Clinical guidelines for the prevention of coronaryheart disease are important not only because they influ-ence practice but also because they present a highlycited collation of evidence for a multitude of riskmarkers.1 2 For example, the European primary pre-vention guidelines published in 20031 mentionedmore than 40 risk markers and have been cited morethan 800 times.A fundamental problem in developing rational clin-
ical guidelines has been the lack of explicit, systematiccomparisons of the strength of causal evidence acrossthe diverse range of risk markers, which compete forclinical attention. Traditional vertical systematicreviews, which focus on one risk marker or a relativelyhomogeneous group of related risk markers, are animportant influence on the development of clinicalguidelines. However, individual risk markers may bechampioned by different experts, with few attempts atharmonising, displaying, and comparing the evidenceacross different markers. This may contribute to an adhoc selection not based on strength of causal evidence,of which risk markers beyond smoking, blood pres-sure, and cholesterol concentration are included inguidelines. The European guidelines,1 for example,did not consider atrial fibrillation, unlike the
1Epidemiology and PopulationHealth, London School of Hygieneand Tropical Medicine, LondonWC1E 7HT2Department of Epidemiology andPublic Health, University CollegeLondon Medical School, London3Molecular and CellularTherapeutics, Royal College ofSurgeons in Ireland, BeaumontHospital, Dublin, Ireland4Cardiothoracic Unit, GreatOrmond Street Hospital forChildren NHS Trust, London5Center for Stroke Research Berlin(CSB), Charité-Universitätsmedizin Berlin,Germany6INSERM, Villejuif, France7Institute of Internal Medicine,Russian Academy of MedicalSciences, Novosibirsk, Russia8Department of Medicine, GrooteSchuur Hospital and University ofCape Town, Cape Town, SouthAfrica9Instituto de Estudios de la Salud,Barcelona, Spain10Research Centre for Preventionand Health, Glostrup UniversityHospital, Glostrup, Denmark11Department of Epidemiology,Erasmus Medical Center,Rotterdam, Netherlands12MRC CAiTE centre, OakfieldHouse, Bristol
Correspondence to: H [email protected]
Cite this as: BMJ 2009;339:b4265doi:10.1136/bmj.b4265
BMJ | ONLINE FIRST | bmj.com page 1 of 11

contemporaneous American guidelines.2 The large3
and expanding array of risk markers underscores theimportance of this problem, particularly sincemany ofthe markers are of uncertain causal relevance and fewyet provide targets for prevention of disease.We developed a newmethodology of horizontal sys-
tematic review to assess causal relevance across a rangeof risk markers. We provide a high level overview ofsynthesised evidence, based on explicit criteria ofbiases and causal relevance. To show the potential ofthis approachwe focused on four riskmarkers: depres-sion, exercise, C reactive protein, and diabetes. Weselected these four markers because they differ in sev-eral respects, including conceptual domain (psycho-social marker, behavioural marker, circulatingbiomarker, defined metabolic disease), measurementproperties (presence or absence of standard instru-ments and internationally agreed definitions), andwhether exposure was endogenous (proximal in theputative causal pathway) or exogenous (more distal).We purposively selected one risk marker—diabetes—widely accepted as having an established causal role, aswell as three markers where the causal role is not uni-versally accepted. We hypothesised that concordanceof research evidence from differing research designseach with different sources of error provides the stron-gest evidence on the causal relevance of a putative riskfactor.4 Specifically, we sought evidence from threemajor study designs that offer different approaches totackling confounding and reverse causation: tradi-tional prospective observational studies with multi-variate adjustments, studies that use genetic variantsas instruments to tackle confounding (so calledMende-lian randomisation),5 6 and randomised controlledtrials where exposure to the risk marker is experimen-tally manipulated. Finally, in the light of the horizontalcomparisonwe compared the recommendationsmadefor these four riskmarkers in themost recent guidelineson prevention of coronary heart disease.
METHODS
The horizontal systematic review assesses causal rele-vance across a range of riskmarkers and study designs.We set out a priori eligibility criteria for studies, sys-tematically obtained the studies, and extracted and dis-played the data. Firstly, we separated information onrisk markers for first coronary heart disease events inpeople initially free from clinical disease and prognos-tic factors in patients with existing coronary heartdisease because of the clinical importance of distin-guishing between primary and secondary prevention.Secondly, where more than one systematic review wasidentified we displayed the largest meta-analysis orstudy (which tended to be better quality according tothe MOOSE,7 and QUORUM8 statements) in thetables of main results and included details of the othersin the web extra appendix. Thirdly, we agreed a priorithat if we could find no systematic review for any ran-domised controlled trials of the risk marker then wewould review the largest individual study. Fourthly,we stratified data extraction and synthesis by study
design (observational studies, genetic association stu-dies, and randomised controlled trials), but analysedhorizontally.
Observational studies
In January 2008we searchedMedline to identifymeta-analyses of observational studies in healthy popula-tions (aetiologic) and among patients with existing cor-onary disease (prognostic), and contacted experts.Existing coronary disease included patients with myo-cardial infarction or those undergoing coronary revas-cularisation or coronary angiography. Search termsincluded the expanded medical subject heading(MESH) of cardiovascular disease, meta-analysis as aMESH topic or publication type, and then the fourindividual risk markers as either the MESH term ortext words. English and non-English language publica-tions were eligible. Eligible outcomes were fatal coron-ary heart disease and non-fatal myocardial infarction(aetiologic and prognostic studies) and, for prognosticstudies only, all cause mortality. Meta-analyses wereonly eligible for inclusion if they reported summaryestimates based on longitudinal studies.Two reviewers (HK and AAS) extracted data, with
recourse to a third reviewer in the event of disagree-ment. We extracted summary data on prespecifieditems: age adjusted (or unadjusted) relative risks with95% confidence intervals; adjusted relative risks with95% confidence intervals; number of studies adjustingfor smoking, blood pressure, and cholesterol concen-tration (aetiologic) or disease severity (prognostic);attenuation between age and multivariate adjustedrelative risks; the prevalence of exposure in individualstudies; the methods used to measure exposure; thenumber and type of outcomes; the level of meta-analy-sis (literature only, or pooled analysis of individual par-ticipant data across the studies); measure ofheterogeneity; whether separate estimates werereported among people aged over 75 years, women,or non-Western populations; evidence of the presenceof a dose-response relation—that is, extending beyonddichotomous comparisons; the extent to which theduration of follow-up influenced the strength of theestimates (if effects are stronger with shorter periodsof follow-up this is consistent with reverse causality);and evidence of publication bias.
Genetic studies
We searched for meta-analyses of the associationsbetween genotype and each of the four individual riskmarkers through Medline using gene as the MESHterm or text words or Mendelian in any field; meta-analysis as a MESH topic or publication type; andthen the four individual risk markers as either theMESH term or text words. To identify meta-analysesof the association between genotype and coronaryheart disease outcome we searched individual singlenucleotide polymorphisms in all fields identifiedfrom recent systematic reviews for depression(SLC6A4, MTHFR, APOEw1), the CRP gene,w2 andtype 2 diabetes (TCF7L2, FTO, CDKN2A/
RESEARCH
page 2 of 11 BMJ | ONLINE FIRST | bmj.com

CDKN2B, PPARG, ICF2BP2, KCNJ11, HHEXIDE,CDKAL1, SLC30A8w3) together with expandedMESH headings of cardiovascular disease and meta-analysis as a MESH topic or publication type. Foreach variant two independent reviewers (HH andAN) extracted information on prespecified items:whether the single nucleotide polymorphismwas iden-tified fromgenomewide scans, the number of outcomeevents, the number of studies in the meta-analysis,unadjusted relative risks (95% confidence intervals),and whether there was a formal test on the use of thegenetic variant as an instrumental variable.6
Randomised trials
Randomised controlled trials and meta-analyses ofthese were identified through searches of Medline.Search terms included theMESH heading of coronaryheart disease or CHD or myocardial infarction or MI;trial as a MESH heading; the four individual risk mar-kers as either theMESH term or text words; andmeta-analysis or systematic review as a MESH heading orreview as a publication type. Given the importance ofevidence from randomised controlled trials to informguidelines, we accepted individual trials where nometa-analyses were available. We also searchedthrough the reference list from the guideline publica-tions to identify relevant randomised controlled trials.Only randomised controlled trials that reported coron-ary heart disease event outcomes were eligible (aetio-logic and prognostic studies) or death in the setting ofpatients with coronary heart disease (prognostic stu-dies). Two independent reviewers (HK and AAS)extracted details on the nature of the intervention, thenumber of studies in the meta-analysis, the numberand type of end points, the relative risk (95% confi-dence interval) of coronary heart disease or death,and whether the intervention had an effect on the riskmarker.
Selection of guidelines
Tomake contemporaneous comparisons with our evi-dence reviewwe included guidelines only published in2007 as this was the most recent information availableto us. We identified two guidelines, which were devel-oped through independent processes, from the Scot-tish Intercollegiate Guideline Network9 and thefourth Joint European Societies10 11 (coordinated bythe European Society of Cardiology, and representingnine professional organisations).Across each guidelineand risk marker we compared the evidence cited,description of the causal relevance of the marker,recommendations onmeasurement in healthy popula-tion settings, inclusion in risk scores, recommenda-tions for specific interventions, and target levels orgoals for risk marker levels.
RESULTS
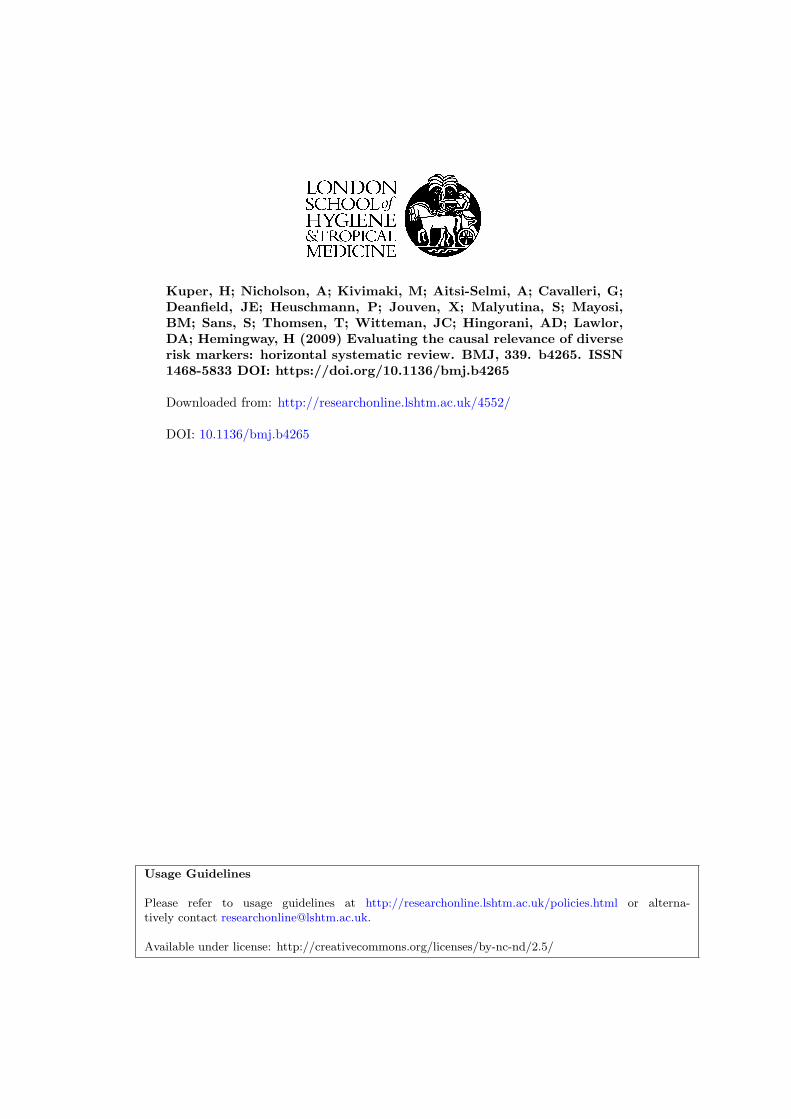
The figure shows the results of the meta-analyses ofobservational studies, genetic variants, and rando-mised controlled trials for depression, exercise, C reac-tive protein, and diabetes in relation to risk of coronary
heart disease. These riskmarkers differed noticeably inthe type and amount of evidence identified.
Observational studies
Table 1 summarises the largest meta-analyses foundfor each of the risk markers. Meta-analyses of observa-tional studies reported adjusted aetiologic relative risksof coronary heart disease for depression of 1.9 (95%confidence interval 1.5 to 2.4; 1262 events in 11 stu-dies), for top compared with bottom fourth of exerciseof 0.7 (0.5 to 1.0; 500 events in three studies), for topcompared with bottom third of C reactive protein of1.6 (1.5 to 1.7; 7068 events in 22 studies), and for dia-betes in women of 3.0 (2.4 to 3.7) and inmen of 2.0 (1.8to 2.3; >4964 events in 29 studies). Meta-analyses ofthe association in patients with coronary heart disease(prognostic studies) reported an adjusted relative riskof further coronary heart disease events or death fordepression of 1.6 (1.3 to 1.9; >525 events in 11 studies)and an adjusted relative risk of cardiac death for dia-betes of 1.5 (1.1 to 2.0; 240 events in four studies). Noprognostic meta-analyses were identified for the effectof exercise or C reactive protein on outcome amongpatients with coronary heart disease. A dose-responseeffect was reported for intensity of physical activity butnot consistently for major depression compared withminor depression, concentration of C reactive protein,or glucose control in people with diabetes. None of themeta-analyses reported effects separately among thoseolder than 75 years (or other age groups of older peo-ple), and only for diabetes was there evidence of con-sistent effects in non-Western populations. Effectestimates for C reactive protein and diabetes were pre-sented separately for men and women, with observa-tional evidence for diabetes showing a strongerassociation with coronary heart disease amongwomen than among men. No sex differences werefound for the association of C reactive protein withcoronary heart disease. The exercise meta-analysiswas restricted to women and the depression meta-ana-lysis did not report effects separately in women andmen.Confounding—Adjustments for a priori confounders
of smoking, bloodpressure, and cholesterol concentra-tion were found in four of 22 aetiologic studies fordepression and coronary heart disease and one ofthree studies for physical activity. Adjustments in theC reactive protein studies (20/22) and diabetes studies(26/37) were generally more consistent and complete,although beyond smoking it was unclear which vari-ables were included inmultivariate analyses. For aetio-logical meta-analyses of the four risk markers, theeffect on coronary heart disease was apparent aftermultivariable adjustments. Reporting of unadjustedor age adjusted and multivariate adjusted results wasinconsistent.Biases—Statistical heterogeneity, present in all the
meta-analyses, was partly attributable to differencesin measurement of exposure for depression and physi-cal activity, and year of publication for C reactive pro-tein. Depression was defined by 12 different methods,
RESEARCH
BMJ | ONLINE FIRST | bmj.com page 3 of 11

but relatively standardised methods were used formeasurement of C reactive protein concentration anddiabetes. For depression, but not for C reactive proteinor diabetes, stronger effectswere observedwith shorterfollow-up. Adjustment for severity of coronary heartdisease in prognostic studies reduced the relative riskfor depression by 45%. Evidence of small study bias(often indicative of publication bias or a strong associa-tion betweenmethodological weakness and a non-nullassociation in the expected direction in smaller studiescompared with larger studies) was present for depres-sion but absent for physical activity, diabetes, and Creactive protein.Other meta-analyses of observational studies—The find-
ings of the meta-analyses of observational studiesincluded in our analysis were consistent with resultsof other eligible meta-analyses on this subject (seeweb extra appendix). For depression, adjusted relativerisks rangedbetween1.5 (1.4 to 1.6) and 1.9 (1.5 to 2.4).Similarly, a consistently strong association was foundbetween diabetes and the incidence andmortality aftercoronary heart disease, with stronger relations identi-fied forwomen than formen. Exercisewas consistentlyprotective for coronary heart disease, ranging from 0.5(0.5 to 0.6) to 0.8 (0.6 to 1.2). Othermeta-analyses con-firmed the increased risk for coronary heart disease forpeople in the highest third of C reactive protein con-centrations.
Genetic evidence
Table 2 summarises the results of our search for meta-analyses of genetic variants, indexing differences in therisk markers of interest. Meta-analyses for two geneticvariants were identified, which have been investigatedin relation to both depression and coronary heart dis-ease: MTHFR12 and APOE.13 14 The MTHFR variantwas positively associatedwithboth depression and cor-onary heart disease, whereas the ε2 APOE genotypewas linked to a reduced risk of depression and of cor-onaryheart disease.12 15w4No replicated genetic variantfor physical activity was identified that could beassessed in relation to coronary heart disease.We iden-tified two syntheses of a genetic variant in the CRPgene in which the expected relation for coronaryheart disease events under a causal model, in the lightof its effect on C reactive protein levels, was notobserved.16w2 Despite the large number of meta-ana-lyses showing genes associated with diabetes, noneexamined the association of these variants with coron-ary heart disease.
Randomised controlled trials
We identified four randomised controlled trials of dif-ferent interventions for the treatment of depressionamong patients with coronary heart disease (table 3).None of these trials showed a beneficial effect on deathor cardiovascular events.w5-w8 No randomised con-trolled trials were identified on the effect of treatingdepression in healthy populations (or on the effect ofprevention of depression) in relation to risk of coron-ary heart disease. No randomised controlled trials
Depression
Rel
ativ
e ri
sk (9
5% C
I)
0.5
1.0
2.0
4.0
Observational studiesGenetic studiesRandomised controlled trials
Aetiologic
Prognosti
c
MTHFR
v depress
ion
MTHFR
v co
ronary heart d
isease
APOE v depre
ssion
APOE v co
ronary heart d
isease
Cognitive behavio
ural therapy
IPT with
or with
out cita
lopram
Sertralin
e
Mitraza
pine or cita
lopram
Exercise
Rel
ativ
e ri
sk (9
5% C
I)
0.5
1.0
2.0
4.0
Aetiologic
Rehabilitatio
n
C reactive protein
Rel
ativ
e ri
sk (9
5% C
I)
0.5
1.0
2.0
4.0
Aetiologic
C reacti
ve pro
tein
T1444C
v C re
active
prote
in
C reacti
ve pro
tein
T1444C
v coro
nary heart
disease
Type 2 diabetes
Rel
ativ
e ri
sk (9
5% C
I)
0.3
0.5
1.0
2.0
4.0
Prognosti
c
Aetiologic
Glucose
lowerin
g (Stettle
r)
Gluco
se co
ntrol
Insulin
Pioglitazo
ne (Lin
coff)
Pioglitazo
ne
Rosiglit
azone
Decreasing risk(evidence of reversibility)
Meta-analyses of
observational studies,
genetic variants, and
randomised controlled trials
for depression, exercise,
C reactive protein, and
diabetes in relation to risk
of coronary heart disease.
IPT=interpersonal
psychotherapy
RESEARCH
page 4 of 11 BMJ | ONLINE FIRST | bmj.com

Table
1|Indicators
ofcausalrelevance
andpotentialbiasin
meta-analysesofobservationalstudiesofdepression,exercise,Creactiveprotein
concentration,anddiabetesin
relationto
coronary
heart
disease
Variables
Depression
Exercise
Creactiveprotein
Type2diabetes
Healthypopulation
Patients
withcoronary
heartdisease
Healthypopulation
Patients
withcoronary
heartdisease
Healthypopulation
Patients
withcoronary
heartdisease
Healthypopulation
Patients
withcoronary
heartdisease
(stents)
Outcomes
Non-fatalm
yocardial
infarctionorfatalcoronary
hea
rtdisea
se
Death
Coronaryheartdisease
Death
orcoronaryheart
disease
Coronaryheartdisease
Death
orcoronaryheart
disease
Fatalcoronaryheart
disease
Death,rep
eat
revascularisation,or
myocardialinfarction
Comparison
Dep
ressionvno
dep
ression
Depressionvno
depression
Topfourthvbottomfourth
Topthirdvbottom
third
Diabetesmellitusvno
diabetesmellitus
Diabetesmellitusvno
diabetesmellitus
Largestmeta-analysis
Nicholson2006w10
Nicholson2006w10
Ogu
ma2004w11
Danesh
2004w12
Huxley2000w13
Lee2006w14
Levelo
fdata
source
Literature
Literature
Literature
Newdata
andliterature
Literature
Pooleddata
Noofoutcomeevents
4016
1867
500
7068
>8261
240
Noofstudiesin
meta-
analysis
22
34
30
22
037
4
Measu
rementofexposu
reScale=1
6*;
antidep
ressant=4;doctor
diagn
osed=2
Scale=3
4†
Leisure
timephysical
activity=2;totalp
hysical
activity=1
22/22studiesusedhigh
sensitivityCreactive
protein
assaymethods
NR
Historyofdiabetes
requiringcurrenttreatm
ent
withinsulin,o
ralagen
ts,o
r
dietarytherapy
Prevalence
ofexposu
re(%
)2-50
2-51
25
33
1-48
21
Age
adjusted
orunadjusted
relative
risk
(95%
CI)
1.8
(1.5
to2.1);su
bsetof
21studieswith3990
events
1.8
(1.5
to2.1);su
bsetof
31studieswith1719
events
NR
NR
Women:3.7
(2.6
to5.2);
men:2.2
(1.8
to2.6);
subsetof22studies,
events
NR
1.4
(1.1
to1.8)
Adjustedrelative
risk
(95%
CI)
1.9
(1.5
to2.4);su
bsetof
11studieswith1262
events
1.6
(1.3
to1.9);su
bsetof
11studieswith>525
events
0.7
(0.5
to1.0)
1.6
(1.5
to1.7)
Women:3.0
(2.4
to3.7);
men:2.0
(1.8
to2.3);
subsetof29studieswith
>4964events
1.5
(1.1
to2.0)
Noofstudiesadjustedfor
smoking/cholesterol
concentrationandblood
pressure
(causal)or
disea
seseverity
(prognostic)
4/22
13/34;relative
risk
reducedfrom
2.2
(1.6
to
3.0)to1.5(1.1to2.1)after
adjustmentforleft
ventricularfunction
1/3
20/22reported
adjustmen
tforsm
oking
and“someother
establishedrisk
markers”
26/37
4/4
Adjustmen
tford
isease
severity
Heterogen
eityI2(%
)(any
markersthatexplain)
52(M
easu
rement
instrumen
t)
54
NR
54(yearofpublication)
Women74;men43
Notapplicable(pooled
data)
Olderpeople(≥75)
NR
NR
NR
NR
NR
NR
Women
NR
NR
Onlywomen
Effectsimila
rin
women
andmen
Effectstrongerin
women
NR
Non-W
estern
populations
Studieslacking
Studieslacking
Studieslacking
Studieslacking
Yes
No
Effectchanges
with
durationoffollo
w-up
Yes;stronger
effectswith
shorterfollowup
NR
No
No
NR
Length
offollo
w-up(yea
rs)
3-37
0.25-15
73-20
4-36
5
Publicationbias
Present(Egger’stest
39
P=0
.08)
Present(Egger’stest
P=0
.01)
Noevidence
(Egger’stest
P=0
.45)
Notform
ally
investigated
Noeviden
ce(Egger ’s
test)
NR
Dose
resp
onse
Eviden
cefordose
resp
onse:stronger
associationforclinical
dep
ression(2.3,1
.8to
3.1)thandepressive
symptomscale(1.7,1.4to
2.0)
Noevidence
fordose
resp
onse:wea
ker
associationforclinical
depression(1.4,0.8
to
2.5)thandep
ressive
symptomscale(1.9,1.6to
2.3)
NS(P=0
.20)
NR
NR
NR
NR=n
otreported.
*Generalwellbeingschedule=2
,CenterforEpidemiologicalStudiesdepressionscale=5
,diagnostic
interview
schedule=2
,geriatric
depressionscale=1
,Zungselfratingdepressionscale=1
,generalhealthquestionnaire/p
resentstate
examination=1
,generalhealthquestionnaire=1
,Hamiltonratingscale=1
,symptom=1
,Minneso
tamultiphasicpersonality
inventory—depression=1
.
†CenterforEpidemiologicalStudiesdepressionscale=6
,Zungselfratingdepressionscale=4
,Millon=3
,Becksdepressioninventory
alone=6
,Becksdepressioninventory
combined=3
,diagnostic
interviewschedule=2
,own=2
,cognitivebehaviour
assessment =1,schedule
foraffectivedisorders
andschizophrenia=1
,Hamiltonratingscale
fordepression=1
,depressionanxiety
stress
scales=1,Diagnostic
andStatisticalManualofMentalDisorders=1
,interview=1
,hosp
italanxiety
and
depressionscale=1
,amitryptiline=1
.
RESEARCH
BMJ | ONLINE FIRST | bmj.com page 5 of 11

were found of interventions that specifically increasedphysical activity (in isolation from, for example,improvements in diet, or compliance with drugs) inhealthy populations, whereas exercise based rehabili-tation reduced the risk of mortality among people withcoronary heart disease (0.7, 0.6 to 1.0).w9 Currentlythere are no interventions that specifically lower Creactive protein levels, and hence no randomised con-trolled trials that could test the causal importance of Creactive protein in coronary heart disease. Rando-mised controlled trials (fourmeta-analyses and 70 indi-vidual trials) of different hypoglycaemic agents inpatients with diabetes without or with manifest coron-ary heart disease provided some, but not consistent,support that lowering glucose concentrations reducedthe rate of coronary heart disease events.w17-w21
Guidelines
Neither the Scottish Intercollegiate Guideline Net-work nor the European guidelines adopted an explicitmethod for displaying and comparing evidence acrossrisk markers (table 4). The Scottish but not Europeanguidelines reported a level of evidence for some state-ments. Both guidelines made clear, albeit differing,statements on the importance of depression in theonset and progression of coronary heart disease.Neither the only randomised trial with statisticalpower to detect differences in event rates(ENRICHD)w5 nor theCochranemeta-analysis of psy-chological interventions17 was cited in the executivesummary of the European guidelines. Post hoc sub-group analyses were cited.18 The Scottish guidelines
cited neither trials normeta-analyses but did cite a pre-vious position statement, which itself cites only anolder narrative systematic review. Neither guidelinesuggested that C reactive protein was an importantrisk marker: for the Scottish guidelines it was neithermentioned nor any rationale given as to why not.Observational studies and Mendelian randomisationstudies were cited for the European guidelines meta-analyses, and the association was stated as “often ser-iously confounded.”
DISCUSSION
The horizontal systematic review is a new method tocompare the evidence on diverse riskmarkers in a uni-fied explicit framework of the largest available synth-eses of the most important forms of evidence. Thisapproach highlighted differences and deficiencies inthe evidence of causal relevance across the fourselected risk markers: psychosocial, behavioural, bio-marker, and metabolic disease. The evidence thatdepression, low physical activity, or C reactive proteinconcentration causes coronary heart disease seems lessstrong than that for diabetes. Randomised trials of spe-cific interventions are lacking for C reactive proteinand null for depression, and although they supportthe role of exercise in the secondary prevention of cor-onary heart disease they are not available to test thecausal hypothesis. Neither the European nor Scottishguidelines gave explicit criteria for assessing evidenceto enable prioritisation of the impact of individual riskmarkers. However the emphasis given to the causal
Table 2 | Genetic variants (single nucleotide polymorphisms, SNPs) associated with risk marker (depression, exercise, C reactive protein, and diabetes) and
coronary heart disease in healthy populations
VariableMTHFR C677T
(TT v CC) rs1801133APOE carriers(ε2 v ε3/3) No SNPs
CRP T1444C rs1130864(TT v any C)
8 SNPs identifiedin recent review*
Outcomes Depression Coronary heartdisease
Depression ε2 vε3 allele
Coronary heartdisease ε2carriers v ε3/3
Exercise C reactiveprotein
Coronary heartdisease
Type 2 diabetes Coronary heartdisease
SNP identifiedfrom genomewide scans
No No No No — No No Yes Not same as fortype 2 diabetes
Largestmeta-analysis
Gilbody2007w15 Lewis 2005w4 Lopez-Leon2008w1
Bennett2007w16
— Lawlor 2008w2 Lawlor 2008w2 Jafar-Mohammadi2008w3
—
No of outcomeevents
1280 26 000 827 21 331 — NA 4610 >6700 —
No of studies inmeta-analysis
10 80 7 17 — 5 5 5 reports (eachwith multiplereplicationstudies)
—
Unadjustedrelative risk(95% CI)
1.36(1.11 to 1.67)
1.14(1.05 to 1.24)
0.51(0.39 to 0.68)
0.80(0.70 to 0.90)
1.21(1.09 to 1.43)(geometricweighted meandifference)
1.01(0.74 to 1.38)†
Range1.12-1.37
—
Instrumentalvariable test*
NA NA NA NA — Null finding(underpowered)
Null finding(underpowered)
NA NA
NA=not available.*Testing whether risk marker is associated with coronary heart disease to extent it is associated with genetic variant—that is, exploiting part of phenotypic variation which is not related to
potential confounding markers. A positive finding supports causality whereas a null finding suggests that observed association between risk marker and coronary heart disease may be
confounded or due to reverse causality.
†Adjusted estimate.
RESEARCH
page 6 of 11 BMJ | ONLINE FIRST | bmj.com

and clinical relevance of depression in the guidelineswas inconsistent with the available evidence.
Closing the translational gap
Discordance exists between the large number of mar-kers that are associated with coronary heart disease3
and the small number of targets for intervention. Thishighlights the need for our approach, which aims toprioritise targets. Our approach is horizontal in twosenses: a comparisonwasmade across diversemarkersand a comparison was made across different forms ofevidence. We selected four risk markers as examples;the approach is scaleable to all risk markers.
Three complementary designs for obtaining causal
evidence
Associations between putative riskmarkers and coron-ary heart disease are easy to show in observational stu-dies but may be confounded, as has been shown bynegative trials of hormone replacement therapy andvitamins on coronary heart disease.19 We marshalledthree approaches, which aimed, with varying limita-tions, to mimic the ideal, unconfounded experiment;prospective observational studies (multivariate adjust-ment for confounders), genetic studies (which utilisegenetic variants that influence themodifiable exposureand that are assigned at random and can therefore beused as an instrument for the unconfounded andunbiased associationof the genetic variantwith the out-come of interest), and randomised trials (where theinvestigator influences exposure). Low density lipo-protein cholesterol provides an example with conver-ging evidence from all these approaches: robustassociations between high concentrations of low den-sity lipoprotein cholesterol and coronary heart diseaseshown in observational cohort studies20; genetic var-iants that relate to lower concentrations of low densitylipoprotein cholesterol (for example, in PCSK9,21 theAPOE,22 and LDL receptor gene)23 also found to beassociated with a reduced risk of coronary heart dis-ease; and trials on low density lipoprotein cholesterollowering confirmed the protection against coronaryheart disease.24 We excluded study designs that maybe associated with lower validity, such as individualobservational studies that have not (yet) been synthe-sised, non-randomised trials, and studies on biologicalmechanisms. Such studies have been the basis forguideline recommendations.25 We included the formsof large scale evidence, which aims to evaluate the cau-sal hypothesis, with a low tolerance for false positivefindings. Our approach could be extended to incorpo-rate small scale experimental studies in humans (as partof a “teleoanalysis” approach)26 and, with duecaveats,27 experimental studies in animals. Such exten-sions to other forms of evidence should acknowledgethat studies in the discovery phase have a higher toler-ance for false positive findings, as the aim is not toabandon a potentially important risk markerprematurely.28
Observational evidence
Risk markers were associated with relative risks from1.5 (C reactive protein) to over 3 (diabetes), but adjust-ment for established risk factors of smoking, bloodpressure, and cholesterol concentration was least com-mon among studies of depression and exercise. Thesepsychosocial (depression) and behavioural (exercise)factors were also more prone to information biases,withmultiple instruments used to determine exposure.There was evidence of reverse causality and publica-tion bias for depression.We found nometa-analyses ina prognostic setting of C reactive protein or exercise.Given that the guidelines make recommendations insecondary prevention and since aetiological markersmay not necessarily be prognostic, this lack of synthe-sised evidence is important. Thus, for example, meta-analyses of body mass index in the prognosis ofpatients with coronary disease suggest no adverseeffect for obesity,29 whereas those for aetiological asso-ciations show an increased risk.30
Genetic evidence
Genetic studies using Mendelian randomisation havebeen more frequently applied to assessing C reactiveprotein31w2 than for our other three risk factors.Despitebeing relatively underpowered, the emerging evidencedoes not suggest an important role for C reactive pro-tein in causing coronary heart disease. A new and largecollaboration should provide a more definitive answerin the near future.32 For depression, exercise, and dia-betes, evidence from Mendelian randomisation fortheir causal role in risk of coronary heart disease waslimited. The robust positive associations of MTHFRwith both depression and coronary heart diseasecould indicate a causal effect of depressionon coronaryheart disease but is more likely to reflect folate intakeandmetabolism as a causal marker for both outcomes.The emergence of whole genome association studiesand complete genome sequencing is improving ourunderstanding of the genomic architecture underlyingcomplex traits. Mendelian randomisation may offer apowerful tool to understand causality, particularly forrisk marker traits that are controlled by a limited num-ber of genetic variants of relatively strong effect.
Randomised controlled trials
Successful treatment of depression in patients withestablished coronary heart disease in randomised con-trolled trials does not show benefits in subsequentdeath or rates of coronary heart disease events. Thisprovides no support for the causal hypothesis thatavoiding depression is important in the secondary pre-vention of coronary heart disease, but it is a matter ofdebatewhether it provides evidence against. For exam-ple, it might be argued that it is the intervention ratherthan the hypothesis that is wrong. Trials were lackingfor the effect of C reactive protein concentration orphysical activity among healthy populations, whereasthere was evidence that glucose control may providesome reduction in coronary heart disease events. Inter-pretation was difficult in the situation of trials with
RESEARCH
BMJ | ONLINE FIRST | bmj.com page 7 of 11

pleiotropic effects; for instance, the evidence that exer-cise in combinationwith other aspects of rehabilitationreduced the risk of death amongpatientswith coronaryheart disease.w9 A new specific C reactive protein inhi-bitor drug is being used to determine the functions of Creactive protein in the experimental setting and will betested in the settingof acute coronary events.However,the lack of oral bioavailability and short half life cur-rently precludes its use in long termprevention trials inhumans.33 Randomised controlled trials of lipid lower-ing statins are a non-specific test of the role ofC reactive protein and coronary heart disease, becauseof the major effect on low density lipoproteinconcentrations.34 It has been shown that false findingsfrom observational studies continue to be influential,despite being contradicted by randomised trialevidence.35 Null randomised trials have led to revi-sions in the causal and mechanistic hypotheses—forexample, the finding that positive inotropic agents donot prolong life in heart failure, refocused attentionaway from a mainly haemodynamic model of heartfailure.36
Clinical implications and consistency of the guidelines
By using horizontal systematic reviews, clinicians,guideline developers, funders of research, publichealth policy makers, and journal editors and theirpeer reviewers might be aided in making more consis-tent and less biased decisions. The graphical summaryof evidence may serve a practical purpose in guidelinegroups, facilitating more explicit debate of the impor-tance of riskmarkers across the multiple fields of inter-est of contributors. The two most recent guidelines onprimary prevention of cardiovascular disease refer to awide “penumbra” of risk markers beyond smoking,blood pressure, and cholesterol concentration; over50 markers in the most recent European guidelines.1
The guidelines cite more than 1100 references (jointsocieties) and 315 references (Scottish IntercollegiateGuideline Network) but do not provide a systematiccomparison of the quality or strength of evidenceacross the risk markers that were included. There wasinconsistency in the conclusions reached by the twoguidelines across the four risk markers that we evalu-ated. For instance, C reactive protein was not consid-ered by the Scottish Intercollegiate GuidelineNetwork. Depression was accorded higher promi-nence in the European guidelines than in the Scottishguidelines and within the European guidelines wasaccorded higher prominence than C reactive protein,which is not consistent with the evidence in the hori-zontal systematic review. Depression is worth treatingin its own right, irrespective of any causal relation withcoronary heart disease; but the same is true for otherconditions, such as chronic obstructive airways dis-ease, which are not mentioned in the guidelines.
Limitations of this horizontal systematic review
There are important limitations in this initial illustra-tion of a horizontal systematic review. Firstly, themethod depends on the availability and quality ofTa
ble
3|Randomisedtrials
ofinterven
tionsthatalterdepression,exercise,Creactiveprotein,andglycaemic
controlandtheireffectsoncoronary
heartdiseaseevents
Depression
Exercise
Creactive
protein
Type2diabetes
None
Sertraline
CBT,group
therapy
Mitrazapine
orcitalopram
IPTor
citalopram
None
Exercise
only
None
None
Glucose
control
Pioglitazone
Rosiglitazone
Glucose
control
(various)
Pioglitazone
Population
Healthy
Coronaryhea
rt
disease
plus
dep
ression
Coronaryhea
rt
disea
seplus
depression
Coronaryhea
rt
disea
seplus
dep
ression
Coronaryheart
disease
plus
dep
ression
Healthy
Coronary
hea
rt
disea
se
Healthy
Coron-
ary
heart
disease
Type2diabetes
Type2
diabetes
Type2
diabetes
Type2
diabetes
Type2diabetes
pluscoronary
hea
rtdisease
Outcomes
—Dea
thDeath
Coronaryhea
rt
disea
se
Cardiovascular
disease
event
Coron-
aryhea
rt
disea
se
Dea
thCoron-
aryheart
disease
Dea
thNon-fatal
myocardial
infarctionordeath
from
coronary
hea
rtdisease
Myocardial
infarction
Myocardial
infarction
Cardiacevent
Dea
th
RCTorMA
—RCT
RCT
RCT
RCT
0MA
00
MA
MA
MA
MA
RCT
Noofstudies
inmeta-analysis
00
00
00
12
00
219
42
60
Reference
—Sadheartw6
ENRICHDw5
MIND-ITw
8CREATE
w7
—Jolliffe
2005w9
——
Huang2001w17
Lincoff
2007w18
Nissen
2007w19
Stettler
2006w20
Erdmann
2007w21
Noofoutcomeevents
—7
340
42
12
—215
——
NR
290
158
1,197
176
Unadjusted
effecton
outcomerelative
risk
(95%
CI)
—0.4
(0.1
to1.4)
1.0
(0.8
to1.2)
1.1
(0.6
to2.0)
1.5
(0.4
to6.9)
—0.7
(0.6
to
1.0)
——
0.9
(0.7
to1.0)
0.8
(0.6
to1.0)
1.4
(1.0
to2.0)
0.9
(0.8
to1.0)
0.9
(0.6
to1.2)
Interventioneffect
onrisk
marker
—Sertralin
e
significantly
superiorto
placeboon
CGI-Iscalebut
notonHAM-D
scale
Significantbut
modest
reductionin
depression
with
intervention
Nodifference
inprevalence
ofdep
ression
ordep
ressive
symptoms
Citalopram
effective,but
noadditional
impactofIPT
—NR
——
Fastingplasm
a
glucose
andHbA1C
lowerin
interventionthan
controlgroups
NR
NR
HbA1Clower
after
interventionin
allsixstudies
Significant
impacton
loweringHbA1C
CBT=cognitivebehaviouraltherapy;
CG-I=clinicalglobalim
pressionim
provementscale;HAM-D
=Hamiltondepression;IPT=
interpersonalpsych
otherapy;
MA=m
eta-analysis;
RCT=randomisedcontrolledtrial;NR=n
otreported.
RESEARCH
page 8 of 11 BMJ | ONLINE FIRST | bmj.com

Table
4|Guidelinerecommendationsforprimarypreventionofcoronary
heartdiseasein
relationto
dep
ression,exercise,Creactive
protein,anddiabetesin
fourthJointEu
ropeanSocieties1
011and
ScottishIntercollegiate
Netw
ork
(SIGN)guidelines9
(both
publish
edin
2007)
Variables
Depression
Exercise
Creactiveprotein
Diabetes
4th
JointEu
ropean
Societies
SIGN
4th
JointEu
ropean
Societies
SIGN
4th
JointEu
ropean
Societies
SIGN
4th
JointEu
ropean
Societies
SIGN
Meta-analysesandtrials
cited
Observational:Rugu
lies
2002,w
22Wulsin
2003,w
23
Barth2004w24;TrialsMA:
Ree
s2004,w
25Linden
1996,w
26Dusseldorp
1999w27
Observational:
nil;
trials:Ree
s2004w25
Observational:
nil;
trials:nil
Observational:
nil;
trials:nil
Observational:
Danesh
2004w12:
trials:nil
Observational:
nil;
trials:nil
Observational:
nil;
trials:UKPDSw28
Observational:nil;
trials:nil
Descriptionofcausal
relevance
“Increasingscientific
eviden
cethatp
sychosocial
factors(including
depression)contribute
indep
enden
tlytotherisk
of
CHD[coronaryhea
rtdisea
se]”(E26)
“strongandconsisten
teviden
ce...indep
enden
trisk
factor”(p43);eviden
celevel2
++
“Alack
ofregu
larphysical
activitymaycontribute
totheearlyonsetand
progressionofCVD
[cardiovasculardisease]”
(E19)
“indep
enden
trisk
factor”(p16);level
ofeviden
ce2++
“seriously
confounded
”(E28)
Notincludedin
guideline
(andnorationale
forexclusion)
Noclea
rstatemen
tbutreferredto
EASD
guidelines
(E25)
“Importantrisk
factor”(p4)
Mea
suremen
trecommendedin
opportunisticassessm
ent
ofhealthypopulations
Yes:“Assess
allpatientsfor
psychosocialriskfactors”
(E27)
Noclearstatemen
t:“Depression…sh
ould
be
taken
into
accountwhen
assessingindividualrisk”
(p44)
Yes:
“Assessmen
t...core
task[s]forphysiciansand
otherhealthworkers”(E20)
No
No
—Noclea
rstatemen
tYes:“Glucose
should
be
mea
suredwhen
assessing
cardiovascularrisk
”and
“riskshouldbeestimatedat
leastonce
everyfive
yearsin
adultsovertheage
of40”
(p9)
Methodofmea
surement
recommended
Yes:
“clin
icalinterviewor
standardised
questionnaires
”;two
screen
ingquestionsare
proposed(E27)
No
Yes:
”Brief
interview
concerning..physical
activityatwork
and
leisure”;nosp
ecific
standardisedinstrumen
trecommen
ded
(S38)
No
No
—No
Yes:randomglucose
inall;if
≥6.1
but≤7
mmol/lthen
fastingglucose
if≥7
.0mmol/lthen
glucose
tolerance
test
Use
inrisk
prediction
scores*
No
No(butsociald
eprivation
isincluded
)No(buta“key
elementof
risk
evaluation”)(E19)
No
No: “Contributionto
risk
estimation
generallymodest”)
(E11)
—No
Yes:p
resence
orabsence
of
diabetes
Interven
tions
Yes:
“Prescribe
multim
odal,beh
avioural
intervention,integrating
individualo
rgroup
counsellingfor
psychosocialriskmarkers
andcopingwithstress
and
illness.Refertoasp
ecialist
incase
ofclinically
sign
ificantemotional
distress”(E27)
No: “Nocleareviden
cethat
treatingdep
ressionis
effective
”(p43);“Smokers
withCHDandcomorbid
clinicald
epressionshould
have
theirdep
ression
treatedboth
foralle
viation
ofdepressivesymptoms
andto
increa
sethe
likelihoodofstopping
smoking”
(p21)
Yes:
“Professionaladvice
abouttheintensity,
durationandfreq
uency
of
exercise”
(S40)
Notdescribed
(nationalguidance
cited)
None
—Yes
No:hypoglycaem
icagents
notdiscussed
Goalsforriskmarkerchange
None
None
Yes:
“30minutesof
moderatelyvigo
rous
exerciseonmostdays
of
thewee
kwillreduce
risk
”(E19)
Yes:
“Alladults
should
accumulate
30minutesof
moderate
intensity
activityonmost
days
oftheweek”
(p17);levelo
feviden
ce4
No
—Yes:inalltoachieve
“Blood
glucose
<6mmol/l”;“M
ore
rigo
rousrisk
factorcontrol
inhighrisk
subjects:
fastingbloodglucose
<6mmol/landHbA1C<6.5%
iffeasible”(E9)
No
UKPDS=U
nitedKingdom
Prosp
ectiveDiabetesStudy;
EASD=E
uropeanSociety
forDiabetes.
E=e
xecu
tive
summary
pagenumber;S=fulltext
pagenumber.Levels
ofevidence
usedin
SIGN:2++=h
ighquality
systematicreviewsofcase-controlorcohortstudies;
highquality
case-controlstudiesorcohortswithlow
risk
ofconfoundingor
biasandhighprobabilitythatrelationis
causal;4=e
xpertopinion.
*Assessingcardiovascularrisk
usingSIGNguidelinesto
assignpreventive
treatm
ent(ASSIGNscore)in
SIGNandHeartScore
infourthJointEuropeanSocieties.
RESEARCH
BMJ | ONLINE FIRST | bmj.com page 9 of 11

large scale syntheses of evidence. These aremore com-monly available for blood based markers than forbehavioural or psychosocial markers; horizontal sys-tematic reviews may stimulate research groups toraise or defend the profile of research in their subdisci-plines. A range of measures of effect were included inthe reviews, and where the confidence intervals for theeffect estimates werewide this precluded reaching firmconclusions. Increasing use of horizontal systematicreviews may provide an impetus to improving thenumber and quality of meta-analyses, particularlythose using individual participant data. Secondly, thehorizontal systematic review is narrative, withoutnovel methods for data analysis, offering no explicitranking of causal relevance nor attempting to posit adecision threshold above which a marker might beconsidered causal.
Research implications and need for unbiased field
synopses
Further research is required to develop the method ofhorizontal systematic review. Firstly, methods couldbe developed to derive relative weights of evidencebuilding on the judgments of groups of experts,37 Baye-sian methods could be used for the synthesis of evi-dence, or models could be developed to combinefeatures from different studies to derive quantitativeestimates.38 Secondly, extension is required to thewhole range of risk markers that are included in guide-lines, thus providing a systematic synopsis of the speci-alty. Thirdly, extension to other chronic diseasesshould be explored—for example, in the specialty ofcancer, horizontal systematic reviews could build onthe assessment of causality used by the InternationalAgency for Research on Cancer. Fourthly, horizontalsystematic reviews should be regularly updated as evi-dence changes to minimise the lag time between thegeneration of evidence and the development of guide-lines and could take advantage of continually updateddatabases of genetic studies in this process. The
conclusions of our review are not altered if the publica-tion year of evidence is truncated two years before thepublication of guidelines—that is, 2005. Fifthly, thereare important considerations beyond causal relevancewhen developing guidelines, such as economic consid-erations and the additional deleterious effects of therisk markers (for example, the impact of depressionon quality of life), and the framework could beextended to encompass these considerations. Sixthly,it should be noted that non-causal markers can be usedin risk prediction (for example, socioeconomic posi-tion) and this requires distinct consideration in theobservational evidence.
Conclusion
Horizontal systematic review in which the causal rele-vanceof diverse riskmarkers is compared in an explicitframework helps clarify the relative standing of eachrisk marker. Field synopses, expanded to include thewhole range of risk markers considered of potentialclinical or public health relevance, should be devel-oped to prioritise research efforts and to focus recom-mendations on those markers most likely to be causal.
This work was developed during meetings of the Nucleus ofEpidemiology and Public Health, European Association of CardiovascularPrevention and Rehabilitation, European Society of Cardiology in Paris2007 and Sofia Antipolis 2008 (HH chair, members GC, JED, PH, XJ, SM,BMM, SS, TT, JCMW, ADH, and DAL).Contributors:The writing group included HK, AN, MK, and HH. HK, AN, andMK contributed equally to the study. HK, HH, AN, and AAS carried out thesearches and extracted the data. All authors took part in the discussiongroup where the new methodology was developed, commented on earlydrafts of the manuscript through to revisions, approved the final draft,had full access to all the data, and can take responsibility for the integrityof the data and the accuracy of the data analysis.Funding:MK is supported by the Academy of Finland. HK is supported bya grant from the Wellcome Trust. DAL is supported by a UK Department ofHealth Career Scientist Award and works in a centre that receives supportfrom the UK Medical Research Council. ADH is supported by a BritishHeart Foundation senior research fellowship (FS 05/125).Competing interests: ADH is a member of the editorial board of Drugand Therapeutics Bulletin and has acted as an adviser toGlaxoSmithKline and London Genetics. He has received honorariums forspeaking at educational meetings sponsored by the pharmaceuticalindustry and has donated all or most of these to charity.Ethical approval: Not required.Data sharing: No additional data are available.
1 De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R,Dallongeville J, et al. European guidelines on cardiovascular diseaseprevention in clinical practice. Third Joint Task Force of European andother Societies on Cardiovascular Disease Prevention in ClinicalPractice. Eur Heart J 2003;24:1601-10.
2 Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fortmann SP,et al. AHA guidelines for primary prevention of cardiovasculardisease and stroke: 2002 update: consensus panel guide tocomprehensive risk reduction for adult patients without coronary orother atherosclerotic vascular diseases. American Heart AssociationScience Advisory and Coordinating Committee. Circulation2002;106:388-91.
3 Hopkins PN, Williams RR. A survey of 246 suggested coronary riskfactors. Atherosclerosis 1981;40:1-52.
4 Shrier I, Boivin JF, Steele RJ, Platt RW, Furlan A, Kakuma R, et al.Shouldmeta-analyses of interventions includeobservational studiesin addition to randomized controlled trials? A critical examination ofunderlying principles. Am J Epidemiol 2007;166:1203-9.
5 Davey Smith G, Ebrahim S. ‘Mendelian randomization’: can geneticepidemiology contribute to understanding environmentaldeterminants of disease? Int J Epidemiol 2003;32:1-22.
6 Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G.Mendelian randomization: using genes as instruments for makingcausal inferences in epidemiology. Stat Med 2008;27:1133-63.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Diverse psychosocial, behavioural, and biological markers are claimed to be independentlyassociated with coronary heart disease and are included in guidelines
Traditional vertical systematic reviews focus on one risk marker and one research design at atime
Horizontal comparisons across different types of risk markers, incorporating differentresearch designs each with differing limitations, are lacking
WHAT THIS STUDY ADDS
Observational evidence from horizontal systematic review was strongest for diabetes and Creactive protein concentration as risk markers for coronary heart disease
Evidence from Mendelian randomisation was present for C reactive protein only, which didnot support a causal association with coronary heart disease
Randomised trial evidence was lacking for C reactive protein and did not show a protectiveeffect in coronary heart disease from treating depression; for no risk marker did it providestrong support for the causal hypothesis
RESEARCH
page 10 of 11 BMJ | ONLINE FIRST | bmj.com

7 Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D,et al. Meta-analysis of observational studies in epidemiology: aproposal for reporting. Meta-analysis Of Observational Studies inEpidemiology (MOOSE) group. JAMA 2000;283:2008-12.
8 Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.Improving the quality of reports of meta-analyses of randomisedcontrolled trials: the QUOROM statement. Quality of Reporting ofMeta-analyses. Lancet 1999;354:1896-900.
9 Scottish Intercollegiate Network. Risk estimation and the preventionof cardiovascular disease. In: SIGN, ed. Edinburgh: SIGN, 2007.
10 Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R,et al. European guidelines on cardiovascular disease prevention inclinical practice: executive summary. Fourth Joint Task Force of theEuropean Society of Cardiology and Other Societies onCardiovascular Disease Prevention in Clinical Practice (constitutedby representatives of nine societies and by invited experts). Eur JCardiovasc Prev Rehabil 2007;14(suppl 2):E1-40.
11 Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R,et al. European guidelines on cardiovascular disease prevention inclinical practice: full text. Fourth Joint Task Force of the EuropeanSociety of Cardiology and other Societies on Cardiovascular DiseasePrevention in Clinical Practice (constituted by representatives of ninesocieties and by invited experts). Eur J Cardiovasc Prev Rehabil2007;14(suppl 2):S1-113.
12 Klerk M, Verhoef P, Clarke R, Blom HJ, Kok FJ, Schouten EG. MTHFR677C–>T polymorphism and risk of coronary heart disease: a meta-analysis. JAMA 2002;288:2023-31.
13 Lopez Leon S, Croes EA, Sayed-Tabatabaei FA, Claes S, VanBroeckhoven C, van Duijn CM. The dopamine D4 receptor gene 48-base-pair-repeat polymorphism and mood disorders: a meta-analysis. Biol Psychiatry 2005;57:999-1003.
14 Lopez-Leon S, Janssens AC, Gonzalez-Zuloeta Ladd AM, Del-Favero J,Claes SJ, Oostra BA, et al. Meta-analyses of genetic studies onmajordepressive disorder.Mol Psychiatry 2008;13:772-85.
15 Song Y, Stampfer MJ, Liu S. Meta-analysis: apolipoprotein Egenotypes and risk for coronary heart disease. Ann Intern Med2004;141:137-47.
16 Casas JP, Shah T, Cooper J, Hawe E, McMahon AD, Gaffney D, et al.Insight into the nature of the CRP-coronary event association usingMendelian randomization. Int J Epidemiol 2006;35:922-31.
17 Rees K, Bennett P, West R, Davey SG, Ebrahim S. Psychologicalinterventions for coronaryheart disease.CochraneDatabaseSyst Rev2004;(2):CD002902.
18 Schneiderman N, Saab PG, Catellier D, Powell LH, DeBusk R,Williams RB. Psychosocial treatment within sex by ethnicitysubgroups in the enhancing recovery in coronary heart diseaseclinical trial. PsychosomMed 2004;66:475-83.
19 Lawlor DA, Davey Smith G, Kundu D, Bruckdorfer KR, Ebrahim S.Those confounded vitamins: what can we learn from the differencesbetween observational versus randomised trial evidence? Lancet2004;363:1724-7.
20 Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J,et al. Blood cholesterol and vascularmortality by age, sex, andbloodpressure: a meta-analysis of individual data from 61 prospectivestudies with 55,000 vascular deaths. Lancet 2007;370:1829-39.
21 Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequencevariations in PCSK9, low LDL, and protection against coronary heartdisease. N Engl J Med 2006;354:1264-72.
22 Bennet AM, Di Angelantonio E, Ye Z, Wensley F, Dahlin A, Ahlbom A,et al. Association of apolipoprotein E genotypes with lipid levels andcoronary risk. JAMA 2007;298:1300-11.
23 Linsel-Nitschke P, Gotz A, Erdmann J, Braenne I, Braund P,HengstenbergC, et al. Lifelong reductionof LDL-cholesterol related toa common variant in the LDL-receptor gene decreases the risk ofcoronary artery disease—a Mendelian randomisation study. PLoSONE 2008;3:e2986.
24 Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C,et al. Efficacy and safety of cholesterol-lowering treatment:prospective meta-analysis of data from 90,056 participants in 14randomised trials of statins. Lancet 2005;366:1267-78.
25 Pearson TA,MensahGA, Alexander RW, Anderson JL, CannonRO3rd,Criqui M, et al. Markers of inflammation and cardiovascular disease:application to clinical and public health practice: a statement forhealthcare professionals from the Centers for Disease Control andPrevention and the American Heart Association. Circulation2003;107:499-511.
26 Wald NJ, Morris JK. Teleoanalysis: combining data from differenttypes of study. BMJ 2003;327:616-8.
27 Perel P, Roberts I, Sena E, Wheble P, Briscoe C, Sandercock P, et al.Comparison of treatment effects between animal experiments andclinical trials: systematic review. BMJ 2007;334:197-200.
28 Contopoulos-Ioannidis DG, Alexiou GA, Gouvias TC, Ioannidis JP.Medicine. Life cycle of translational research for medicalinterventions. Science 2008;321:1298-9.
29 Romero-Corral A, Montori VM, Somers VK, Korinek J, Thomas RJ,Allison TG, et al. Association of bodyweight with total mortality andwith cardiovascular events in coronary artery disease: a systematicreview of cohort studies. Lancet 2006;368:666-78.
30 Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC,Woodward M, Knekt P, et al. Association of overweight withincreased risk of coronary heart disease partly independent of bloodpressure and cholesterol levels: ameta-analysis of 21 cohort studiesincluding more than 300 000 persons. Arch Intern Med2007;167:1720-8.
31 KivimakiM, LawlorDA,DaveySmithG, KumariM,DonaldA,BrittonA,et al. Does high C-reactive protein concentration increaseatherosclerosis? The Whitehall II Study. PLoS ONE 2008;3:e3013.
32 Danesh J, Erqou S, Walker M, Thompson SG, Tipping R, Ford C, et al.The Emerging Risk Factors Collaboration: analysis of individual dataon lipid, inflammatory and other markers in over 1.1 millionparticipants in 104 prospective studies of cardiovascular diseases.Eur J Epidemiol 2007;22:839-69.
33 Pepys MB, Hirschfield GM, Tennent GA, Gallimore JR, Kahan MC,Bellotti V, et al. Targeting C-reactive protein for the treatment ofcardiovascular disease. Nature 2006;440:1217-21.
34 Casas JP, Shah T, Hingorani AD, Danesh J, Pepys MB. C-reactiveprotein and coronary heart disease: a critical review. J Intern Med2008;264:295-314.
35 Tatsioni A, Bonitsis NG, Ioannidis JP. Persistence of contradictedclaims in the literature. JAMA 2007;298:2517-26.
36 Katz AM. Pathophysiology of heart failure: identifying targets forpharmacotherapy.Med Clin North Am 2003;87:303-16.
37 Hemingway H, Chen R, Junghans C, Timmis A, Eldridge S, Black N,et al. Appropriateness criteria for coronary angiography in angina:reliability and validity. Ann Intern Med 2008;149:221-31.
38 Mouchart M, Russo F, Wunsch G. Structural modelling, exogeneity,and causality. In: Engelhardt H, Kohler HP, Prskwetz A, eds. Causalanalysis in population studies: concepts, methods, applications.Dordrecht: Springer, 2008.
39 Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test.BMJ1997;315:629-34.
Accepted: 12 July 2009
RESEARCH
BMJ | ONLINE FIRST | bmj.com page 11 of 11