next – foot and ankle manual therapy and treatment
TRANSCRIPT

Next – Foot and AnkleManual Therapy and treatment
Haley Main DPT, COMT GTS
Searcy, Arkansas
www.iaom-us.com Diagnose Precisely * Treat Effectively
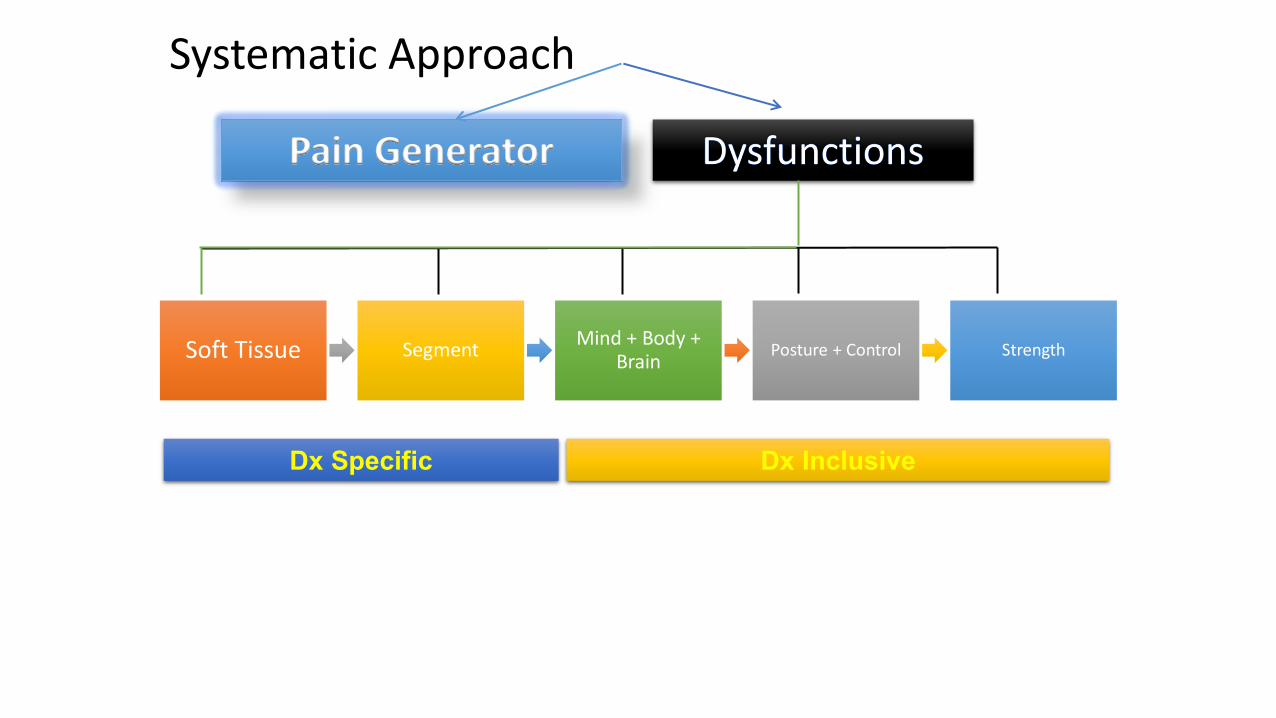
Systematic Approach
Pain Generator
Dx Specific Dx Inclusive
Soft Tissue SegmentMind + Body +
BrainPosture + Control Strength

What is Always
your first treatment?

Diagnosis Explanation Story
Dx Explanation
Prognosis
Goals
Plan of care
Set Up Appointments

Diagnosis Explanation Formula
• Share the good news:
• Diagnosis• Medical terminology
• Layman’s terms
• Explanation of the diagnosis
• “This heals”
• Co-morbid factors
• Dysfunctions
• Prognosis
• Goals

Diagnosis Explanation FORM
• Thank you for sharing your story and performing all the tests and measures and letting me know how each one affected your symptoms.
• Your exam fit a pattern and makes sense.
• After reading your paperwork, talking with you and hearing your story, along with the results from your exam, your signs and symptoms are consistent with an {arthritis of the foot}.

Diagnosis Explanation Form
• Start with good news
• However, don’t worry.
• Almost everyone gets joint pain at some point of their life. It heals.
• I have successfully treated many of cases just like yours. You particularly have a good prognosis due to the fact that when I performed joint traction to your ankle, we were able to decrease your symptoms.
• This is a good sign we can help your feel and move better.

Diagnosis Explanation Form
• Besides the hip, you also have some dysfunctions of structures surrounding the disc that can limit your ability to heal.
• Other areas that are affecting your ability to heal are [tight muscles, some stiff joints and improper muscle control, etc.]
• I will work on these during your treatments and alsogive you self-treatment options to perform at home.

Diagnosis Explanation Form
Brain’s Role in Pain
• Your brain also plays an important role in your healing. The more you worry or fear your condition, the brain senses danger. Then it sends stronger pain signals.
• The more you trust that you are going to get better think about other, more positive, aspects in life, it senses less danger. Therefore, it sends less pain signals.

Diagnosis Explanation Form
Exercise + Control
• Re-gaining control of your body/back movements will also help create a healing environment.
• You will be given exercise to activate your inner core muscles and we will perform exercises with a head-mounted laser.
• Once you have good control and your pain will decrease with activities,
• We will work on more outer core strengthening to prevent re-occurrence of these symptoms.

Diagnosis Explanation Form
Wellness can improve healing
• Some important things you can do to help with overall healing are:
• Sleep at least 7 hours per night (present 7 simple things you and do it improve healing handout)
• Eat healthy nutrient-rich foods (and limit processed foods)
• Perform aerobic exercise every day.
• Add any co-morbid factors that influence healing

Diagnosis Explanation Form
Match Tx to Helping Functional Limitations
• There are many advanced treatment techniques I will perform in the clinic in order to provide a proper healing environment for the hip joint so that you can get back to doing {match with functional limitations}.
• I will also have several exercises and self-management techniques I will teach your how to perform at home.
• If you have someone that can help treat you at home, bring them into treatment and I’ll help them help you.
• Do you have any questions for me so far?

• You have had pain for ____ weeks/months/years, right?
• How would you feel if, together, we can get your pain 50% better in the next ___ weeks?
• Let’s create some goals for you for the next 4 weeks.
• I would like to see you ___ x per week. Can you make that commitment?
GOALS

Conclusion
Be Present and Listen
Perform and through skilled History and Exam…while building your ’story’
Give the Patient Hope and a Path to Healing

Conclusion
Be Present and Listen
Perform and through skilled History and Exam…while building your ’story’
Give the Patient Hope and a Path to Healing

Harnessing the Power of Placebo
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.
TEDMED. “Harnessing the Power of Placebos.” Alia Crum. Online video clip. YouTube.
Harnessing the Power of Placebos
• Psychologist performed study testing social context and placebo• Patients had histamine skin prick test performed which created skin reaction
• All patients received placebo cream but doctor had different messages
• ½ participants were told cream would make rash better
• Other ½ were told cream would make rash worse…
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.

TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.

Harnessing the Power of Placebos
• Social context matters • What the doctor did and what the patient thought of doctor had tremendous
influence on results.
• Test #2• Altered the warmth and competence of doctors
• Fundamental qualities we judge people on
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.
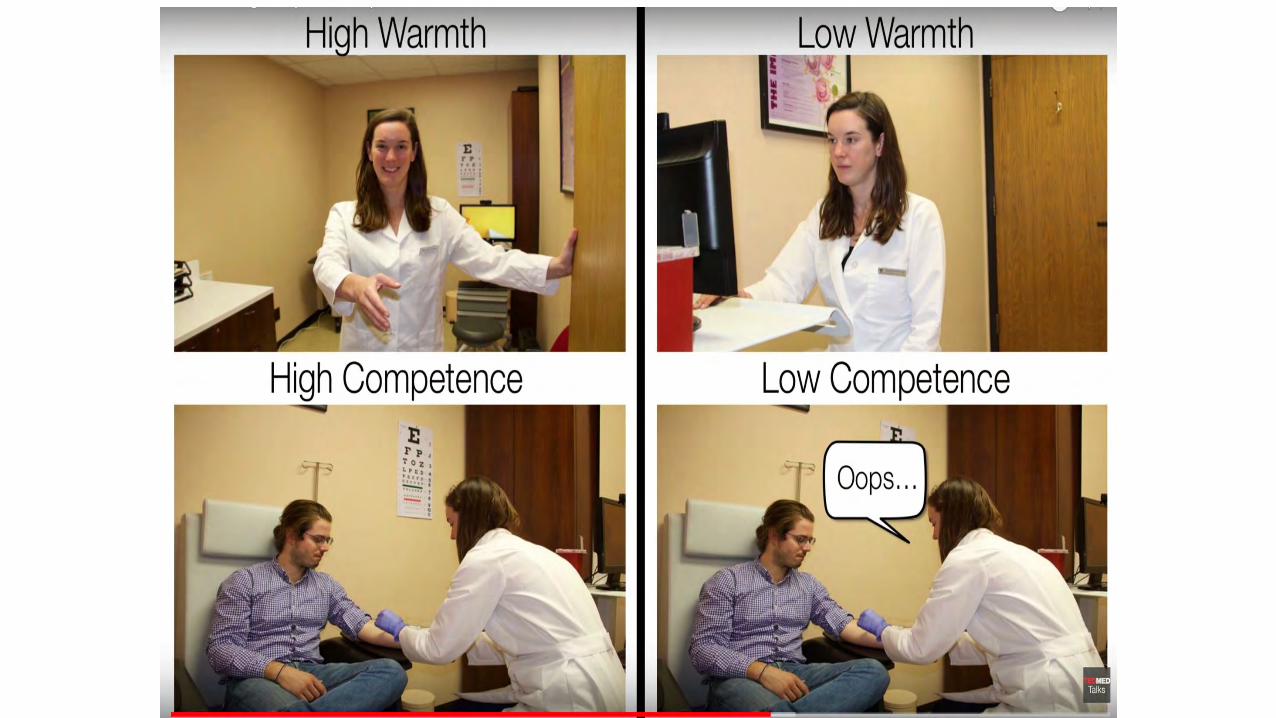
Harnessing the Power of Placebos
• Results of Test #2• Warm and competent doctor’s comments had stronger effect and increased
healing effects as positive expectations she set were more powerful
• Cold and incompetent doctor’s comments had no effect to the cream.
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.

High warmthHigh competence
Low warmthLow competence
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.

Harnessing the Power of Placebos
• Why does this matter?• Mindsets about treatments influence results
• Social context matters…• What we say
• How we dress and present ourselves
• Precision of examination
• Clinic environment
TEDMED. “Harnessing the Power of Placebos.” Online video clip. YouTube. Youtube, 19 September 2017. Web. 30 March 2018.

21
3
5
Osseous - Medial
1. Medial malleolus
2. Sustentaculum tali
3. Navicular tubercle
4. TaloNavicular Joint line
5. Medial tubercle of the posterior process of the talus

4
8
6
7
Osseous - Medial
4. TNJ line6. 1st MTP joint line7. Cuneiform/metatarsal joint line8. Navicular/cuboid joint line

Medial Malleolus
Sustentaculum Tali
NavicularTuberosity
Osseous - Medial

Talar Head
Talonavicular Joint Space
Medial tubercle of the posterior process of the talus
1st MTP Joint
Osseous - Medial

Medial Cuneiform-MTT 1 Joint
Navicular-Medial Cuneiform Joint
Osseous - Medial

1
3
2
4
5
6
Osseous - Lateral
1. Lateral malleollus2. Peroneal tubercle3. Talar neck/head4. Calcaneal trumpet and
CalcaneoCuboid joint line5. Cuboid/4th&5th MT joint line6. Cuboid/navicular joint line

Lateral Malleolus
PeronealTrochlea
Sinus Tarsi
Osseous - Lateral

Osseous - Lateral
Trumpet of the Calcaneus
Cuboid-MTT IV & V Joint line
CalcaneoCuboidJoint line

Osseous- Dorsal
Talar Neck and Head
Cuboid and Navicular/Lateral Cuneiform Joint line
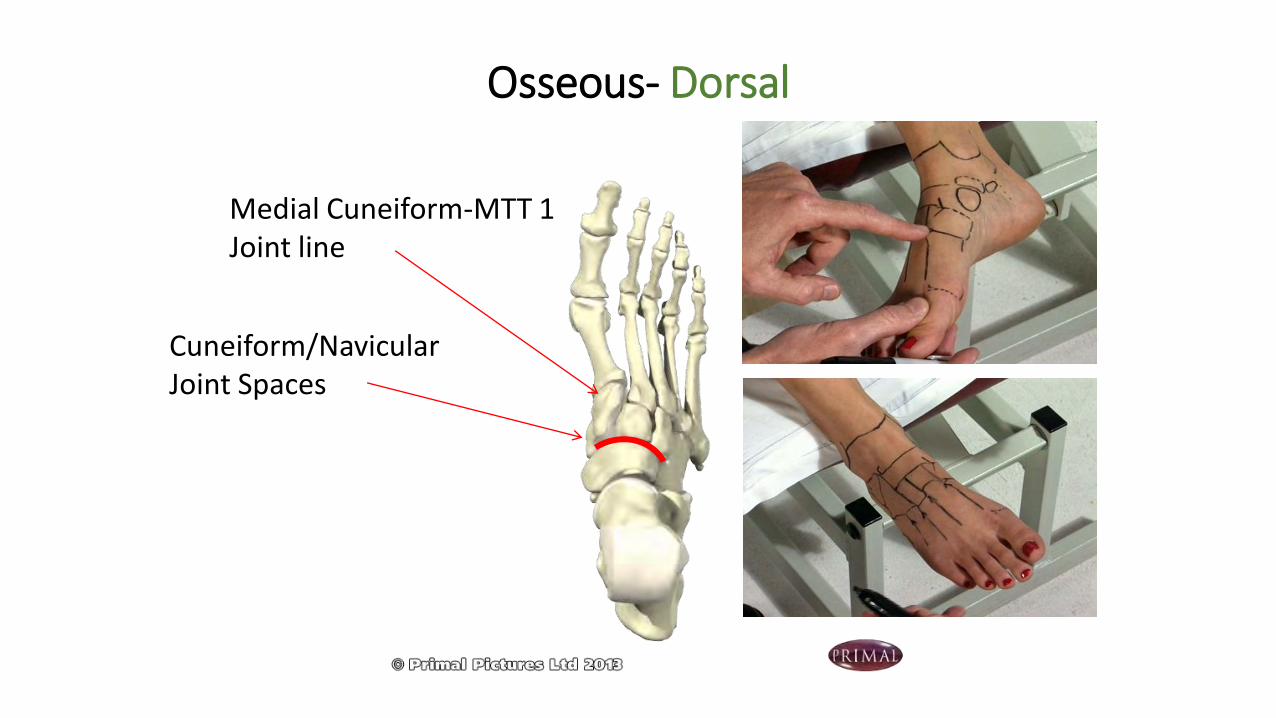
Cuneiform/Navicular Joint Spaces
Osseous- Dorsal
Medial Cuneiform-MTT 1 Joint line

Talocrural Joint
• Passive Dorsiflexion
a. Full knee extension
b. Slight knee flexion
c. Active dorsiflexion
• Passive Plantar Flexion
• Perform to end range, back off slightly & then perform quick movement into end range to assess end-feel
Clinical ExaminationPassive Tests in Supine

Subtalar Joint
• Passive test in Supine for provocation
Inversion
Eversion
The testing hand moves the calcaneus into inversion, and then into eversion along a line connecting sustentaculumtali to sinus tarsi. Overpressure is exerted to provoke symptoms. The other hand gently guides the forefoot.
Clinical ExaminationPassive Tests in Supine
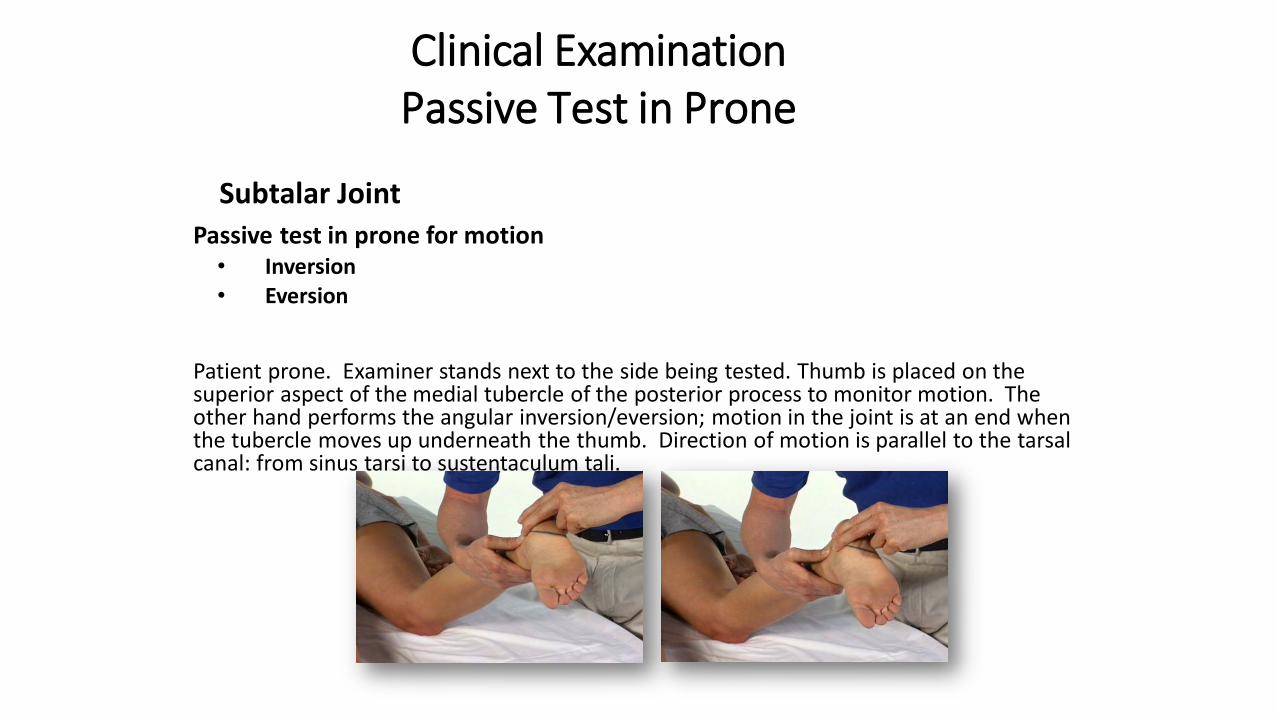
Subtalar Joint
Passive test in prone for motion• Inversion• Eversion
Patient prone. Examiner stands next to the side being tested. Thumb is placed on the superior aspect of the medial tubercle of the posterior process to monitor motion. The other hand performs the angular inversion/eversion; motion in the joint is at an end when the tubercle moves up underneath the thumb. Direction of motion is parallel to the tarsal canal: from sinus tarsi to sustentaculum tali.
Clinical ExaminationPassive Test in Prone

Midtarsal Joints• Stabilize calcaneus in eversion
• Passive PF/DF: grasp region of MTP 2/3, movement is perpendicular to dorsum of foot
• Passive Abd/Add: grasp foot at level of metatarsals, movement is parallel to dorsum of foot
• Passive Pron/Sup: grasp navicular & cuboid, pronate & supinate around an axis going through MT2
Clinical ExaminationPassive Tests in Supine

Should we look at the arch? • Normalized plantar arch height: Women > Men
High arch vs. low arch
• Low arch associated with:
• ’d medial loading
• Plantar fasciitis
• Tendopathies (especially Tib posterior)
• Patellar tendinitis
• Medial knee pain
Clinical Examination: Extra Test
Williams DS, et al. Arch structure and injury patterns in runners. Clin Biomech. 2001; 16:341-7.Hogan MT, Staheli LT. Arch height and lower limb pain: An adult civilian study. Foot Ankle Int. 2002; 23:43-7.Michelson JD, et al. The injury risk associated with pes planus in athletes. Foot Ankle Int 2002; 23:629-33.
Wikimedia Commons

Is there a limit?
Capsular Pattern Indicates:
Arthritis (Synovitis)
Traumatic
Systemic
Arthrosis (Degenerative)
Activated
Non-Activated
Interpretation

IAOM-US

Exam Results
IAOM-US
IAOM-US

IAOM-US

• MLPP: 10 deg PF• MCPP: Maximum inversion• Capsular pattern:
• Supination (flexion-adduction-inversion) more limited than pronation
• Noncapsular pattern• Needs joint specific testing
• Chronic cases with immobilization or trauma in the history
• Chronic Achillodynia
Midtarsal Joints

Midtarsal Joints
1 Joint Specific Testing1.1. Talonavicular Joint
Navicular bone glide planto-medio-proximal to dorso-latero-distal
1.2. Calcaneocuboid Joint
Cuboid glide planto-medial to dorso-lateral
1.3 Cuboid-Navicular / Lateral Cuneiform Joint
Cuboid glide planto-medial to dorso-lateral
2 Joint Specific Treatment Techniques2.1. Improvement of Supination
2.1.1. Talonavicular joint Navicular bone glide planto-medio-proximal
2.1.2. Calcaneocuboid jointCuboid glide planto-medial
2.1.3. Cuboid-navicular / Lateral cuneiform jointCuboid glide planto-medial
2.2. Improvement of Pronation
2.2.1. Talonavicular joint Navicular bone glide dorso-latero-distal
2.2.2. Calcaneocuboid jointCuboid glide dorso-lateral
2.2.3. Cuboid-navicular / Lateral cuneiform jointCuboid glide dorso-lateral
2.3. Proprioceptive Training
2.3.1. For supination
2.3.2. For pronation

Navicular bone glide planto-medio-proximal to dorso-latero-distal.
CalcaneocuboidJoint: Cuboid glide
planto-medial to dorsolateral
Cuboid-Navicular/Lateral Cuneiform Joint:
Cuboid glide planto-medial to dorsolateral
Joint Specific TestingTalonavicular Joint

Talonavicular Joint.Navicular bone glideplanto-medio-proximal.
With spin in Eversion to emphasize the mobilization effect.
Joint Specific TreatmentImprovement of Supination (3-D)
With spin in Inversion to emphasize the osteokinematic/functional effect.

Calcaneocuboid Joint.: Cuboid glide planto-medial.
Plantar glide of the cuboid with spin in Inversion to emphasize the mobilization effect as well as the osteokinematic/functional effect.
Joint Specific TreatmentImprovement of Supination (3-D)

Cuboid-navicular/Lateral cuneiform joint: Cuboid glide planto-medial.
Joint Specific TreatmentImprovement of Supination (3-D)
CNJ (Direction is perpendicular to dorsum of foot)-Use cross arm technique (outside arm is the mob hand)-Brace the stab fingers against table but keep calcaneus off the mat-Stab navicular and lat cuneiform by orienting at dorsum of foot with thumb at 2nd -3rd
MT and fingers plantar corresponding to this location. -Mob with hypothenar at cuboid

Talonavicular Joint.Navicular bone glidedorso-latero-distal.
With spin in inversionto emphasize the mobilization effect.
With spin in eversion to emphasize the osteokinematic/functional effect.
Joint Specific TreatmentImprovement of Pronation

Calcaneocuboid Joint.: Cuboid glide dorsolateral.
Dorsal glide of the Cuboid with spin in eversionTo emphasize the mobilization effect as well as the osteokinematic/functional effect.
Joint Specific TreatmentImprovement of Pronation

Cuboid-navicular/Lateral cuneiform joint: Cuboid glide dorsolateral.
Stabilize navicular-cuneiform and mobilize cuboid.Position leg in internal rotation.Direction is perpendicular to dorsum of foot-Brace the stab fingers against table -Stab navicular and lat cuneiform by orienting at dorsum of foot with fingers at 2nd -3rd MT and hypothenar eminence plantar corresponding to this location. -Mob with hypothenar at cuboid
Joint Specific TreatmentImprovement of Pronation

Cuboid-navicular/Lateral cuneiform joint:Cuboid manipulation (alternative technique)
Patient is prone.Cuboid manipulation performed starting with the knee flexed to 70 degrees and the ankle near neutral. The knee is then passively extended as the ankle is plantarflexed with slight supination of the subtalar joint. A thrust force is applied using both thumbs on the plantar aspect of the cuboid.
Jennings J, Davies GJ. Treatment of cuboid syndrome secondary to lateral ankle sprains: a case series. J Orthop Sports Phys Ther.
2005;35(7):409-15.
Joint Specific TreatmentImprovement of Pronation

Example: Calcaneocuboid Joint for Supination
Beginning position End position
Joint Specific TreatmentNeuromuscular Reeducation

Traction Medial-Lateral Glide of Proximal Phalanx
Dorsal-Plantar Glideof Proximal Phalanx
Joint Specific TreatmentMTP 1 Joint

Traction: prepositioned in extension,supination, and abduction
Medial Glide of Proximal Phalanx:prepositioned in abduction with spin in supination.
Dorsal Glide of Proximal Phalanx:prepositioned in extension with spin in supination.
Joint Specific TreatmentHallux Valgus

TractionDone to detect hypermobility or in presence of painful gliding (or for warm up to joint testing)
Anterior-Posterior Glide of Talus Left picture: Anterior-posterior glide. (In instances of small hands testing large feet
left shows posterior glide, right shows anterior glide of the talus)
Talocrural Joint: Joint Specific Testing
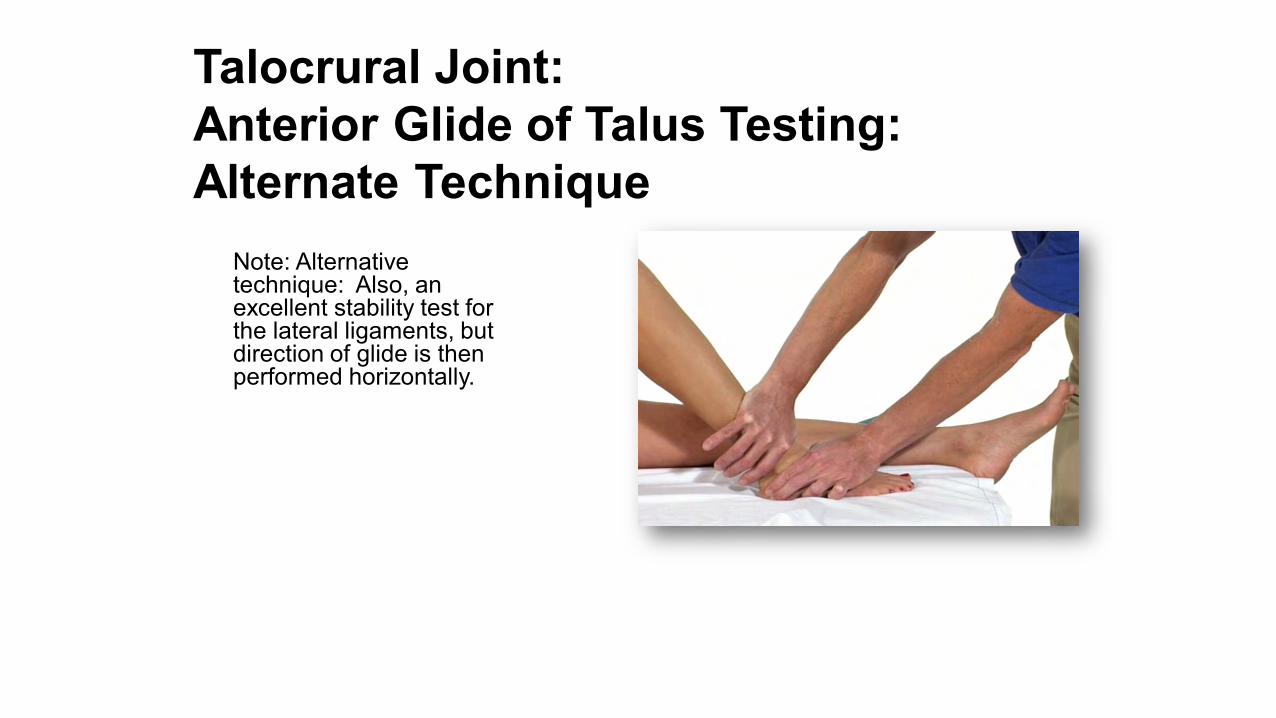
Note: Alternative technique: Also, an excellent stability test for the lateral ligaments, but direction of glide is then performed horizontally.
Talocrural Joint: Anterior Glide of Talus Testing: Alternate Technique

Traction: 1. Manipulation technique (no belt
stabilization needed)2. Mobilization technique (with belt
stabilization of lower leg)Performed in maximal loose-packed position of 10° plantar flexion
Traction: prepositioned in dorsiflexion
Talocrural Joint: Joint Specific TreatmentImprovement Dorsiflexion

Talocrural Joint: Joint Specific TreatmentAlternative Technique for Traction

Posterior Glide of the Talus: maximal loose-packed position
Posterior Glide of the Talus: prepositioned in dorsal extension
Talocrural Joint: Joint Specific Treatment

Proprioceptive training in a joint specific manner is a combination of the arthrokinematic gliding technique with the passive or active osteokinematic movement.
Talocrural Joint: Joint Specific TreatmentNeuromuscular Reeducation in Nonweightbearing

Home exercise to improve dorsiflexion of the talocrural joint. →
Prepositioned Anterior Glide Techniques of Tibia/Fibula when ROM > 90°
Note: For all talocrural joint specific techniques in weightbearing, the calcaneus should be in the neutral position.
Talocrural Joint:

Emphasis on the lateral capsule.
Starting position: glide anterior slightly lateral. End position: after reaching maximalanterior glide, a minimal internal rotationspin is performed with the lower leg.
Talocrural Joint: Joint Specific TreatmentPrepositioned Anterior Glide of Tibia/Fibula

Emphasis on the medial capsule.
Starting position: glide anterior. End position: after reaching maximal anterior glide, a minimal external rotation spin is performed with the lower leg.
Talocrural Joint: Joint Specific TreatmentPrepositioned Anterior Glide of Tibia/Fibula

Maximal extension: = Dorsiflexion + internal rotation of the lower leg
Starting position End position
No wedge
Talocrural Joint: Joint Specific TreatmentNeuromuscular Reeducation
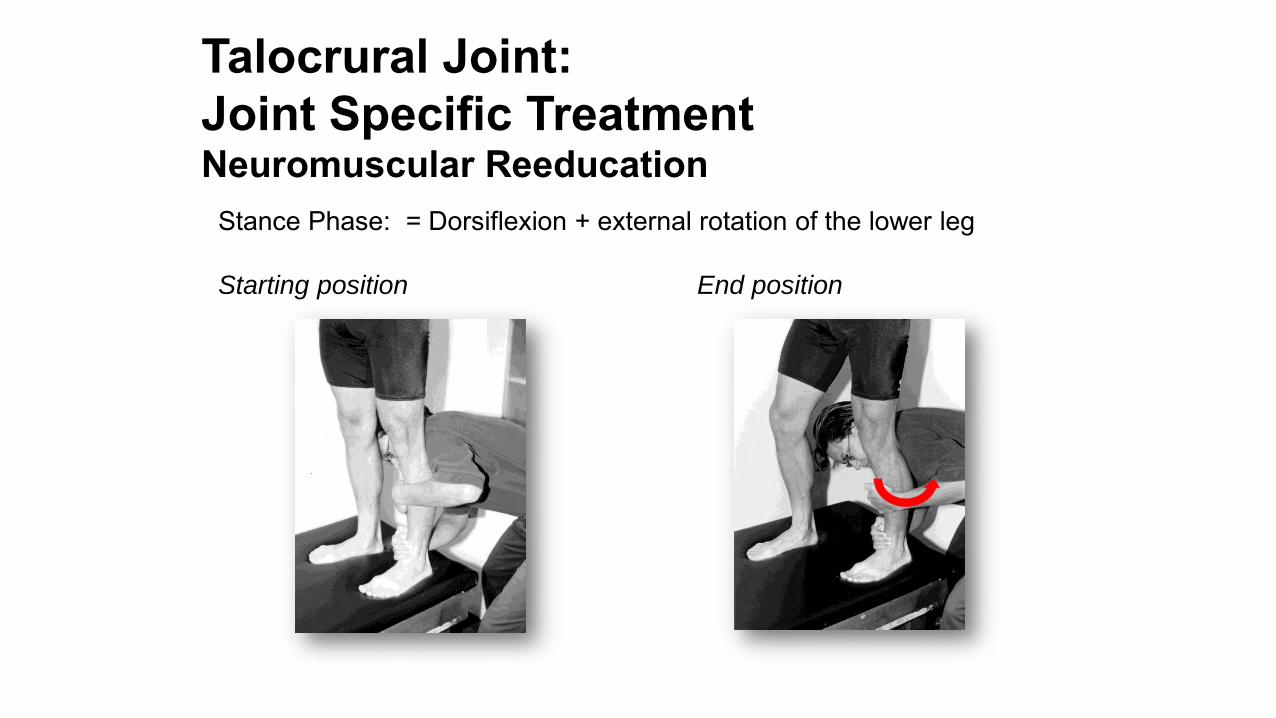
Stance Phase: = Dorsiflexion + external rotation of the lower leg
Starting position End position
Talocrural Joint: Joint Specific TreatmentNeuromuscular Reeducation

Talocrural Joint: Joint Specific TreatmentImprovement of Plantar Flexion

maximal loose-packed position
Talocrural Joint: Joint Specific TreatmentPosterior Glide of the Tibia/Fibula

Prepositioned in plantar flexionEmphasis on the lateral capsule
Glide posterior. After reaching maximal posterior glide, a minimal external rotation
spin is performed with the lower leg.
Talocrural Joint: Joint Specific TreatmentPosterior Glide of the Tibia/Fibula

Prepositioned in plantar flexionEmphasis on the medial capsule
Glide posterior. After reaching maximal posterior glide, a minimal internal rotation
spin is performed with the lower leg.
Talocrural Joint: Joint Specific TreatmentPosterior Glide of the Tibia/Fibula
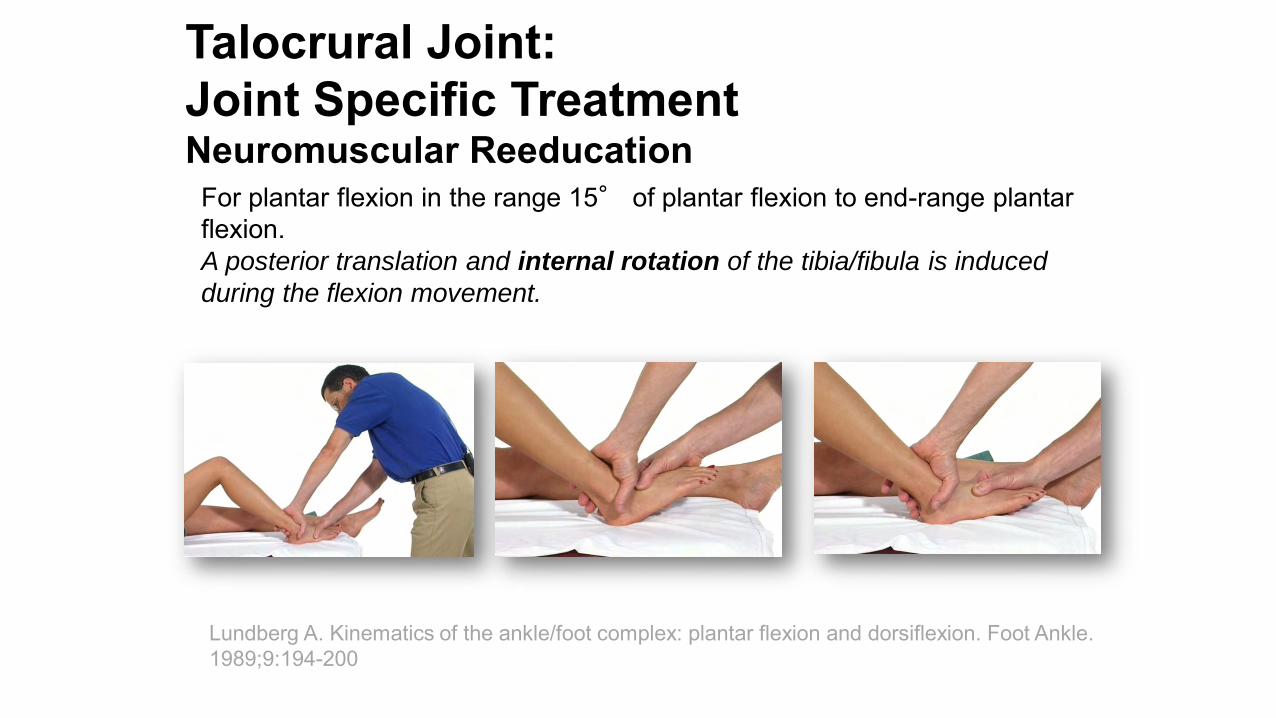
For plantar flexion in the range 15° of plantar flexion to end-range plantar flexion.A posterior translation and internal rotation of the tibia/fibula is induced
during the flexion movement.
Lundberg A. Kinematics of the ankle/foot complex: plantar flexion and dorsiflexion. Foot Ankle. 1989;9:194-200
Talocrural Joint: Joint Specific TreatmentNeuromuscular Reeducation

SUBTALAR JOINT
1 Joint Specific TestingAngular movement in inversion/eversion.
2 Joint Specific Treatment Techniques2.1. Improvement of supination/pronation
2.1.1. Traction from the maximal loose-packed position2.1.2. Medial glide/slide of the calcaneus 2.1.3. Lateral glide/slide of the calcaneus 2.1.4. Neuromuscular re-education: calcaneus medial 2.1.5. Neuromuscular re-education: calcaneus lateral 2.1.6. Proximal glide/slide of the calcaneus2.1.7. Distal glide/slide of the calcaneus2.1.7. Neuromuscular re-education: calceanus proximal2.1.7. Neuromuscular re-education: calceanus distal

Traction: from the maximal loose-packed position. Emphasis on posterior talocalcaneal joint.
Subtalar Joint Testing – Angular Movement in Inversion/Eversion
Treatment – Traction

maximal loose-packed position.
Similar technique to the alternative
technique for talocrural joint.
Here the hand is placed more distally,
over the calcaneus (MCP II is placed in
the sinus tarsi), in order to emphasize the
subtalar complex.
Close-up.
Subtalar Joint Alternative Technique for Traction

“S” SHAPE CONGRUENCY
Anteromedial calcaneus concavePosterolateral calcaneus convex
Anteromedial talus convexPosterolateral talus concave
Unable to evaluate if the limitation of motion is due to the anteromedialfacet of the STJ or the posterolateralfacet of the STJ → perform both medial and lateral glide mobilizations for restoration of pronation. Same for restoration of supination.
Subtalar Joint Gliding Techniques
MedialLateral

Calcaneus Lateral
Lateral Glide to Improve Eversion (1-D) in Anterior/Medial Talocalcaneal JointLateral Slide to Improve Inversion (1-D)in Posterior Talocalcaneal Joint
El Rassi G, Riddle EC, Kumar SJ. Arthrofibrosis involving the middle facet of the talocalcanealjoint in children and adolescents.J Bone Joint Surg Am. 2005 Oct;87(10):2227-31.
Calcaneus Medial
Medial Glide to Improve Inversion (1-D)in Anterior/Medial Talocalcaneal JointMedial Slide to Improve Eversion (1-D)in Posterior Talocalcaneal Joint
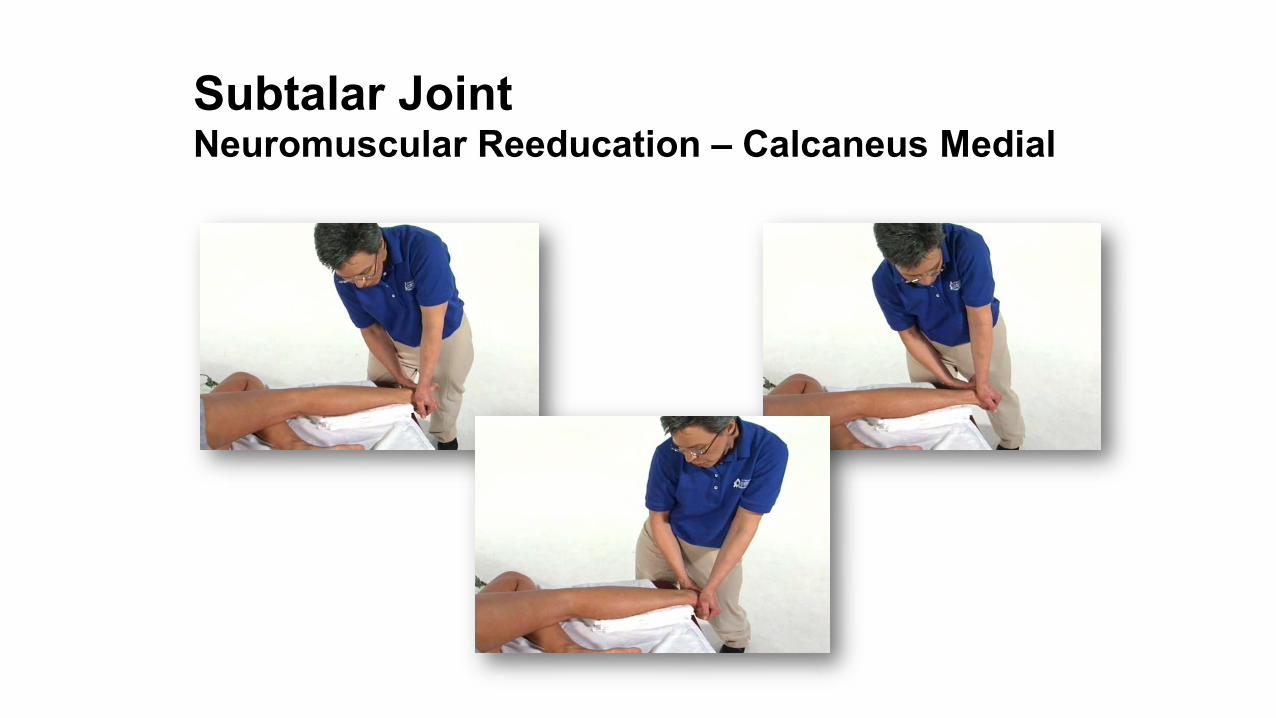
Subtalar Joint Neuromuscular Reeducation – Calcaneus Medial
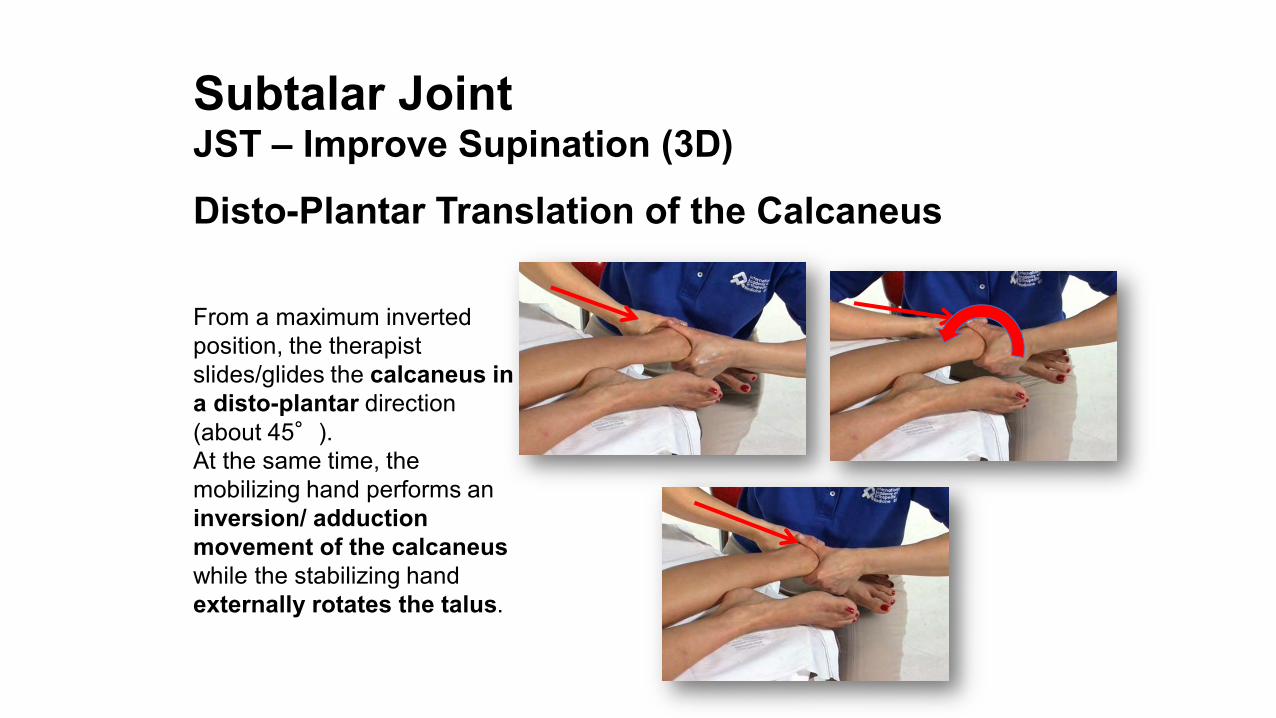
From a maximum inverted position, the therapist slides/glides the calcaneus in a disto-plantar direction (about 45°). At the same time, the mobilizing hand performs an inversion/ adduction movement of the calcaneuswhile the stabilizing hand externally rotates the talus.
Subtalar Joint JST – Improve Supination (3D)
Disto-Plantar Translation of the Calcaneus

From a maximum evertedposition, the therapist glides/slides the calcaneus in a proximo-dorsal direction (about 45°). At the same time, the mobilizing hand performs an eversion/ abduction movement of the calcaneuswhile the stabilizing hand internally rotates the talus.
Subtalar Joint JST – Improve Pronation (3D)
Proximo-Dorsal Translation of the Calcaneus

Superficial peroneal nerve▫ Traction neuropathy▫ Compression neuropathy▫ SLR with ankle plantarflexed
and inverted
O'Neill PJ, Parks BG, Walsh R, Simmons LM, Miller SD. Excursion and strain of the superficial peroneal nerve during inversion ankle sprain. J Bone Joint Surg Am. 2007 May;89(5):979-86.
Inversion Trauma Associated Injuries Neural

Inversion Trauma Associated Injuries Neural
Treatment: Neural MobilizationDistal prepositioning:
Toes in flexion
Proximal prepositioning:The hip is in slight flexion,
abduction, and external rotation, knee in flexion and the tibia externally rotated.
Movement:Slow repetitive movement from eversion into inversion of the ankle and foot.

Joint Specific Manual Therapy
Extension limitation < 20° of flexion
• Tibiofemoral Emphasis (top illustration)
• Meniscofemoral Emphasis
• Position and performance are similar toTibiofemoral emphasized capsule stretch, however femoral glide occurs posterior superior (45° in relation to tibial plateau).
• P2PS. Femur posterior/superior and in internal rotation at stretching phase. Knee is pre-positioned in extension. The hand at distal aspect of thigh per-forms rhythmic spin into internal rotation during posterior/superior glide. Avoid direct pressure on the suprapatellar recess, since this can be uncomfortable for the patient.

MeniscotibialEmphasisPOSITIONThe patient lies supine. The distal femur is supported by a sandbag or towel, so that the proximal tibia has no contact with the treatment table.PERFORMANCEThe distal femur is stabilized with one hand, while the hand at the proximal tibia performs a posterior glide, parallel to the tibial plateau. In the stretching phase a tibial spin in external rotation is added.P2PG. Tibia posterior and in external rotation at the stretching phase. The knee is pre-positioned in extension. The hand at the distal aspect of the thigh fixates the thigh while the proximal hand at the tibia performs a rhythmic spin into external rotation during the posterior glide mobilization.
Joint Specific Manual TherapyExtension limitation < 20° of flexion

Thank you