new therapies for treatment of valvular heart disease- is ... · new therapies for treatment of...
TRANSCRIPT

New Therapies for Treatment of
Valvular Heart Disease-
Is Open Heart Surgery Still
Necessary

Part 2: Procedures Available and
Options for Candidates
Frank J. Lutrin, MD FACS
Lutheran General Hospital
Cardiac Surgery Associates

No disclosures

In the old days…..
Aortic valve disease was treated with Mechanical Aortic
Valve replacement
Along came tissue valve replacement to offer a
different option
Decisions weighed the longevity advantage of
Mechanical against its disadvantage of need for lifelong
anticoagulation and thromboembolic risks









Options:
Mechanical or tissue AVR
Valve Repair or resuspension
Aortic Root Replacement
Valve sparing aortic root replacement
AVR plus ascending aorta replacement
Any of above in combo with CABG
Transvalvular aortic valve replacement
Options for AVR Tailored specifically
to patient considerations

Patient’s suitability for open operation
Type of aortic valve problem: stenosis versus
incompetence
Isolated AVR may decide mini versus full sternotomy
Associated coronary artery disease
Associated aneurysmal disease
Etiology of the aortic valve disease
Conditions requiring Tailoring the
options

Pathway to determine specific
treatment option

Pathway to determine specific
treatment option

Suitability for open operation: age, previous operations,
overall physical state and comorbidities
Coronary angiogram
Assessment of LV function
Evaluation of Aorta from root to arch
Discussion of valve type: tissue versus mechanical
Pre-operative workup

should be addressed at the time of AVR
May require single or multivessel revascularisation
May eliminate the option of mini sternotomy
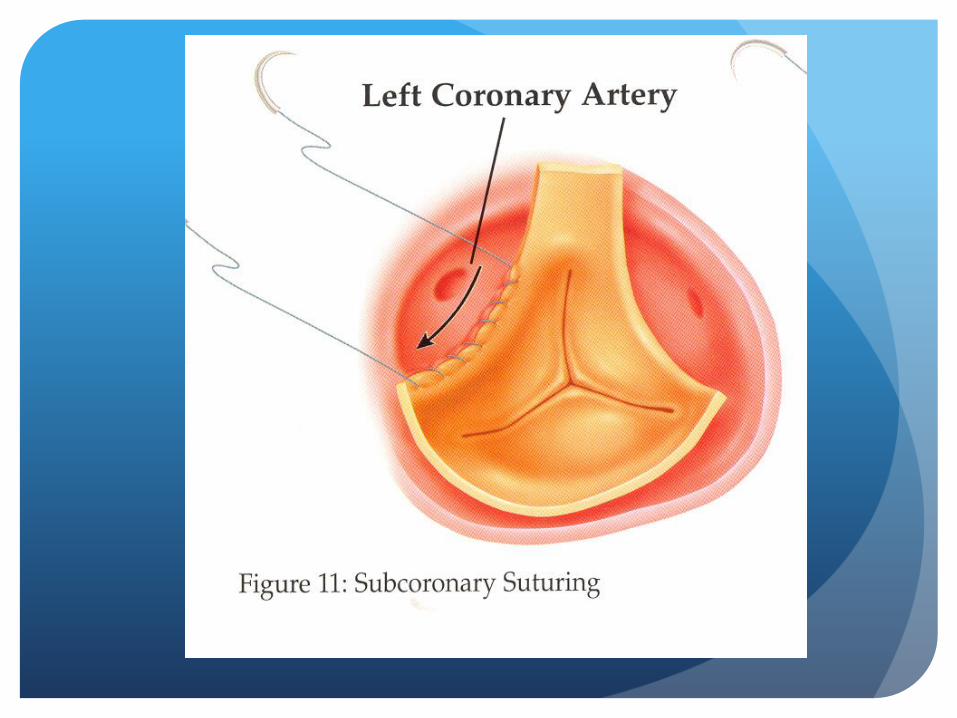
Shows relationship of coronaries to annulus
Coronary anatomy




Can help determine risk assessment
Associated pulmonary hypertension and Nitric Oxide
requirement
Planning for inotrope requirement
LV function

Normal Aorta
Hostile Aorta
Aortic root/sinus of valsalva aneurysm
Ascending aortic aneurysm after STJ
Involvement of Aortic Arch
Aortic Concerns

Evaluation of Aorta

Evaluation of Aorta

Evaluation of Aorta

Endocarditis
Leaflet prolapse
Rheumatic Stenosis and regurgitation
Annular dilatation/Aneurysmal distortion of valve
Calcific Aortic Stenosis
Bicuspid or trileaflet
Etiology of Disease Process


Full sternotomy
Mini sternotomy
CABG with LIMA and/or veins
Femoral cannulation or aortic cannulation
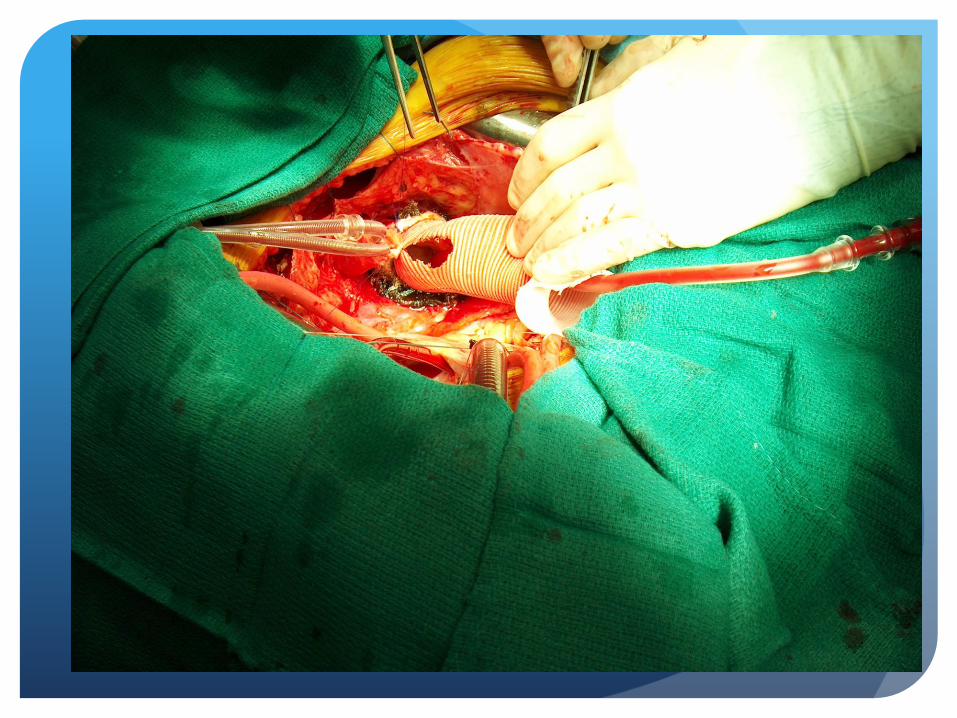
Root replacement with Valved conduit
Valve sparing Aortic root replacement
Ascending aorta replacement with or without Arch
Need for circulatory arrest
Planning of operation

General Anesthetic
Sternotomy
Cardiopulmonary bypass
Arresting the heart
Open aorta, remove valve, decalcify annulus, seat prosthesis
Close and restart
Wean off bypass
What does a standard AVR
encompass?
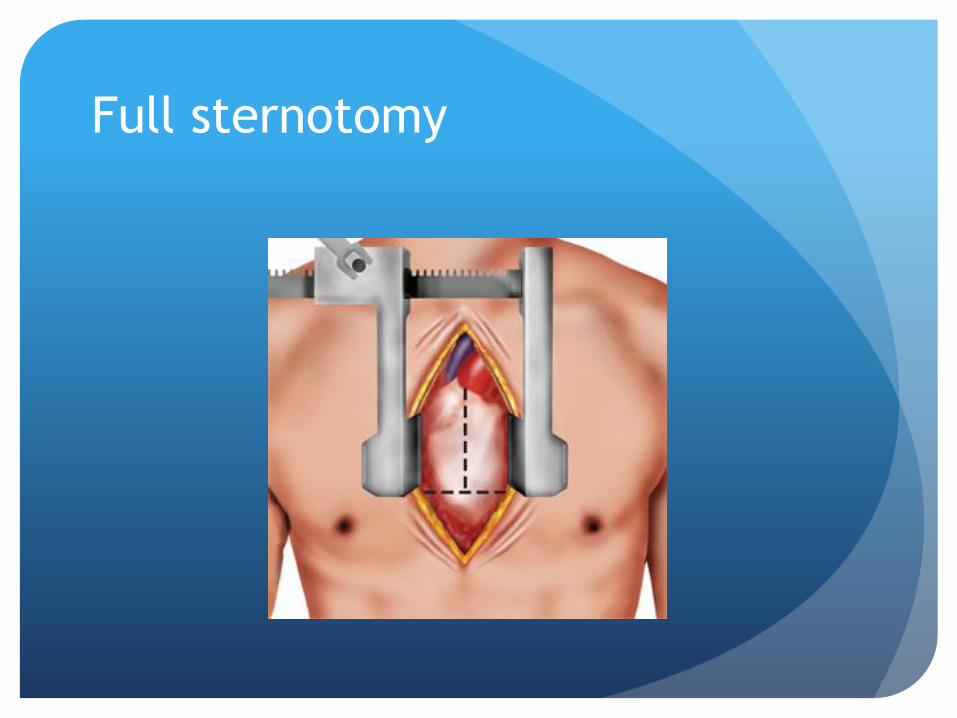
Full sternotomy

Mini sternotomy

General Anesthetic
Sternotomy
Cardiopulmonary bypass
Arresting the heart
Open aorta, remove valve, decalcify annulus, seat prosthesis
Close and restart
Wean off bypass
What does a standard AVR
encompass?


General Anesthetic
Sternotomy
Cardiopulmonary bypass
Arresting the heart
Open aorta, remove valve, decalcify annulus, seat prosthesis
Close and restart
Wean off bypass
What does a standard AVR
encompass?







Composite Valved Graft Aortic Root Replacement
Valve Sparing Root Replacement (normal functioning
Valve)
Aortic Root Aneurysm











Extreme frailty
Advanced age
Previous sternotomy for heart surgery
Previous radiation
Previous mediastinitis
Hostile Aorta
Very poor LV function
Inoperable

Femoral Access
Apical Access
Pre-op stenting if needed
CTA to evaluate Aorta and runoff/Femorals/Iliacs
CTA and Echo to determine annular size
Inoperable or high risk operable
Transcatheter AVR (TAVR)








Long Term Outcomes of AVR in
Octogenerians
515 patients in the Emory Hospital System (1996-2006)
60-69y (206 pts) 70-79y (221 pts) 80-89y (88 pts)
In Hospital Mortality and LOS similar in all groups
Pre op COPD, stroke and RF were predictors of in-hospital mortality
Age significantly impeded long term survival along with smoking, stroke, diabetes and RF
Age on its own not prohibitory : median survival 7.4 years for octogenerians

Placement of AoRtic TranscathertER
Valve Trial (PARTNER)
PARTNER A : looked at surgically inoperable patients
comparing TAVR with standard non-operative therapy
Partner B: looked at surgically high risk patients
comparing TAVR with surgical AVR

PARTNER Mortality
Partner A:
30 day Mortality 3.4% (TAVR) vs 6.5% (AVR)
1 year Mortality 24.2% (TAVR) vs 26.8% (AVR)
Partner B:
30 day Mortality 5.0% (TAVR) vs 2.8% (Std)
1 year Mortality 30.7% (TAVR) vs 50.7% (Std)

TAVR has substantially reduced risk of cardiac death in
inoperable patients with AS
TF TAVR has lower peri-procedural risk than TA TAVR or
Surgical AVR
TF TAVR has higher early Cardiovascular mortality than TA
TAVR or Surgical AVR

PARTNER Neuro events
Early Events within 1 week 4.6% (TAVR) vs 1.4% (AVR
Late 2year data reaches parity

STS Database (1991-2007)
145 911 patients 65 years and older (1026 centers)
Median age 76 years
CLD 16%
Renal Failure 6%
Heart Failure 38%
Reoperation 12%

Median Survivals (STS DB)
60-69yrs 13 years (10 years with CABG)
70-79yrs 9 years ( 8 years with CABG)
>80yrs 6 years ( 6 years with CABG)
If pre-op STS risk >10% Median Survival 2.5-2.7 years

STS Risk factors affecting Median
Survival
CLD 50% reduction
Renal Failure 50% reduction
Heart Failure 25% reduction
Reoperation 25% reduction

Conclusions
Surgical AVR best first option for aortic valve disease
Transfemoral TAVR is a very good option for inoperable
AS patients and for high risk patients with non-CV risks
like renal failure or CLD
TAVR of any access (TA/Tao/TF) has substantial survival
benefit in surgically inoperable AS patients compared
with no intervention





Endovascular Valve Edge-to-Edge Repair
Study II (EVEREST II) Trial
Mortality rates similar at 1 year for Surgical Mitral repair
versus Mitraclip
Mitraclip repair had lower reduction of MR at 1 year
Mitraclip: 20% required Mitral Surgery at 1 year
Mitral Repair: 2.2% required Mitral Surgery at 1 year
Mitraclip: 25% required Mitral Surgery at 4 years
Mitral Repair: 5.5% required Surgery at 4 years