new targets & new drugs in hepatocellular carcinoma
TRANSCRIPT

NewTargetsandNewAgentsinHepatocellularCarcinoma
EricRaymondMD,PhDChairofMedicalOncology
@GroupeHospitalierParisSaint-JosephFrance
Disclosures
• ConsulEngrole:– Pfizer– NovarEs– EliLilly– Ipsen

Normaliza9onofTumorMicroenvironmentinHepatocellular
CarcinomaEricRaymondMD,PhD
ChairofMedicalOncology@GroupeHospitalierParisSaint-Joseph

Cellular&MolecularComponentsoftheHepatocellularCarcinomaMicroenvironment
EndothelialcellsPericytesVEGFR-PDGFR
Tcells(CD4-Treg)CD4:PD1-CTLA4-CD28Treg:CD73-CD39
Dendri9ccellsPDL1-PD1-MSHII-CD80/86
TumorassociatedmacrophagesCXCR4-TGFβR
TumorcellsTGFβR-MET-PDL1
FibroblastsFGFR
TGFβHGFFGF19IL8IL10
SDF1/CXCL12

Characteris9csofHepatocellularCarcinomaMicroenvironment
• Likelytovaryaccordingtothetypeoftumorcarcinogenesis– Alcohol– ViralhepaEEsB/CinducedinflammaEon– NASH– Others
• Likelytobeinfluencedbyfocalhypoxia– Tumorangiogenesisbeinggenuineorinducedbysorafenib– InducEonofmesenchymaldifferenEaEon– InducEonoflacEcacidmetabolism– FacilitatetheoccurrencesofspecificoncogenicmutaEons
• Associatedwithlocalimmunosuppression– InhibiEonofT-cellfuncEons(PD1/PDL1,CTLA4)
‘Epigene(c’changesmaybefocalaccoun(ngfortumorheterogeneityanddri9occurringover(mefacilita(ngresistancetosingleagenttherapy,pledgingforcombina(ons

VEGFR&PDGFRasAn9-angiogenicTargetsforHepatocellularCarcinoma
NewTargetsandNewAgentsinHepatocellularCarcinoma
EndothelialcellsPericytesVEGFR-PDGFR

Learningfrom7YearsofExperiencewithSorafenibinAdvancedhepatocellularcarcinoma
SorafenibBe>erthanSorafenib
2005
2006
2007
2008
2009
2010
2011
2012
5
10
15
Med
ian
over
al s
urvi
val
of s
oraf
enib
(mon
th)
Lag times of accrual
SHARP
SUNITINIB
GIDEON
BRISK
ASIAN-PACIFICSUNITINIB
BRISKPlacebo SHARP
Placebo ASIAN-PACIFIC
Non-Asian patients
Asian patients
FaivreS,deGramontA,RaymondE.TargetOncol.2016
SofarnodrughasbeenabletocompetewithsorafenibasfirstlinetherapyinHCC

RegorafenibaMu9kinaseInhibitor
F
phaseIIIRESORCEtrial

RegorafenibaMu9kinaseInhibitor
Regorafenibwasannouncedtoprovideoverallsurvivalbenefitoverplaceboinsecondlineinpa9entswhohavefailedsorafenibfirstline(DatapresentedatthisWORLDGI2016)

PD1&PDL1asTargetsforHepatocellularCarcinoma
NewTargetsandNewAgentsinHepatocellularCarcinoma
Tcells(CD4-Treg)CD4:PD1-CTLA4-CD28Treg:CD73-CD39
Dendri9ccellsPDL1-PD1-MSHII-CD80/86
TumorcellsTGFβR-MET-PDL1

MHC
PD-L1
PD-1
PD-1
T-cellreceptor
PD-L2
Tcell
NFκB
Other
PI3K
Tumorcell
IFNγ
IFNγR
Shp-2
Nivolumab
ImmuneCheckpointInhibi9onbyNivolumab
• NivolumabisafullyhumanIgG4anE-PD-1monoclonalanEbodythatselecEvelyblockstheinteracEonbetweenPD-1andPD-L1/PD-L2,1restoringT-cellimmuneacEvitydirectedagainstthetumorcell
1. TopalianSL,etal.NEnglJMed.2012;366:2443-2454

CA209-040:StudyDesign
• PaEentsreceivednivolumabQ2Wforupto2years(maximumof48doses),dependingonresponse– Imagingfordiseaseassessmentperformedevery6weeks
• A3+3designwasusedinthephase1doseescalaEonphase• Here,wereportinterimresultsfromtheongoingdoseescalaEonphaseandpartoftheexpansionphase
DoseEscala9on Expansion
Uninfectedsorafenibprogressors3mg/kg(n=50)
HCV-infectedExpandat3mg/kg
(n=50)
HBV-infectedDoseTBD(n=50)
Uninfected 0.3mg/kg 1mg/kg 3mg/kg 10mg/kg0.1mg/kg
HCV-infected 0.3mg/kg 1mg/kg 3mg/kg 10mg/kg
Uninfectedsorafenib-naïveorintolerant3mg/kg(n=50)
HBV-infected 0.3mg/kg0.1mg/kg 1mg/kg 3mg/kg 10mg/kg
AnthonyB.El-Khoueiryetal.ASCO2015

• 58-year-oldwhitemalewithHCV-infectedHCC,ECOG0,Child-PughA5• Progressedonsorafenib
CA209-040:DurablePar9alResponsetoNivolumab
Week12 Week48Baseline
Arterial
Venous+ +
+
+
+
++
+
++
AnthonyB.El-Khoueiryetal.ASCO2015
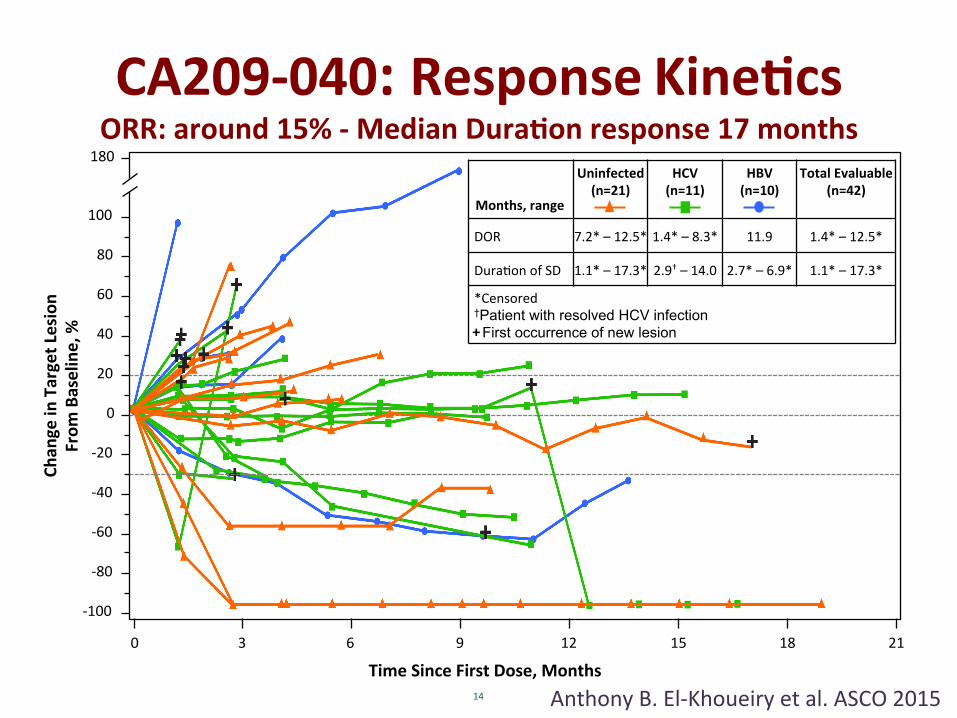
CA209-040:ResponseKine9csORR:around15%-MedianDura9onresponse17months
TimeSinceFirstDose,Months
Chan
geinTargetLesion
From
Baseline,%
180
0 3 6 9 12 15 18 21
-100
-80
-60
-40
-20
0
20
40
60
80
100
Months,range
Uninfected(n=21)
HCV(n=11)
HBV(n=10)
TotalEvaluable(n=42)
DOR 7.2*–12.5* 1.4*–8.3* 11.9 1.4*–12.5*
DuraEonofSD 1.1*–17.3* 2.9†–14.0 2.7*–6.9* 1.1*–17.3*
*Censored†Patient with resolved HCV infection First occurrence of new lesion
14
+
AnthonyB.El-Khoueiryetal.ASCO2015

CA209-040:PreliminaryOverallSurvival
OverallSurvivalRate,%(95%CI)* Total(N=47)
At9months 70(52–82)
At12months 62(42–76)
*OverallsurvivalesEmatedusingKaplan-Meiermethod
AnthonyB.El-Khoueiryetal.ASCO2015
MedianOS:14monthsirrespec9veofpriorsorafenibtreatmentAE>grade3:1%-Welltolerated
UpdateASCO2016

HGF&c-METInhibi9oninHepatocellularCarcinoma
NewTargetsandNewAgentsinHepatocellularCarcinoma
HepatocytesTumorcellsTGFβR-MET-PDL1

mRNAoverexpression
Proteinoverexpression
Geneamplifica9on
Muta9on
ChronicliverinflammaEon(viral–others)
Fibroblastsandfibrosis
Localimmunosupression
GenuineHypoxia
Treatmentinducedhypoxia(embolizaEon,anE-angiogenic)
EpigeneEcchangesassociatedwithHGF/c-METacEvaEon
HGFsEmulaEonofhepatocytesandhepatocarcinomacellsharboringc-MET

c-METinhibitorsinlatestagedrugdevelopment
METIV-HCC–Tivan9nib–phase3trial
CELESTIAL–Cabozan9nib–phase3trial
• Firstgenera(on• Specificity?• Resultspending

Inhibi9onofc-METWithTepo9nib

TolerabilityandAc9vityofSecond-LineTepo9nib,aPotentandHighlySelec9vec-MetInhibitor,inPa9entswithAdvancedHepatocellular
CarcinomaPreviouslyTreatedwithSorafenib
30
10
-10-20
-40-50-60B
est r
elat
ive
chan
ge in
sum
of lo
nges
t dia
met
erin
bas
elin
e (%
)
Tepotinib 300 mgDose level
Tepotinib 500 mg20
0
-30
Abstract No. 238
Faivreetal.WorldGI2016
CT after 2 cycles showed objective response by RECIST (-48%)
PET scan after 2 cycles showed significant decrease of size and metabolic activity

FGF19&FGFR4asTargetsinHepatocellularCarcinoma
NewTargetsandNewAgentsinHepatocellularCarcinoma
TumorcellsTGFβR-MET-PDL1
FibroblastsFGFR
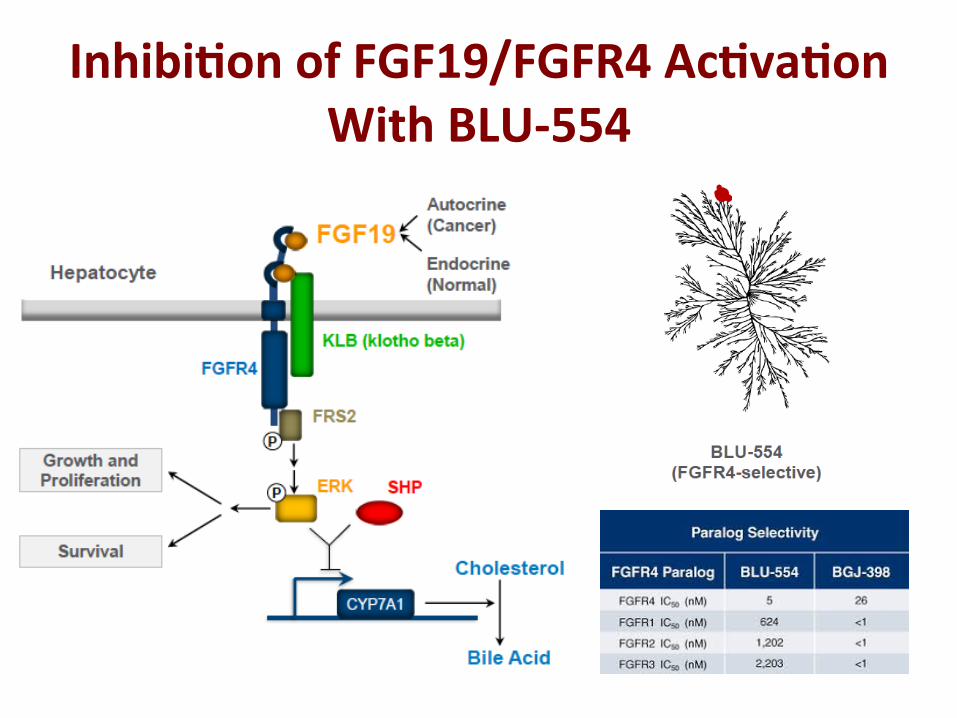
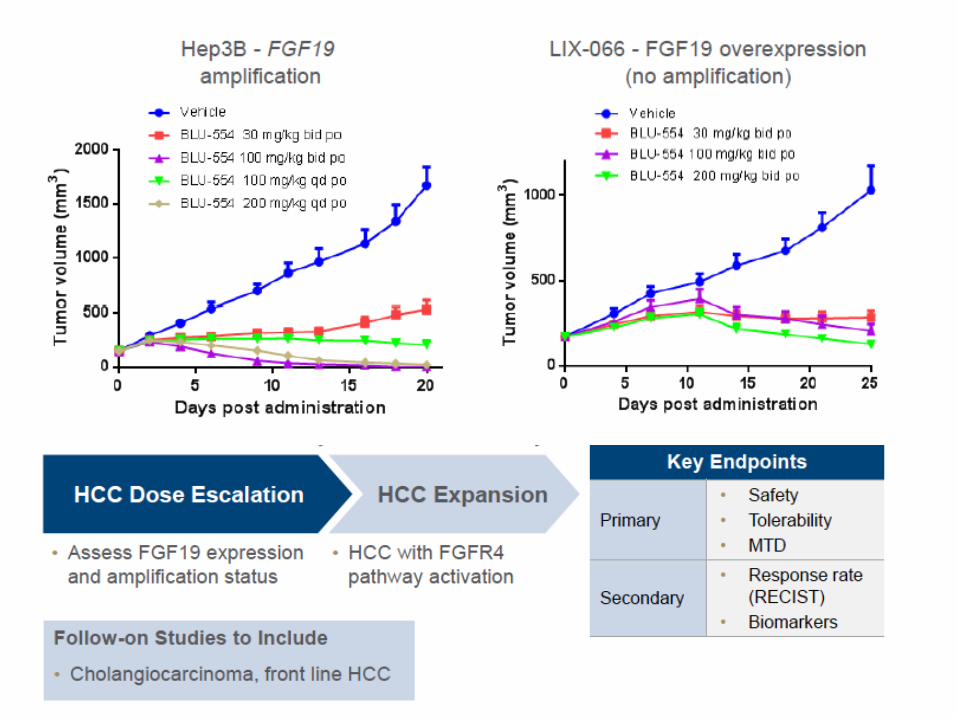
Inhibi9onofFGF19/FGFR4Ac9va9onWithBLU-554

TGFβ&TGFβ-RasTargetsinHepatocellularCarcinoma
NewTargetsandNewAgentsinHepatocellularCarcinoma
EndothelialcellsPericytesVEGFR-PDGFR
Tcells(CD4-Treg)CD4:PD1-CTLA4-CD28Treg:CD73-CD39
TumorassociatedmacrophagesCXCR4-TGFβR
TumorcellsTGFβR-MET-PDL1

• >30TGFβmembers(TGFβ1-3,acEvins,NODAL,BMP,GDF,AMH)
NeuzilletC.,Pharmacol.Ther.(2015)WakefieldLM.,Nat.Rev.Cancer(2013)
CanonicalandNon-CanonicalTGFβPathway

Galuniser9b:TGF-βRIInhibitorinHepatocellularCarcinoma

TumoralExplant Slicing
Control
DrugA
DrugB
CultureanddrugtesEng
O2
CO2
O2/CO2/T°monitor
Evalua9on of Drugs in Ex Vivo Organotypic Culture Assays From SurgicalSpecimensofHumanHepatocellularCarcinoma:StudyingtheTumorCells inTheirGenuineStroma
BySerovaetal,Oncotarget2015

Exvivo Prolifera9onControl TGFβinh.
Apoptosis
P-SMAD2/3(PDbiomarker)
(13pts)
(13pts)
(11pts)
TGFβRIInhibi9onInducedbyGaluniser9binHumanHepatocellularCarcinomaExplants
BySerovaetal,Oncotarget2015

A Phase 2 Study of a Second Line Galunisertib in Patients With Advanced Hepatocellular Carcinoma
StudyDesignforPartAandPartB
Screening Patients with
Child Pugh A or B7 Hepatocarcinoma
who progress Under sorafenib
Galunisertib 160 mg/day
Galunisertib 300 mg/day
R A N D O M I Z E
Galunisertib 300 mg/day
Part A AFP ≥1.5 ULN
Part B AFP <1.5 ULN
Abbreviation: ULN, upper limit of normal.
CourtesyofFaivreS.etal.Pres.ASCOGI2014andASCO2016

Galuniser9b(TGFβRIInhibitor)inPa9entsWithHepatocellularCarcinoma
n/N (%) Median AFP responders 25/103 (24%) 21.4 mo AFP non-responders 78/103 (76%) 6.8 mo
Overallsurvival
AFPresponders=paEentswhodecreasedcirculaEngAFPlevelsby>20%
AFPnonresponders
AFPresponders
CourtesyofFaivreS.etal.Pres.ASCOGI2014andASCO2016
Part A AFP ≥1.5 ULN
Part B AFP <1.5 ULN

ArmanddeGramontunpublished
PD-L1ExpressioninHepatocellularCarcinoma
Tumorboundary
CD3
PD-L1
Combina9onwithPD-L1inhibitors
T-cells
Cancercells
InvivotransgenicC57B16/ASB-Bmicemodel

Galuniser9binCombina9onWithSorafenibInvivotransgenicC57B16/ASB-Bmicemodel
At12weeks
Randomization N = 32
Transgenic C57Bl6/ASV-B Mice; age 8 weeks
Placebo N = 8
Sorafenib + galunisertib
N = 8
Echo-Doppler Every 4 weeks
Sorafenib (30 mg.kg-1)
N = 8
Galunisertib (100 mg.kg-1)
N = 8
Rijeras-Raballanetal.Unpublisheddata

NewTargetsandNewAgentsinHepatocellularCarcinoma
Sorafenib(1stline)
Regorafenib(2ndline)
Tumorangiogenesis
Galuniser9b(TGFβ-RI)
Tepo9nib(c-MET)
BLU‑554
(FGF19/FGFR4)
Microenvironmentsignaling
NivolumabPembrolizumab
(PD-L1)
IpilimumabTremelimumab
(CTLA4)
Immunestroma
ç Combina9onsè

Conclusions• Variouscomponentsoftumormicroenvironmentcouldbeusedastargetstocontroltumorgrowthinhepatocellularcarcinoma
• Inhibi9onoftumorangiogenesis,microenvironmentsignalingandlocalimmunosuppressionappearaspromisingop9onsfortumorgrowthcontrol
• Combina9ontherapiesnormalizingthemicroenvironmentofferpromiseforop9malcontrolofhepatocellularcarcinogenesis

Thanksforyouraoen9on
EricRaymondMD,PhDChairofMedicalOncology
@GroupeHospitalierParisSaint-JosephFrance