new student enrollment packet - amazon s3 · new student enrollment packet . ... o 3 hepatitis b o...
TRANSCRIPT
Twin Falls School District 201 Main Ave. W. Twin Falls, ID 83301 (208) 733-6900 www.tfsd.org
NEW STUDENT ENROLLMENT PACKET Welcome to the Twin Falls School District! Enclosed are the registration forms that are required for your child to be enrolled in one of our schools. In addition to these forms, the following documents are mandatory:
• Certified Birth Certificate o www.vitalrecords.dhw.idaho.gov o www.vitalchek.com (if outside of Idaho)
• Complete Immunization Records o 5 DTaP o 2 MMR o 4 Polio o 3 Hepatitis B o 2 Vericella o 2 Hepatitis A o 7th graders only: TDaP Booster and Meningoccal o Children must be in compliance with Idaho Immunization Laws in
order to attend school. You can ask you school’s secretary for more information.
• Proof of Residence o Utility bill, lease, or rental contracts
Hii ni muhimu sana. Tafadhali tafuta mtu
wa kutafsiri.
C'est im
portant. S'il vous plait,
trouvez un traducteur.

Student Enrollment FormTwin Falls School District #411201 Main Ave W.Twin Falls , ID 83301 Immunizations
Phone: 208-733-6900 Proof of ResidencyFax: 208-733-6987 Birth Certificatewww.tfsd.org
Student Last Name Student First Name Student Middle Name
Name Child Will Use at School Date of Birth
Male
Primary Contact Phone Number
Grade Level This Academic Year
Female
Home Address Street, Apt/Suite
City, State, Zip Code
Street, Apt/Suite
City, State, Zip Code
Yes No
Mailing Address (if different from home address)
Is the student Hipanic or Latino?
What is the student's race?
Has the student previously been enrolled in the Twin Falls School District? If so, where?
AM
PM
Offical Use Only
If Kindergarten, AM or PM
preference?
Gender
American Indian or Alaska Native
Students must be registered in the elementary school zone where they reside. If you wish to enroll in a school outside the zone in which you reside or from outside the district, you must follow the transfer policy.
Within which elementary school zone is the student's home address?
Ethn
icity
School:
AsianBlack or African American
WhiteNative Hawaiian/ Other Pacific Islander

The most recent copy of this form should be kept in the student cumulative file Form Updated October 2017
Father's Name (Last, First)Father's Day PhoneFather's EmployerFather's Home PhoneFather's Email
Mother's Name (Last, First)Mother's Day PhoneMother's EmployerMother's Home PhoneMother's Email
Other Legal Guardian's Name (Last, First)Relationship to StudentsGuardian's Day PhoneGuardian's EmployerGuardian's Home PhoneGuardian's Email
Both ParentsWho does the student reside with?
Yes No Number of BrothersNumber of Sisters
Does the student have siblings in the Twin Falls School District
List siblings first and last names
Who has guardianship of this student? Father Only
Pare
nt/G
uard
ian
Info
rmat
ion
This means the student has a parent, step-parent or sibling serving in the active or resere components of the Army, Navy, Air Force, Marine Corps, Coast Guard, or National Guard. The TFSD is required to collect
this information under the federall education law ESSA.
Is the student a military connected student?
National Guard or Reserve
Unable to Provide
Active Duty
Not Military Connected
Guardian OnlyMother Only

The most recent copy of this form should be kept in the student cumulative file Form Updated October 2017
Name (Last, First)PhoneRelationshipPhone Type
Name (Last, First)PhoneRelationshipPhone Type
Name (Last, First)PhoneRelationshipPhone Type
No
No
Address of Last School AttendedPhone Number of Last School Attended
Health and Emergency Information
Name of Last School Attended
Dentist's NameDentist's Phone Number
List any medications prescribed by a licensed medical practitioner. This includes inhalers. (if medication is administered at school, proper documentation is required.)
Emergency Contact #1
Emergency Contact #2
Parents are always the first contact but please provide information for individuals (other than
parent/guardian) the school may contact in case of student illness or injury and parents cannot be
reached.
Doctor's NameDoctor's Phone Number
Will the student ride a school bus to or from school? YesIf yes, please fill out the bus transportation services form included in this packet.
Emergency Contact # 3
Previous School Attended (outside
the TFSD)
List any allergies and/or health conditions the student may have. This includes asthma.
Will the student ride a bike to or from school? Yes
Fax Number of Last School Attended
The most recent copy of this form should be kept in the student cumulative file Form Updated October 2017
Special EducationResource ProgramsSelf Contained
Adapted Physical EducationLimited English Proficient504Gifted and TalentedMigrant
Speech TherapyHomelessProbationTitle 1 MathTitle 1 Reading
Who is filling out this form?
Special Programs
Please check any special programs or services in which the student has
participated.
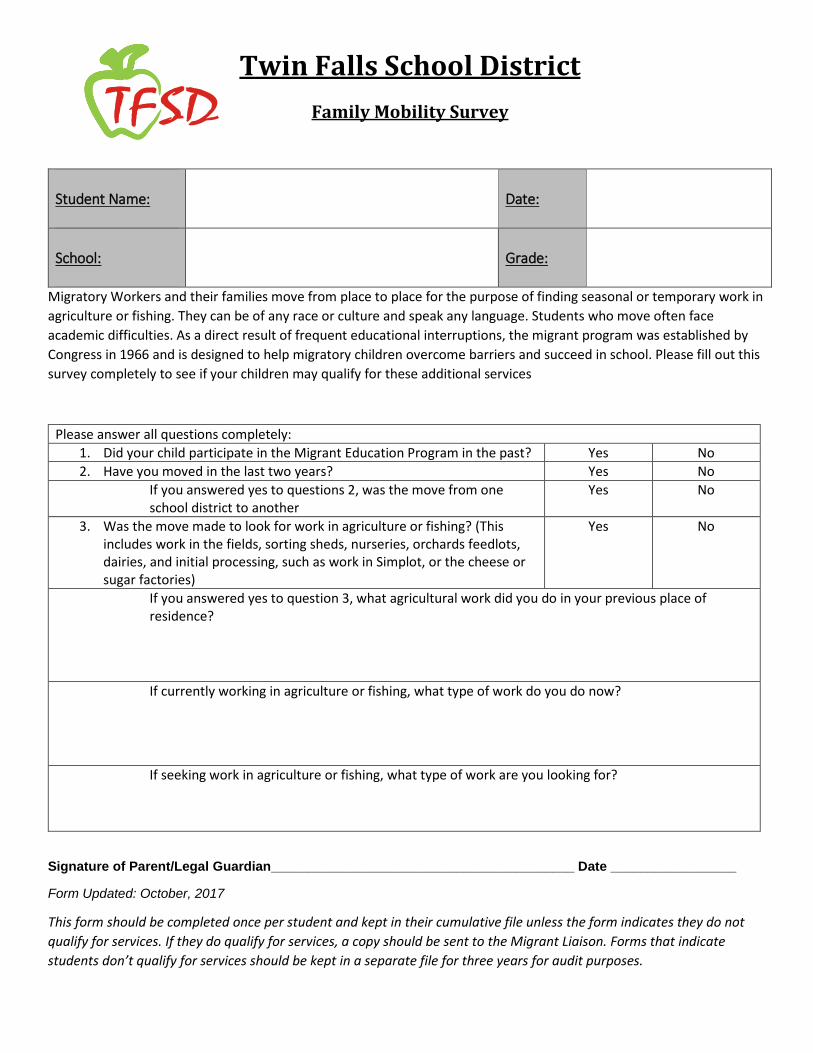
Twin Falls School District Family Mobility Survey
Student Name:
Date:
School:
Grade:
Migratory Workers and their families move from place to place for the purpose of finding seasonal or temporary work in agriculture or fishing. They can be of any race or culture and speak any language. Students who move often face academic difficulties. As a direct result of frequent educational interruptions, the migrant program was established by Congress in 1966 and is designed to help migratory children overcome barriers and succeed in school. Please fill out this survey completely to see if your children may qualify for these additional services
Please answer all questions completely: 1. Did your child participate in the Migrant Education Program in the past? Yes No 2. Have you moved in the last two years? Yes No
If you answered yes to questions 2, was the move from one school district to another
Yes No
3. Was the move made to look for work in agriculture or fishing? (This includes work in the fields, sorting sheds, nurseries, orchards feedlots, dairies, and initial processing, such as work in Simplot, or the cheese or sugar factories)
Yes No
If you answered yes to question 3, what agricultural work did you do in your previous place of residence?
If currently working in agriculture or fishing, what type of work do you do now?
If seeking work in agriculture or fishing, what type of work are you looking for?
Signature of Parent/Legal Guardian_________________________________________ Date _________________
Form Updated: October, 2017
This form should be completed once per student and kept in their cumulative file unless the form indicates they do not qualify for services. If they do qualify for services, a copy should be sent to the Migrant Liaison. Forms that indicate students don’t qualify for services should be kept in a separate file for three years for audit purposes.
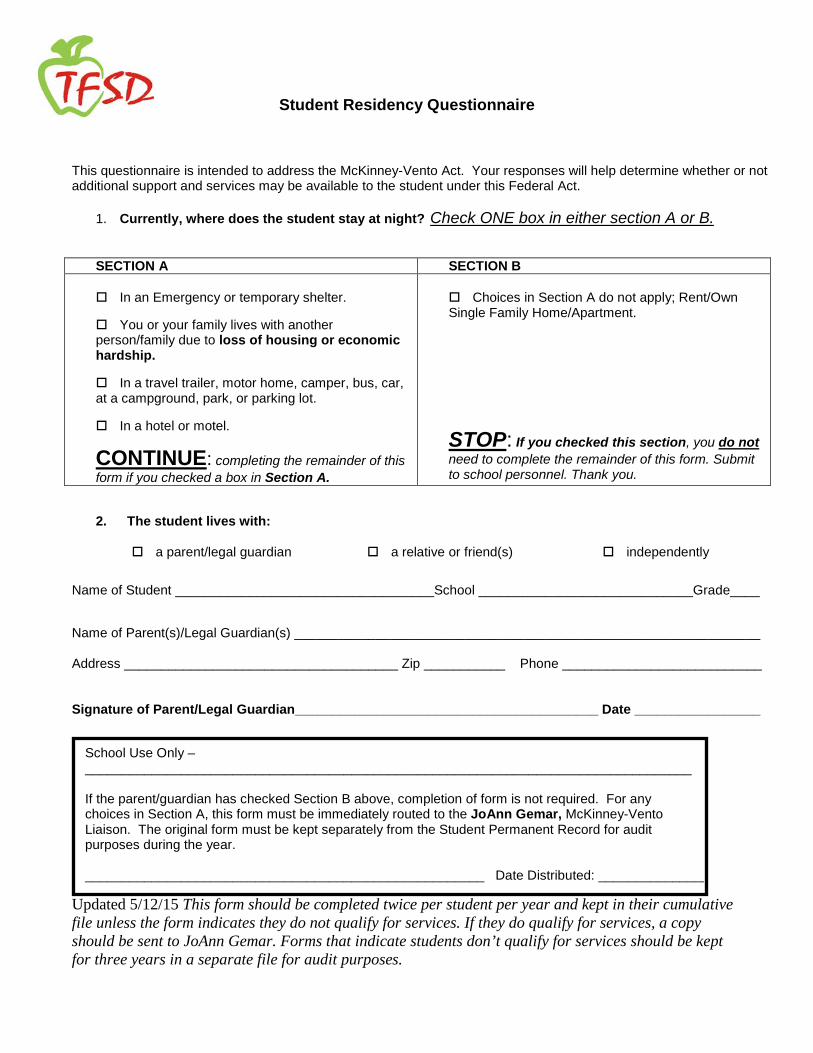
Student Residency Questionnaire
This questionnaire is intended to address the McKinney-Vento Act. Your responses will help determine whether or not additional support and services may be available to the student under this Federal Act.
1. Currently, where does the student stay at night? Check ONE box in either section A or B.
SECTION A SECTION B In an Emergency or temporary shelter. You or your family lives with another person/family due to loss of housing or economic hardship. In a travel trailer, motor home, camper, bus, car, at a campground, park, or parking lot. In a hotel or motel.
CONTINUE: completing the remainder of this form if you checked a box in Section A.
Choices in Section A do not apply; Rent/Own Single Family Home/Apartment.
STOP: If you checked this section, you do not need to complete the remainder of this form. Submit to school personnel. Thank you.
2. The student lives with:
a parent/legal guardian a relative or friend(s) independently
Name of Student ___________________________________School _____________________________Grade____
Name of Parent(s)/Legal Guardian(s) _______________________________________________________________ Address _____________________________________ Zip ___________ Phone ___________________________
Signature of Parent/Legal Guardian_________________________________________ Date _________________
School Use Only – __________________________________________________________________________________ If the parent/guardian has checked Section B above, completion of form is not required. For any choices in Section A, this form must be immediately routed to the JoAnn Gemar, McKinney-Vento Liaison. The original form must be kept separately from the Student Permanent Record for audit purposes during the year. ______________________________________________________ Date Distributed: _______________
Updated 5/12/15 This form should be completed twice per student per year and kept in their cumulative file unless the form indicates they do not qualify for services. If they do qualify for services, a copy should be sent to JoAnn Gemar. Forms that indicate students don’t qualify for services should be kept for three years in a separate file for audit purposes.

Twin Falls School District Statewide Home Language Survey
Our school district along with the Idaho State Department of Education and the Office for Civil Rights require that students’ language(s) are identified. This survey’s purpose is to determine whether they are potentially eligible for language services.
Student Name:
Date:
Birthdate:
Gender: Male Female
School:
Grade:
1. What language(s) are spoken in the home?
____________________________________________________________________________________________________
2. What language(s) does your student speak most often?
___________________________________________________________________________________________________
3. Which language(s) did your student first learn?
___________________________________________________________________________________________________
4. Which language does your child speak with you? ____________________________________________
5. Which language do you use when speaking with your child? _______________________________
6. Which language do you want phone calls and letters? _______________________________________
7. What is your relationship to the child? ☐Mother ☐Father ☐Guardian
☐Other (specify) ___________________________________
8. Is there any additional information you would like the school to know about your
child? _____________________________________________________________________________________________
__________________________________________________ ______________________________ Signature of person filling out the form Date
Updated: October, 2017
This form should be completed once per student and kept in their cumulative file unless the form indicates they do not qualify for services. If they do qualify for services, a copy should be sent to your school’s ELL teacher of Bill Brulotte.

Twin Falls School District #411 2960F1 Computing Device and Network Acceptable Use Agreement
School district computing device and network users are expected to act in a responsible, ethical, and legal manner, in accordance with district policy and the laws of the State of Idaho and the United States. The computing devices and network are provided to further the district’s stated educational goals only, and they are to be used by authorized individuals only. Individuals using these systems are subject to having all activities monitored by IT or other security personnel. Anyone using these systems expressly consents to such monitoring. It is possible for all users of the Internet, including your child, to access information that is not intended for minors. Although the district has taken reasonable steps to ensure that the Internet connection is used only for purposes consistent with the curriculum and that inappropriate sites as defined by the Children’s Internet Protection Act are filtered, the district or school cannot entirely prevent the availability of inappropriate material on the Internet. Further, it is possible that a determined user may make use of computing device or network resources for inappropriate purposes. Deliberate misuse of the computing devices, the network, or the Internet may result in disciplinary action as outlined in the Computing Device and Network Acceptable Use Policy. Curriculum for students will include instruction on Internet safety topics, including appropriate online social interaction. I understand that my child is expected to use good judgment and follow the guidelines of the Computing Device and Network Acceptable Use Policy. With school administration and teacher approval, your child may be allowed to use, but will not be required to use, his or her own electronic devices during class time for educational purposes. The school district cannot be responsible for the content accessed via a student’s own voice, messaging, or data services. The district will not pay for or reimburse for any voice, messaging, or data charges incurred by a student’s use of his or her own device. The school district does not assume liability in the event of lost, stolen, or damaged devices. Please Check One
Yes, my child may use his or her own electronic devices at school.
No, my child may not use his or her own electronic devices at school. I have discussed the information contained in the Computing Device and Network Acceptable Use Policy with my child. Should my child breach the policy guidelines, I understand that my child may lose privileges relating to the use of computing devices and the Internet or be subject to other disciplinary action. I agree to indemnify and hold harmless the school district, the trustees, administrators, teachers and other staff against all claims, damages, losses, and costs, of whatever kind, that may result from my child’s use of his or her access to such networks or his or her violation of district policy. Further, I accept full responsibility for supervision of my child’s use of his or her access account(s) and/or use of district-owned devices, if and when such use is not in the school setting. I give my child permission to use a district provided account(s) to access the district’s computer network, the Internet, and Internet sites. _________________________________ _________________________________ Parent Name (please print) Student Name (please print) _________________________________ _________________________________ Parent Signature Student Signature _________________________________ _________________________________ Date Date
201 Main Avenue WestTwin Falls, Idaho 83301
Telephone: 208-733-6900Fax: 208-733-6987
2960F1-1 This form should be filled out when a student enrolls in a TFSD School and should be kept in the student cumulative file.

Twin Falls School District 2017-18
Notification of Rights under FERPA
The Family Educational Rights and Privacy Act (FERPA)
affords parents and students who are 18 years of age or older
("eligible students") certain rights with respect to the student's
education records. These rights are:
1. The right to inspect and review the student's education
records within 45 days after the day the school receives a
request for access.
Parents or eligible students should submit to the school
principal a written request that identifies the records they
wish to inspect. The school official will make
arrangements for access and notify the parent or eligible
student of the time and place where the records may be
inspected.
2. The right to request the amendment of the student’s
education records that the parent or eligible student
believes are inaccurate, misleading, or otherwise in
violation of the student’s privacy rights under FERPA.
Parents or eligible students who wish to ask the school to
amend a record should write to the school principal,
clearly identify the part of the record they want changed,
and specify why it should be changed. If the school
decides not to amend the record as requested by the parent
or eligible student, the school will notify the parent or
eligible student of the decision and of their right to a
hearing regarding the request for amendment. Additional
information regarding the hearing procedures will be
provided to the parent or eligible student when notified of
the right to a hearing.
3. The right to provide written consent before the school
discloses personally identifiable information (PII) from
the student's education records, except to the extent that
FERPA authorizes disclosure without consent.
One exception, which permits disclosure without consent,
is disclosure to school officials with legitimate
educational interests. A school official is a person
employed by the school as an administrator, supervisor,
instructor, or support staff member (including health or
medical staff and law enforcement unit personnel) or a
person serving on the school board. A school official also
may include a volunteer or contractor outside of the
school who performs an institutional service or function
for which the school would otherwise use its own
employees and who is under the direct control of the
school with respect to the use and maintenance of PII
from education records, such as an attorney, auditor,
medical consultant, or therapist; a parent or student
volunteering to serve on an official committee, such as a
disciplinary or grievance committee; or a parent, student,
or other volunteer assisting another school official in
performing his or her tasks. A school official has a
legitimate educational interest if the official needs to
review an education record in order to fulfill his or her
professional responsibility.
Upon request, the school discloses education records
without consent to officials of another school district in
which a student seeks or intends to enroll, or is already
enrolled if the disclosure is for purposes of the student’s
enrollment or transfer.
4. The right to file a complaint with the U.S. Department of
Education concerning alleged failures by the Twin Falls
School District to comply with the requirements of
FERPA. The name and address of the Office that
administers FERPA are:
Family Policy Compliance Office
U.S. Department of Education
400 Maryland Avenue, SW
Washington, DC 20202
FERPA Notice for Directory Information
The Family Educational Rights and Privacy Act (FERPA), a
Federal law, requires that the Twin Falls School District, with
certain exceptions, obtain your written consent prior to the
disclosure of personally identifiable information from your
child’s education records. However, the Twin Falls School
District may disclose appropriately designated “directory
information” without written consent, unless you have advised
the District to the contrary in accordance with District
procedures. The primary purpose of directory information is
to allow the Twin Falls School District to include this type of
information from your child’s education records in certain
school publications. Examples include:
A playbill, showing your student’s role in a drama
production;
The annual yearbook;
Honor roll or other recognition lists;
Graduation programs; and
Sports activity sheets, such as for wrestling, showing
weight and height of team members.
Directory information, which is information that is generally
not considered harmful or an invasion of privacy if released,
can also be disclosed to outside organizations without a
parent’s prior written consent. Outside organizations include,
but are not limited to, companies that manufacture class rings
or publish yearbooks. In addition, two federal laws require
local educational agencies (LEAs) receiving assistance under
the Elementary and Secondary Education Act of 1965 (ESEA)
to provide military recruiters, upon request, with the following
information – names, addresses and telephone listings – unless
parents have advised the LEA that they do not want their
student’s information disclosed without their prior written
consent.
If you do not wish to have your child’s directory information released, please indicate so on the TFSD Student Opt-Out Form, located on our website at www.tfsd.org. Please understand that signing this form

would exclude your child’s directory information from any documents that are typically made public or relating to school-related organizations and activities such as:
Yearbooks Alumni Directories Graduation Programs Honor Roll and other recognition lists Sports activity programs Theatrical programs District productions/publications Classroom or student pictures
If you do not want the Twin Falls School District to disclose
directory information from your child’s education records
without your prior written consent, you must complete the Opt
Out form by August 20, 2017 or two weeks from the date you
receive this notice. If you do not have access to the internet, please contact the Twin Falls School District Office at 733-6900 and forms can be mailed to you. Please submit Opt-Out Forms to:
Twin Falls School District
Attn: Eva Craner 201 Main Ave. W
Twin Falls, ID 83301
The Twin Falls School District has designated the following
information as directory information:
Student’s name
Address
Telephone listing
Electronic mail address (e-mail)
Photograph of the student used by the district for
recognition of student achievement and community
relations, including, but not limited to, publication in
the district’s or school’s newsletters, in the school
setting and on the district’s or school’s web site;
Major field of study
Date and place of birth
Participation in officially recognized activities and
sports
Weight and height of members of athletic team
Dates of attendance, degrees and awards received
Most recent previous school or school district
MEDIA RELEASE
Throughout the course of the school year, the media may be in our schools or at school sanctioned events to cover our activities. The majority of the media coverage featuring students is considered human interest stories that do not contain sensitive subject matter or are not controversial in nature. Often, reporters are present at our request to showcase our students and teachers engaged in exciting educational activities.
The Twin Falls School District includes in its classification of directory information student names and photographic images of students participating in regular classroom or school-authorized events. This simply means that the media may publish and/or broadcast the names and photographs of students participating in school-related activities without prior parental consent. If you do not wish to have your child featured in any form of media, please sign the media portion of the FERPA Opt-Out Form, and we will exclude them from any media photos or publications. If you have not completed an Opt-Out Form, your student will be allowed to participate in human interest stories. The TFSD Student Opt-Out Form is located on the TFSD website at www.tfsd.org under enrolling your student. In instances where the building administrator has a concern about maintaining student confidentiality or the sensitive nature of media related stories, parental permission will be sought prior to allowing the student to participate.
PPRA
PPRA affords parents and eligible students certain rights regarding the district's conduct of surveys, collection and use of information for marketing purposes, and certain physical exams. These include the right to inspect and consent or opt out of: 1. The administration of surveys that contain questions from one or more of eight protected areas:
Political affiliations; Mental and psychological problems potentially
embarrassing to the student and his/her family; Sex behavior and attitudes; Illegal, antisocial, self-incriminating and
demeaning behavior; Critical appraisals of other individuals with whom
respondents have close family relationships; Legally recognized privileged or analogous
relationships, such as those of lawyers, physicians and ministers;
Religious practices, affiliations or beliefs; or Income (other than that required by law to
determine eligibility for participation in a program or for receiving financial assistance under such program).
2. Activities involving the collection, disclosure, or use of personal information collected from students for the purpose of marketing. 3. Any non-emergency, invasive physical examination or screening.
If you have any questions regarding the information provided in this notice, please contact Eva
Craner at 733-6900.
Thank you!

Mid-Columbia Bus Company Twin Falls District School Bus Transportation Services
Complete if student is new to Twin Falls District or change of address or phone number
Student’s Name___________________________________________________ Grade__________
Address_________________________________________________________________________
Parent’s / Guardian’s Name___________________________________________________________
Home Phone #_____________________________ Cell Phone #_____________________________
Emergency Contact Name & Phone______________________________________________________
Email___________________________________________________________________________
School Attending__________________________________________________________________
________ New Student to Twin Falls School District ________ Information Change
Transportation Needed
________ Morning Only ________ Afternoon Only ________Both Ways
Additional Students at Listed Address (Full Legal Name)
1) Student Name _________________________ Grade _____ M / F
2) Student Name _________________________ Grade _____ M / F
3) Student Name _________________________ Grade _____ M / F
4) Student Name _________________________ Grade _____ M / F
5) Student Name _________________________ Grade _____ M / F
By signing below, I acknowledge that I have received The Safe Bus Riding Rules and Regulations. I agree to be responsible for following all the rules and expectations of the school and Mid-Columbia Bus Company. I understand the consequences for failure to follow the rules and regulations.
Student Signature _______________________________________ Date _____________
Parent Signature ________________________________________ Date _____________ Mid-Columbia Bus Company Revised 06/2017