new relationships for health plans: accountable systems of care 1 michigan association of health...
TRANSCRIPT

1
NEW RELATIONSHIPS FOR HEALTH PLANS: ACCOUNTABLE SYSTEMS OF CARE
Michigan Association of Health Plans2015 Summer Conference

Nuyen, Tomtishen and Aoun, P.C.
HAVEN’T WE SEEN THIS ALL BEFORE?
1990s
Predominant focus: lower costs
Success under risk contracts driven by risk selection
Health IT just starting
HMO focused with robust UR and benefit designs requiring gatekeepers
Commercial payor focused
Today
Focus on both costs and quality
Risk adjustment seeks to equalize the playing field
Greater investment in health IT spurred by federal $$$; data analytics
Programs can operate in PPO or traditional FFS products; new focus on evidence-based care
Medicare is “in the game” 2

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE ACOs Over 400 ACOs serving more than 7 million
Medicare beneficiaries Close to 20 in Michigan, including 1 Pioneer ACO
(DMC/Tenet) 3 received shared savings distributions with
respect to 2013 (collectively, $ 26.7M); 1 had a loss ($2.5M)
MedPAC analysis – Study of ACOs in 78 markets (1.7 million beneficiaries). ACOs performed comparable to Medicare FFS In high use areas, ACOs saved Medicare about 2%.
3

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE ACOs Traditional options
Track 1 – upside only Track 2 – upside and downside risk (up to 60% share of
savings) – only 5 ACOs chose this Track Pioneer – higher levels of upside and downside risk (60-
75%); prospective assignment – currently 19 remain in the program (initially 32)
New Options Track 3 (new) – higher levels of upside and downside risk
(up to 75% share of savings) Next Generation – higher levels of upside and downside
risk (80-100%) with improvements in benchmarks, attribution and beneficiary engagement; flexibility in payment arrangements
Investment Model - incentives to foster ACOs in rural areas, e.g., advance payment for infrastructure
4

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE P4P TRAIN Bundled Payments
Bronson, Borgess and DMC/Tenet in Phase 2 (risk bearing) Borgess and DMC (knee and hip replacement); Bronson (knee and hip replacement, neurosurgery
and cardiac) Numerous other Michigan hospitals (and physician
groups) are currently in Phase 1 (evaluation) Trinity Health Beaumont Health (Oakwood and Botsford) Marquette General Hospital Portage Health Lakeland Hospital
5

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE P4P TRAIN Bundled Payments
Comprehensive Joint Replacement Model (proposed rule) Knee and Hip Replacement Mandatory participation in 75 areas
Flint and Saginaw are designated Hospitals must assume risk for admission
and 90 days post-acute care
6

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE P4P TRAIN Hospital Value-Based Purchasing Measures performance across various
domains Outcomes (mortality, patient safety)
(30%) Patient Satisfaction (30%) Clinical Processes of Care (20%) Efficiency (20%)
FY 2015: 1.5% (by 2017, it will reach max of 2.0%) Multiplier effect (2.58 in FY 2015)
7
Nuyen, Tomtishen and Aoun, P.C.
MEDICARE P4P TRAIN Hospital Value-Based Purchasing Efficiency domain evaluates
Medicare Spending Per Beneficiary for admission and services rendered within 30 days following admission (even if such services are unrelated)
8

Nuyen, Tomtishen and Aoun, P.C.
MEDICARE P4P TRAIN Other Initiatives
Hospital and physician quality reporting Inpatient reporting to include episode
payment
Physician payment reform – Merit-based incentive payments (includes penalties) begins in 2019 Ability to opt out if participating in a
sufficient number of “alternative payment models”
9

Nuyen, Tomtishen and Aoun, P.C.
STATE INNOVATION MODEL & MEDICAID
Payment for Value Increasing number of Patient Centered
Medical Homes Establishment of Accountable Systems of
Care Initially shared savings (level 1), but
ultimately downside risk assumption (level 2) Community Health Innovation Regions –
multi-stakeholder involvement to improve health, cost and satisfaction
Medicaid re-bid
10

Welcome
Detroit Medical Center2015
11

Welcome
12
DMC By the Numbers
Detroit Medical Center is proud to be part of Tenet Healthcare Corporation, a national, diversified healthcare services company, with:
80 Hospitals, including DMC210 Outpatient Centers105,000 Employees
7 Hospitals and 2 Institutes51 Outpatient Facilities1,811 Licensed Beds3,000 Affiliated Physicians13,323 Employees
2014 Patient StatsDischarges
Adult/Child: 77,275Newborn: 5,456
Outpatient Visits: 1,100,383ER Visits: 354,073Surgeries:Inpatient: 20,572Outpatient: 36,224
7 Children’s Hospital of Michigan Outpatient Facilities
1 Huron Valley-Sinai HospitalOutpatient Facility
32 Rehabilitation Institute of Michigan Outpatient Facilities
9 Sinai-Grace HospitalOutpatient Facilities
2 Sinai-Grace Hospital and Harper University Hospital Professional Buildings
Children’s Hospital of MichiganDetroit Receiving Hospital and University Health CenterHarper University HospitalHeart HospitalHutzel Women’s HospitalRehabilitation Institute of Michigan

Welcome
13
LeapFrogDMC Harper/Hutzel
DMC Huron Valley-SinaiDMC Detroit Receiving
DMC Sinai-Grace

Welcome
14
DMC Detroit ReceivingDMC Sinai-Grace
MPRO's 2014 Governor's Awards of Excellence
Detroit Receiving Hospital Harper University Hospital/Hutzel Women's Sinai-Grace Hospital and Huron Valley-Sinai Hospital
Environmental and Excellence Achievements
Nation’s leading health care community supporting environmental stewardship working to improve patient safety and care through tools, best practices and knowledge sharing.

Welcome
15
DMC Awarded CMS National Health Care $10 Million Innovation Award
DMC among few to receive $10 million grant from Centers for Medicare and Medicaid Services to test new primary care model in Detroit
• DMC Chief Medical Officer Dr. Suzanne White is one of only 39 recipients of about 3,000 applicants across the United States. The grant will enable the DMC to test an innovative primary care and preventative health model that reaches patients who use some of Detroit’s busiest emergency departments.
• The project, entitled Gateway to Health: An Innovative Model for Primary Care Expansion in Detroit, will make patient-centered medical care immediately accessible to individuals without existing primary care physicians, arriving to four DMC emergency departments at DMC Harper University Hospital, DMC Detroit Receiving Hospital, DMC Sinai-Grace Hospital and DMC Children’s Hospital of Michigan.

Welcome
16
2014 Most Wired HospitalFor the eighth consecutive year, Detroit Medical Center has been named to the nation’s MOST WIRED list, according to the results of the 2014 Most Wired Survey and Benchmarking Study released in the July issue of Hospitals & Health Networks magazine, which has named the Most Wired hospitals and health systems since 1999.
The Most Wired Survey is conducted annually by Hospitals & Health Networks magazine. It focuses on how the nation’s hospitals use information technologies for quality, customer service, public health and safety, business processes and workforce issues.
DMC EMR and IT Awards

Welcome
17
“The focus of the Michigan Pioneer ACO is not on cutting required care but rather on improving care transitions and care coordination,” said DMC Chief Medical Officer Dr. Suzanne White. “The efforts of the Michigan Pioneer ACO will continue to focus on improving quality and outcomes, while reducing unnecessary costs.”
“The focus of the Michigan Pioneer ACO is not on cutting required care but rather on improving care transitions and care coordination,” said DMC Chief Medical Officer Dr. Suzanne White. “The efforts of the Michigan Pioneer ACO will continue to focus on improving quality and outcomes, while reducing unnecessary costs.”

Welcome
18
Payer Provider relationships• Guaranteed failure• Unbalanced deal• Lack of timely data• Too much faith on
abilities to manage everything
• Lack of focus and attention
• Lack of statistical validity
• Guaranteed success• Balanced and fair
agreement• Timely and accurate
data• Real involvement of
physicians• Using process
improvement techniques

Welcome
19
Recent Examples in the Market
• Getting the incentive deal in June – without data by doctor – “…well, that’s coming.”
• Not getting first of year data until May.• Plan authorizing an admit to “not upset the member”
over Med. Dir objections.• Call 24 HH agencies – none will take patient.• Payer and DME Co. arguing over payment for DME –
patient sits in hospital Fri-Mon.• DRG audit – request records – downgrade before getting
records.

Welcome
20
Questions
• How do we eliminate redundancy between plans and providers– auths, UM, etc.?
• How can collaboration happen on a higher level?
• When will there be national standards for health plans to adhere for provider service? See next slide – Trust?

Welcome
21
Trust Toward PayorsComposite Trust Measures*
• The average score for all payor was 51.8; the average change from 2014 was -0.7.• Cigna, Blue Cross / Blue Shield, and Aetna all were above-average performers.• Humana, Bluecard, Wellpoint / Anthem, and UnitedHealthcare were all below-average performers.• BCBS, Humana, and Bluecard improved on their scores from 2014; Cigna, Aetna, Anthem, and United all declined in trust from 2014. The largest decrease was by Anthem with a drop of nearly 4 points.
*Composite Trust Index Score values are calculated as an equally-weighted mean of all three individual Trust measures.

Welcome
22

23

24
Who Is MidMichigan?
Non-profit health system affiliated with the University of Michigan Health System
More than 5,000 employees and physicians
4 Hospitals 17 Locations with Medical
Offices 6 Health Parks 7 Urgent Cares 8 Continuing Care
Locations

25
Population Health InitiativesCurrent Strategies and Accomplishments• ConnectCare Self-funded PPO Product• Accountable Care Organization (ACO) • Medicare Shared Savings Program• Narrow Network Development• Merger and Acquisition Activity• Partnerships with Health Plans• Board Approved Population Health Strategy• State Innovation Model (SIM)• Patient-centered Medical Home / Neighborhood• Patient Registry / Health Information Exchange / Data Warehouse

26
Overarching Population Health Strategy
Enhance the patient experience to strengthen patient engagement and loyalty
Continue to develop value-based payment strategies with payors and increase covered lives
Collaborate and align efforts with physicians and community/state agencies to transform care in meaningful ways
Invest in tools and personnel to create a team-based care management approach and effectively coordinate patient care

27
Matching Services to Health Status
5%
15-35%
60-80%
High Risk
Dedicated, individualized care plan, avoid (re)admissions, care
coordination
High risk care management, navigators, care planning,
palliative care, behavioral health
Avoid duplication, overutilization & higher acuity
sites, enhance access & patient engagement
Moderate care management, patient portal, patient engagement & self
management
Patient engagement, self management; convenient, affordable, accessible care
Patient portal, telehealth & e-visits, retail clinics, hybrid/concierge model
Moderate Risk
Low Risk
Patient Needs Tailored Services
Con
sum
ptio
n o
f H
ealth
Car
e S
ervi
ces

28
Health Factors Affecting Health Outcomes1
Health Factors
Health Behaviors 30%
Tobacco use
Diet & Exercise
Alcohol use
Clinical Care 20%Access to care
Quality of care
Social & Economic Factors 40%
Education
Employment
Income
Family & Social Support
Community Safety
Physical Environment 10%
Environmental Quality
Built Environment
1http://www.countyhealthrankings.org/our-approach

Health Plan Barriers
Hindering Forward Progress
o Misaligned incentives• Less than 2% of revenue is from value based purchasing
arrangements• Significant majority of revenue continues to be fee-for-service
o Time gap between implementation and incentive realization• Benefits are being captured now, primarily benefiting health plans and
negatively impacting the potential for future rewards to providerso Focus on “rules” (technical denials) rather than rewarding overall
performance and positive trendso Lack of consistent guidelines, benchmarks and regulations across all
payors
29

Health Plan Barriers
Future Opportunities
o Identify and implement strategies to address the 80% of health factors that affect health outcomes
o Make room for and encourage provider self-management• Transition care management responsibilities along with the
delegated risk to decrease cost• Share savings with healthcare providers
o Reduce overhead costs (consistent with your expectations of healthcare providers)
30

©2014 Trinity Health. All Rights Reserved. 3131
Hospitals in 21 States85*
Home Health &
Hospice Agencies44
Continuing Care Facilities70
Employed Physicians
3,300
PACE Center Locations14
Affiliated Physicians
22,890
Other Continuing Care Facility
Employed Physicians
Affiliated Physicians
Hospital
Home Care Agency
PACE Center
Introduction to Trinity Health: Our 21-State Diversified Network
128 Long-term care, assisted, independent living and affordable housing communities

©2014 Trinity Health. All Rights Reserved. 32
Stein’s Law
32
“If something cannot go on forever it will stop”

©2014 Trinity Health - Livonia, MI 33
Accenture Research shows: By 2017, nearly 1 in
5 Americans will purchase benefits from a health
insurance exchange (30 mil in private exchange
and another 30 mil in public exchange)
33
RETIREES:
IBM moves 110,000 retirees to Towers Watson’s
Medicare exchange for 2014
PART-TIMERS:
Target discontinues coverage for
part-time employees and shifts them to
public exchanges (via a private model)
ACTIVE EMPLOYEES:Walgreens will offer its 160,000 employees subsidies to buy insurance on Aon Hewitt’s private exchange in 2014

©2014 Trinity Health. All Rights Reserved. 34
Transition from Fee For Service to Risk
34
• Quality Reporting• Gaps in Care• QI Program
• Hospitalist Program• SNFist Program• Discharge Program• Home Care
Program• Actuarial Services
• High Risk Clinic• Enrollment Clinic• Claims Payment• Network Mgmt• Customer Service
• Care Management
Pay for Performance
Gain Sharing/ACO Model
SymmetricRisk
HealthPlan
% Premium
Competencies
30%
Full RiskCapitation
• Quality Reporting• Gaps in Care• QI Program
• Quality Reporting• Gaps in Care• QI Program
• Hospitalist Program• SNFist Program• Discharge Program• Home Care
Program• Actuarial Services
• Care Management
• Quality Reporting• Gaps in Care• QI Program
• Care Management
• High Risk Clinic• Enrollment Clinic• Claims Payment• Network Mgmt• Customer Service
• Hospitalist Program• SNFist Program• Discharge Program• Home Care
Program• Actuarial Services
• Care Management
• Quality Reporting• Gaps in Care• QI Program
5%
50%90% 100%
Model
• Marketing and Sales• Licensing

©2014 Trinity Health. All Rights Reserved. 35
Insights that will drive strategy
35
• Lowest cost silver plans (top 3 to 5) players captured > 90% market share (out of pocket cost also, important)
Lowest cost premiums drive market share
• ~70%+ renewed with the same insurance company as the last year
Inertia is strong and barriers to switch are high
• Narrow network can be traded off with lower monthly $ premium.
• Broad physician network is more important than a broad hospital network
Network is important after cost
• Trust is important for consumers. New entrants/less familiar brand names would be less preferred
Trust in Insurance company
• Strategic growth dictates that we be precise in the discounts we accept in order to capture lives
Commercial-like rates
are necessary
1
2
3
4
5

©2014 Trinity Health. All Rights Reserved. 36
Trinity Health is investing in capabilities to deploy a proactive population health management model nationally
36
… which employs comprehensive medical management infrastructure programs…
‘Virtuous Cycle’ of
Improved care
… and yields superior outcomes
Designed to address patient needs at all points of care before and including the hospital
Improved accessImproved coordination and
ownership of careImproved disease stabilizationImproved patient and physician
satisfactionImproved quality and utilization
measurements
Hospitalist programHigh-risk clinicHome care programFacility case mgmt. Behavioral HealthDiabetes Disease mgmt.COPD complex care mgmt.CHF complex care mgmt.ESRD programUrgent care centersHealth educationPalliative care programHospice programChest pain care mgmt. program
©2014 Trinity Health. All Rights Reserved. 37
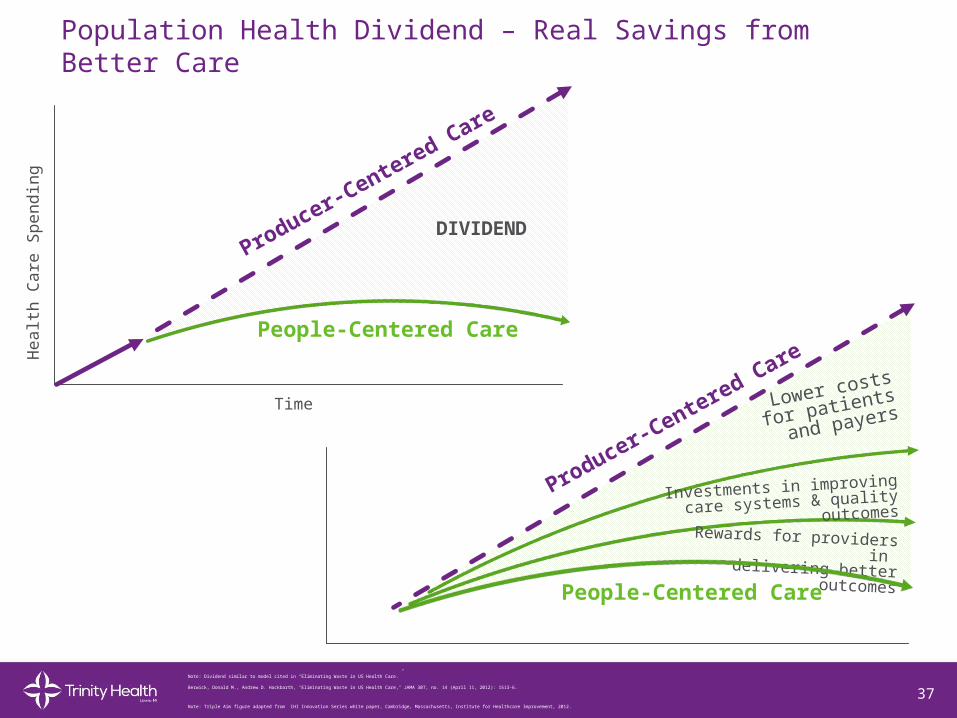
Population Health Dividend – Real Savings from Better Care
37
Producer-Centered Care
People-Centered Care
Time
He
alth
Ca
re S
pe
nd
ing
DIVIDEND
Note: Dividend similar to model cited in “Eliminating Waste in US Health Care.”
Berwick, Donald M., Andrew D. Hackbarth, "Eliminating Waste in US Health Care," JAMA 307, no. 14 (April 11, 2012): 1513-6.
Investments in improving
care systems & quality outcomes
Rewards for providers in delivering better outcomes
Producer-Centered Care
People-Centered Care
Lower costs for
patients and
payers
Note: Triple Aim figure adapted from IHI Innovation Series white paper, Cambridge, Massachusetts, Institute for Healthcare Improvement, 2012.

©2014 Trinity Health. All Rights Reserved. 38
2016 2018 2020
30% ? 50% ? 75%
75% of contracts to be value-based by 2020
Trinity Health Goal
©2015 Trinity Health - Livonia, MI 38