new jersey lead poisoning elimination plan jersey lead... · it sets forth a call to action and a...
TRANSCRIPT
Overview
Vision: To eliminate childhood lead poisoning in New Jersey.
Mission: To promote the health and well-being of people in New Jersey so that lead poisoning is eliminated*.
Purpose: To provide a blueprint to eliminate lead poisoning through the development of collaborative partnerships among public and private organizations that support and promote comprehensive community-based services.
Related Objectives
Healthy People 2010 Objectives:
Eliminate elevated blood lead levels in children.
Increase the proportion of persons living in pre-1950’s housing that has been tested for the presence of lead-based paint.
Healthy New Jersey 2010 Objectives:
Increase the percentage of children screened for lead poisoning by two years of age to 85.0 percent. (Baseline: FY 2000 33.0 percent)
Reduce the percentage of tested children whose initial blood lead level is >10 ug/dL by 50 percent. (Baseline: FY 2000 5.0 percent)
*”Eliminated” means no children with blood lead levels >10 ug/dL.
1

Introduction
The New Jersey Department of Health and Senior Services (DHSS) is the recipient of federal funding for childhood lead poisoning, through a Childhood Lead Poisoning Prevention Cooperative Agreement with the U.S. Centers for Disease Control and Prevention (CDC). In Healthy People 2010, the U.S. Department of Health and Human Services, of which CDC is a part, set forth a national goal of eliminating childhood lead poisoning by the year 2010. In 2003, CDC required all States receiving Childhood Lead Poisoning Prevention funding to develop a State Plan to Eliminate Childhood Lead Poisoning. This document has been developed in response to that mandate. But this Plan is more than just the fulfillment of a requirement for federal funding. It sets forth a call to action and a road map for achieving a very significant public health milestone. And the process of developing this Plan has promoted cooperative working relationships between multiple State and local, public and private agencies that will be vital to the achievement of this ambitious goal.
The State of New Jersey and the DHSS have a long history of responding to lead poisoning in children. The Department’s Laboratory has been testing children’s blood for lead since 1956. In 1958, Jersey City was the first community in the State to launch a screening and follow-up program after three children died from lead poisoning within two days. Newark, Paterson, Camden and Trenton also initiated lead poisoning programs during this period. In order to coordinate childhood lead poisoning prevention (CLPP) activities throughout the State, the Department established the Accident Prevention and Poison Control Program in 1967. In 1971, the federal Lead Based Paint Poison Prevention Act made funds directly available to high-risk cities to establish CLPP programs. Ten New Jersey cities received grants from CDC during the period 1971-1982. When the Maternal and Child Health Block Grant was created in 1981, the DHSS devoted a significant amount of its allocation to continuing support of these CLPP programs. Since the direct CDC CLPP grants were re-established in 1991, DHSS has received funding and been a partner with CDC in the national campaign to reduce and eliminate lead poisoning in children.
New Jersey’s efforts to address childhood lead poisoning have been facilitated by strong, often landmark, legislation. In 1971, New Jersey adopted one of the first State laws prohibiting the use of lead paint on toys, furniture and dwellings, and empowering public health agencies to order the removal of lead hazards. This was seven years before the national ban on the sale of lead paint issued by the Consumer Product Safety Commission. In subsequent years, additional State laws and regulations have been adopted addressing lead poisoning in children. In 1977, the DHSS adopted regulations incorporating childhood lead poisoning prevention as a core activity under Minimum Standards of Performance for all local health departments in the State. In 1986, a law was passed requiring the DHSS to establish a program for screening children at high risk of lead poisoning through local health departments and other agencies. This was superseded in 1996 by a law requiring health care providers to screen all children in their care under six years of age. A companion law required health care insurers to cover lead screening. A law adopted in 1993 requires that anyone who performs lead paint inspections or abatement to be certified by the State and to follow State-specified work practices.
2
The most recent legislation addressing childhood lead poisoning in New Jersey is Public Law 2003, Chapter 311, the Lead Hazard Control Assistance Act. This law passed the Legislature on January 12, 2004 and was signed by Governor James E. McGreevey on January 20, 2004. The purpose of the Act is to provide a comprehensive program to identify lead hazards in residential housing and also to identify housing which is safe from exposure to lead hazards in order to eradicate the major source of lead exposure to our State’s children. The comprehensive program will emphasize methods to safeguard children residing in rental housing and require the State to track the progress of making all of New Jersey’s rental housing stock more lead safe. It also created the Lead Hazard Control Assistance Fund, with a dedicated funding mechanism, to assist property owners with the cost of removal of lead paint and/or making their properties lead safe. This law promotes primary prevention of childhood lead poisoning and provides the resources needed to make it possible.
The most significant provisions of the Act are: • requires the New Jersey Department of Community Affairs (DCA) to promulgate
regulations requiring all multiple-unit dwellings with three or more units be maintained in such a manner as to be free of lead-based paint hazards and provide standards and specifications for such maintenance;
• establishes the assessment of a $20 per unit fee to inspect multi-family housing for lead-based paint hazards;
• requires the DCA to create and maintain a registry of residential housing that provides information on the lead status of each housing unit;
• establishes the Lead Hazard Control Assistance Fund; • sets aside $.50 from the sales tax on each can of paint sold in New Jersey and places it in
the Lead Hazard Control Assistance Fund; • establishes the Emergency Lead Poisoning Relocation Fund; • removes the payment limitations set forth in the Relocation Assistance Act for the
purposes of relocating a lead poisoned child; • establishes a training requirement for persons for hire who seek to engage in lead safe
maintenance work or lead hazard control work; and requires the DCA to establish guidelines for interim control methods.
These laws provide a strong basis for action by State government, as well as by local health departments and housing agencies. Given the extent of lead poisoning in New Jersey, no one agency can successfully deal with all the issues involved in addressing this problem. A combination of the State laws cited above and Executive Branch directives has distributed the responsibility for addressing lead poisoning among a number of agencies of New Jersey State government. The agencies directly involved in addressing lead poisoning are:
• Department of Health and Senior Services - screening, surveillance, oversight of local health departments follow-up of children with elevated blood lead, occupational lead poisoning, regulation of lead inspectors and abatement workers, and licensure of laboratories, lead curricula development and certification of training facilities;
• Department of Community Affairs - all housing issues including the administration and enforcement of uniform construction codes and property maintenance codes, the
3
administration of federal and state funded housing acquisition and renovation initiatives including lead hazard control grants and full implementation of the Lead Safe Housing Rule, and the administration of other housing assistance programs such as rental assistance;
• Department of Human Services - Medicaid, licensed child care centers, and foster children;
• Department of Environmental Protection - environmental hazards in soil, air, and water; and
• Department of Banking and Insurance - health insurance and property liability insurance.
Communication and cooperation among these agencies is facilitated through the Interagency Task Force on the Prevention of Lead Poisoning. The Task Force includes representatives of the State agencies involved in addressing lead poisoning. It also includes representation from professional, medical, environmental and community-based organizations. The Task Force meets bi-monthly. The Chair is the Director of the Division of Codes and Standards in the Department of Community Affairs. A list of the agencies and organizations participating in the Task Force is attached (Appendix 1).
The Task Force was created in 1988. It is a committee of the Governor’s Council on the Prevention of Mental Retardation and Developmental Disabilities, and its Chair sits on the Council. This gives the Task Force access to the highest levels of State government.
The Task Force has previously produced documents to guide statewide planning and policy, including a “Lead Poisoning Prevention Action Agenda” in 1989, and “Recommendations for the Primary Prevention of Lead Poisoning” in August 1995. In 1996, in response to the report of HUD’s Lead-Based Paint Hazard Reduction and Financing Task Force, the Task Force created a Title X Committee, which included representatives of rental property owners, real estate agents, the insurance industry, and attorneys. The committee’s recommendations were incorporated into amendments to the State multiple-unit dwelling code that were adopted by the Department of Community Affairs. In 2003, the Task Force undertook a review of the progress towards achievement of the 1995 Recommendations. This resulted in the preparation and approval of a Strategic Plan for the Prevention of Lead Poisoning in New Jersey. The Task Force’s Strategic Plan became the basis for the development of this Elimination Plan.
4
Why is Lead Poisoning in Children a Priority for New Jersey?
Lead is a heavy metal that has been widely used in industrial processes and consumer products. When absorbed into the human body, lead affects the blood, kidneys and nervous system. Lead’s effects on the nervous system are particularly serious and can cause learning disabilities, hyperactivity, decreased hearing, mental retardation and possible death. Lead is particularly hazardous to children between six months and six years of age because their neurological system and organs are still developing. Children who have suffered from the adverse effects of lead exposure for an extended period of time are frequently in need of special health and educational services in order to assist them to develop to their potential as productive members of society. Failure to identify and assist these children can produce an economic and social impact, not only on the individual for the rest of their lives, but also on society as a whole. Research indicates that lead poisoning in childhood can result in school failure, violence and criminal behavior, reduced earning potential and health problems later in life.
As the most densely populated state of the Union, and among those states with the oldest housing and an extensive industrial heritage, New Jersey contains a substantial amount of lead, subjecting its residents to the dangers of lead poisoning. New Jersey’s demographics are consistent with the known high risk factors for childhood lead poisoning. Although a relatively small state in size, with a population of nearly 8.5 million people New Jersey is the most densely populated state in the nation, with 1,134 people per square mile. Thus 94.3 % of New Jersey’s population lives within urbanized areas. The least “urbanized” county still has 46.9 % of the population living in an urbanized area. Of the 135,549 families living in poverty, there were 48,730 families with children under 5 years old.
The primary method for lead to enter the body is through the ingestion of lead containing substances. Lead was removed from gasoline in the United States in the early 1980’s. This action is credited with reducing the level of lead in the air, and thereby, the amount of lead inhaled by children. However, significant amounts of lead remain in the environment, where it poses a threat to children. Some common lead containing substances that are ingested or inhaled by children include: lead-based paint; dust and soil in which children play; tap water; food stored in lead soldered cans or improperly glazed pottery; and traditional folk remedies and cosmetics containing lead.
Due to the fact that lead-based paint and other lead-containing substances are present throughout the environment in New Jersey, all children in the State are at risk. Some children, however, are at particularly high risk due to exposure to high dose sources of lead in their immediate environment. For example, the rates of lead poisoning remain high among low-income and/or minority children and children in urban areas. These potential high dose sources include:
- leaded paint that is peeling, chipped, or otherwise in a deteriorated condition; - lead-contaminated dust created during removal or disturbance of leaded paint in the
process of home renovation; and - lead-contaminated dust brought into the home by adults who work in an occupation that
involves lead or materials containing lead, or who engage in a hobby where lead is used.
5

Today, the primary lead hazard to children comes from lead-based paint. In recognition of the danger that lead-based paint presents to children; such paint was banned for residential use in New Jersey in 1971, and nationwide in 1978. These bans have effectively reduced the risk of lead exposure for children who live in houses built after 1978, but any house built before 1978 still may contain leaded paint. Housing built prior to 1950 presents the greatest risk due to the high percentage by volume of lead. Statewide, there are nearly one million housing units built before 1950, which is 30.2% of all housing units in the State (Appendix 3). Every county in the State has more than 9,000 housing units built before 1950.
6
The Extent of Childhood Lead Poisoning in New Jersey
United States Centers for Disease Control and Prevention (CDC) guidelines state that a blood lead test of 10 micrograms per deciliter (ug/dL) or greater should be considered elevated. In addition, the CDC guidelines state that a confirmed blood lead test result of 20 ug/dL or greater should trigger public health follow-up, including an environmental investigation to determine the source of the lead, and case management assistance to the family.
While 97% of the children tested in New Jersey in State Fiscal Year (SFY) 2003 had blood lead levels below the CDC threshold of 10 ug/dL, there were 5,230 children with a blood lead test result above this level, which was 3% of all children tested. This included 832 children who had at least one test result of 20 ug/dL or greater (Appendix 4, Table 1).
While every county in New Jersey had children with elevated blood test results in SFY 2003, the number and percentage of children with elevated blood lead were highest in the urban counties of Camden, Essex, Hudson, Mercer, Passaic and Union. The numbers were highest in Essex, where there were 1,879 children with blood lead levels > 10 ug/dL, seven percent of all Essex County children tested. This was 36% of all children in New Jersey with elevated test results. The percentage of children with elevated blood lead in Essex County is more than double the statewide percentage, and significantly higher than in any other county. However, elevated test results were not limited to urban areas. High percentages of children with elevated test results were also found in rural Cumberland and Salem counties in South Jersey. This documents that childhood lead poisoning continues to be a statewide problem.
As expected, the older urban centers, which have the largest portion of high risk housing units, also have the highest levels of lead poisoning. Data for the largest municipalities (population > 35,000) are presented in Appendix 4, Table 2. The municipality with the highest percentage of children with elevated blood lead test results was East Orange, with 9.9%, followed closely by Irvington at 9.4%. Other municipalities with percentages of children with elevated blood lead significantly higher than the statewide percentage of 3% included Atlantic City (3.9%), Camden (3.9%), Montclair (4.3%), New Brunswick (4.3%), Newark (8.1%), Passaic (3.8%), Paterson (6.5%), Plainfield (4.4%) and Trenton (8.1%). Of the 60 municipalities for which the data were analyzed, there were only four (Berkeley Township, Bridgewater, Manchester Township, and Mount Laurel) where no children with elevated blood lead were reported.
New Jersey has already made significant progress towards eliminating childhood lead poisoning. In the past decade (1994-2003), the number of children reported to the DHSS with blood lead levels > 20 ug/dL has declined from 4,757 in SFY 1994 to 832 in SFY 2003, an 82.5% decrease (Appendix 4, Figure 1). Since the reporting of all blood levels began in July 1999, the number of children reported with blood lead levels > 10 ug/dL has declined from 6,847 in SFY 2000 to 5,230 in SFY 2003, a 23.6% decrease. While progress is being made, even one child with lead poisoning is one child too many. Therefore it is our State’s goal to reduce the number of children with lead poisoning, at or above 10 ug/dL, to zero by 2010.
7
Process for Development of the Elimination Plan
The Department of Health and Senior Services (DHSS) has been an active partner in the Interagency Task Force on the Prevention of Lead Poisoning since its inception. Through the Task Force, DHSS staff has worked with their colleagues of other State agencies and representatives of statewide and community-based organizations to develop and implement policies and initiatives to reduce childhood lead poisoning in New Jersey. As described previously, the Task Force has produced a series of documents guiding State policy and actions on childhood lead poisoning, culminating in the Strategic Plan for the Prevention of Lead Poisoning in New Jersey in 2003.
CDC’s mandate to develop a State plan for the elimination of childhood lead poisoning included a requirement to create an advisory committee, including representatives of all the key constituencies required to implement the Plan. Given its history and track record, the DHSS decided to turn to the Task Force to assist it in developing this plan, rather than create a separate advisory committee. All of the key constituencies were already involved with the Task Force. The 2003 Strategic Plan provided a baseline and framework for development of the New Jersey Elimination Plan. Most importantly, as a long-established and on-going group, the Task Force provides a structure for coordinating collaboration not only in writing the Plan, but in its implementation and evaluation as well.
At a retreat held in November 2003, vision, mission and purpose statements were generated. At the end of the retreat, working groups were established for the four key areas of the Plan:
• Screening and follow-up of children with elevated blood lead • Public and Professional Education • Lead-Safe Housing • Other Environmental Lead Sources
A fifth working group on Surveillance was developed later. A call went out through the Task Force’s email list to any other members who were unable to attend the retreat, but who wanted to participate in the plan development through joining a working group. Each group chose leadership and an appropriate name for itself. Appendix 2 lists the working groups and their members.
Between December 2003 and June 2004, each working group met to develop objectives and strategies in their area. DHSS Childhood Lead Poisoning Prevention staff was assigned to each working group to provide guidance and technical assistance. Starting with its March 2004 meeting, the evolving drafts were shared with the entire Task Force for review and comment. The final Plan was approved by the Task Force at its meeting on September 2, 2004. The Plan was then submitted to the Commissioner of Health and Senior Services for formal approval. Each of the participating agencies and organizations was requested to obtain endorsement from its senior leadership. Letters from those agencies and organizations formally endorsing the Plan are attached (Appendix 5).
8
Elimination Plan
9
Section 1: Surveillance
Surveillance is the acquisition of data on the incidence and prevalence of lead poisoning
Goals: • Maintain a Surveillance System for New Jersey capable of tracking all blood lead tests and
follow-up of children with elevated blood lead. • Monitor progress in preventing childhood lead poisoning and in reducing exposure to lead
hazards in the environment. • Ensure that public resources devoted to childhood lead poisoning prevention are used
effectively and efficiently by local health departments and community partners.
Current Status: New Jersey has had a system for reporting children with elevated blood lead, and tracking of environmental investigations, since the mid-1980’s. This system was significantly upgraded in 1993 with the development of a PC-based environmental investigation tracking system. Public Law 1995, Chapter 328 authorized the Department of Health and Senior Services (DHSS) to require the reporting of all blood lead tests performed on children. In response, the DHSS developed specifications for a comprehensive Childhood Lead Poisoning Prevention Surveillance System (CLPPSS) to process these reports. This system has been partially, but not fully, implemented as described below. At present, several data systems have been assembled in order to provide the data, reports and analyses necessary to perform childhood lead poisoning prevention activities. DHSS is currently investigating the acquisition of an integrated data system for childhood lead poisoning activities to replace our current systems.
The Childhood Lead Poisoning Prevention Surveillance System (CLPPSS) provides the base for New Jersey’s surveillance system for childhood lead poisoning. This system is built on a database which contains all blood lead test results reported since July 1999, all elevated blood lead tests reported since 1975, and all environmental actions reported by local health departments since 1985. The system is capable of processing both electronically and hard copy reported results, printing notices to local health departments for children with elevated blood lead test results residing in their jurisdiction, printing standard reports, and performing a variety of data analyses.
The State lead screening law requires clinical laboratories to report all blood lead test results to the DHSS. About 90% of the blood lead test results are reported electronically. Blood lead test results are loaded into CLPPSS, where the results are initially evaluated for completeness of information, with adult results forwarded to the Occupation Health Program. The child and address information is either matched to an existing record or creates a new record. The final step standardizes addresses to the US Postal Service standard and adds geographic information, e.g., county and municipality. Hard copy, non-elevated blood lead test results are entered into a temporary database before being batch processed by CLPPSS. All blood lead test results undergo routine processing to extract reports where the blood lead level was > 20 ug/dL. The elevated results currently are processed by a stand-alone, SAS-based, system, and then processed to determine whether a notice needs to be sent to the local health
10
department. Multi-part forms are printed for those children for whom an environmental investigation may be required.
The information in the databases is constantly updated, based on information from laboratories and local health departments. Data tables containing information on local health departments, clinical testing laboratories, and medical providers are periodically updated as new information becomes available. CLPPSS has several built-in standard reports for monitoring the activities of local health departments, while ad hoc reporting is performed using customized SAS programs. CLPPSS is linked with the New Jersey State Immunization Information System (NJSIIS), through which lead screening results are uploaded to the NJSIIS. This enables participating medical providers to use NJSIIS to track both immunization and lead screening in children.
The law requiring screening of all of New Jersey’s children for lead poisoning also mandates that an annual report on childhood lead poisoning be produced. DHSS wrote its first report for FY 1998. The reports describe testing results, environmental activities performed by local health departments, actions taken by agencies to reduce childhood lead poisoning, and planned activities for the upcoming years. FY 2000 was the first report based upon universal reporting of all blood lead test results, which began in July 1999. The FY 2002, report presented data at the municipal level for the first time. These reports are sent to the Governor’s Office, State Legislature, and local health departments. They also are available to the general public. The reports from SFY 2000 forward are available on the Department’s web site.
DHSS collaborates with the Division of Medical Assistance and Health Services in the Department of Human Services in matching of Medicaid enrollment records with records of children tested for lead poisoning. Since SFY 2000, matches were performed for the state fiscal year and the federal fiscal year. CLPPSS is also being used to measure the effectiveness of the pilot projects to increase the screening of Medicaid-enrolled children. In addition, DHSS is working with the Division of Youth and Family Services (DYFS), New Jersey’s child protection agency, to identify children in their foster care program who have been tested for lead poisoning.
A variety of ad hoc analyses are done to assist public and private agencies in grant applications, provide information on smaller geographic regions than in the annual reports, assist public and allied health students in class projects, and provide information to consultants hired by public and private entities. The data have been used to create mailing lists that were used to recruit participates into studies that were designed to reduce environmental exposure to lead.
CLPPSS was being developed for DHSS by the New Jersey Office of Information Technology (OIT). However, the system is not currently fully operational as designed. Currently, CLPPSS is used for receipt, geocoding, and storage of electronic laboratory reports. All of the other key functions of the surveillance system - loading of laboratory records, environmental reporting and tracking, and report creation, are still being done manually through SAS programs written by DHSS staff. After working with OIT for seven years to resolve these problems, the DHSS is currently investigating other alternatives, including the potential for purchasing a working surveillance system already operational in other states.
11

Objective 1: By June 2005, obtain and install software capable of providing a fully integrated surveillance system.
Strategies: • Research childhood lead poisoning surveillance systems that have been developed for other
States and are available for purchase, to determine if any of them meet, or could be modified to meet, New Jersey requirements.
• Select and contract with a data system vendor to provide New Jersey with a surveillance system.
• Install, test, and implement the new surveillance system. • Train appropriate DHSS and local health department staff in system operations, including
confidentiality/privacy guidelines.
12

Objective 2: By December 2005, provide local health departments with access to the surveillance system.
Strategies: • The specifications for purchase or development of the surveillance database will require that
the system be capable of tracking environmental activities and case management, including home visits.
• Create jurisdiction-specific standard reports and maps. • Establish access and security protocols that will allow local health departments to access the
records of children in their jurisdiction, while limiting access to other records in the surveillance database.
• Provide training and technical assistance to local health department staff that will have access to records of children in their jurisdiction.
• Modify DHSS protocols for notification of local health departments of children with elevated blood lead. Instead of printing and mailing hard copy forms, email notices will be sent to designated local health department staff, alerting them to new cases in their jurisdiction.
• In the last phase, local health departments will be able to manage their childhood lead poisoning cases electronically. Designated staff will be able to update the electronic records in CLPPSS for any environmental activities that they have completed, create secondary environmental investigations, update child demographics, and medical case management activities.
13

Objective 3: By June 2005, improve quality and increase electronic reporting of blood lead test results to 95%.
Strategies: • Work with DHSS Clinical Laboratory Improvement Services (CLIS) in DHSS to identify all
clinical laboratories licensed to perform lead testing on blood samples. • Identify clinical laboratories who still report via hard copy reports. • Work with laboratory directors to encourage electronic reporting of test results. • Work with clinical laboratory directors and medical providers to improve the quality of the
reported data.
14
Objective 4. By October of each year, complete the Annual Report on Childhood Lead Poisoning in New Jersey for the preceding State Fiscal Year (July 1 - June 30).
Strategies: • Complete processing of blood lead test results for the Fiscal Year • Complete entry of all reports from local health departments of environmental inspections and
abatements completed during the Fiscal Year. • Utilize the surveillance database to generate reports on screening, children with elevated
blood lead, and environmental actions. • Send Report to Commissioner for transmittal to Governor and Legislature. • Distribute report to press, partner organizations, and public. • Post report on DHSS website. • Present Annual Report findings to the Interagency Task Force on Prevention of Lead
Poisoning; obtain feedback from Task Force members on usefulness of Report and recommendations for improvements in future years.
15

Objective 5: On an on-going basis, provide and compare surveillance system data with data from other databases that have information related to children at risk of lead poisoning
Strategies: • Quarterly provide the New Jersey State Immunization Information System with lead data.
When matches are identified, blood lead test result data will be imported into the immunization registry, and birth certificate number will be exported to CLPPSS.
• Match blood lead test reports with Medicaid enrollment database on a quarterly and annual basis, including both the State Fiscal and Federal Fiscal years.
• When requested by DYFS, match blood lead test reports with the foster care enrollment database.
• Utilize information from the electronic birth certificate database. Birth certificate numbers exported from the immunization registry will be used to obtain information from the electronic birth certificate data, which will be used to clean records in the surveillance system.
16

Objective 6: On an on-going basis, provide DHSS childhood lead poisoning prevention staff, and partners, with data to evaluate the effectiveness of activities to reduce/eliminate lead poisoning in New Jersey.
Strategies: • Address data will be regularly cleaned and processed to have a standardized format with geo-
coding for county, municipality, FIPS codes, zip +4 codes, census tracts and blocks, longitude and latitude.
• Screening prevalence and incidence rates will be calculated for a variety of geographic boundaries: state, county, municipality, zip code, and local health department jurisdiction. For the urban areas, it will also calculate rates by census tract. The information will be presented in tabular form and visually as maps.
• Records will be linked with U.S. Census data to provide analyses based upon parameters contained within the Census.
• These analyses will provide a profile of who is currently affected by lead poisoning and where they live. This information will be used, along with Census data, to assess screening penetration throughout the State. Particular emphasis will be placed upon those geographic areas where there are high numbers of children with elevated blood lead and the presence of known risk factors, (e.g., percentage of pre-1950 housing units).
• Collaborate with the OIT Geographic Information Systems (GIS) unit to develop maps that visually highlight areas of concern.
• The results will be compared to the data collected in previous periods to measure the effect of activities. Surveillance data will be used to develop program evaluation plans before implementing new activities within communities.
• Continue to provide each local health department with a quarterly report on all open cases of children reported with elevated blood lead.
• Provide each local health department with a quarterly summary report of follow-up blood lead tests of all children in case management for elevated blood lead.
• Provide each local health department with access to data files of all blood lead tests performed on children resident in their jurisdiction on a quarterly basis.
17

Objective 7: By June 2007, provide public access to user-created summary reports.
Strategies: • Develop software to enable the general public to do queries against a copy of the data base
that is missing individual identifier information using predefined reports to produce summary tables or maps.
18

Section 2: Identification and follow-up of children with elevated blood lead.
Children already exposed to lead hazards need to be identified through screening, and referred for follow-up services - environmental investigation and case management assistance to their families,
Goals: • Increase the percentage of children screened for lead poisoning by two years of age to
85.0 percent. (Baseline: FY2003, 40.4 percent)
• Reduce the number of children whose blood lead level is >10 ug/dL to zero. (Baseline: FY 2003 - 5,230 children)
• All children identified with elevated blood lead will receive follow-up services in accordance with the CDC case management guidelines.
Current Status:
Identification: New Jersey State law (N.J.S.A. 26:2-137.4) requires all physicians, nurse practitioners, and health care facilities to perform lead screening on each patient under six years of age to whom they provide health care services. The law also requires clinical laboratories licensed by the DHSS to report the results of all blood lead tests. The DHSS adopted regulations (N.J.A.C. 8:51A) implementing this law in 1997. These regulations, which follow federal Centers for Disease Control and Prevention (CDC) guidelines, require health care providers to do a blood lead test on all one and two-year old children. Older children, up until six years of age, are to be tested only if they have never been previously tested, or are assessed to be at high risk. While it is recommended that children be tested at or about their first and second birthdays, the regulations specify that children be tested between nine and 18 months of age, and again between 18 and 26 months of age. In addition, children determined to be a high risk should be tested starting at six months of age.
During FY 2003, laboratories reported 183,379 blood lead tests to the DHSS. Based on these reports, 172,932 individual children, ages birth through 16 years of age, were identified as having been tested for lead poisoning. This represents a 25% increase over the number of children tested during FY 2000, when reporting of all tests was initiated. However, the total number of children tested in FY 2003 increased only by 1,220 (0.7%) over the number of children tested in FY 2002 (Appendix 4, Table 3).
All children in New Jersey who were between six months and two and one-half years of age during FY 2003 should have received a blood lead test. There were 90,112 children in this age range with reported blood lead tests that year. This number represents 40.4% of the estimated 222,837 children in this age group, based on the 2000 U.S. Census. Table 4 shows the number and percentage of children in this age group who were tested, by county. The percentage of children tested ranges from a high of 48% in Passaic County to a low of 19% in Burlington County.
19

The DHSS has records on 76,494 children who were born between July 1, 2000 and June 30, 2001 for whom at least one blood lead test has been reported in their lifetime. This number is 68.6% of the estimated number of two-year-old children in New Jersey, based on the 2000 Census. Likewise, there were 54,417 children who were one-year old as of June 30, 2003, who had at least one blood lead test reported, which is 48.9% of the estimated number of one-year-olds in New Jersey. And 84,321 children who were three years of age as of that date, 74.1% of the estimated number of three-year-olds, have also been tested (Table 5).
Follow-up: U.S. Centers for Disease Control and Prevention (CDC) guidelines state that a blood lead test of 10 micrograms per deciliter (ug/dL) or greater should be considered elevated. In addition, the CDC guidelines state that a confirmed blood lead test result of 20 ug/dL or greater should trigger public health follow-up, including an environmental investigation to determine the source of the lead, and case management assistance to the family. Following these guidelines, blood lead test reports to the DHSS are analyzed to see if the result is above either of these thresholds. If the result is 20 ug/dL or greater, the local health department covering the community where the child resides is notified.
State law and DHSS regulations require the local health department to conduct an environmental investigation of each of these cases and to provide case management for the families of these children. New Jersey law (N.J.S.A. 24:14A) requires local boards of health to investigate all reported cases of lead poisoning within their jurisdiction and to order the abatement of all lead paint hazards identified in the course of the investigation. A home visit by a public health nurse is conducted to educate the parents about lead poisoning and the steps that they can take to protect their child. The nurse provides on-going case management services to assist the family in getting follow-up testing and medical treatment. DHS/DMAHS Medicaid HMOs provide case management services for lead burdened children with blood lead levels of 10 ug/dL or greater. DHS/DMAHS conducts case tracking for fee-for-service lead burdened children with blood lead levels of 10 ug/dL or greater.
The DHSS maintains a system for notifying each local health department of all children with elevated blood lead reported in its jurisdiction. During FY 2003, 76 of the 112 local health departments in the State (68%) received at least one notice of a child with elevated blood lead residing within its jurisdiction. However, 71% of reported cases of children with reported elevated blood lead test results resided within the jurisdictions of only 13 local health departments (Table 6).
Looking at all cases reported to local health departments over the past six years, more than 90% of investigations had been completed, and 77% of properties with lead hazards had been abated, by the end of FY 2003 (Table 7). This illustrates that it can take several years to complete abatement of a property where lead hazards have been identified.
20
Objective 1: Identify barriers to lead screening services.
Strategies:
Continue the Lead Screening Improvement Pilot Projects. These projects are a collaborative effort among Department of Human Services (DHS)/Division of Medical Assistance and Health Services (DMAHS), DHSS, American Civil Liberties Union Foundation (ACLU), Association for Children of New Jersey (ACNJ), New Jersey Chapter of the American Academy of Pediatrics (NJ/AAP), local health departments, University of Medicine and Dentistry of New Jersey (UMDNJ), regional Maternal and Child Health consortia and the HMOs under contract with DHS to provide health services to children enrolled in Medicaid. The purpose of the pilot projects is to increase lead screening percentages among Medicaid-enrolled children in the target cities. This lead screening pilot was implemented in the cities of Camden and Irvington from August 2002 through December 2003. Starting in July 2004, the projects were expanded to include the cities of Paterson, Jersey City and Bridgeton/Millville. Barriers that have been identified and are being addressed during the pilot projects include: • Physician reluctance to provide in-office blood lead testing. • Child care providers not consistent in collecting/keeping records of blood lead test
results. • Health insurer policies requiring physicians to refer clients to blood collection stations
operated by the major clinical laboratories. These laboratory operations can have limited operating hours, and/or are located in areas that are not convenient for families to get to, some are minimally staffed resulting in long waiting times.
• Lack of parental awareness of importance of blood lead testing in young children.
Continue to assess individual medical practice screening rates. To date a limited amount of assessment has been done of lead screening rates in individual medical practices. On behalf of the DHS/DMAHS, the Peer Review Organization of New Jersey (PRO/NJ) conducted audits of large pediatric practices in several communities to determine how many of the children in their care who were enrolled in Medicaid had received a blood lead test. DHS/DMAHS staff also audited the records of all of New Jersey’s Federally Qualified Health Centers (FQHCs). Medical records of Medicaid-enrolled children between six and 26 months of age were reviewed. The FQHC audits will be continued on an annual basis. Individual practice audits will be conducted as resources and opportunity permit.
The Physicians Lead Advisory Committee (PLAC) will continue to serve as an advisory group to the DHSS on policy and actions to address childhood lead poisoning. The PLAC consists of physicians with expertise and/or interest in childhood lead poisoning. It includes representatives from the New Jersey Chapter of the American Academy of Pediatrics, the University of Medicine and Dentistry of New Jersey, and at least one physician from each of the Maternal and Child Health Consortia regions. The PLAC meets on a formal basis at least once per year. A primary barrier noted by members of the PLAC in recent meetings is that many physicians no longer collect blood samples in their offices for any type of test. Several factors and trends in medical care have combined to discourage the collection of blood samples.
21
These include:
• New federal rules regarding blood-borne pathogens and disposal of medical waste have increased the cost of blood sample collection.
• A law requiring federal (as well as State) licensing of all clinical laboratories has resulted in many physician practices discontinuing in-office laboratories for simple analyses.
• The evolution of insurance payments from fee-for-service to capitation means that many insurers no longer reimburse physicians for the cost of blood sample collection. However, the Medicaid HMO contract provides financial incentives to providers who perform in-office screenings.
The Interagency Task Force for the Prevention of Lead Poisoning (Task Force) will establish a statewide Lead Screening Advisory Group whose members include but are not limited to representatives from DHS/DMAHS, DHSS, local health departments, DCA, at least one DCA HUD grantee, Medicaid HMOs, commercial health insurance carriers, and the New Jersey Physician Lead Advisory Committee. The role of the advisory group will be to: • Identify lead screening services stakeholders including but not limited to parents, health
care providers and State agencies with regulatory authority. • Develop and conduct a comprehensive assessment of barriers and successes with
representatives of each stakeholder group. • Develop a universal statement listing perceived and real barriers to performing lead
screenings. • Identify national and statewide best practices that address barriers to obtaining lead
screening services.
22

Objective 2: Develop interventions to address and eliminate barriers.
Strategies:
DHS/DMAHS Lead Screening Improvement Pilot Projects will continue to be implemented in Camden and Irvington, and will be expanded to include Jersey City, Paterson and Bridgeton/Millville in 2004/2005. Lessons learned will be applied to other high-risk municipalities. All of the pilot project cities will continue to incorporate the following strategies: • Medicaid HMO Medical Directors will write letters to health care providers, reviewing
federal and State screening requirements and encouraging the performance of blood lead screenings in the physician’s office by using either the filter paper, venous, or capillary methods for collection of blood lead samples. As needed, the Medicaid HMO Medical Directors will meet with providers who are non-compliant with lead screening requirements. Medicaid HMO representatives will continue to visit medical practices to reinforce written correspondence from the Medical Directors.
• Promote the use of filter paper as a means of collecting blood lead samples in the physician’s office. All Medicaid HMOs will contract with Medtox laboratories to analyze filter paper samples.
• Additional reimbursement for all blood lead tests done in the physicians’ office. • Child Care Health Consultants associated with the Unified Child Care Agencies and
Abbott District nurse consultants will continue to conduct lead education training programs for child care centers directors, Abbott district family workers, family child care providers and Head Start staff. Child care center directors will continue to distribute lead education packets to the parents/guardians of child enrollees and will inquire and document the lead screening status of age-appropriate enrollees. Documentation will be kept with immunization records to facilitate audits.
• Local Health Officers will communicate with health care providers and child care directors/providers encouraging lead screenings for children under six years of age. Local health department personnel who perform immunization audits will review enrollee records for documentation of lead screening status.
• Continue to sponsor various community health events to provide the general public with lead poisoning prevention information.
DHSS and DHS/DMAHS will adopt, on a statewide basis, those strategies shown to be effective in the pilot projects. Based on the results so far in Camden and Irvington, the following strategies have already been implemented statewide: • Promotion of the use of filter paper as a means of collecting blood lead samples in the
physicians office. All Medicaid-contracted HMOs are required to contract with Medtox laboratories for the analysis of filter paper samples. DHSS has sent a letter to all physicians doing lead screening, promoting the use of filter paper for in-office sample collection.
• Enhanced reimbursement for blood lead tests done in the physicians’ office.
Explore the feasibility of performing lead screenings at WIC (Women, Infants and Children Supplemental Feeding) program sites. • The Newark Department of Health and Human Services CLPP Program is currently
23

collaborating with the Newark WIC program to provide on-site lead testing at the primary WIC sites in Newark. This pilot project is funded by CDC through the DHSS. A phlebotomist schedules site visits with the WIC Program Coordinator and conducts screenings on a monthly basis. Children will be screened during the parent/guardian certification and/or re-certification visits to the WIC program. The Lead Care portable lead analyzer is utilized to conduct initial capillary tests on children, with results available to parents within three minutes. If necessary, a venous confirmatory test is conducted at the time of the visit. Depending on the child’s health insurance status either the physician is contacted stating that his/her patient is being seen at WIC that day and needs to be screened or if the child is found to be uninsured he or she will be enrolled in the health department’s pediatric clinic. A NJ FamilyCare application will be completed for children found to be uninsured.
• If the pilot project proves successful, it will be expanded to additional WIC sites in Newark as resources permit.
• UMDNJ in Newark will also conduct a pilot project of lead screening at its WIC sites, using a different model. With the support of private funding, UMDNJ will hire a phlebotomist for the WIC site. This person will draw venous samples which will be sent to the hospital laboratory for analysis.
• DHSS and its partners will evaluate these pilot projects, as well as examine similar pilots at WIC sites in other States. If any of these prove to be cost-effective in increasing the percentage of lead screening among children served by WIC, DHSS will attempt to identify resources to expand these services to other WIC sites in the State.
The DHSS will develop and implement a targeted screening plan. The plan will identify those communities with the highest number of children at risk with particular emphasis on communities whose percentage of children screened is lower than the statewide average. It will delineate additional activities to reach the parents of these children. The Physician Lead Advisory Committee provided medical consultation to the DHSS in the development of the plan and will continue to provide guidance during its implementation and evaluation. • For FY 2005, 16 communities have been identified as potential targets: Atlantic City,
Bridgeton, Camden, East Orange, Elizabeth, Irvington, Jersey City, Montclair, Newark, New Brunswick, Orange, Passaic, Paterson, Perth Amboy, Plainfield and Trenton.
• DHSS will use its blood lead reporting database to develop GIS maps of each target community to assist in identifying those areas with the highest rates that should be particularly targeted for screening and educational outreach.
• DHSS will reach out to safety net providers in these communities, including the Federally Qualified Health Centers (FQHC), hospital outpatient clinics, and local health departments, to develop systems for screening and referral of children who may have “fallen through the cracks” because they do not have health insurance and/or a medical home. DHSS will begin this initiative in September 2004 with a pilot project in the City of Camden through a collaboration with the CAMCare FQHC.
• DHSS will seek resources to purchase, or to assist community providers in the purchase, of LeadCare portable lead analyzers to facilitate walk-in and community-based outreach screening. DHSS staff will develop and disseminate model protocols and forms for the use of these analyzers and for reporting of results to primary care providers and to the DHSS surveillance system.
24

The DHSS partnered with the New Jersey Chapter of the American Academy of Pediatrics (AAP/NJ) in the development and implementation of a tool kit for physicians and their staffs entitled Educating Physicians in Their Communities (EPIC). The purpose of the tool kit, developed in 2004, is to encourage physician practices that serve young children to conduct on-site blood lead testing. The program includes a Powerpoint presentation with speaker notes that is presented by a physician and nurse/health educator team. The practice is given an accompanying binder which includes federal and state resources, AAP policy statements, summaries of State laws and regulations, and suggested anticipatory guidance for each well child visit starting at the first visit with a family, at the time of birth. Results of the pilot which was conducted in 11 physicians offices in Trenton, shows that many of the physicians were fairly knowledgeable of their responsibility to assess and screen children. However, office staff required basic lead education to better serve their patients and their families. DHSS and AAP/NJ will continue to seek funding to reproduce and distribute the curricula statewide and to provide consultation to trainers in implementing and evaluating the program.
Target child care facilities as places to promote lead screening. Healthy Child Care New Jersey, a collaboration among DHSS, DHS and AAP/NJ, will develop and implement programs targeted to child care providers and their parent clients. Strategies include: • Development of a training curriculum for child care providers. • Training and utilization of the Child Care Health Consultation Coordinators. These
Coordinators are full-time nurses employed by each of the Unified Child Care Agencies (UCCAs). There is a UCCA in every county in the State. The Coordinators provide technical assistance and training on health-related matters to child care providers and staff.
• Training local health department child health nurses to be local Child Care Health Consultants.
• Development of a Uniform Child Health Record (UCHR) for use to keep health records for all children in child care. Blood lead test results are included on the UCHR. Effective in October 2003, DHS rules will require all licensed child care facilities to complete a UCHR on all enrolled children.
• DHS/DMAHS has contracted with Scholastic Publications to develop materials on lead poisoning and screening for child care staff and parents. These will be distributed in the Fall of 2004.
• DHSS and DHS/DMAHS will seek to encourage collaborations between child care facilities and medical providers to assist in screening the children enrolled in child care. A major component of the Camden pilot project will be a collaboration among CAMCare and Camden Head Start.
DHSS will mandate that those local health departments that are eligible to receive State Public Health Priority Funding use a portion of these funds to support activities to promote and/or provide lead screening. These funds can also be used to include assessment of lead screening records as part of the immunization audits of licensed child care facilities. To facilitate these audits, the DHSS has modified the standard immunization record form to include a line to record lead test results.
25
Objective 3: Identify barriers to efficient and effective follow-up and develop interventions that promote the implementation of the CDC guidelines.
Strategies:
DHSS will continue to maintain a system to notify local health departments of children with EBL, tracking the number of environmental investigations conducted and abatement of environmental hazards by local health departments, and tracking home visits and case management by public health nurses.
DHSS will continually review Chapter XIII of the New Jersey State Sanitary Code, and adopt changes as warranted, to assure that environmental investigations in New Jersey are conducted in accordance with CDC and HUD guidelines. Chapter XIII contains the rules that govern local health department activities when children with elevated blood lead levels are identified.
DHSS will hire a nurse consultant by October 2004 to coordinate case management activities of local health departments. The nurse consultant will create a working group, including local health department nurse case managers, to develop a State case management plan for children with elevated blood lead that is consistent with the CDC guidelines “Managing Elevated Blood Lead Levels Among Young Children” by June 2005.
The DHSS will provide grants to support lead inspections and case management in those jurisdictions with the highest numbers of children with elevated blood lead. DHSS has budgeted $2,613,884 for grants to 15 local health departments in FY2005. The DHSS will also continue to support all local health departments by providing training, technical assistance and consultation to inspectors and case managers.
DHSS will mandate that those local health departments that are eligible to receive State Public Health Priority Funding use a portion of these funds to support activities related to childhood lead poisoning, including environmental investigations and case management.
DHS/DMAHS will continue to monitor and audit HMO lead case management. DMAHS will also continue to directly monitor and track children with elevated blood lead in Medicaid fee-for-service and the follow-up care that is provided by the primary care provider.
The DHSS and DHS/DMAHS will continue to collaborate with the DHS Division of Youth and Family Services (DYFS) to monitor and track children in foster care who are found to have elevated blood lead levels.
DHSS will seek to establish follow-up services for children with elevated blood lead between 10 and 19 ug/dL
• Newark CLPP program will continue to receive test results of children tested at Newark DHHS child health clinic and WIC sites and identify children with blood lead levels between 10-19 ug/dL. As workload permits, Newark DHHS Lead Inspectors will conduct visual risk assessment of the residences and will test paint and dust if potential hazards are found.
26
Inspectors will issue a report to the property owner and parents, with recommendations for hazard reduction and interim controls and will conduct follow-up visits within 3-6 months after initial assessment.
• DHSS staff will research model programs in other areas of the country that provide education, home visits and follow-up services for families of children with blood leads 10-19 ug/dL (ex. Philadelphia “Lead Safe Babies” project).
• DHSS will seek to obtain resources to implement follow-up services for these children, based on the results of the Newark pilot project and its research into best practices.
• DHSS will modify its surveillance and reporting system to notify local health departments of children with blood lead test results > 10 ug/dL.
• DHSS will encourage local health departments to follow-up children with blood lead test results 10-19 ug/dL as local resources permit.
The Lead Screening Advisory Group will develop and conduct a comprehensive assessment of barriers and successes in regard to performing effective and efficient case management that follows CDC guidelines and New Jersey Chapter XIII.
27

Section 3: Education
Education is the first step to promote awareness, increase knowledge and provide the skills necessary to prevent lead poisoning.
Goal:
• Mobilize communities to implement lead poisoning prevention strategies.
Current Status:
The Interagency Task Force has an ad-hoc Education subcommittee whose primary purpose is to coordinate the annual Childhood Lead Poisoning Prevention Week observance. This group expanded its purpose and membership during the Elimination Plan process and became the Education working group. Many of the members of the working group expressed their enthusiasm to continue their collaborative efforts from the planning phase into the implementation phase. This working group will form the basis for the Childhood Lead Poisoning Prevention Education steering committee.
To successfully reach the mission of eliminating childhood lead poisoning in New Jersey, all municipalities, regardless of risk level, must be equipped with the knowledge, skills, and opportunities necessary to create self-sustaining lead-safe environments. Involvement must come from the bottom up starting with grassroots community group members who educate their neighbors to top down with officials who enact local policy and enforce State regulations. Through coordination efforts on the municipal and regional level, supported by State agencies, funding and services can be leveraged so that real change can occur.
Educational efforts to date have been disjointed creating a lack of communication among stakeholders, assumptions of need of the target audiences, and limited access to New Jersey’s diverse ethnic and cultural populations. Regional Coalitions were established in January 2003 to coordinate educational initiatives on a regional level. High-risk municipalities have begun to develop capacity to address childhood lead poisoning through the establishment of pilot projects and targeted funding to address lead hazards in housing units.
28
Objective 1: Increase professional and public awareness, knowledge and skills about lead poisoning.
Strategies:
Establish a statewide Childhood Lead Poisoning Prevention Education steering committee whose members include but are not limited to Federal agencies, State departments and Regional Coalition leadership to determine critical capacity building components. The Childhood Lead Poisoning Prevention Education steering committee will: • perform a biannual needs assessment of educational materials. • identify and secure resources based upon needs assessment results. • create, as needed, educational resources based upon needs assessment. • evaluate audiovisual educational materials, including but not limited to videos, pamphlets
and curriculum. • create a clearinghouse of educational resources. • develop a system to identify and provide on an ongoing basis *resources that meet the
current educational needs of New Jersey’s ethnically, culturally and linguistically diverse populations. *Resources=audio, visual, web-based, speakers bureau, technical assistance contacts
• identify and promote web-based educational materials. The Task Force will establish a web page with information on childhood lead poisoning in New Jersey and links to other State and national websites with additional information and resources.
• Annually recommend updates to ongoing trainings, sponsored by Task Force representatives, based upon best practices.
• Identify and promote continuing education events, trainings and networking opportunities.
• Biannually, hold a statewide conference with built-in networking opportunities.
Continue to provide continuing education, training and networking opportunities for professionals who are to include but are not limited to child care providers, real estate personnel, school educators, health and human service staff, and community-based organizations.
Continue to seek air time for public service announcements developed by State agencies.
Dust testing kits will be distributed to pregnant women living in pre-1978 housing in communities with high levels of lead poisoning. This initiative, proposed by Governor McGreevey in January 2004, will be funded by a one million dollar State appropriation to the DHSS for SFY 2005. The funds will be granted to a non-profit agency, Family Health Initiatives (FHI). FHI will purchase approximately 40,000 kits for distribution to pregnant women through health centers and private providers in these communities. Distribution and provider training will be carried out in collaboration with the regional Maternal and Child Health Consortia. The kits will include educational messages about prevention of lead hazards in housing and instructions for follow-up evaluations of positive results.
29
DHSS will: • Provide training for local health department staff engaged in childhood lead poisoning
prevention and follow-up work through the Child Health Regional Network. • Train local health department staff in proper lead abatement, inspection and risk
assessment practices. • Identify resources to implement a statewide public awareness campaign as prepared by
DHSS CLPP staff. The proposal includes using a mix of media outlets including cable TV, billboards, radio, movie theatres and New Jersey Transit buses and rail.
• Promote and distribute the four-minute lead poisoning prevention video, using a rap music format, produced by New Jersey Network (NJN) with DHSS support. The video was developed as an educational tool targeted to parents with children of lead screening age. The final product was premiered during Childhood Lead Poisoning Prevention Week in October 2002. To date over seven hundred copies of the video have been distributed to agencies who serve families with young children. NJN nominated the video and it was the recipient of a CINE Golden Eagle award in the category Professional Non-Telecast, Science and Technology. A 30 second version of the video has also been produced for use as a PSA.
• Develop a Spanish language video, based upon the success of the Prevent Lead Poisoning rap video, to increase the Latino community’s awareness of lead poisoning. The video will feature Latin music and will involve representatives of the various Hispanic communities in New Brunswick. The video will be distributed through the Regional Coalitions.
• Coordinate the marketing, duplication and distribution of the video “Keep Your House Lead Free” that was developed by the DHSS CLPP in 2004. Duplicate and distribute 400 videos through the Regional Coalitions.
• Partner with EPA Office Region II to support the printing and distribution of the pamphlet Protect Your Family From Lead in Your Home in Russian and Arabic.
• Educate physicians and other health care providers using the EPIC curriculum and to distribute information about the lead screening regulations.
• Coordinate and promote the statewide Childhood Lead Poisoning Prevention (CLPP) Week observance.
DHS/DMAHS will: • Continue to update as needed a site on their Department’s web page discussing EPSDT
and lead poisoning prevention. • Continue to distribute Medicaid Provider Newsletters that will annually contain State and
federal lead screening requirements. • Continue to distribute their health promotion and lead poisoning prevention flyers. The
flyers have been made available to a variety of venues that serve Medicaid enrollees. • Continue to send outreach letters to the caregivers/guardians of Medicaid fee-for-service
children who did not receive an age appropriate lead screening. • Continue to distribute a multi-language stuffer encouraging age appropriate lead
screenings to Medicaid beneficiaries. Text is in English, Spanish, French, Chinese, Korean, Polish, Arabic and Portuguese.
• Continue to provide stakeholders with an overview of EPSDT services including lead poisoning prevention and screening requirements.
30

• Require Medicaid HMOs to continue to provide educational materials and sponsor educational events to their members.
DHS/DMAHS and DHS/DYFS will continue to collaborate in efforts to increase the awareness of EPSDT, lead poisoning prevention and screening requirements for the children receiving services through DYFS. Initiatives include: in-services for designated DYFS staff; inclusion of DHS/DMAHS Health Promotion and Lead Poisoning Prevention flyers in foster parent packets and in foster child placement packets.
DHS/Office for Prevention of Mental Retardation and Developmental Disabilities (OPMRDD) will: • Continue to serve as the sponsor of the New Jersey Interagency Task Force on the
Prevention of Lead Poisoning as a committee of the Governor’s Council on Prevention of Mental Retardation and Developmental Disabilities.
• Continue to implement the Get the Lead Out prevention education program targeting child care center staff, parents and community groups.
• Continue to implement the Lead Exploratorium project, a mobile lead education exhibit equipped with interactive teaching stations designed for preschool aged children.
• Continue to implement the Train-the-Trainer program targeting professional staff who provide lead poisoning prevention education to individuals and community groups.
• Continue to issue requests for proposals for programs that address prevention of developmental disabilities. Lead poisoning prevention projects are a primary focus. Three such projects are funded among the SFY 2005 grants.
• Continue to provide educational materials and technical assistance on childhood lead poisoning prevention.
DCA will: • Continue to provide educational materials and make appearances at community events to
promote lead-safe work practices and regulatory compliance through their Lead-Based Paint Abatement Program.
• Continue to fund lead-safe work practices trainings for rehabilitation contractors, property owners, weatherization technicians and contractors.
• Continue to provide trainings to promote compliance with HUD’s Lead-Safe Housing Rule for State-certified lead evaluation and abatement contractors, property owners, builders and community organizations.
• Develop a multimedia statewide marketing campaign to promote the lead hazard control assistance and emergency relocation programs
• Pay for training opportunities in lead related disciplines through the LHCA fund. Training opportunities will be limited to those which conform to state and/or federal standards on course curriculum. Until the curriculum is developed for lead-safe work practices, DCA will limit funding to courses approved by either the U.S. Environmental Protection Agency or the U.S. Department of Housing and Urban Development.
New Jersey Citizen Policy and Education Fund will continue to conduct at least four training programs per year in the following areas: lead-safe work practices, reducing lead hazards and conducting accurate dust wipe samplings.
31

Objective 2: Promote and support locally-initiated education and primary prevention through the leadership of the Regional Coalitions.
Strategies:
Continue to support the formation of regional childhood lead poisoning prevention coalitions whose purpose is to develop local lead poisoning education programs. Regional coalitions, covering the whole State, where formed in January 2003 through the solicitation of competitive proposals. The following have received funding: • Northern New Jersey Maternal and Child Health Consortium (Bergen and Passaic
counties); • Monmouth County Health Department (Monmouth and Ocean counties); • Camden County Health Department (for a seven county South Jersey region); and • Gateway Northwest Maternal and Child Health Network (on behalf of itself, Central New
Jersey Maternal and Child Health Consortium, and Hudson Perinatal Consortium covering a ten county region in northern and central New Jersey).
The Regional Coalitions will continue to identify their needs and resources and secure non-financial and financial commitments from their member agencies to include but not limited to, staff time, purchase of educational supplies, and meeting space as a means to sustain regional coalitions outreach and education efforts.
Establish quarterly meetings for Regional Coalition leadership to discuss coordination and leveraging of services throughout state.
Continue to identify State department resources and referral resources to include but not limited to, personnel who can provide grant writing assistance to the Regional Coalition leadership for the purpose of matching funds, partnering State and local agencies, development and distribution of educational materials and media, and coordination and leveraging of services.
Establish by October 2004 a group comprised of State department leadership and Regional Coalition leadership to meet quarterly to enhance state and local partnering regarding funding.
The Regional Coalitions will continue to assist the Department of Community Affairs in lead poisoning prevention initiatives through the Lead Interventions for Children-At-Risk (LICAR) program, and distribute educational materials promoting lead-safe work practices during remodeling and rehabilitation projects.
DCA will work with the Regional Coalitions, to facilitate the consolidation of efforts in obtaining funding for educational grants from HUD’s Office of Healthy Homes and Lead Hazard Control. Among other things, these grants require an outreach component that refers property owners to lead hazard control resources.
The Interagency Task Force Lead Coalition Review Panel will conduct annual performance reviews to evaluate the effectiveness of the Regional Coalitions.
32

Objective 3: Establish key capacity building components in high-risk municipalities.
Strategies:
Continue support of the Newark Partnership for Lead Safe Children. Major projects planned by the Partnership include: • Continued use of the “Leadie Eddie” van to provide lead poisoning prevention education
programs at child care centers and at faith-based and other community-based locations. • Assistance to property owners to make their rental properties lead safe. • Development of a DWI Court Model for landlords who have been remanded to Lead
Court. • Training programs to Newark ClearCorps members and Programs for Parents (Essex
County) staff on reducing lead hazards and how to correctly conduct dust wipe sampling. • Train the Trainer educational programs on lead poisoning prevention for the staff of
community-based organizations; and • Educational programs for property owners about lead poisoning prevention and the
availability of public and private lead abatement funds.
Continue the DHS/DMAHS Lead Screening Improvement Pilot Projects in Camden and Irvington and expand to other high-risk cities starting in 2004 - Jersey City, Paterson and Bridgeton/Millville. The pilot project cities will continue to sponsor community health events to provide the general public with lead poisoning prevention information.
The DCA Lead Interventions for Children-At-Risk Program (LICAR) will continue to provide funding to support primary prevention efforts in the targeted municipalities of Camden, East Orange, Elizabeth, Irvington, Jersey City, New Brunswick, Orange Township, Passaic, Paterson, Perth Amboy, Plainfield, and Trenton.
Continue to support the Irvington Lead Coalition, which was formed in 2003 as a result of the Lead Screening Improvement Pilot Projects. The Coalition includes representatives of local and State government and community organizations. Participants include the Irvington Department of Health and Department of Community Development, DHSS, DHS, DCA, UMDNJ, and the Gateway Northwest MCH Network. In addition to continuing efforts to increase screening, the Coalition is developing initiatives to educate the public and to reduce lead hazards in the community. Through UMDNJ, private funding has been secured for these initiatives.
Continue to support the New Brunswick Lead Coalition, formed in 2002, which is a component of the Healthier New Brunswick 2010 Initiative, sponsored by New Brunswick Tomorrow. The mission of Healthier New Brunswick 2010 is to build a healthier community to insure the health of New Brunswick’s children and families. The Coalition will continue to educate parents about the importance of lead screening for all children, and preventive measures that can be taken if a child is at risk of exposure to lead. The Middlesex County Health Department provides overall coordination of the activities.
33

The Leaguers Head Start Program located in Newark will continue to partner with CLEARCorps to conduct dust wipe sampling in the homes of Head Start children in Newark with blood lead levels between 5-14 ug/dL.
Programs for Parents (Essex County) will continue to conduct dust wipe sampling in Family Child Care Homes.
The Childhood Lead Poisoning Prevention Education steering committee will biannually assess State, County and Municipality assets and progress in building capacity.
34
Section 4: Housing and Child Occupied Facilities
Lead-Safe Maintenance, Rehabilitation and Abatement are critical components in creating and maintaining lead-safe buildings.
Goals:
• Increase the number of housing units in New Jersey that are lead-free or lead-safe.
• Promote and fund lead-safe maintenance, rehabilitation work practices and abatement services.
Current Status:
Lead Hazard Control Assistance Act (LHCA) The Lead Hazard Control Assistance Act (LHCA) provides a comprehensive program to identify lead hazards in residential housing and identify housing which is safe from exposure to lead hazards. The comprehensive program will emphasize methods to safeguard children residing in rental housing and require the State to track the progress of making all of New Jersey’s rental housing stock more lead safe. Specifically the Act: • establishes the Lead Hazard Control Assistance Fund • establishes the Emergency Lead Poisoning Relocation Fund • requires the creation and maintenance of a registry of residential housing that provides
information on the lead status of each housing unit. • establishes the assessment of a $20 per unit fee to inspect multi-family housing for lead-
based paint hazards • requires local boards of health to report violations and enforcement procedures under
Chapter XIII to DCA when relocation assistance is required. • removes the payment limitations set forth in the Relocation Assistance Act for the
purposes of relocating a lead poisoned child. • establishes a training requirement for persons for hire who seek to engage in lead safe
maintenance work or lead hazard control work. • requires the establishment of guidelines for interim control methods. • requires that DCA issue and promulgate regulations that assure that any hotel or multiple
dwelling be maintained in such a manner as to be free of lead-based paint hazards and that the DCA provide standards and specifications for such maintenance.
• requires that the DCA report to the legislature their progress in implementing the legislation.
A proposed rule was published in the NJ Register on June 6, 2004 that would implement those provisions of the “Lead Hazard Control Assistance Act,” P.L. 2003, c.311 (N.J.S.A. 52:27D-437.1 et seq.) under which the Department of Community Affairs is authorized to provide deferred payment loans with forgiveness and deferred payment loans without forgiveness for lead hazard control work and relocation of families with young children who are at risk of exposure to lead hazards. It is estimated that the rules will be adopted in October 2004. Program
35

activities will immediately begin upon adoption of rules and will serve as an ongoing source of funds dedicated to this purpose.
The LHCA Act created the Lead Hazard Control Assistance Fund and the Emergency Lead Poisoning Relocation Fund. The purpose of the Lead Hazard Control Assistance Fund (LHCA Fund) is to provide financial assistance in the form of grants and loans to eligible property owners. The LHCA Fund shall: • identify lead-based paint hazards in residential housing; • eradicate lead hazards to the greatest extent feasible through the performance of lead
hazard control work (interim controls or lead abatement) and the correction of conditions creating lead-based paint hazards;
• relocate tenant households when they are living in conditions which pose an immediate risk of continuing exposure to lead hazards for any of their children;
• identify housing in which people are safe from ongoing exposure to lead-based paint hazards and create a registry of that housing;
• increase public awareness to the dangers of lead-based paint; and • provide educational opportunities such as training contractors in how they should
perform maintenance, repair and rehabilitation of residential buildings in a manner that minimizes human exposure to lead-based paint and dust.
The purpose of the Emergency Lead Poisoning Relocation Fund (ELPR Fund) is to provide financial assistance in the form of grants and loans to relocate a child and his/her family when that child has tested positive for lead poisoning and that child is removed from his dwelling unit in connection with an order to abate a lead-based paint hazard. The relocation may be temporary or permanent and the child and family must be relocated to a lead safe housing unit. ELPR Fund shall: • Pay for the actual moving and related expenses that the IEH Unit determines are
reasonable and necessary to relocate an eligible household to a comparable dwelling unit that is lead safe. This may include:
o transportation of personal property within 50 miles o packing, crating, uncrating and unpacking of the personal property o disconnecting, dismantling, removing, reassembling, and reinstalling relocated
household appliances, and other person property o utility hookups, including reinstallation of telephone and cable television service o credit checks o storage of the personal property for a period not to exceed 12 months o insurance for the replacement value of the personal property in connection with
the move and necessary storage or if insurance is not reasonable in cost, self insurance that shall reimburse the household for the replacement of lost, stolen or damaged property when that damage occurred during the move or during the storage period through no fault of the household.
o increase in rent and utilities for a period not to exceed 12 months.
• Pay for costs of temporary relocation. This may include: o cost of hotel/motel o out of pocket expense
36
o transportation o storage of personal belongings
Lead Interventions for Children-At-Risk Program (LICAR) DCA administers the LICAR Program with $3 million in funding from the US HUD Office of Healthy Homes and Lead Hazard Control and $2.2 million in funding from DCA’s allocation of federal HOME Investment Partnership Program funds.
LICAR is an umbrella or grouping of initiatives designed to meet DCA’s goal of eliminating childhood lead poisoning in New Jersey by 2010. The LICAR Program strategy, through partnerships with municipalities, local boards of health and community based organizations, focuses resources from multiple sources. These financial resources are utilized to fund efforts which can be divided into two basic strategies or approaches: primary prevention efforts which include any effort to prevent lead-based paint poisoning; and responsive efforts to abate lead hazards in residences where children have been lead poisoned. The LICAR goal is to abate lead based paint hazards in 200 units occupied by lead-poisoned children and perform interim controls in 147 units by March 2007.
The LICAR Program targets its limited resources to municipalities with the greatest need and the fewest resources. The DHSS reports on childhood lead poisoning across the State on an annual basis. Through evaluation of the information provided in their Annual Report, it was determined that approximately 80% of childhood lead poisonings in New Jersey occur within 15 municipalities. They are: Bridgeton, Camden, East Orange, Elizabeth, Irvington, Jersey City, New Brunswick, Newark, Orange Township, Passaic, Paterson, Perth Amboy, Plainfield, Trenton, and Vineland. These municipalities were then prioritized based upon their existing resources directed to lead-based paint hazard reduction. At this time, the LICAR Program is awarded to the following municipalities: Camden, East Orange, Elizabeth, Irvington, Jersey City, New Brunswick, Orange Township, Passaic, Paterson, and Perth Amboy.
There are currently two Program Tracks offered under the LICAR umbrella which are based upon funding source. The first funding source is a DCA set aside of a portion of its HOME Investment Partnership Program (HOME) allocation to fund lead abatements. The second funding source is a grant from the HUD Office of Healthy Homes and Lead Hazard Control (OHHLHC). To differentiate between these two funding sources we refer to them as HOME LICAR and HUD LICAR Program Tracks. The HOME LICAR Program is available to the 10 municipalities identified in Targeted Municipal Partners. The HUD LICAR Program track is funded through a competitive grant application process. The DCA partnered with 7 of the eligible municipalities in the latest OHHLHC application and was awarded $3 million.
Child Care All child care facilities in New Jersey that serve five or more children are required to be licensed by the Department of Human Services. In 2000, the Bureau of Licensing adopted amendments to the child care licensing regulations to strengthen the provisions related to lead paint. The rules provide that all licensed centers located in buildings constructed before 1978 must have an inspection to determine if lead paint is present. If so, the facility must have a hazard assessment done and develop a plan for removing the paint or maintaining it in a lead safe condition.
37
Objective 1: Increase the number of lead-free and lead-safe buildings.
Strategies:
The LHCA Act will provide an ongoing resource for property owners to control lead-based paint hazards in residential dwellings. DCA will administer the LHCA Fund and the ELPR Fund. The SFY 2005 State Budget has an appropriation of $7 million for start-up of the LHCA Fund. In subsequent years, the fund will receive a minimum of $7 million and a maximum of $14 million from the sales tax set-aside on sales of paint. Rules implementing the Fund were proposed on June 7, 2004. DCA will adopt these rules in the Fall of 2004. DCA will process centrally online applications from property owners.
DCA will develop a multimedia statewide marketing campaign to promote the lead hazard control assistance and emergency relocation programs including but not limited to: • television and radio public service announcements(PSAs) • multi-cultural, multi-lingual informational print material produced by DCA and
distributed through existing neighborhood based delivery systems-local/county governments, state and local non-profit organizations, and health care providers
• notices and articles in local newspapers, neighborhood-based newsletters, and professional journals
• Childhood Lead Poisoning Prevention Week mailings to all Mayors by the Commissioners of Community Affairs, Health and Senior Services and Human Services
DCA will continue implementation of the LICAR project in the ten target cities. The LICAR goal is to abate lead based paint hazards in 200 units occupied by lead-poisoned children and perform interim controls in 147 units by March 2007.
DCA will request funding renewals under the HUD Lead Hazard Control Grant Program as long as the need persists. Opportunities for partnerships in future applications to HUD and other funding sources will continue to be offered to all eligible municipalities.
DCA will implement the provisions of 24 CFR Part 35 Lead Safe Housing Rule in the administration of its housing assistance programs. This federal rule requires states and units of local government to control lead-based paint hazards in federally assisted housing. Through full implementation of 24 CFR Part 35, the DCA will continue to identify and reduce lead-based paint hazards in pre-1978 housing participating in its HOME and Community Development Block Grant funded rehabilitation initiatives.
DCA will reduce lead-based paint hazards in approximately 13,000 housing units through the enforcement of Section 8 Housing Assistance Program’s annual Housing Quality Standards inspections.
Establish a model community-based lead hazard in housing reduction program in the city of Newark. This project will be sponsored by the Gateway Maternal and Child Health Consortium in collaboration with CLEARCorps, a national non-profit organization. AmeriCorps volunteers will be recruited and trained to perform lead-safe maintenance and to educate community
38

members about lead poisoning prevention. If successful, funding will be sought to expand this model to additional cities.
The DHS Bureau of Licensing will enforce its regulations concerning the presence of lead paint in licensed child care facilities. All new child care centers that open in buildings constructed before 1978 will be required to have an inspection by a State-certified Lead Evaluator. DHS staff will perform periodic follow-up inspections to enforce its regulations that all child care centers located in pre-1978 buildings must be lead free or maintained in a lead-safe condition.
39

Objective 2: To require periodic inspections to ensure lead-safe maintenance.
Strategies:
DCA is currently proposing amendments to: • N.J.A.C. 5:10, Regulations for the Maintenance of Hotels and Multiple Dwellings, which
would require landlords of multifamily dwellings to maintain housing in a lead-safe manner and would incorporate lead hazard inspections into the existing 5-year cyclical inspections for multifamily rental units.
• N.J.A.C. 5:15, Emergency Shelters for the Homeless • N.J.A.C. 5:17, Lead Hazard Evaluation and Abatement Code • N.J.A.C. 5:27, Regulations Governing Rooming and Boarding Houses and • N.J.A.C. 5:28, New Jersey State Housing Code.
The proposed amendments to the State Housing Code would apply the same requirements set forth for multifamily dwellings to one- and two-family tenant occupied houses. These requirements would only become effective if adopted by municipal ordinance. These rules appeared in the May 3, 2004 New Jersey Register, and regulations are expected to be effective after they appear in the New Jersey Register.
DCA will continue to notify all landlords of their obligations under the regulations.
The Task Force will provide technical assistance to local community organizations advocating for municipal ordinances that adopt the lead-safe requirements of the State Housing Code and/or other local ordinances requiring property inspections and/or lead-safe maintenance.
40

Objective 3: Develop a lead-safe housing registry that would track housing units that have undergone lead hazard reduction work.
Strategies:
DCA obtained funding from a HUD Lead Hazard Control Grant to develop a lead-safe housing registry. However, the original registry was limited in scope and would not have been widely available. The Lead Hazard Control Assistance Act mandated the creation of a lead-safe housing registry and makes available substantial financial resources for this purpose. The two sources of funds should be sufficient to create and maintain a lead-safe housing registry. DCA anticipates having the registry online by spring of 2005.
Housing appearing on the registry shall be categorized as either: • lead-free, which shall include any housing constructed after 1977 and housing certified to
be free of lead-based paint by a certified inspector • lead-abated, including housing where lead-based paint hazards have been permanently
abated; • lead-hazard controlled; including housing in which preventative maintenance practices
and interim controls have been implemented; or • lead-free interior, which shall include housing certified to have a lead-free interior by a
certified inspector.
The Lead Safe Housing Registry will be a governmental record open to public inspection.
41

Objective 4: To incorporate lead-safe work practices while performing maintenance and rehabilitation work.
Strategies:
The LHCA Act created a fund which will pay for training opportunities in lead related disciplines. Lead related disciplines include, but are not limited to: abatement supervisor, abatement worker, inspector/risk assessor, dust wipe technician, project designer, lead-safe work practices, and lead-safe maintenance practices. All training will be coordinated with the Task Force and advertised on the DCA internet site. Training opportunities will be limited to those which conform to state and/or federal standards on course curriculum. Until the curriculum is developed for lead-safe work practices, DCA will limit funding to courses approved by either the U.S. Environmental Protection Agency or the U.S. Department of Housing and Urban Development.
DCA will continue to facilitate the coordination of efforts in making annual application for HUD Lead Outreach Grant funds which has as one of its purposes raising public awareness of the safe methods to maintain and renovate housing.
DCA will continue to distribute educational materials promoting lead-safe work practices during remodeling and rehabilitation projects and will partner with the Regional Coalitions.
DCA will continue to provide trainings to promote compliance with HUD’s Lead-Safe Housing Rule for State-certified lead evaluation and abatement contractors, property owners, builders and community organizations.
DCA will continue to provide funding for the delivery of Lead Safe Work Practices training courses as well as technical assistance on the implementation of the rule.
DHSS will continue to develop and implement lead safe work practices standards. Lead safe maintenance and sampling technician trainings will use approved EPA and HUD courses.
DHSS will continue to promote the availability of appropriate training courses in all related disciplines.
DHSS will collaborate and work with lead industry and advocacy groups to promote the work practice standards developed by both federal and state agencies.
42
Objective 5: To evaluate the effectiveness of various treatment methods used to reduce lead-based paint hazards.
Strategies:
UMDNJ in collaboration with DCA and DHSS, will analyze existing data and conduct studies regarding treatment and methods. UMDNJ will determine which techniques are currently being recommended and widely used. Subsequently, studies will be conducted to examine variables such as efficiency, precision, and cost to determine which techniques should be used. This will pertain to topics such as paint removal, window replacement, and general abatement.
DCA will identify individuals working in the area of lead hazard control and form a working group to exchange knowledge and ideas. These working groups would meet quarterly and be composed of Task Force members, contractors, and inspectors. This could be used as an educational tool for people in the field of lead hazard control.
DHSS will continue to investigate and evaluate the effectiveness of cleaning techniques following lead hazard control and reduction work to determine compliance with EPA and HUD standards.
DHSS will continue to promote best practices to lead contractors, workers, inspector/risk assessors and property owners.
43

Section 5: Environment
Multiple sources of lead in the environmental must be addressed in order to eliminate children’s exposure to hazardous levels of lead.
Goal:
• To reduce levels of lead in the environment: air, soil, and water.
Introduction:
There are multiple sources of lead in the environment. In order to eliminate lead poisoning in children, all of these will need to be addressed at some point. The removal of lead from gasoline resulted in a significant decrease in the average blood lead level in children during the 1980’s. At this time, the primary source of elevated blood lead levels in children is lead paint. Activities to address lead paint through abatement and lead-safe maintenance are addressed in Section 4 of this Plan.
As lead hazards from paint are reduced and eliminated, the remaining sources of lead in the environment will assume increased importance as we move toward the goal of full elimination. Lead poisoning elimination efforts need to not forget the total lead-body burden concepts. This reminds us that as certain portions of potential exposure are addressed/controlled, the currently suggested, less significant contributions from other sources may become of greater relative significance. In addition, if the recent studies demonstrating that even lower levels than the presently acceptable blood lead levels continue to be correlated with certain observable effects, then an increased emphasis on the other environmental sources would be required.
Much of the lead in the environmental is found in soil and water as the legacy of past uses of lead. Soil can accumulate lead from deposition from leaded gasoline and industrial emissions, as well as flaking of lead paint from the exterior of buildings. Old lead pipes, brass plumbing fixtures, and solder can leach lead into water. Housing renovation and demolition waste can create lead hazards if not handled properly. And there are still uses of lead in industry that must be monitored and controlled to assure that new hazards are not being created.
The New Jersey Department of Environmental Protection (DEP) has a number of programs that address lead hazards in the environmental, including water, soil, air, and waste disposal, which are described in this section. Some of these programs focus specifically on lead. Others include lead as one of a number of priority pollutants that they address. While lead paint is the primary focus of lead hazard reduction activities in New Jersey at this time, all of these other programs have a vital role to play in the eventual elimination of lead as a hazard to which children are exposed in the environment.
44
Objective 1: Continue to implement the lead and copper rule, including the evaluation of water systems that exceed the lead action level of 15 parts per billion.
Current Status:
In May 1991, USEPA established an action level of 15 micrograms per liter (or, parts per billion) for lead in public drinking water supplies. DEP’s Bureau of Safe Drinking Water (BSDW) maintains the database containing lead data. The lead water system monitoring data is used to track compliance with regulations, and to determine which water systems need to install corrosion control treatment. New Jersey has about 4,381 Public Water Systems (PWS). All Community and Nontransient Noncommunity Water Systems are required to sample for lead. Samples are collected from the most vulnerable taps (homes most likely to be affected by lead plumbing materials) at the most vulnerable time (first flush, or draw). For 2002, DEP reported that 19 of 604 (about 3%) of Community Water Systems, and 95 of 884 (less than 11%) of Nontransient Noncommunity Water Systems (such as schools or factories) had Action Level Violations for Lead.
Strategy:
DEP will continue to report yearly compilations of violations of the lead rule.
Sub-objective 1.a: By the end of 2005, DEP will report on the occurrence of lead in private wells in New Jersey.
Current Status:
DEP adopted the Private Well Testing Act (PWTA) which requires well testing (including lead) for real-estate transactions (effective, 9/16/2002). An action level for lead of 10 parts per billion, the ground water standard, is being used since the PWTA requires a flushed raw water sample be used for compliance with the Act. Under the PWTA, certain wells must be tested before a house can be sold. Landlords of certain properties must also test for certain drinking water parameters and provide a written copy of the result to their tenants. Every time these rental properties subject to the Act are leased, a written copy of the most recent test results must be given to the lessee. The law does not prohibit the sale of property if the water fails one or more drinking water standards. The law mainly ensures that all parties to the real estate transaction know the facts about the well water so that they can make well-informed decisions.
Strategies:
DEP has established an information website, http://www.state.nj.us/dep/pwta/ for buyers and sellers of residential properties with private wells.
DEP will compile general compilations of water test results (from private well testing) that may be identified by county and municipality or other appropriate areas of delineation.
45

DEP will explore development of a lead issue strategy for outreach to affected parties, including communities, the New Jersey Realtor’s Association and the NJU Home Inspector Advisory Committee.
Sub-objective 1.b: By June 2005, assess the status of lead drinking water monitoring/remediation efforts in selected school districts in New Jersey.
Specifically, this sub-objective is to1) determine compliance with the Lead Contamination Reduction Act (LCRA); and 2) develop a strategy for providing outreach to all New Jersey school districts and registered day care enters on the LCRA and the Lead in School Drinking Water Guidance.
Strategies:
DEP has already begun working with DHSS to acquire blood lead data for New Jersey children.
Using EPA and DHSS blood level data, EPA and DEP will continue to jointly prioritize school districts and registered day care centers for future investigation and targeted outreach.
EPA and DEP assess the status of school and registered day care center monitoring and remediation program in priority areas and provide technical assistance as required.
EPA and DEP/DHSS will develop materials for distribution to all school districts and registered day care centers on the LCRA requirements and guidance.
In conjunction with partners (EPA, DHSS, DOE, DHS and PTO), DEP will develop a strategy to provide outreach to all school districts and registered day care centers in the state.
46
Objective 2: By 2005, DEP will achieve 50% reduction of Persistent Bioaccumulative Toxins (PBT) chemicals (that include lead) as compared to base year 1991 by minimizing the generation of solid and hazardous waste.
Current Status: DEP encourages reduction of wastes through recycling items that contain lead and by controlling disposal. Efforts such as Household Hazardous Waste disposal acceptance days and the Lead-acid Battery Act prohibiting disposal and requiring dry cell battery manufacturers to submit battery management plans for collection of used batteries (including those that contain lead) are both important in management and reduction of wastes containing lead. For 2000, recycling rates for lead-acid batteries reportedly approached 100%.
DEP also regulates the management (storage, transportation and disposal) of lead-based paint debris generated from the abatement projects. If the debris generated from abatement, renovation and remodeling activities meets the classification of "household waste" the debris waste must be transported by a transporter licensed by the Department to transport solid waste and must be disposed of at a permitted solid waste landfill.
If the debris does not meet the classification of "household waste", and is generated from demolition activities, the generator must classify the material based on his/her knowledge or by collecting a representative sample(s) of the debris and analyzing the sample(s) of the material. If the concentration of lead is above 5.0 mg/l, the debris must be managed as hazardous waste in accordance with hazardous waste generator requirements for storage, transportation and disposed of as such waste.
On June 17, 2002 the New Jersey Department of Environmental Protection (the Department) adopted an amendment to the Universal Waste Rule (UWR) including consumer electronics as a universal waste. Under the UWR, a generator of consumer electronics is regulated as a small or large quantity handler. A small quantity handler of universal waste accumulates less than 5,000 kilograms (11,000 pounds) of universal waste at any given time. A generator of consumer electronics may send their electronics to another universal waste handler or to a demanufacturer. Demanufacturers of consumer electronics are regulated in New Jersey as a Class D recycling center. Large quantity handlers of universal wastes may not demanufacture electronics.
Strategies: DEP will continue to annually report on Lead-acid battery recycling in the State.
DEP, as a member of the Northeast Waste Management Officials Association (NEWMOA) will review (with regards to considering a New Jersey initiative) NEWMOA’s 2003 project, “Solid Waste (Reducing Electronic Waste)”, which is intended to help states reduce environmental impacts of the management and disposal of waste electronic products, particularly computers, televisions, and other electronic devices that contain hazardous materials, such as lead. Used electronics is a rapidly growing waste stream. A product stewardship approach used for electronics management has been a recent topic in a national dialogue, as the National Electronics Product Stewardship Initiative (NEPSI). DEP will continue to contact EPA for updates on the NEPSI.
47

Objective 3: By June 2005, through pollution prevention techniques, facilities covered under the Pollution Prevention Rules will reduce the quantity of lead and lead compounds generated as non-product output (production-related waste) by 50% from 1993 levels.
Current Status:
The New Jersey Pollution Prevention Act of 1991 was enacted to minimize the use of toxic substances (including lead), and the generation of waste or non-product output (NPO). NPO is used to describe all toxic wastes that are generated at manufacturing facilities, regardless of whether those wastes eventually end up as emissions to air, water or solid waste. Non-product output information is compiled from data submitted by facilities under the Worker and Community Right-to-know Act, normally referred to as facility-level “materials accounting data,” that can provide a complete view of hazardous substances as they flow through communities and facilities manufacturing operations.
From 1994 to 2001, lead use in New Jersey reportedly increased almost 50 million pounds, while lead compounds decreased almost 34 million pounds. Lead usage increased in 49 facilities, while usage decreased in 15 facilities; and lead compounds increased in 54 facilities, and decreased in 31 facilities. Most of the lead NPO was shipped off-site for additional treatment. Trends for both on-site and off-site treatment show increases, but likely are due to new reporting requirements that are capturing additional data, rather than facilities increasing their waste quantities over time. On-site releases for lead and lead compounds have demonstrated a reduction of approximately 77%.
Strategies:
DEP will continue to ensure that appropriate procedures are in place at covered facilities to prevent accidental releases & discharges of regulated hazardous substances (including lead).
DEP will continue to collect, process and disseminate state and federal chemical inventory and environmental lead release data.
DEP will continue to consider lower thresholds for PBTs.
48
Objective 4: Continue to conduct efforts to locate and evaluate point sources of lead emissions.
Current Status:
The Community Right-to-Know regulation requires manufacturing and select non-manufacturing facilities to report the use, storage or production of hazardous substances, including lead, at their facility. In addition, large quantity manufacturers or users are required to report the amounts of hazardous substances released to the environment. Beginning in 2000, the reporting thresholds were lowered for several substances, including lead, that are persistent, bioaccumulative, or toxic in the environment (known as PBTs). These lower thresholds provide more information about emissions of these substances, including lead. This federal Toxic Release Inventory (TRI) requirement lowers the reporting thresholds for lead and lead compounds to 100.
DEP’s Air Quality Permitting Program (AQPP) is responsible for permitting stationary sources of air pollution (e.g., factories, power plants, etc.) - both old sources (those already constructed) and newer facilities - to ensure they do not adversely affect air quality in the state. To accomplish this, AQPP reviews air pollution control permit applications, evaluates air quality impact and health risks; and ensures stack emissions are measured properly.
Strategies:
A five-year summary of covered facilities reporting use of lead is in preparation by DEP. In 2001, a lowered reporting threshold for lead resulted in a larger number of facilities, although these are generally smaller quantity users of lead. This information may be useful for focusing on compliance assistance, enforcement, and community-related issues.
Using risk assessment screening tools, DEP, AQP will continue to target source facilities for additional Risk Reduction efforts for lead.
49
Objective 5: Continue to enforce laws and regulations to clean up industrial lead contamination.
Current Status:
More than 12,000 properties potentially contaminated by hazardous substances (including lead) that may need remediation, can be transformed via redevelopment. The Office of Brownfield Reuse provides coordination to accelerate the process for clean-up and return of these properties to productive uses. The Brownfield and Contaminated Site Remediation Act establishes provisions that advance brownfields reuse as part of a comprehensive program for urban redevelopment. Recent action (Executive. Order No. 38) reduces regulatory uncertainty, expands potential reuses of brownfield sites, and ensures no tolerance for “warehousing” (leaving sites abandoned and avoiding or delaying remediation).
Strategies:
DEP’ s Office of Brownfield Reuse is pursuing a new initiative to promote redevelopment of multiple brownfield sites in areas where for reason of size, location or complexity, sites have remained unaddressed. This initiative brings community residents and developers together in a process to remediate sites with a focus on reuse, whether as open space, housing or other construction. Many of these sites are in underserved areas where contamination (possibly including lead) may not have been addressed.
DEP will work with USEPA on remediation of an area-wide Brownfield project (cluster of Brownfield sites) in a selected urban community that may include historic lead contamination issues.
50

Objective 6: Sustain research efforts to reduce levels of lead in air, water, soil, and other products to which people are exposed.
Current Status:
Task Force member agencies seek to sustain research efforts to reduce levels of lead in the environment, through DEP’s environmental lead research efforts, such as the environmental assessment and reclamation technology review.
Strategies:
Results of research sampling and measurement (conducted from late 1998 through early 2003) of wet and dry deposition levels including lead in New Jersey’s ambient air by the New Jersey Air Deposition Network (NJADN) will have summary results available in 2004. The multi-year study will be under review for funding sources after evaluation and assessment of those results.
DEP-Division of Science, Research and Technology is continuing environmental lead research is addressing lead migration and contamination from outdoor shooting range soils (containing spent lead shot and bullets). This is a federally-funded project.
A meeting will be convened by December 2004 for DEP, USEPA, DHSS and DCA to discuss issues related to indoor shooting ranges.
By December 2005, if successful in obtaining funding, DEP will complete a pilot study to characterize local air toxics, including lead, in a highly industrialized urban community. Partnerships will include the Environmental Occupational Health and Sciences Institute (EOHSI), the Paterson Public Schools, and EPA.
51
Objective 7: By April 2005, prepare draft recommendations concerning a revised ambient air monitoring strategy for lead.
Current Status:
DEP has conducted this monitoring as required per National Ambient Air Quality Standards (NAAQS). The two types of standards under this federal requirement are primary standards, intended to protect the public health, and secondary standards, intended to protect public welfare (e.g. visibility, crop damage, materials degradation). The primary and secondary NAAQS for lead are equal and have been set at 1.5 micrograms per cubic meter (ug/m3) for a calendar quarterly average. Since the Department began collecting data in the late 1960’s, air quality has improved dramatically. At the present time, the state is meeting the National Ambient Air Quality Standards (NAAQS) for lead.
Although lead is a potentially important pollutant in air toxic studies, ambient air lead monitoring is rapidly disappearing nationally due to the continuing very low values being observed. New Jersey’s continued low values has also prompted EPA to allow a phase-out of this monitoring, although DEP plans to re-evaluate the ambient air monitoring strategy for lead.
Strategies:
DEP will designate a Lead in Ambient Air Strategies Workgroup (LAAS) as being responsible for assembling resources on current methodologies in use and assessing potential new methods for ambient air lead monitoring, such as focusing on deposition as opposed to air measurements for the protection of public health.
The LAAS workgroup will prepare preliminary recommendations regarding a revised Ambient Air Monitoring Strategy for Lead for discussion with DHSS for finalization.
A final recommendation will be submitted to USEPA for consideration as an alternative monitoring strategy to currently mandated federal requirements.
52
Objective 8: By December 2005, DEP will report on interim results of Environmental Justice Dialogue Meetings concerning environmental lead issues.
Current Status:
On February 19, 2004, Governor McGreevey signed an executive order calling for state agencies to consider the health and environmental impacts of their decision-making on communities of color and low-income communities. “A major goal is to reduce environmental health risks, not only for everyone, but especially mindful of communities that to date have been disproportionately and unfairly impacted by pollution”.
The executive order also calls for greater inter-agency cooperation to increase community involvement in environmental and public health decision-making and to target outreach efforts more effectively to communities confronting environmental justice issues. The goal is to leverage existing agency resources to create comprehensive, yet streamlined reviews of decisions that affect low-income and minority communities. DEP has already begun conducting environmental justice Dialogue meetings. These dialogues are intended to address environmental justice issues by hearing and considering the interests and concerns of the affected community.
DEP will also be required to use environmental and public health data to identify existing and proposed industrial and commercial facilities in communities of color and low-income neighborhoods that should be targeted for more aggressive compliance, enforcement, remediation and permitting strategies to reduce residents’ exposure to toxics and other pollution (including lead).
Strategies:
DEP and DHSS shall jointly develop a strategy to identify and reduce the most significant environmental and public health risks facing each of the selected communities through chronic health disease surveillance, health monitoring, data gathering, community education and public participation; with particular consideration of lead issues.
Improve both EPA and DEP's ability to address environmental justice issues by hearing and considering the interests and concerns of the environmental justice community.
Hold several environmental justice dialogues in geographically diverse areas of the State.
53
Evaluation Plan
The DHSS Childhood Lead Poisoning Prevention Surveillance System will be the primary means of tracking progress towards the Year 2010 goal of eliminating lead poisoning in New Jersey. DHSS will produce and publish an Annual Report on Childhood Lead Poisoning in New Jersey by October of each year. This report will contain summary tables and analysis on blood lead testing, children with elevated blood lead, and environmental actions of local health departments, for the preceding State Fiscal Year (July 1 - June 30). By law, the report is addressed to the Governor and the State Legislature. It will be posted on the DHSS website, and printed copies will be distributed to the members of the Interagency Task Force on the Prevention of Lead Poisoning, local health departments, and any other interested parties.
The Department of Community Affairs (DCA) will establish and maintain tracking systems for the use of the Lead Hazard Control Assistance Fund, the HUD Lead Hazard Reduction Grant and the Lead in Children At Risk program. These systems will document the number of housing units made lead-safe through these initiatives. The DCA Lead-Safe Housing Registry will document the number of and location of lead-safe housing units in New Jersey.
The Childhood Lead Poisoning Prevention Education Committee will develop an evaluation process for each of the education and primary prevention initiatives. When needed, the committee will seek partners from the UMDNJ - School of Public Health, Rutgers University, and other academic institutions in New Jersey to assist with the design and completion of these evaluations.
The Interagency Task Force will review the Elimination Plan on an annual basis. Progress towards achievement of the goals and objectives will be assessed. Strategies for the following year will be modified, and/or new strategies developed, to further the achievement of the goals. A revised Elimination Plan will be completed and published.
54

Appendices
55

Appendix 1
Interagency Task Force on the Prevention of Lead Poisoning
State Agencies Department of Banking and Insurance
Office of the Insurance Ombudsman
Department of Community Affairs Division of Codes and Standards
Division of Housing and Community Resources
Department of Environmental Protection Division of Science, Research and Technology
Bureau of Safe Drinking Water
Department of Health and Senior Services Division of Family Health Services
Consumer and Environmental Health
Occupational Health Services
Don Bryan Phyllis Sabino
William Connolly Amy Fenwick-Frank Kristy Paolillo Chrystene Wyluda
Robert Haug Dianne Kinnane
Colleen O’Hara
Randy England Eileen Murphy
Ed Stevenson
Barker Hamill
Sylvia Dellas Kevin McNally
Crystal Motlasz
Joseph Eldridge Cynthia Mitchell
Barbara Gerwel Devendra Singh
David Valiante
56
Department of Human Services Office forPrevention of Mental
Retardation and Developmental Disabilities
Division of Medical Assistance and Health Services
Division of Youth and Family Services
U.S. Environmental Protection Agency Division of Enforcement and
Compliance Assistance
Statewide Organizations American Civil Liberties Union Foundation
Amerigroup
The Arc of New Jersey/Prevention Coalition
Association for Children of New Jersey
New Jersey Apartment Association
New Jersey Citizen Policy and Education Fund
Local, regional, and community-based organizations
Deborah Cohen Ellen Dunn
Peg Bennett Ann Clemency Kohler Maribeth Robenolt
Cindy Rogers Sue Welsh Don Wiggins
Dawn D’Orlando Maria McGowan
Laura Livingston
Robin Dahlberg Arlene Kohn Gilbert
Sara Campbell-Hicks Maryann Kokidis
Ann Wilson
Mary Coogan
Conor Fennessy
John Weber
Camden County Department of Health and Human Services Claudia Funaro
Camden County Office for Economic Opportunity Stacey Bentley James Wynn
57
Gateway Northwest Maternal and Child Health Network Felicia Johnson
HOPES, Inc Sara Kalambur
Isles Elyse Pivnick
Maplewood Health Department Bob Roe
Monmouth County Health Department Marcie Tyson
Newark Department of Health and Human Services Tracey Hawkins
Northern NJ Maternal and Child Health Consortium Judy Weisel
Partners for Environmental Quality Interfaith Coalition Fletcher Harper
Paterson Department of Health Joseph Surowiec
Programs for Parents of Essex County Diane Jordan Cindy Sickora
Regional Perinatal Consortium of Monmouth and Ocean Counties
Rutgers Cooperative Extension
South Jersey Lead Consortium
Stony Brook - Millstone Watershed Association
Trenton Department of Health
Tri-County Community Action Agency
Union County Legal Services
Beatriz Oesterheld
Jan Goodman Joe Ponessa
Stanley Stopa
Bob Tucker
Sandra Galayda
Meredith Povisils
Alfred Donnarumma
58

University of Medicine and Dentistry of New Jersey School of Osteopathic Medicine Rosie Horner
Myra Vaughns
Department of Preventive Medicine and Community Health William Halperin
Nisha Jani Donald Louria
59

Appendix 2
Working Group Members
Section 1: Surveillance
Tamarah Christian Newark Dept of Health and Human Services Chuin Choi Eng Newark Dept of Health and Human Services William Halperin University of Medicine and Dentistry of NJ Nisha Jani University of Medicine and Dentistry of NJ Kevin McNally New Jersey Dept of Health and Senior Services Jaydeep Nanavaty New Jersey Dept of Health and Senior Services Joe Sweatlock New Jersey Dept of Health and Senior Services
Section 2: Screening (AKA: Detectors)
Peg Bennett New Jersey Dept of Human Services Tamarah Christian (Co-Chair) Newark Dept of Health and Human Services Sandi Galayda Trenton Dept of Health Nancy Grinyer Paterson Dept of Health Tracey Hawkins Newark Dept of Health and Human Services Nisha Jani UMDNJ-School of Medicine Diane Jordan Programs for Parents of Essex County Maria McGowen New Jersey Dept of Human Services Maribeth Robenolt New Jersey Dept of Human Services Cynthia Rogers New Jersey Dept of Human Services Luis Santa Cruz Health Net of NJ Michele Schwartz New Jersey Dept of Human Services William Silverman (Chair) Horizon Mercy
Section 3: Education (AKA: Leaducators)
Deborah Cohen New Jersey Dept of Human Services Veronica D’Alessandro New Jersey Dept of Community Affairs Sylvia Dellas New Jersey Dept of Health and Senior Services Dawn D’Orlando New Jersey Dept of Human Services Ellen Dunn New Jersey Dept of Human Services Claudia Funaro Camden Co Dept of Health and Human Services Jeanne Gorman New Jersey Apartment Association Rosie Horner University of Medicine and Dentistry of NJ Felicia Johnson Gateway Northwest MCH Network Holly Miller Trenton Dept of Health Crystal Motlasz (Co-Chair) New Jersey Dept of Health and Senior Services
60

Section 3: Education (AKA: Leaducators) continued Beatriz Oesterheld
Charles Quinn Marcie Tyson Myra Vaughns John Weber Judith Weisel (Co-Chair) Ann Wilson
Regional Perinatal Consortium of Monmouth and Ocean Counties
New Jersey Dept of Health and Senior Services Monmouth Co Health Dept University of Medicine and Dentistry of NJ
New Jersey Citizen Policy and Education Fund Northern New Jersey MCH Consortium
The Arc of New Jersey/Prevention Coalition
Section 4: Housing (AKA: Maintenance, Rehabilitation, and Abatement, Inc.)
Veronica D’Alessandro (Chair) Joe Eldridge Jeanne Gorman William Halperin Bob HaugDiane Kinnane Laura Livingston Cynthia Mitchell Kristy Paolillo Gene VanBenthysen
New Jersey Dept of Community Affairs New Jersey Dept of Health and Senior Services
New Jersey Apartment Association University of Medicine and Dentistry of NJ
New Jersey Dept of Community Affairs New Jersey Dept of Community Affairs
U.S. Environmental Protection Agency New Jersey Dept of Health and Senior Services
New Jersey Dept of Community Affairs New Jersey Dept of Health and Senior Services
Section 5: Environment (AKA: Eliminators)
Santina Bruzzone (Co-Chair) Randy England Laura Livingston (Chair) Kevin McNally Joe Ponessa Chrystene Wyluda
Paterson Dept of Health New Jersey Dept of Environmental Protection
U.S. Environmental Protection Agency New Jersey Dept of Health and Senior Services
Rutgers Cooperative Extension New Jersey Dept of Community Affairs
61

Appendix 3
HOUSING BUILT BEFORE 1950 IN NEW JERSEY
County Total
Housing Units # of Units
Built Pre-1950 % of Units
Built Pre-1950
Atlantic 114,090 24,868 21.8%
Bergen 339,820 126,125 37.1%
Burlington 161,311 26,363 16.3%
Camden 199,679 57,949 29.0%
Cape May 91,047 20,248 22.2%
Cumberland 52,863 16,316 30.9%
Essex 301,011 142,297 47.3%
Gloucester 95,054 19,029 20.0%
Hudson 240,618 125,180 52.0%
Hunterdon 45,032 11,720 26.0%
Mercer 133,280 44,117 33.1%
Middlesex 273,637 52,430 19.2%
Monmouth 240,884 56,969 23.6%
Morris 174,379 40,039 23.0%
Ocean 248,711 24,076 9.7%
Passaic 170,048 70,979 41.7%
Salem 26,158 9,623 36.8%
Somerset 112,023 21,286 19.0%
Sussex 56,528 12,221 21.6%
Union 192,945 82,231 42.6%
Warren 41,157 14,786 35.9%
Statewide 3,310,275 998,852 30.2%
Source: 2000 U.S. Census of Housing and Population
62
Appendix 4
Data Tables
63

Table 1
CHILDREN WITH BLOOD TEST RESULTS REPORTED IN FY 2003 NUMBER AND PERCENT OF CHILDREN WITH ELEVATED BLOOD LEAD
BY COUNTY OF RESIDENCE
County Children
Tested Less than 10 ug/dL
10 ug/dL or More
20 ug/dL or More
Percent >=10 ug/dL
Percent >=20 ug/dL
Atlantic 3,920 3,825 95 24 2.4% 0.6%
Bergen 13,449 13,299 150 30 1.1% 0.2%
Burlington 3,199 3,161 38 4 1.2% 0.1%
Camden 7,102 6,929 173 20 2.4% 0.3%
Cape May 972 953 19 3 2.0% 0.3%
Cumberland 3,356 3,145 211 25 6.3% 0.7%
Essex 26,782 24,903 1,879 343 7.0% 1.3%
Gloucester 2,367 2,329 38 8 1.6% 0.3%
Hudson 12,883 12,622 261 64 2.0% 0.5%
Hunterdon 1,448 1,428 20 7 1.4% 0.5%
Mercer 5,390 5,108 282 38 5.2% 0.7%
Middlesex 13,014 12,828 186 28 1.4% 0.2%
Monmouth 7,938 7,827 111 20 1.4% 0.3%
Morris 6,437 6,375 62 11 1.0% 0.2%
Ocean 4,424 4,365 59 13 1.3% 0.3%
Passaic 13,904 13,328 576 99 4.1% 0.7%
Salem 681 651 30 5 4.4% 0.7%
Somerset 4,011 3,962 49 7 1.2% 0.2%
Sussex 1,286 1,275 11 4 0.9% 0.3%
Union 12,045 11,731 314 73 2.6% 0.6%
Warren 1,307 1,278 29 6 2.2% 0.5%
Zip Unknown 27,017 26,380 637 0 2.4% 0.0%
TOTAL 172,932 167,702 5,230 832 3.0% 0.5%
64

Table 2
CHILDREN WITH BLOOD TEST RESULTS REPORTED IN FY 2003 BY BLOOD LEAD LEVEL
AND MUNICIPALITY OF RESIDENCE FOR MUNICIPALITIES WITH POPULATION > 35,000
MUNICIPALITY
Total Children Tested
Number <10
Number >=10
Number >=20
Percent >=10
Percent >=20
Atlantic City 955 918 37 10 3.9% 1.0%
Bayonne City 697 687 10 3 1.4% 0.4%
Belleville Township 813 802 11 3 1.4% 0.4%
Berkeley Township 208 208 0 0 0.0% 0.0%
Bloomfield Township 955 930 25 4 2.6% 0.4%
Brick Township 553 550 3 0 0.5% 0.0%
Bridgewater Township 345 345 0 0 0.0% 0.0%
Camden City 3,344 3,214 130 10 3.9% 0.3%
Cherry Hill Township 525 522 3 1 0.6% 0.2%
Clifton City 1,539 1,497 42 10 2.7% 0.6%
Dover Township 626 624 2 0 0.3% 0.0%
East Brunswick 570 568 2 0 0.4% 0.0%
East Orange City 2,644 2,381 263 59 9.9% 2.2%
Edison Township 1,479 1,468 11 2 0.7% 0.1%
Elizabeth City 4,218 4,085 133 30 3.2% 0.7%
Evesham Township 357 356 1 0 0.3% 0.0%
Ewing Township 330 326 4 0 1.2% 0.0%
Fort Lee Boro 439 437 2 1 0.5% 0.2%
Franklin Township 1,143 1,136 7 0 0.6% 0.0%
Gloucester Township 455 453 2 0 0.4% 0.0%
Hackensack City 1,113 1,098 15 2 1.3% 0.2%
65

MUNICIPALITY
Total Children Tested
Number <10
Number >=10
Number >=20
Percent >=10
Percent >=20
Hamilton Township 1,087 1,052 35 6 3.2% 0.6%
Hillsborough Township 205 203 2 1 1.0% 0.5%
Hoboken City 413 405 8 2 1.9% 0.5%
Howell Township 556 553 3 0 0.5% 0.0%
Irvington Township 3,469 3,143 326 61 9.4% 1.8%
Jackson Township 372 370 2 0 0.5% 0.0%
Jersey City 5,361 5,201 160 38 3.0% 0.7%
Kearny Town 767 764 3 0 0.4% 0.0%
Lakewood Township 1,305 1,264 41 11 3.1% 0.8%
Linden City 717 708 9 0 1.3% 0.0%
Manchester Township 172 172 0 0 0.0% 0.0%
Marlboro Township 508 506 2 0 0.4% 0.0%
Middletown Township 660 659 1 0 0.2% 0.0%
Montclair Township 866 829 37 5 4.3% 0.6%
Mount Laurel Township 275 275 0 0 0.0% 0.0%
New Brunswick City 1,810 1,733 77 14 4.3% 0.8%
Newark City 12,852 11,811 1,041 180 8.1% 1.4%
North Bergen Township 1,286 1,271 15 3 1.2% 0.2%
North Brunswick Township 568 565 3 0 0.5% 0.0%
Old Bridge Township 905 902 3 1 0.3% 0.1%
Parsippany-Troy Hills Township 532 531 1 0 0.2% 0.0%
Passaic City 4,208 4,049 159 25 3.8% 0.6%
Paterson City 5,582 5,218 364 61 6.5% 1.1%
66

MUNICIPALITY
Total Children Tested
Number <10
Number >=10
Number >=20
Percent >=10
Percent >=20
Pennsauken Township 444 430 14 4 3.2% 0.9%
Perth Amboy City 1,496 1,455 41 4 2.7% 0.3%
Piscataway Township 815 811 4 0 0.5% 0.0%
Plainfield City 1,778 1,700 78 25 4.4% 1.4%
Sayreville Boro 597 593 4 0 0.7% 0.0%
South Brunswick Township 711 704 7 2 1.0% 0.3%
Teaneck Township 589 574 15 4 2.5% 0.7%
Trenton City 2,720 2,501 219 28 8.1% 1.0%
Union City 1,937 1,898 39 16 2.0% 0.8%
Union Township 964 945 19 5 2.0% 0.5%
Vineland City 1,230 1,212 18 2 1.5% 0.2%
Washington Township 418 415 3 0 0.7% 0.0%
Wayne Township 703 702 1 1 0.1% 0.1%
West New York Town 1,392 1,378 14 0 1.0% 0.0%
West Orange Township 899 874 25 1 2.8% 0.1%
Woodbridge Township 1,394 1,379 15 1 1.1% 0.1%
TOTAL 85,871 82,360 3,511 636 4.1% 0.7%
67

Table 3
CHILDREN TESTED FY 2002 - 2003
FY 2002 FY 2003 Change
2002 - 03
Percent Change
2002 - 03 ALL CHILDREN
Number of Children Tested
6 – 29 MONTH OLDS
Number of Children in NJ*
Number of Children Tested
Percent of Children Tested
171,712
222,837
89,460
40.1%
172,932
222,837
90,112
40.4%
1,220
652
0.3%
0.7%
0.7%
0.7%
* Estimated, based on number of one and two-year old children in the 2000 U.S. Census.
68

Table 4
CHILDREN 6 TO 29 MONTHS OF AGE WITH BLOOD LEAD TEST RESULTS REPORTED IN FY2003
BY COUNTY OF RESIDENCE
County No. of
Children* Children
Tested Percent Tested
Percent <10ug/dL
Percent >=10ug/dL
Percent >=20ug/dL
Atlantic 6,403 2,059 32.2% 98.1% 1.9% 0.3%
Bergen 21,968 8,826 40.2% 99.0% 1.0% 0.2%
Burlington 10,728 2,047 19.1% 99.0% 1.0% 0.1%
Camden 13,663 3,730 27.3% 97.9% 2.1% 0.2%
Cape May 2,103 563 26.8% 98.0% 2.0% 0.2%
Cumberland 3,639 1,548 42.5% 93.6% 6.4% 0.8%
Essex 22,734 10,484 46.1% 94.1% 5.9% 1.1%
Gloucester 6,666 1,621 24.3% 98.5% 1.5% 0.4%
Hudson 15,205 5,130 33.7% 97.4% 2.6% 0.6%
Hunterdon 3,121 1,238 39.7% 98.9% 1.1% 0.3%
Mercer 8,810 2,691 30.5% 95.4% 4.6% 0.6%
Middlesex 19,683 7,307 37.1% 98.8% 1.2% 0.2%
Monmouth 16,744 4,858 29.0% 98.9% 1.1% 0.2%
Morris 12,987 4,748 36.6% 99.1% 0.9% 0.2%
Ocean 12,765 2,671 20.9% 98.8% 1.2% 0.3%
Passaic 14,232 6,771 47.6% 96.6% 3.4% 0.7%
Salem 1,540 382 24.8% 96.9% 3.1% 0.5%
Somerset 8,843 2,578 29.2% 98.8% 1.2% 0.2%
Sussex 3,876 850 21.9% 99.5% 0.5% 0.1%
Union 14,402 5,749 39.9% 97.4% 2.6% 0.6%
Warren 2,725 975 35.8% 98.3% 1.7% 0.2%
Unknown 13,286 98.2% 1.8% 0.0%
Total 222,837 90,112 40.4% 97.6% 2.4% 0.4%
*U.S. Census 2000 children 1 and 2 years old
69

Table 5
ALL CHILDREN TESTED SINCE JULY 1999 BY AGE DURING FY 2003
Age of Child* Number of Children**
Children Tested
Percent of Children
Tested
Less than 1
One Year
Two Years
Three Years
110,298
111,308
111,529
113,708
5,135
54,417
76,494
84,321
4.7%
48.9%
68.6%
74.1%
* Age on June 30, 2003
** U.S. Census 2000
70
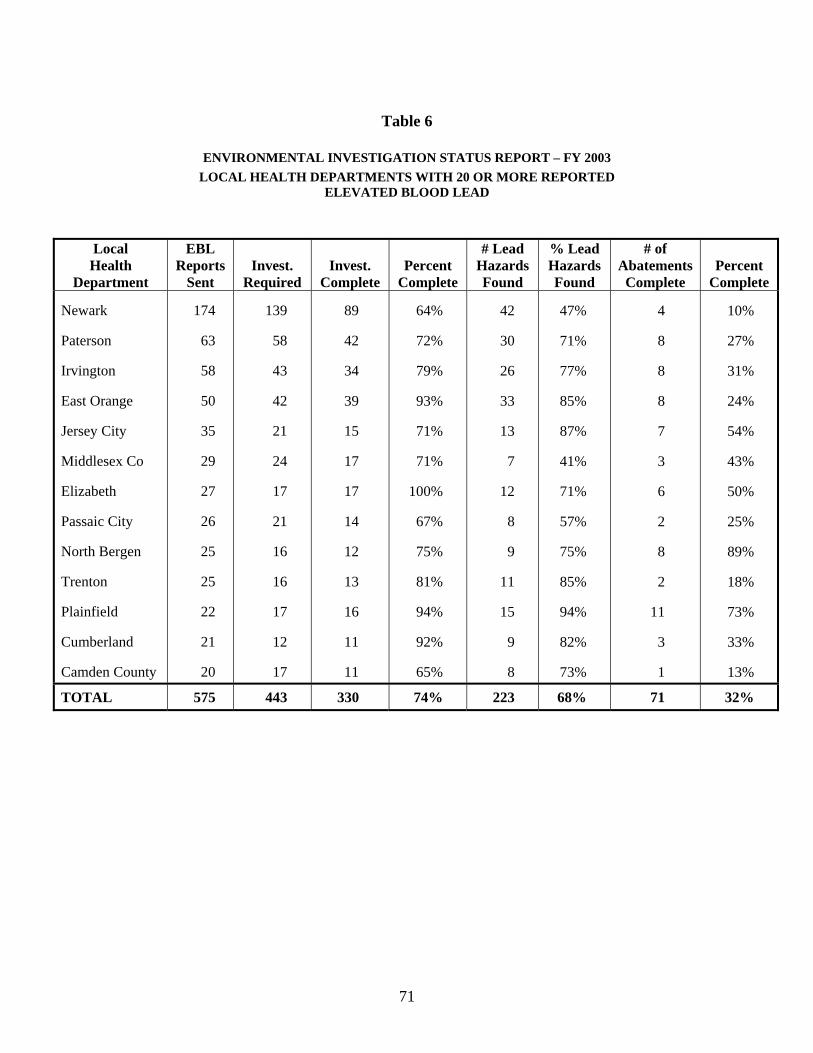
Table 6
ENVIRONMENTAL INVESTIGATION STATUS REPORT – FY 2003
LOCAL HEALTH DEPARTMENTS WITH 20 OR MORE REPORTED ELEVATED BLOOD LEAD
Local Health
Department
EBL Reports
Sent Invest.
Required Invest.
Complete Percent
Complete
# Lead Hazards Found
% Lead Hazards Found
# of Abatements
Complete Percent
Complete
Newark 174 139 89 64% 42 47% 4 10%
Paterson 63 58 42 72% 30 71% 8 27%
Irvington 58 43 34 79% 26 77% 8 31%
East Orange 50 42 39 93% 33 85% 8 24%
Jersey City 35 21 15 71% 13 87% 7 54%
Middlesex Co 29 24 17 71% 7 41% 3 43%
Elizabeth 27 17 17 100% 12 71% 6 50%
Passaic City 26 21 14 67% 8 57% 2 25%
North Bergen 25 16 12 75% 9 75% 8 89%
Trenton 25 16 13 81% 11 85% 2 18%
Plainfield 22 17 16 94% 15 94% 11 73%
Cumberland 21 12 11 92% 9 82% 3 33%
Camden County 20 17 11 65% 8 73% 1 13%
TOTAL 575 443 330 74% 223 68% 71 32%
71

Table 7
CURRENT ENVIRONMENTAL INVESTIGATION STATUS BY FISCAL YEAR FY 1997 THROUGH FY 2003
EBL Percent # Lead % Lead # of % Fiscal Reports Invest. Invest. Invest. Hazard Hazard Abatement Abatement Year Sent Required Complete Complete Found Found Complete Complete
FY 1997 2,168 1,532 1,478 97% 801 54% 749 94%
FY 1998 2,014 1,475 1,437 97% 781 54% 703 90%
FY 1999 1,518 1,056 1,006 95% 652 65% 525 81%
FY 2000 1,144 825 772 94% 596 77% 419 70%
FY 2001 932 664 622 94% 457 74% 316 69%
FY 2002 865 613 582 95% 417 72% 255 61%
FY 2003 802 606 433 72% 290 67% 102 35%
TOTAL 9,443 6,771 6,330 93% 3,994 63% 3,069 77%
Note: This table is cumulative, and reflects the status of all cases as of June 30, 2003
72
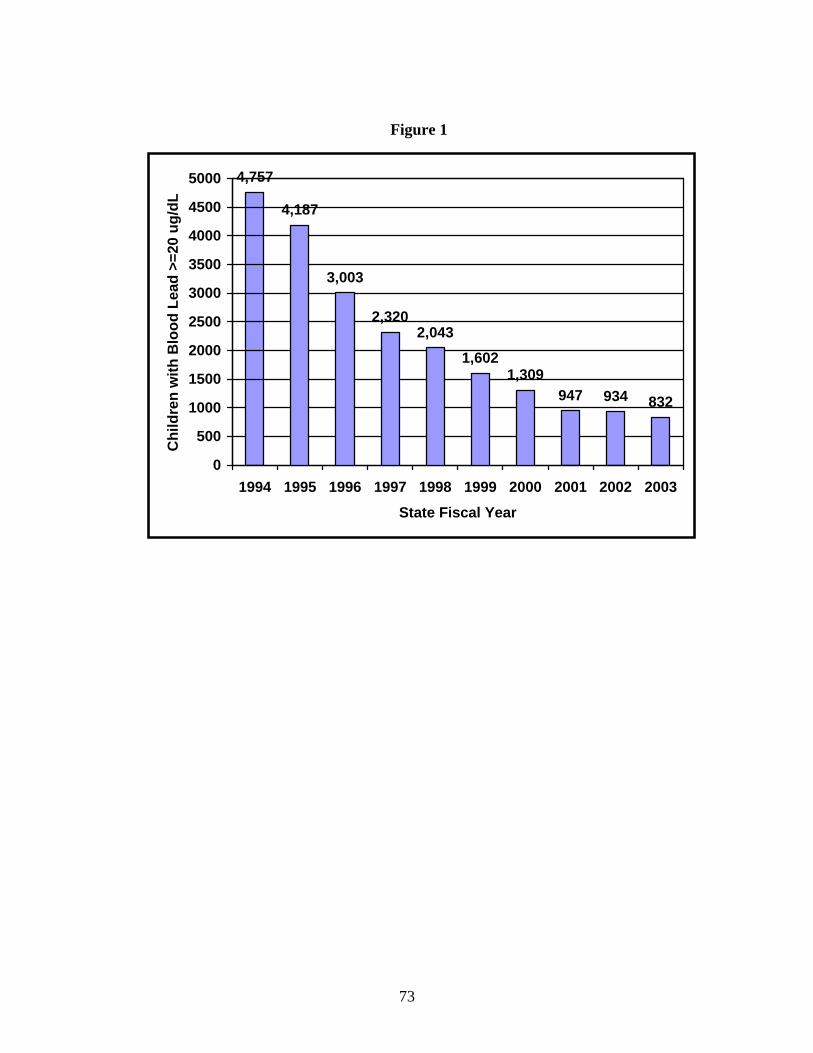
5000 4,757 C
hild
ren
with
Blo
od L
ead
>=20
ug/
dL 4500 4,187
4000
3500 3,003
3000
2500 2,320 2,043
2000 1,602 1500 1,309
947 934 8321000
500
0 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
State Fiscal Year
Figure 1
73

Appendix 5
Letters of Endorsement
74