new horizons in dyslipidemia management in primary … pcsk9 activity inhibits intracellular...
TRANSCRIPT

New Horizons in
Dyslipidemia Management
in Primary Care

Copyright © 2017 by
Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
by any means – graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of
Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.

Optimal control of dyslipidemia in
patients with CVD
Presenter Disclosure
Presenter – Peter Lin, MD
Relationships with commercial interests:
▪ Grants/Research Support: N/A
▪ Speakers Bureau/Honoraria: AstraZeneca, BMS, Takeda, Purdue, Boehringer Ingelheim, Bayer, Lilly, Amgen, Janssen, Forest Laboratories, J&J, Merck, Novartis, Pfizer, Servier, Sanofi, Abbott, Mylan
▪ Consulting Fees: AstraZeneca, Boerhinger Ingelheim, Bayer, Lilly, Merck, Sanofi, Amgen
▪ Other: N/A

Learning Objectives
Upon completion of this activity, participants will be able to:
▪ Discuss the role of LDL-C lowering in cardiovascular risk reduction with
emphasis on the results of recently completed clinical trials
▪ Evaluate recommendations for lipid lowering agents beyond or in addition to
statin therapy for patients with atherosclerotic cardiovascular disease
▪ Explain the mechanism of action of proprotein convertase subtilisin/kexin type
9 (PCSK9) inhibitors and apply the latest clinical data to patient management
strategies
▪ Apply best guideline practice recommendations into routine clinical practice
based on specific patient characteristics

Clot
Cholesterol
Blood Pressure

History of Statin Development 70s
Dr. Akira Endo - Sankyo
• 70s drug companies focus on antibiotics
• 1971 Funghi research project started
– ML 236 B potent inhibitor of HMG Co A reductase

HeFH
Stroke
PAD
Searching for more patients to protect with Statins MI

Where did we get our LDL-C Targets?
Rx - Drug group
Pl - Placebo group
Adapted from Kastelein JJ. Atherosclerosis 1999;143(Suppl 1):S17–S21Heart Protection Study Collaborative Group. Lancet 2002;360:7–22
4S-Pl
4S-RxLipid-Pl
LIPID-Rx
CARE-Pl
CARE-Rx
25
1.3(50)
Percen
t w
ith
CH
D e
ven
t
HPS-Rx
HPS-Pl
1.8(70)
2.3(90)
2.84(110)
3.36(130)
3.87(150)
4.39(170)
4.91(190)
5.43(210)
20
15
10
5
0 End of study LDL-Cmmol/L(mg/dL)
2.5(100)
Target LDL-C 2.5 (100 mg/dL)

Rx - Drug group
Pl - Placebo group
4S-Pl
4S-RxLipid-Pl
LIPID-Rx
CARE-Pl
CARE-Rx
25
1.3(50)
HPS-Rx
HPS-Pl
1.8(70)
2.3(90)
2.84(110)
3.36(130)
3.87(150)
4.39(170)
4.91(190)
5.43(210)
20
15
10
5
0 End of study LDL-Cmmol/L(mg/dL)
A 10mg
Adapted from Kastelein JJ. Atherosclerosis 1999;143(Suppl 1):S17–S21Heart Protection Study Collaborative Group. Lancet 2002;360:7–22
Percen
t w
ith
CH
D e
ven
t
A 80mg
1.8(70)
Where did we get our LDL-C Targets?
Target LDL-C 1.8 (70 mg/dL)

Residual Risk
*CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke
HR = 0.78 (95% CI 0.69, 0.89)
P=0.0002
Pro
port
ion o
f patients
experiencin
g m
ajo
r CV e
vent
atorvastatin 10 mg
atorvastatin 80 mg
0.14
Time (years)
0.08
0.12
0.04
0.10
0.06
0.02
0
LaRosa JC, et al. N Engl J Med. 2005;352:1425–35
0 1 2 3 4 5 6
Residual
Risk

Residual Risk

In the Presence of PCSK9, the LDL-R Is Degraded and Does Not Cycle Back to Cell Surface
Qian YW, et al. J Lipid Res. 2007;48:1488-1498; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.
Serum LDL-Cholesterol Binds to LDL-Receptors. Following Internalization, LDL is Degraded and the Receptor Recycled
LDL
LDL-R
Endocytosis
LDL-R
Recycling Endosome
LDL Degradation
LDL
LDL-R
Endocytosis
Endosome
PCSK9
PCSK9
Self-procession
Hepatocyte
Plasma
© 2013 Amgen Canada Inc. All rights reserved.
Golgi
Apparatus
Endoplasmic
Reticulum
(ER)NucleusLDL, LDL-R and
PCSK9 Degradation

Distribution of Plasma LDL Cholesterol Levels (Panel A) and Incidence of Coronary Heart Disease (Panel B) among Black Subjects, According to the Presence or Absence of a
PCSK9142X or PCSK9679X Allele
Cohen, J. et al. N Engl J Med 2006;354:1264-1272

Blocking PCSK9 Activity Inhibits Intracellular Degradation of LDL-R
Qian YW, et al. J Lipid Res. 2007;48:1488-1498; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.
Monoclonal Antibody binds to PCSK9 and inhibits Binding to the LDL-Receptor
PCSK9
Self-procession
PCSK9 mAb
LDL-R
Endocytosis
Endosome
LDL
Degradation
LDL-R
Recycling
Lysosome
LDL
Hepatocyte
Plasma
© 2013 Amgen Canada Inc. All rights reserved.
Golgi
Apparatus
Endoplasmic
Reticulum
(ER)Nucleus
PCSK9 Inhibitors: Targeted Therapy

Even Maximal Statin Therapy May Not Be Sufficient
In Achieving LDL-C Target
*As per Canadian Product Monographs
1. Crestor (rosuvastatin) Product Monograph. AstraZeneca. April 21, 2015.
2. Lipitor (atorvastatin) Product Monograph. Pfizer. Feb 18, 2016.
3. Pravachol (pravastatin) Product Monograph Bristol-Myers Squibb Canada. Nov 30, 2015.
4. Mevacor (lovastatin) Product Monograph. Merck. Jul. 24, 2012.
5. Zocor (simvastatin) Product Monograph. Merck. Dec 10, 2014.
6. Lescol (fluvastatin) Product Monograph. Novartis. Aug. 26, 2016.
7. Adapted from CURVES Investigators. Am J Cardiol. 1998;81:582-587.
0% 10% 20% 30% 40% 50% 60%
Atorvastatin 10 mg 20 mg 40 mg
Simvastatin 10 mg 20 mg 40 mg
Pravastatin 10 mg 20 mg 40 mg
Lovastatin 20 mg 40 mg 80 mg
Fluvastatin 20 mg 40 mg
Rosuvastatin 10 mg 20 mg5 mg 10 mg 20 mg 40 mg
80 mg
Doubling the statin dose results in only 6% LDL-C reduction

PCSK9Expression
LDL-RExpression
Statin Influence on LDL-C Metabolism plus LDL-R and PCSK9
Acetyl-CoA + acetoacetyl-CoA
HMG-CoAreductase
Plasma
NucleusEndoplasmic
Reticulum (ER)
Hepatocyte
SREBPActivation
LDL-RPCSK9Protein
LDL Proteinat Cell Surface
LDL
PCSK9 Secretion
Hepatocyte Cholesterol
Content
HMG-CoA
Intracellular
Cholesterol
Biosynthesis
STATIN
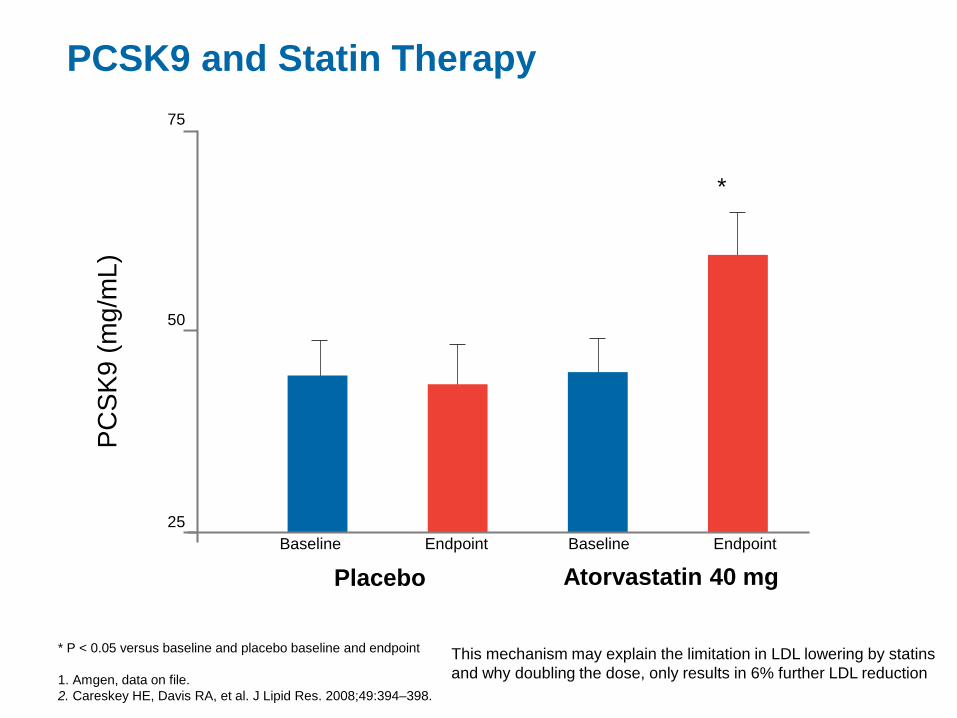
PCSK9 and Statin Therapy
* P < 0.05 versus baseline and placebo baseline and endpoint
1. Amgen, data on file.
2. Careskey HE, Davis RA, et al. J Lipid Res. 2008;49:394–398.
This mechanism may explain the limitation in LDL lowering by statins
and why doubling the dose, only results in 6% further LDL reduction
25
50
75
Baseline Endpoint
Placebo Atorvastatin 40 mg
*
Baseline Endpoint
PC
SK
9 (
mg/m
L)

Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
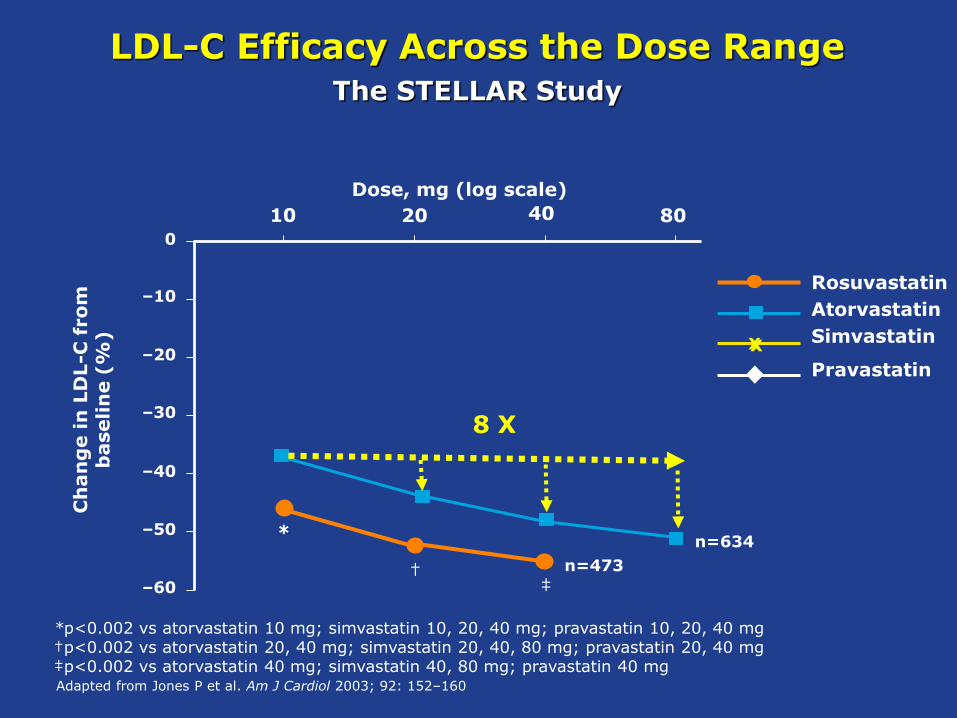
*p<0.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg†p<0.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg‡p<0.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg
–60
–50
–40
–30
–20
–10
0
Dose, mg (log scale)
10 20 40 80
X
‡
Ch
an
ge in
LD
L-C
from
b
aseli
ne (
%)
n=648
n=634*
X
X
X
X
n=473
n=485
†
LDL-C Efficacy Across the Dose RangeThe STELLAR Study
Adapted from Jones P et al. Am J Cardiol 2003; 92: 152–160
X
Rosuvastatin
Atorvastatin
Simvastatin
Pravastatin
*p<0.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg†p<0.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg‡p<0.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg
–60
–50
–40
–30
–20
–10
0
Dose, mg (log scale)
10 20 40 80
X
‡
Ch
an
ge in
LD
L-C
from
b
aseli
ne (
%)
n=634*
n=473†
LDL-C Efficacy Across the Dose RangeThe STELLAR Study
Adapted from Jones P et al. Am J Cardiol 2003; 92: 152–160
X
8 X

PROFICIO
Program to
Reduce LDL-C and
Cardiovascular
Outcomes
Following
Inhibition of
PCSK9
In Different
Populations
(Latin): To advance ;To make progress

Evolocumab Clinical Program: PROFICIO
Reduce LDL-C
(FH, ASCVD, Intolerant)
CV EventsAtherosclerosis

PROFICIO Addresses Key Scientific Questions for Evolocumab
Question Description Study
What is the safety/efficacy of
evolocumab alone?
What is the safety/efficacy with statins?Combination
therapyLAPLACE-1/-2
Does AMG 145 work in patients with
LDLR mutations?
Does AMG 145 work in patients with
mutations in both LDLR alleles?
HoFH/
severe FHTESLA/ TAUSSIG
What is the safety/efficacy in statin-
intolerant patients?
What is the long-term safety/efficacy?Long-term
effectDESCARTES, OSLER-1/-2
Does LDL-C reduction via evolocumab
slow or reverse atherosclerosis?
Does LDL-C reduction via evolocumab
impact CV outcomes?CV outcomes FOURIER

PROFICIO Addresses Key Scientific Questions for Evolocumab
Question Description Study
What is the safety/efficacy of
evolocumab alone?Monotherapy
What is the safety/efficacy with statins?Combination
therapy
Does AMG 145 work in patients with
LDLR mutations?HeFH
Does AMG 145 work in patients with
mutations in both LDLR alleles?
HoFH/
severe FH
What is the safety/efficacy in statin-
intolerant patients?
Statin-
intolerant
What is the long-term safety/efficacy?Long-term
effect
Does LDL-C reduction via evolocumab
slow or reverse atherosclerosis?IVUS
Does LDL-C reduction via evolocumab
impact CV outcomes?CV outcomes

PROFICIO Addresses Key Scientific Questions for Evolocumab
Question Description Study
What is the safety/efficacy of
evolocumab alone?Monotherapy MENDEL-1/-2
What is the safety/efficacy with statins?Combination
therapyLAPLACE-1/-2
Does AMG 145 work in patients with
LDLR mutations?HeFH RUTHERFORD-1/-2
Does AMG 145 work in patients with
mutations in both LDLR alleles?
HoFH/
severe FHTESLA/ TAUSSIG
What is the safety/efficacy in statin-
intolerant patients?
Statin-
intolerantGAUSS-1/-2/-3
What is the long-term safety/efficacy?Long-term
effectDESCARTES, OSLER-1/-2
Does LDL-C reduction via evolocumab
slow or reverse atherosclerosis?IVUS GLAGOV
Does LDL-C reduction via evolocumab
impact CV outcomes?CV outcomes FOURIER

Evolocumab Clinical Program: PROFICIO
Reduce LDL-C
(FH, ASCVD, Intolerant)
CV Events
Fourier TrialAtherosclerosis

Do not copy or distribute. ©2017 Amgen Canada Inc. All rights reserved.

An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical School
2.37 mmol/L

FOURIER: Median LDL-C Levels Over
Time: All Patients
LDL-C was significantly reduced in the evolocumab group (median: 0.78 mmol/L) including 42% who
achieved levels ≤ 0.65 mmol/L vs < 0.1% in the placebo group
Data shown are median values with 95% confidence intervals in the two arms; ITT.
Sabatine MS, et al . NEJM. [published online ahead of print March 17, 2017]. doi: 10.1056/NEJMoa1615664
13,251 13,151 12,954 12,596 12,311 10,812 6,926 3,352 79013,779Placebo13,288 13,144 12,964 12,645 12,359 10,902 6,958 3,323 76813,784Evolocumab
No. at risk
40 12 24 36 48 60 72 84 96 108 120 132 144 156 168
LD
L C
ho
lest
ero
l (m
mo
l/L)
Weeks
59% mean reduction (95% CI 58-60), P < 0.001
Absolute reduction: 1.45 mmol/L (95% CI 1.43-1.47)
2.4
2.2
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
2.6
Placebo
Median 2.38 mmol/L
Evolocumab
Median 0.78 mmol/L

Screening
29
Primary Efficacy Outcome Measure:
Major Cardiovascular Events*
*CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke
HR = 0.78 (95% CI 0.69, 0.89)
P=0.0002
Pro
po
rtio
n o
f p
ati
en
ts e
xp
eri
en
cin
g
majo
r card
iovascu
lar
even
t
0
0.05
0.10
0.15
Atorvastatin 10 mg
Atorvastatin 80 mg
0 1 2 3 4 5 6
Time (years)
LaRosa JC, et al. N Eng J Med. 2005;352
RRR 22% ARR 2.2% NNT6 45
10.9 %
8.7 %

3.7
6.8
9.9
FOURIER:
Composite of CV Death, MI, or Stroke
HR 0.80 (95% CI 0.73 to 0.88); P < 0.001
No. at RiskPlaceboEvolocumab
Cu
mu
lati
ve In
cid
ence
(%
) Placebo + SOC
Evolocumab + SOC
Months
0
2
4
6
8
9
10
11
0 6 1812 24 3630
1
3
5
7
13,780 13,449 13,142 12,288 7,944 3,893 73113,784 13,501 13,241 12,456 8,094 3,935 724
3.1
5.5
7.9
CV = Cardiovascular; MI = Myocardial infarction; HR = Hazard ratio
Sabatine MS, et al . NEJM. [published online ahead of print March 17, 2017]. doi: 10.1056/NEJMoa1615664
Key Secondary Endpoint
RRR 20 % ARR 2.0 % NNT3 50
RRR 22% ARR 2.2% NNT6 45

TNT
FOURIER
RRR 22% ARR 2.2% NNT6 45
RRR 20% ARR 2% NNT3 50
6 YEARS
3 YEARS

Primary Endpoint — ITT
Simva — 34.7%
2742 events
EZ/Simva — 32.7%
2572 events
Cardiovascular death, MI, documented unstable angina requiring
rehospitalization, coronary revascularization (≥30 days), or stroke
7-year event rates
6.4% RRR
2% ARR
NNT7 50

Do not copy or distribute. ©2017 Amgen Canada Inc. All rights reserved.

Total Mortality: 4S
0.85
0.80
0.00
0.0
1.00
0.95
0.90
Pro
port
ion a
live
Years since randomisation
placebo
simvastatin
64321 5
Log rank p=0.0003
4S Group. Lancet 1994;344:1383–1389.

Screening
35
Mortality
No. of patients (%)
Atorvastatin 10 mg
(n=5006)
Atorvastatin 80 mg
(n=4995)
All-cause mortality 282 (5.6) 284 (5.7)
Cardiovascular
CHD death
Stroke death
Hemorrhagic stroke death
155 (3.1)
127 (2.5)
8 (0.2)
2 (0)
126 (2.5)
101 (2.0)
7 (0.1)
3 (0.1)
Noncardiovascular
Cancer
Trauma
Other
127 (2.5)
75 (1.5)
9 (0.2)
43 (0.9)
158 (3.2)
85 (1.7)
15 (0.3)
58 (1.2)
No single cause of death (by body system, or pathological process) and no single cancer
type drove the non-significant difference in all-cause mortality between groups
No statistically significant differences were observed between treatment groups
for any cause of deathLaRosa JC, et al. N Eng J Med. 2005;352

36
0
1
2
3
4
5
6
7
8
9
10
4S S20 4S
PL
CARE
P40
CARE
PL
LIPID
P40
LIPID
PL
HPS
S40
HPS PL TNT
A80
TNT
A10
IDEAL
A80
IDEAL
S20
Mo
rtal
ity
(%)
non-CVCV
Mortality in Statin Secondary
Prevention Trials
Against placebo Statin vs Statin

HR Simva* EZ/Simva* p-value
All-cause death 0.99 15.3 15.4 0.782
CVD 1.00 6.8 6.9 0.997
CHD 0.96 5.8 5.7 0.499
MI 0.87 14.8 13.1 0.002
Stroke 0.86 4.8 4.2 0.052
Ischemic stroke 0.79 4.1 3.4 0.008
Cor revasc ≥ 30d 0.95 23.4 21.8 0.107
UA 1.06 1.9 2.1 0.618
CVD/MI/stroke 0.90 22.2 20.4 0.003
Ezetimibe/Simva
Better
Simva
Better
Individual Cardiovascular Endpoints and CVD/MI/Stroke
0.6 1.0 1.4*7-year
event rates (%)

Fourier Trial

Do not copy or distribute. ©2017 Amgen Canada Inc. All rights reserved.
An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical School

Do not copy or distribute. ©2017 Amgen Canada Inc. All rights reserved.
True Atherosclerotic Disease

42

43

Are they all the sme?

PCSK9 Inhibitors
PCSK9 = Proprotein Convertase Subtilisin Kexin Type 9
▪ PCSK9 inhibitors (PCSK9i)
−Evolocumab
−Alirocumab
−Bococizumab

Terminology of Monoclonal Antibodies
1. Weiner LM. J Immunother. 2006;29:1-9; 2. Yang XD, et al. Crit Rev Oncol Hematol. 2001;38:17-23;
3. Lonberg N. Nat Biotechnol. 2005;23:1117-1125; 4. Gerber DE. Am Fam Physician. 2008;77:311-319.
Mouse
(0% human)
Human
(100% human)
Humanized
(> 90% human)
Chimeric
(65% human)
-umab-zumab-ximab-omabGeneric suffix:
Source (% human protein)
High LowPotential for immunogenicity

PCSK9 Inhibitors
* Investigational product, not approved by Health Canada
PCSK9 = Proprotein Convertase Subtilisin Kexin Type 9
▪ PCSK9 inhibitors (PCSK9i)
−Evolocumab
−Alirocumab
−Bococizumab*



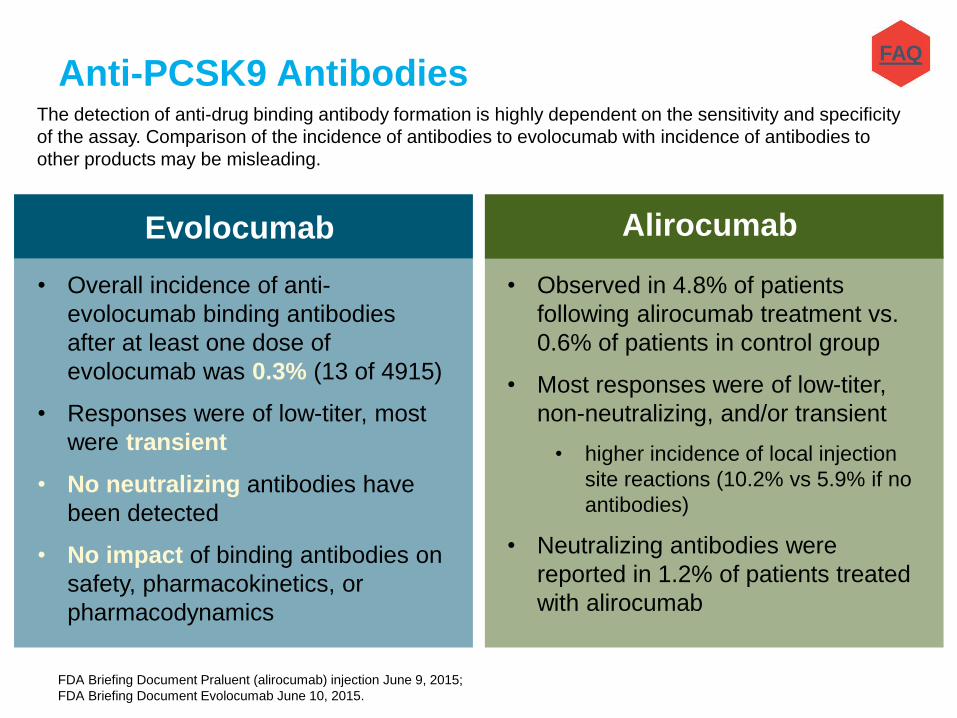
Anti-PCSK9 Antibodies
FDA Briefing Document Praluent (alirocumab) injection June 9, 2015;
FDA Briefing Document Evolocumab June 10, 2015.
Evolocumab
• Overall incidence of anti-
evolocumab binding antibodies
after at least one dose of
evolocumab was 0.3% (13 of 4915)
• Responses were of low-titer, most
were transient
• No neutralizing antibodies have
been detected
• No impact of binding antibodies on
safety, pharmacokinetics, or
pharmacodynamics
Alirocumab
• Observed in 4.8% of patients
following alirocumab treatment vs.
0.6% of patients in control group
• Most responses were of low-titer,
non-neutralizing, and/or transient
• higher incidence of local injection
site reactions (10.2% vs 5.9% if no
antibodies)
• Neutralizing antibodies were
reported in 1.2% of patients treated
with alirocumab
The detection of anti-drug binding antibody formation is highly dependent on the sensitivity and specificity
of the assay. Comparison of the incidence of antibodies to evolocumab with incidence of antibodies to
other products may be misleading.
FAQ
Anti-PCSK9 Antibodies
FDA Briefing Document Praluent (alirocumab) injection June 9, 2015;
FDA Briefing Document Evolocumab June 10, 2015.
Evolocumab
• Overall incidence of anti-
evolocumab binding antibodies
after at least one dose of
evolocumab was 0.3% (13 of 4915)
• Responses were of low-titer, most
were transient
• No neutralizing antibodies have
been detected
• No impact of binding antibodies on
safety, pharmacokinetics, or
pharmacodynamics
Alirocumab
• Observed in 4.8% of patients
following alirocumab treatment vs.
0.6% of patients in control group
• Most responses were of low-titer,
non-neutralizing, and/or transient
• higher incidence of local injection
site reactions (10.2% vs 5.9% if no
antibodies)
• Neutralizing antibodies were
reported in 1.2% of patients treated
with alirocumab
The detection of anti-drug binding antibody formation is highly dependent on the sensitivity and specificity
of the assay. Comparison of the incidence of antibodies to evolocumab with incidence of antibodies to
other products may be misleading.
FAQ

Anti-PCSK9 Antibodies
FDA Briefing Document Praluent (alirocumab) injection June 9, 2015;
FDA Briefing Document Evolocumab June 10, 2015.
Evolocumab
• Overall incidence of anti-
evolocumab binding antibodies
after at least one dose of
evolocumab was 0.3% (13 of 4915)
• Responses were of low-titer, most
were transient
• No neutralizing antibodies have
been detected
• No impact of binding antibodies on
safety, pharmacokinetics, or
pharmacodynamics
Alirocumab
• Observed in 4.8% of patients
following alirocumab treatment vs.
0.6% of patients in control group
• Most responses were of low-titer,
non-neutralizing, and/or transient
• higher incidence of local injection
site reactions (10.2% vs 5.9% if no
antibodies)
• Neutralizing antibodies were
reported in 1.2% of patients treated
with alirocumab
The detection of anti-drug binding antibody formation is highly dependent on the sensitivity and specificity
of the assay. Comparison of the incidence of antibodies to evolocumab with incidence of antibodies to
other products may be misleading.
FAQ

PCSK9 Inhibitor Ongoing OUTCOME Studies
ACS: acute coronary syndrome; CHD: coronary heart disease; CV: cardiovascular; LLT: lipid lowering therapy; MI: myocardial infarction
clinicaltrials.gov accessed August 31, 2015; Swartz GG, et al. Am Heart J. 2014;168(5):682-9.
Evolocumab
FOURIEROutcome Study (5 yrs), N=27 500
• Inclusion criteria: High-risk 2º
prevention population with
LDL-C ≥ 1.8 mmol/L or non-HDL ≥ 2.6
mmol/L
• Evolocumab 140mg Q2W or 420mg
QM + optimal LLT
• 1º endpoint: Time to CV death, MI,
hospitalization for unstable angina,
stroke, or coronary revascularization
Alirocumab
ODYSSEY OutcomesOutcome Study (64 months), N=18 000
• Inclusion criteria: Hospitalized for
ACS within past 1-12 months
• LDL≥ 1.8mmol/L
• Alirocumab 75mg Q2W, up-titrate to
150mg Q2W as needed
• 1º endpoint: Time to CHD death, any
non-fatal MI, fatal and non-fatal
ischemic stroke, unstable angina
requiring hospitalization

PCSK9 Inhibitor Ongoing OUTCOME Studies
ACS: acute coronary syndrome; CHD: coronary heart disease; CV: cardiovascular; LLT: lipid lowering therapy; MI: myocardial infarction
clinicaltrials.gov accessed August 31, 2015; Swartz GG, et al. Am Heart J. 2014;168(5):682-9.
Evolocumab
FOURIEROutcome Study (5 yrs), N=27 500
• Inclusion criteria: High-risk 2º
prevention population with
LDL-C ≥ 1.8 mmol/L or non-HDL ≥ 2.6
mmol/L
• Evolocumab 140mg Q2W or 420mg
QM + optimal LLT
• 1º endpoint: Time to CV death, MI,
hospitalization for unstable angina,
stroke, or coronary revascularization
Alirocumab
ODYSSEY OutcomesOutcome Study (64 months), N=18 000
• Inclusion criteria: Hospitalized for
ACS within past 1-12 months
• LDL≥ 1.8mmol/L
• Alirocumab 75mg Q2W, up-titrate to
150mg Q2W as needed
• 1º endpoint: Time to CHD death, any
non-fatal MI, fatal and non-fatal
ischemic stroke, unstable angina
requiring hospitalization

PCSK9 Inhibitor Ongoing OUTCOME Studies
ACS: acute coronary syndrome; CHD: coronary heart disease; CV: cardiovascular; LLT: lipid lowering therapy; MI: myocardial infarction
clinicaltrials.gov accessed August 31, 2015; Swartz GG, et al. Am Heart J. 2014;168(5):682-9.
Evolocumab
FOURIEROutcome Study (5 yrs), N=27 500
• Inclusion criteria: High-risk 2º
prevention population with
LDL-C ≥ 1.8 mmol/L or non-HDL ≥ 2.6
mmol/L
• Evolocumab 140mg Q2W or 420mg
QM + optimal LLT
• 1º endpoint: Time to CV death, MI,
hospitalization for unstable angina,
stroke, or coronary revascularization
Alirocumab
ODYSSEY OutcomesOutcome Study (64 months), N=18 000
• Inclusion criteria: Hospitalized for
ACS within past 1-12 months
• LDL≥ 1.8mmol/L
• Alirocumab 75mg Q2W, up-titrate to
150mg Q2W as needed
• 1º endpoint: Time to CHD death, any
non-fatal MI, fatal and non-fatal
ischemic stroke, unstable angina
requiring hospitalization

Distribution of Plasma LDL Cholesterol Levels (Panel A) and Incidence of Coronary Heart Disease (Panel B) among Black Subjects, According to the Presence or Absence of a
PCSK9142X or PCSK9679X Allele
Cohen, J. et al. N Engl J Med 2006;354:1264-1272

Meta-analyses suggest earlier, prolonged exposure to lower LDL-C is associated with greater reduction in the risk of CHD
CHD, coronary heart disease; LDL-C, low-density lipoprotein cholesterol
Ference BA, et al. J Am Coll Cardiol. 2012;60:2631-9.
Lower LDL-C
1.0 mmol/L
(38.7 mg/dl)
0.5 mmol/L
(19.3 mg/dl)
0.25 mmol/L
(9.7 mg/dl)
0.125 mmol/L
(4.8 mg/dl)
Sample
Size (N)
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
312,321
169,138
312,321
169,138
312,321
169,138
312,321
169,138
Meta-Analysis
0.46 (0.41-0.51)
0.76 (0.74-0.78)
0.67 (0.64-0.72)
0.87 (0.86-0.88)
0.82 (0.80-0.85)
0.93 (0.93-0.94)
0.91 (0.89-0.92)
0.96 (0.96-0.97)
8.4x10-19
8.4x10-19
8.4x10-19
8.4x10-19
OR (95% CI) p (difference)
0.40 0.50 0.60 0.70 0.80 0.90 1.0

Meta-analyses suggest earlier, prolonged exposure to lower LDL-C is associated with greater reduction in the risk of CHD
CHD, coronary heart disease; LDL-C, low-density lipoprotein cholesterol
Ference BA, et al. J Am Coll Cardiol. 2012;60:2631-9.
Lower LDL-C
1.0 mmol/L
(38.7 mg/dl)
0.5 mmol/L
(19.3 mg/dl)
0.25 mmol/L
(9.7 mg/dl)
0.125 mmol/L
(4.8 mg/dl)
Sample
Size (N)
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
Genetic Studies
Statin Trials
312,321
169,138
312,321
169,138
312,321
169,138
312,321
169,138
Meta-Analysis
0.46 (0.41-0.51)
0.76 (0.74-0.78)
0.67 (0.64-0.72)
0.87 (0.86-0.88)
0.82 (0.80-0.85)
0.93 (0.93-0.94)
0.91 (0.89-0.92)
0.96 (0.96-0.97)
8.4x10-19
8.4x10-19
8.4x10-19
8.4x10-19
OR (95% CI) p (difference)
0.40 0.50 0.60 0.70 0.80 0.90 1.0




3.1
1.2

53% RRR1.2% ARRNNT1 83

PCSK9 Inhibitors and Their Current Indications
ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low density lipoprotein cholesterol;
PCSK9, proprotein convertase subtilisin kexin type 9.
1. Praluent Canadian Product Monograph, April 11, 2016; 2. IRepatha Canadian Product Monograph, June 29 2016;
▪ Alirocumab1
o Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with
• HeFH
• Clinical ASCVD
▪ Evolocumab2
o Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with
• HeFH
• Clinical ASCVD
o Adjunct to diet and other LDL-C lowering therapies in persons ≥12 years with HoFH who require additional LDL-C lowering

PCSK9 Inhibitors and Their Indications
ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low density lipoprotein cholesterol;
PCSK9, proprotein convertase subtilisin kexin type 9.
1. Praluent Canadian Product Monograph, April 11, 2016; 2. IRepatha Canadian Product Monograph, June 29 2016;
▪ Alirocumab1
– Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with
• HeFH
• Clinical ASCVD
▪ Evolocumab2
– Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with
• HeFH
• Clinical ASCVD
– Adjunct to diet and other LDL-C lowering therapies in persons ≥12 years with HoFH who require additional LDL-C lowering

Recommendations for PCSK9i in
FH and ASCVD
• We suggest the use of PCSK9 inhibitors (evolocumab, alirocumab) to lower LDL-C for
patients with heterozygous familial hypercholesterolemia whose LDL-C remains
above target despite maximally tolerated statin therapy (Conditional recommendation, moderate quality
evidence)
• We suggest that PCSK9 inhibitors be considered to lower LDL-C for patients with
atherosclerotic cardiovascular disease in those not at LDL-C goal despite maximally
tolerated statin +/- ezetimibe therapy (Conditional recommendation, moderate quality evidence)
• We suggest that evolocumab be added to background therapy in patients with
homozygous familial hypercholesterolemia and continued if LDL-C lowering is
documented (Conditional recommendation, moderate quality evidence)
Anderson et al. 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of
Cardiovascular Disease in the Adult Canadian Journal of Cardiology 2016;32:1263-1282

Maximize Statin First
Then
PCSK9
Inhibitors