new employee paperwork checklist graduate assistant
TRANSCRIPT

New Employee Paperwork Checklist – Graduate Assistant
Welcome to WOU! All new Graduate Assistants must complete the following forms with Human Resources within three days of beginning work at Western Oregon University. Should you have any questions, please do not hesitate to contact Human Resources at 503.838.8490 or [email protected]. REQUIRED FORMS
1. New Employee Information 2. Federal W-4 (original version required by Human Resources) 3. Oregon W-4 (original version required by Human Resources) 4. I-9 Form (original version required by Human Resources)
a. In order to complete this form, you must present original, unexpired identification from the List of Acceptable Documents to Human Resources. If you are unable to present this identification in-person within three days of your first day of employment, please contact Human Resources to discuss other options.
5. Faculty Payment Plan (complete Graduate Assistant section on second page)
OPTIONAL FORM
1. Direct Deposit (original version required by Human Resources)
IMPORTANT DOCUMENTS TO READ (these are for your records and do not need to be turned into Human Resources)
1. Insurance Market Place 2. Oregon Family Leave Act Poster 3. Family Medical Leave Act and Oregon Family Leave Act Information 4. WolfWeb Memo 5. PERS Notice
All forms listed above can be found under New Employee Paperwork & Onboarding Resources on the Human Resources website and are attached hereto. Should you have any questions, please do not hesitate to contact Human Resources at 503.838.8490 or [email protected].


Employee Information Form
Section 1: Employee Information Legal Name as Printed on Social Security Card: (Last. First, Middle) Social Security Number
- -
Preferred First Name (if different) Primary Phone Number:
( ) Personal Email (Optional)
Permanent Address: Street/PO Box City State Zip County
Preferred WOU Faculty/Staff Email Address Name (see formatting below)
Example: [email protected] for Jane Doe [email protected] Last Name First Letter of First Name
Section 2: Emergency Contact InformationName Relationship Phone Number
( )
Section 3: Employment Information/Job Location Start Date Department Position
Location Job Duties will be Performed: Monmouth, Oregon Other: ____________________________
Type of Appointment: Unclassified Professional Classified Staff Graduate Assistant
Unclassified Faculty Temporary Employee
Section 4: Other Employment
Have you ever been on Western Oregon University payroll? Yes No
If yes, when? ___________________________________________
Are you currently employed by another school in the Oregon University System? Yes No
If yes, what institution? ___________________________________ FTE? _______
Section 5: Retirement Plan Status
Are you an Oregon PERS member? Yes No
If yes, from what agency? _________________________________ Tier? ___________
Are you a member of the Optional Retirement Program (ORP)? Yes No
If yes, where? __________________________________________ Investment company? __________________
Section 6: Signature
___________________________________________ ___________________ Employee Signature Date

This page is intentionally blank. Please continue to next page.
Section 7: Employee Information Name:
Start Date Department Position
Section 8: Miscellaneous (Completion of this Section is Not Required) How did you hear about this job?
Section 9: Affirmative Action Information (Completion of this Section is Not Required)
Gender: Male Female Non-Binary
Race/Ethnicity:
Asian/Pacific Islander: All persons having origins in any of the original peoples of the Far East, Southeast Asia, the Indian subcontinent or the Pacific Islands. The area includes, for example: China, Japan, Korea, the Philippine Islands and Samoa.
Hispanic/Latino: All persons of Mexican, Puerto Rican, Cuban, Central or South American, or other Spanish cultural or origin regardless of race.
Black/African American: All persons having origins in any of the Black racial groups.
American/Alaskan Native: All persons having origins in any of the original peoples of North America, and who maintain cultural identification through tribal affiliation or community recognition.
White (Not of Hispanic Origin): All persons having origin in any of the original peoples of Europe, North Africa, or the Middle East.
Decline or Refuse to Answer
Section 10: Veteran Status Information (Completion of this Section is Not Required)
Vietnam Era Veteran: A veteran whose active military, navy, or air service (or any part of it) was during the period beginning August 4, 1964 and ending May 7, 1975, provided that either of the following is true: 1) the veteran served on active duty for a period of more than 180 days and was discharged or released with other than a dishonorable discharge, or 2) the veteran was discharged or released from active duty because of a service-connected disability
Special Disabled Veteran: Either a) a veteran who is entitled to compensation (or who would be but for the receipt of military retired pay) under laws administered by the Department of Veterans Affairs for a disability (I) rated at 30% or more, or (II) rated at 10 or 20% in the case of a veteran who has been determined under section 1506 of Title 38, to have a serious employment handicap; or b) a veteran who was discharged or released from active duty because of a service-connected disability.
Recently Separated Veteran: A veteran who served on active duty in the U.S. Military, ground, naval, or air service during the one-year period beginning on the date of such veteran’s discharge or release from active duty.
Other Protected Veteran: A veteran who served on active duty during a war or in a campaign or expeditions that met this criterion, go to http://opm.gov/veteran/html/vgmedal2.htm
Section 11: Signature
_____________________________________________ ___________________ Employee Signature Date


Western Oregon University345 Monmouth Ave. N.Monmouth, Oregon 97361 47-2887845




—Provide this form to your employer—
19612101010000Oregon Department of Revenue
2021 Form OR-W-4
Oregon Employee’s Withholding Statement and Exemption Certificate
Office use only
Page 1 of 1, 150-101-402 (Rev. 08-14-20, ver. 01)
Employer’s name
Employee’s signature (This form isn’t valid unless signed.)
Social Security number (SSN)
Federal employer identification number (FEIN)
Date
Address
Employer’s address
City
City
State
State
ZIP code
ZIP code
Note: Your eligibility to claim a certain number of allowances or an exemption from withholding may be subject to review by the Oregon Department of Revenue. Your employer may be required to send a copy of this form to the department for review.
1. Select one: Single Married Married, but withholding at the higher single rate. Note: Check the “Single” box if you’re married and you’re legally separated or if your spouse is a nonresident alien.
2. Allowances. Total number of allowances you’re claiming on line A4, B15, or C5. If you meet aqualification to skip the worksheets and you aren’t exempt, enter 0 .....................................................2.
3. Additional amount, if any, you want withheld from each paycheck ...................................................... 3.
4. Exemption from withholding. I certify that my wages are exempt from withholding and I meetthe conditions for exemption as stated on page 2 of the instructions. Complete both lines below:• Enter the corresponding exemption code. (See instructions) ........................................................... 4a.• Write “Exempt” ................................................................................................................................... 4b.________________________
Sign here. Under penalty of false swearing, I declare that the information provided is true, correct, and complete.
First name Last nameInitial Redetermination
Employer use only.
– –
.00
47-2887845
345 Monmouth Ave N OR 97361
Western Oregon University
Monmouth

150-101-402-1 (Rev. 10-08-20) 1 of 7
Important informationComplete Form OR-W-4 if:• You filed a federal Form W-4 with your employer after
December 31, 2017 and you didn’t file Form OR-W-4 or specify a different number of allowances for Oregon.
• You weren’t satisfied with your prior year Oregon tax-to-pay or refund amount.
• You’ve had a recent personal or financial change that may affect your tax situation, such as a change in your income, filing status, or number of dependents.
Specific information to consider:• Do you (including your spouse) have more than one job?• Do you expect your wages or adjusted gross income
(AGI) on your 2021 return to be more than $100,000 (or $200,000 if filing using the married filing jointly or quali-fied widow(er) filing status)?
• Are you making mid-year changes to your withholding?• Do you receive pension or annuity payments?• Are you a part-year resident, nonresident, or nonresident alien?
If you answered yes to any of these questions, read the “Specific information” section in the instructions before filling out the corresponding worksheets or
Form OR-W-4. The online Oregon Withholding Calculator at www.oregon.gov/dor may provide more accurate results. If you use the online calculator, you don’t need to complete the corresponding worksheets.
Otherwise, read the instructions and complete all applicable worksheets before filling out the Form OR-W-4 and giving it to your employer.
General informationWhat is Oregon income tax withholding? Oregon income tax withholding refers to the amount of Oregon personal income taxes that are withheld from your paychecks to cover your anticipated Oregon tax liability for the year. By law, your employer must withhold a portion of your wages based on your allowances and send the funds to the Department of Revenue.
How is the amount of Oregon income tax withholding determined?You report your marital status, withholding allowances, and any additional amount you want withheld to your employer by completing Form OR-W-4. This information, along with Publication 150-206-436, Oregon Withholding Tax Formulas, which estimates the tax due on your wages, is used by your employer to withhold a specific amount per pay period.
If you have too much tax withheld, you may have a refund when you file your tax return. If you have too little tax withheld, you may owe tax when you file your tax return,
including penalty and interest. See Publication OR-17 for penalty and interest information.
Why has Oregon created Form OR-W-4?In prior years, Oregon employees were able to use the fed-eral Form W-4 to determine and claim Oregon withholding. However, due to federal tax law and form changes, the federal form no longer calculates Oregon withholding correctly. Form(s) W-4 that are submitted to your employer after January 1, 2020 can’t be used to calculate Oregon with-holding. Instead, use Form OR-W-4 to help you calculate allowances for Oregon income tax withholding.
Form OR-W-4 is designed to estimate the amount of tax you’ll need to have withheld for Oregon. Your 2021 tax return may still result in a tax due or refund. For a more accurate calculation, use the Oregon Withholding Calcu-lator at www.oregon.gov/dor to calculate your allowances for Oregon.
How often do I need to complete Form OR-W-4? Complete a new Form OR-W-4 when you start a new job and whenever you have a change in your personal or finan-cial situation that affects your tax situation. This includes changes in your income, marital status, and number of dependents.
What will happen if I don’t complete Form OR-W-4?Your employer will refer to the most recently submitted ver-sion of Form OR-W-4 or Form W-4 when determining with-holding. If you don’t complete Form OR-W-4, your employer will withhold for Oregon based upon the following order:
• An Oregon-only version of the federal Form W-4 for a year prior to 2020.
• Federal Form W-4 for a year prior to 2020.• Eight percent of your wages or other income requiring
withholding.
Specific informationTwo-earners or multiple jobs. If you and your spouse work or if you have more than one job, complete the following steps on the Form OR-W-4 for the highest paying job only:
• Enter the allowances from Worksheet C, line C5 on Form OR-W-4, line 2.
• Enter the additional per-period amount to withhold, if any, from Worksheet C, line C8 on Form OR-W-4, line 3.
For all other (lower-paying) jobs, skip the worksheets and claim -0- allowances on Form OR-W-4 line 2, and -0- addi-tional amount to be withheld on line 3.
If you (including your spouse) have more than two jobs, use the online calculator for more accurate results.
STOP
Oregon Withholding InstructionsForm OR-W-4 2021

150-101-402-1 (Rev. 10-08-20) 2 of 7
Wages or adjusted gross income (AGI) that exceed the threshold. Do you expect to have wages or AGI on your 2021 return that are more than $100,000 (or $200,000 if using the married filing jointly or the qualifying widow(er) filing sta-tus)? Consider using the online calculator to determine the correct amounts to claim on your Form OR-W-4. Otherwise, skip the worksheets. Check the appropriate box on line 1 for your marital status and enter -0- on line 2. You may owe additional tax when you file your return.
Helpful tip: AGI. Your AGI is your total income minus federal adjustments to income. This amount on your 2020 federal Form 1040 may help you estimate your 2021 AGI.
Mid-year changes. If you’re changing your allowances part-way through the year and you claimed too many allowances for the first part of the year, use the online calculator to determine the additional amount you need withheld to make up for the shortage you had during the first part of the year. Otherwise, you may owe tax, penalties, and interest when you file your return. See Publication OR-17 for penalty and interest information.
Pension or annuity payments. Form OR-W-4 can be used to designate the amount of withholding on your pension or annuity payments. Generally, whenever Form OR-W-4 or the instructions refer to jobs or wages, substitute these terms with “pension or annuity” or “pension or annuity payment.”
If you’ve opted out of federal withholding, you’re automati-cally opted out from Oregon withholding also. See Publica-tion OR-ESTIMATE to determine the amount of estimated tax payments you need to make.
If you elect to have Oregon withholding and your pension or annuity payment is required to be withheld at a certain percentage, you aren’t able to claim allowances on Form OR-W-4, line 2. However, you’re able to claim additional withholding on Form OR-W-4, line 3 in addition to the per-centage. If your withholding isn’t required to be withheld at a certain percentage, you’re able to claim amounts on Form OR-W-4, lines 2 and 3.
Exemption from withholding. If you’re exempt from with-holding, skip the worksheets. Complete line 4 and sign Form OR-W-4. For wages, the exemption ends on February 15th of the year following the election. For commercial annui-ties, employer deferred compensation plans, and individual retirement plans the exemption ends once revoked. See additional instructions for line 4 on page 2.
Part-year and nonresidents. If you’re a part-year or nonresi-dent of Oregon, complete the applicable worksheets based on amounts that will be included in the Oregon column of your Oregon return.
Nonresident alien. If all or a portion of your wages are exempt from federal withholding, these wages are also completely or
partially exempt from Oregon withholding. Submit federal Form 8233, Exemption from Withholding on Compensation for Independent Personal Services of a Nonresident Alien Individual, to your employer to exempt all or part of your wages.
If any portion of your wages are not exempt, submit Form OR-W-4 to your employer. As a nonresident alien, you don’t qualify to claim certain items on your Oregon return. Follow the instructions below when completing Form OR-W-4:
• Line 1. Check the “single” box regardless of your marital status.
• Line 2. Usually, you should claim -0- withholding allow-ances. However, if you complete the worksheets, follow the instructions below. — Complete Worksheet B using amounts that will be
listed on your Oregon return. — Once you have completed all applicable worksheets,
subtract 1 allowance from the amount listed on lines A4, B15, or C5.
• Line 4. Don’t claim exempt for having no tax liability or for the portion of your wages exempted under federal Form 8233.
Form OR-W-4 line instructionsType or clearly print your name, Social Security number (SSN), and mailing address.
Note. You must enter a SSN. You can’t use an individual taxpayer identification number (ITIN).
Redetermination check box. If the department issued a determination letter to your employer specifying the amount your employer needs to withhold from your wages and you want to lower your withholding, you must have a personal or financial change affecting your tax situation. If you do, mark the “Redetermination” check box. Provide a copy to your employer and send a copy with all of the applicable worksheets filled out to the department at:
ADP OR-W-4 Project Oregon Department of Revenue PO Box 14560 Salem, OR 97309
Line 1. If you anticipate using the single, married filing separately, or head of household filing status when you file your 2021 return, mark “Single.”
If you anticipate using the married filing jointly, or qualifying widow(er) filing status when you file your 2021 return, mark “Married.” If you meet the married filing jointly qualifica-tions, but want to withhold at the higher “single” rate, mark “Married, but withholding at the higher single rate.”
For the qualifications of each filing status, see federal Publica-tion 501, Exemptions, Standard Deduction, and Filing Information.
Oregon Withholding InstructionsForm OR-W-4 2021
150-101-402-1 (Rev. 10-08-20) 3 of 7
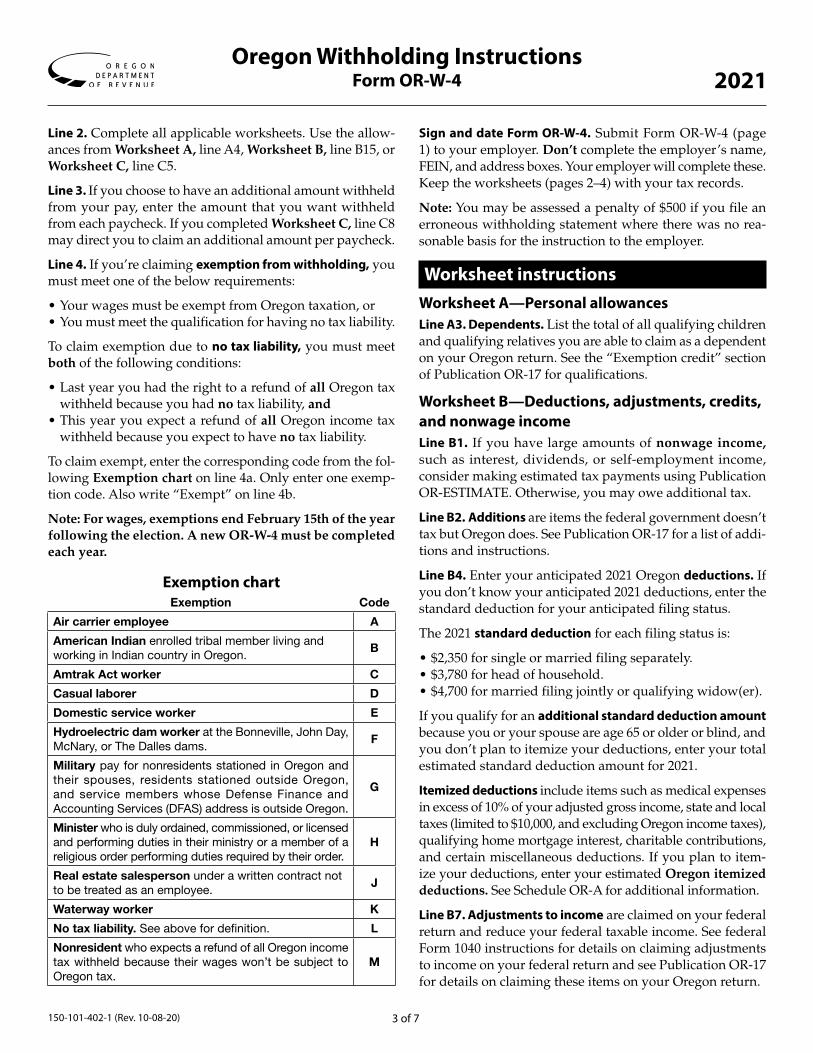
Line 2. Complete all applicable worksheets. Use the allow-ances from Worksheet A, line A4, Worksheet B, line B15, or Worksheet C, line C5.
Line 3. If you choose to have an additional amount withheld from your pay, enter the amount that you want withheld from each paycheck. If you completed Worksheet C, line C8 may direct you to claim an additional amount per paycheck.
Line 4. If you’re claiming exemption from withholding, you must meet one of the below requirements:
• Your wages must be exempt from Oregon taxation, or • You must meet the qualification for having no tax liability.
To claim exemption due to no tax liability, you must meet both of the following conditions:
• Last year you had the right to a refund of all Oregon tax withheld because you had no tax liability, and
• This year you expect a refund of all Oregon income tax withheld because you expect to have no tax liability.
To claim exempt, enter the corresponding code from the fol-lowing Exemption chart on line 4a. Only enter one exemp-tion code. Also write “Exempt” on line 4b.
Note: For wages, exemptions end February 15th of the year following the election. A new OR-W-4 must be completed each year.
Exemption chartExemption Code
Air carrier employee A
American Indian enrolled tribal member living and working in Indian country in Oregon.
B
Amtrak Act worker C
Casual laborer D
Domestic service worker E
Hydroelectric dam worker at the Bonneville, John Day, McNary, or The Dalles dams.
F
Military pay for nonresidents stationed in Oregon and their spouses, residents stationed outside Oregon, and service members whose Defense Finance and Accounting Services (DFAS) address is outside Oregon.
G
Minister who is duly ordained, commissioned, or licensed and performing duties in their ministry or a member of a religious order performing duties required by their order.
H
Real estate salesperson under a written contract not to be treated as an employee.
J
Waterway worker K
No tax liability. See above for definition. L
Nonresident who expects a refund of all Oregon income tax withheld because their wages won’t be subject to Oregon tax.
M
Sign and date Form OR-W-4. Submit Form OR-W-4 (page 1) to your employer. Don’t complete the employer’s name, FEIN, and address boxes. Your employer will complete these. Keep the worksheets (pages 2–4) with your tax records.
Note: You may be assessed a penalty of $500 if you file an erroneous withholding statement where there was no rea-sonable basis for the instruction to the employer.
Worksheet instructionsWorksheet A—Personal allowancesLine A3. Dependents. List the total of all qualifying children and qualifying relatives you are able to claim as a dependent on your Oregon return. See the “Exemption credit” section of Publication OR-17 for qualifications.
Worksheet B—Deductions, adjustments, credits, and nonwage incomeLine B1. If you have large amounts of nonwage income, such as interest, dividends, or self-employment income, consider making estimated tax payments using Publication OR-ESTIMATE. Otherwise, you may owe additional tax.
Line B2. Additions are items the federal government doesn’t tax but Oregon does. See Publication OR-17 for a list of addi-tions and instructions.
Line B4. Enter your anticipated 2021 Oregon deductions. If you don’t know your anticipated 2021 deductions, enter the standard deduction for your anticipated filing status.
The 2021 standard deduction for each filing status is:
• $2,350 for single or married filing separately. • $3,780 for head of household.• $4,700 for married filing jointly or qualifying widow(er).
If you qualify for an additional standard deduction amount because you or your spouse are age 65 or older or blind, and you don’t plan to itemize your deductions, enter your total estimated standard deduction amount for 2021.
Itemized deductions include items such as medical expenses in excess of 10% of your adjusted gross income, state and local taxes (limited to $10,000, and excluding Oregon income taxes), qualifying home mortgage interest, charitable contributions, and certain miscellaneous deductions. If you plan to item-ize your deductions, enter your estimated Oregon itemized deductions. See Schedule OR-A for additional information.
Line B7. Adjustments to income are claimed on your federal return and reduce your federal taxable income. See federal Form 1040 instructions for details on claiming adjustments to income on your federal return and see Publication OR-17 for details on claiming these items on your Oregon return.
Oregon Withholding InstructionsForm OR-W-4 2021
150-101-402-1 (Rev. 10-08-20) 4 of 7
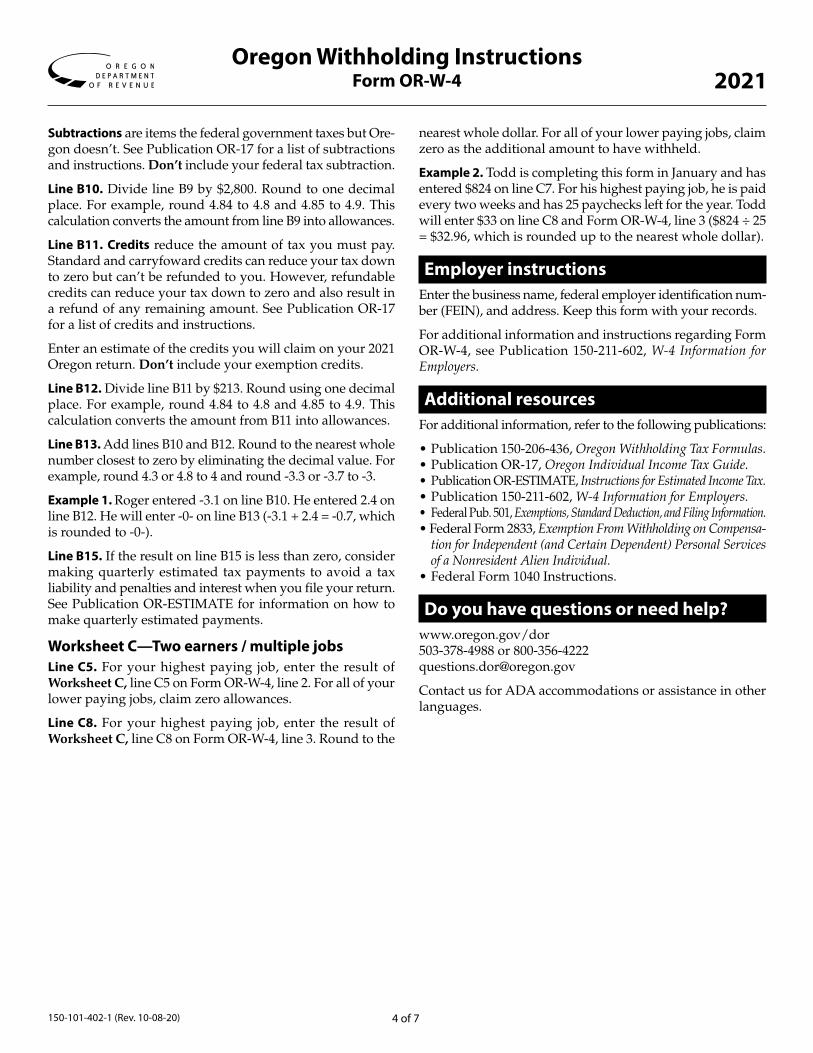
Subtractions are items the federal government taxes but Ore-gon doesn’t. See Publication OR-17 for a list of subtractions and instructions. Don’t include your federal tax subtraction.
Line B10. Divide line B9 by $2,800. Round to one decimal place. For example, round 4.84 to 4.8 and 4.85 to 4.9. This calculation converts the amount from line B9 into allowances.
Line B11. Credits reduce the amount of tax you must pay. Standard and carryfoward credits can reduce your tax down to zero but can’t be refunded to you. However, refundable credits can reduce your tax down to zero and also result in a refund of any remaining amount. See Publication OR-17 for a list of credits and instructions.
Enter an estimate of the credits you will claim on your 2021 Oregon return. Don’t include your exemption credits.
Line B12. Divide line B11 by $213. Round using one decimal place. For example, round 4.84 to 4.8 and 4.85 to 4.9. This calculation converts the amount from B11 into allowances.
Line B13. Add lines B10 and B12. Round to the nearest whole number closest to zero by eliminating the decimal value. For example, round 4.3 or 4.8 to 4 and round -3.3 or -3.7 to -3.
Example 1. Roger entered -3.1 on line B10. He entered 2.4 on line B12. He will enter -0- on line B13 (-3.1 + 2.4 = -0.7, which is rounded to -0-).
Line B15. If the result on line B15 is less than zero, consider making quarterly estimated tax payments to avoid a tax liability and penalties and interest when you file your return. See Publication OR-ESTIMATE for information on how to make quarterly estimated payments.
Worksheet C—Two earners / multiple jobsLine C5. For your highest paying job, enter the result of Worksheet C, line C5 on Form OR-W-4, line 2. For all of your lower paying jobs, claim zero allowances.
Line C8. For your highest paying job, enter the result of Worksheet C, line C8 on Form OR-W-4, line 3. Round to the
nearest whole dollar. For all of your lower paying jobs, claim zero as the additional amount to have withheld.
Example 2. Todd is completing this form in January and has entered $824 on line C7. For his highest paying job, he is paid every two weeks and has 25 paychecks left for the year. Todd will enter $33 on line C8 and Form OR-W-4, line 3 ($824 ÷ 25 = $32.96, which is rounded up to the nearest whole dollar).
Employer instructionsEnter the business name, federal employer identification num-ber (FEIN), and address. Keep this form with your records.
For additional information and instructions regarding Form OR-W-4, see Publication 150-211-602, W-4 Information for Employers.
Additional resourcesFor additional information, refer to the following publications:
• Publication 150-206-436, Oregon Withholding Tax Formulas.• Publication OR-17, Oregon Individual Income Tax Guide.• Publication OR-ESTIMATE, Instructions for Estimated Income Tax.• Publication 150-211-602, W-4 Information for Employers.• Federal Pub. 501, Exemptions, Standard Deduction, and Filing Information.• Federal Form 2833, Exemption From Withholding on Compensa-
tion for Independent (and Certain Dependent) Personal Services of a Nonresident Alien Individual.
• Federal Form 1040 Instructions.
Do you have questions or need help? www.oregon.gov/dor503-378-4988 or 800-356-4222questions.dor@ oregon.gov
Contact us for ADA accommodations or assistance in other languages.
Oregon Withholding InstructionsForm OR-W-4 2021

150-101-402-1 (Rev. 10-08-20) 5 of 7
Oregon Withholding InstructionsForm OR-W-4 2021
A1. Enter “1” for yourself if no one else can claim you as a dependent. Otherwise, enter 0.................... A1.
A2. Enter “1” for your spouse if your spouse doesn’t work. Otherwise, enter 0 ..................................... A2.
A3. Enter the number of dependents you will claim on your Oregon tax return ....................................... A3.
A4. Add lines A1 through A3. Enter the result here and follow the instructions below .............................. A4.
Complete all worksheets that apply. • Worksheet B—Use this worksheet if you plan to do any of the following on your 2021 Oregon return: o Itemize your Oregon deductions or claim additional standard deduction amounts.
o Claim federal adjustments to income or Oregon additions, subtractions, or credits (other than personal exemption credits). o Report nonwage income (such as dividends, interest, or self-employment income).
• Worksheet C—Use this worksheet if you (including your spouse) have more than one job and the combined earnings from all jobs exceed $20,000.
If neither of the above worksheets apply, stop here and enter the number from line A4 on Form OR-W-4, line 2.
Worksheet A—Personal allowances
– Keep this worksheet for your records –
STOP

150-101-402-1 (Rev. 10-08-20) 6 of 7
Oregon Withholding InstructionsForm OR-W-4 2021
Use this worksheet if you plan to do any of the following on your 2021 Oregon return:• Itemize your Oregon deductions or claim additional standard deduction amounts.• Claim federal adjustments to income or Oregon additions, subtractions, or credits (other than personal exemption credits). • Report nonwage income (such as dividends, interest, or self-employment income).
Having your prior year’s Oregon tax return on hand may help you when completing this worksheet. Don’t list numbers as negative unless instructed. For example, write a $1,000 Oregon subtraction as “$1,000”, not “($1,000)”.
B1. Enter your estimated 2021 nonwage income (such as dividends or interest) .............B1.
B2. Enter your estimated 2021 Oregon additions ...............................................................B2.
B3. Add lines B1 and B2 .............................................................................................................................B3.
B4. Enter your estimated 2021 Oregon deductions. (See instructions) ..............................B4.
B5. Enter the standard deduction based on your anticipated 2021 filing status: ..............B5. • Single or Married Filing Separately: $2,350. • Head of Household: $3,780. • Married Filing Jointly or Qualifying Widow(er): $4,700.
B6. Line B4 minus line B5. If the result is zero or less, enter 0 ...................................................................B6.
B7. Enter your estimated 2021 federal adjustments to income and Oregon subtractions (exception—don’t include the federal tax subtraction) ........................................................................B7.
B8. Add lines B6 and B7 .............................................................................................................................B8.
B9. Line B8 minus line B3. If less than zero, enter as a negative amount ..................................................B9.
B10. Line B9 divided by $2,800. Round to one decimal place. If less than zero, enter as a negative amount.................................................................................................................B10.
B11. Enter your estimated 2021 Oregon standard, carryforward, or refundable credits (exception—don’t include personal exemption credits) .................................B11.
B12. Divide line B11 by $213. Round to one decimal place .......................................................................B12.
B13. Add lines B10 and B12. If less than zero, enter as a negative amount. Round to the whole number closest to zero by eliminating the decimal value ..................................................B13.
B14. Enter the number from Worksheet A, line A4 ....................................................................................B14.
B15. Add lines B13 and B14. If zero or less, enter 0. (See instructions) .....................................................B15.
If you plan to use Worksheet C, also enter the result from line B15 on Worksheet C, line C1. Otherwise, stop here and enter the result from line B15 on Form OR-W-4, line 2.
– Keep this worksheet for your records –
Worksheet B—Deductions, adjustments, credits, and nonwage income
STOP
.00
.00
.00
.00
.00
.00
.00
.00
.00
.
.
.00

150-101-402-1 (Rev. 10-08-20) 7 of 7
Oregon Withholding InstructionsForm OR-W-4 2021
If you (including your spouse) have three or more jobs, consider using the Oregon Withholding Calculator at www.oregon.gov/dor for a more accurate calculation of allowances.
If you don’t use the online calculator, use this worksheet to estimate the number of allowances to claim on your highest paying job. Allowances should only be claimed for your highest paying job. Claim zero allowances on Form OR-W-4, line 2 for all of your (or your spouse’s) other jobs to prevent underwithholding.
Only complete this worksheet if you (including your spouse) have more than one job and the combined earnings from all jobs exceed $20,000.
C1. Enter the number from Worksheet B, line B15, if used. Otherwise, enter the number from Worksheet A, line A4 ..................................................................................................... C1.
C2. Enter the number below based on your 2021 anticipated filing status ........................ C2.• Single, Head of Household, or Married Filing Separately: Enter “2”; however, if two of your jobs individually exceed $40,000, enter “4”. • Married Filing Jointly or Qualifying Widow(er): Enter “3”; however, if two of your jobs individually exceed $50,000, enter “6”.
C3. If you (including your spouse) will have three or more jobs at any point during the year, enter the number below based on your 2021 anticipated filing status. Otherwise, enter 0 .................................................................................... C3.
• Single, Head of Household, or Married Filing Separately: Enter “2”. • Married Filing Jointly or Qualifying Widow(er): Enter “3”.
C4. Add lines C2 and C3 .............................................................................................................................C4.
C5. Is line C1 less than line C4? • Yes. Enter 0 on line C5 and on Form OR-W-4, line 2. Complete lines C6 through C8 below to figure the additional withholding amount necessary to avoid a year-end tax bill.• No. Line C1 minus line C4. Enter the result on line C5 (if zero, enter 0) and on Form OR-W-4, line 2. Don’t complete the rest of this worksheet.. ...........................................................................C5.
C6. Line C4 minus line C1 ...........................................................................................................................C6.
C7. Line C6 multiplied by $213 ...................................................................................................................C7.
C8. Line C7 divided by the number of paychecks remaining in 2021 for the highest paying job and rounded to the nearest dollar. Enter the result here and on Form OR-W-4, line 3. This is the additional amount to be withheld from each paycheck ....................................................................... C8.
– Keep this worksheet for your records –
Worksheet C—Two-earners / multiple jobs
STOP
.00
.00

USCIS Form I-9
OMB No. 1615-0047 Expires 10/31/2022
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 10/21/2019 Page 1 of 3Form I-9 10/21/2019 Page 1 of 3
START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.)
Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy)
- -
Employee's E-mail Address Employee's Telephone Number U.S. Social Security Number
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until
(See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following boxes):
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.
(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)
I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.
Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page

Form I-9 10/21/2019 Page 2 of 3Form I-9 10/21/2019 Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 10/31/2022
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1
Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge theemployee is authorized to work in the United States.
The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Today's Date (mm/dd/yyyy)Signature of Employer or Authorized Representative Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)
A. New Name (if applicable)
Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)
Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishescontinuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual.
Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
Western Oregon University
345 Monmouth Ave. N. Monmouth OR 97361

LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Document that contains a photograph (Form I-766)
5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI
b. Form I-94 or Form I-94A that has the following:
(1) The same name as the passport; and
(2) An endorsement of the alien's nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
9. Driver's license issued by a Canadian government authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant Mariner Card
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
7. Employment authorization document issued by the Department of Homeland Security
1. A Social Security Account Number card, unless the card includes one of the following restrictions:
2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240)
3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal
4. Native American tribal document
6. Identification Card for Use of Resident Citizen in the United States (Form I-179)
Documents that Establish Employment Authorization
5. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITH INS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 10/21/2019
Examples of many of these documents appear in the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.

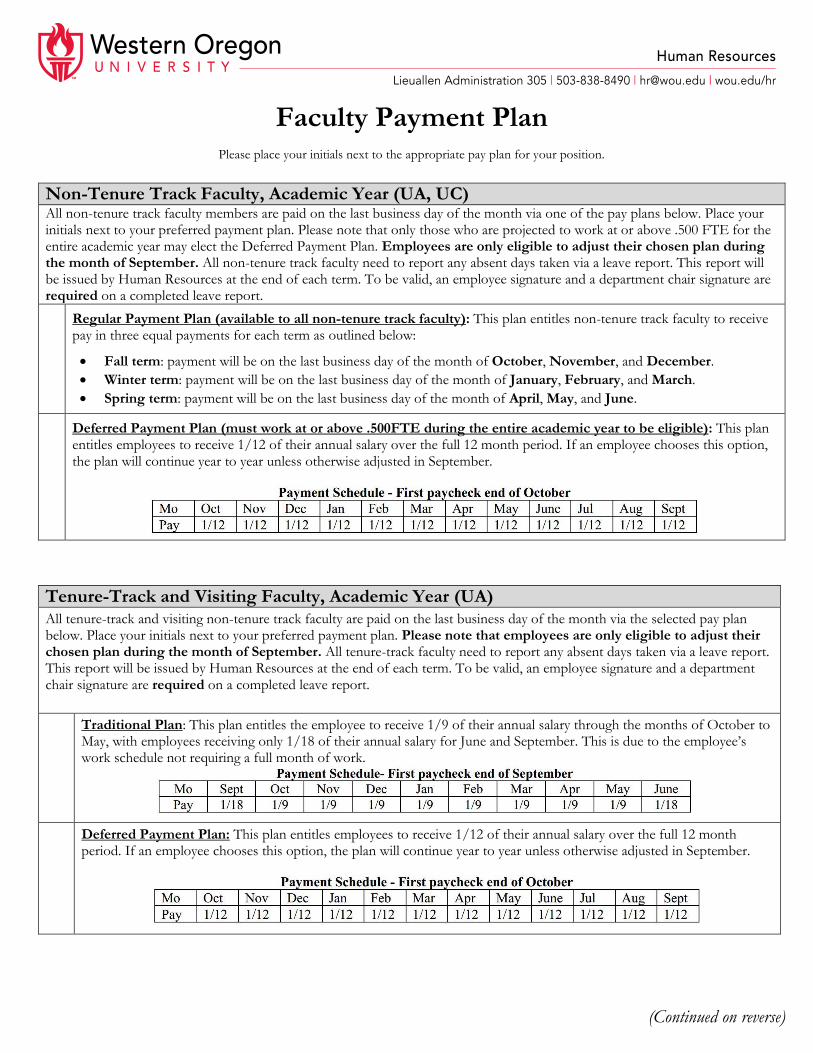
Faculty Payment Plan Please place your initials next to the appropriate pay plan for your position.
Non-Tenure Track Faculty, Academic Year (UA, UC) All non-tenure track faculty members are paid on the last business day of the month via one of the pay plans below. Place your initials next to your preferred payment plan. Please note that only those who are projected to work at or above .500 FTE for the entire academic year may elect the Deferred Payment Plan. Employees are only eligible to adjust their chosen plan during the month of September. All non-tenure track faculty need to report any absent days taken via a leave report. This report will be issued by Human Resources at the end of each term. To be valid, an employee signature and a department chair signature are required on a completed leave report.
Regular Payment Plan (available to all non-tenure track faculty): This plan entitles non-tenure track faculty to receive pay in three equal payments for each term as outlined below:
Fall term: payment will be on the last business day of the month of October, November, and December.
Winter term: payment will be on the last business day of the month of January, February, and March.
Spring term: payment will be on the last business day of the month of April, May, and June.
Deferred Payment Plan (must work at or above .500FTE during the entire academic year to be eligible): This plan entitles employees to receive 1/12 of their annual salary over the full 12 month period. If an employee chooses this option, the plan will continue year to year unless otherwise adjusted in September.
Tenure-Track and Visiting Faculty, Academic Year (UA)
All tenure-track and visiting non-tenure track faculty are paid on the last business day of the month via the selected pay plan below. Place your initials next to your preferred payment plan. Please note that employees are only eligible to adjust their chosen plan during the month of September. All tenure-track faculty need to report any absent days taken via a leave report. This report will be issued by Human Resources at the end of each term. To be valid, an employee signature and a department chair signature are required on a completed leave report.
Traditional Plan: This plan entitles the employee to receive 1/9 of their annual salary through the months of October to May, with employees receiving only 1/18 of their annual salary for June and September. This is due to the employee’s work schedule not requiring a full month of work.
Deferred Payment Plan: This plan entitles employees to receive 1/12 of their annual salary over the full 12 month period. If an employee chooses this option, the plan will continue year to year unless otherwise adjusted in September.
(Continued on reverse)

Faculty Payment Plan Please place your initials next to the appropriate pay plan for your position.
Graduate Assistants (XB) Graduate assistants will receive pay in three equal payments for the terms that they work. Payment is as follows:
Fall term: payment will be on the last business day of the month of October, November, and December.
Winter term: payment will be on the last business day of the month of January, February, and March.
Spring term: payment will be on the last business day of the month of April, May, and June. Employees hired to work during summer will be paid according to the session worked. Payment dates will be included in the summer detail memo.
Stipend (UV)
Faculty paid on a stipend should communicate with their hiring department regarding the amount and pay schedule of their stipend. Payment will occur on the last business day of the month. This amount is subject to payroll taxes.
I have read, understood, and (if applicable) elected a payment plan appropriate for my position:
_______________________________________________________ _____________________ Signature Date
_______________________________________________________ ______________________ Printed Name V#

Direct Deposit & Online Earnings Statement Authorization Payee Information
Last Name First Name M.I. WOU ID#
Employee Type: (check one)
Student Faculty/Staff
New Direct Deposit Bank Name: ABA Routing Number: Account Number:
Account Type: (check one)
Checking – Attach a voided check.*
Savings – Attach verification of bank and account number.* I have instructions with my domestic bank to deposit these funds in their entirety to an international bank outside the U.S.
*Your bank may provide you with a card or form that can be used as well, or you can use the top of your bank statement if it includes both the routing number and account number.
Changing Your Current Direct Deposit Change: (check one)
I wish to stop direct deposit for payroll. I will pick up my check at the Human Resources Office (ADM 306). I wish to stop my current direct deposit and start direct deposit with a new bank account. I wish to continue my current direct deposit and add an additional account, with money being divided between accounts as I determine, clearly
spelled out in an attached document or the back of this form.
Direct Deposit Authorization and Agreement 1. I understand that the deadline for updating my direct deposit is the 10th of each month. If turned in after the 10th, my updated information will
be applied to the next month’s paycheck. If my bank account is closing, I will receive a paper check. 2. By enrolling in direct deposit, I am also opting out of printed payroll earning statements and will access those through Wolf Web. I understand
current monthly earning statements are available on the last business day of each month. 3. It is my responsibility to verify payment has been credited to my account, and that WOU has no liabilities for bank fees for any reason. 4. I have provided accurate and current bank account information. 5. I acknowledge that the origination of ACH transactions to the authorized account must comply with the provisions of Oregon and US law. I
hereby authorize the State of Oregon to initiate credit entries and to initiate, if necessary, debit entries and adjustments for any credit entries in error to my account. This authority will remain in effect until I have cancelled it in person in writing with the Human Resources Office or notification has been sent by my bank that my account is no longer valid.
6. For your safety and protection, WOU requires an original signature and valid photo identification to process any requests for changes or updates to direct deposits.
Signature: Date:
Office Use: Date: By:
GXADIRD PEAEMPL Valid ID Checked

New Health Insurance Marketplace Coverage Options and Your Health Coverage
PART A: General Information :
What is the Health Insurance Marketplace?
Can I Save Money on my Health Insurance Premiums in the Marketplace?
Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace?
How Can I Get More Information?
Form Approved OMB No. 1210-0149 (expires 1-31-201 )
Heather Mercer, Benefits, FMLA, and Worker's Compensation Manager, [email protected], 503.838.8963

PART B: Information About Health Coverage Offered by Your Employer
3. Employer name 4. Employer Identification Number (EIN)
5. Employer address 6. Employer phone number
7. City 8. State 9. ZIP code
10. Who can we contact about employee health coverage at this job?
11. Phone number (if different from above) 12. Email address
Western Oregon University 43-2887845
503.838.8490
Monmouth OR 97361
Heather Mercer
503.838.8963 [email protected]
✔
✔
✔
Classified and Unclassified academic and administrative employees in appointments of at least .50 FTE for90 days or longer.
Spouse; Domestic Partner; and employee's, spouse's, or domestic partner's qualifying Dependent Children(son, daughter, stepson, stepdaughter, adopted child or child placed for adoption, foster child or other legallyplaced child), eligible grandchild, adult child up to age 27, disabled dependent child.
345 Monmouth Ave. N.
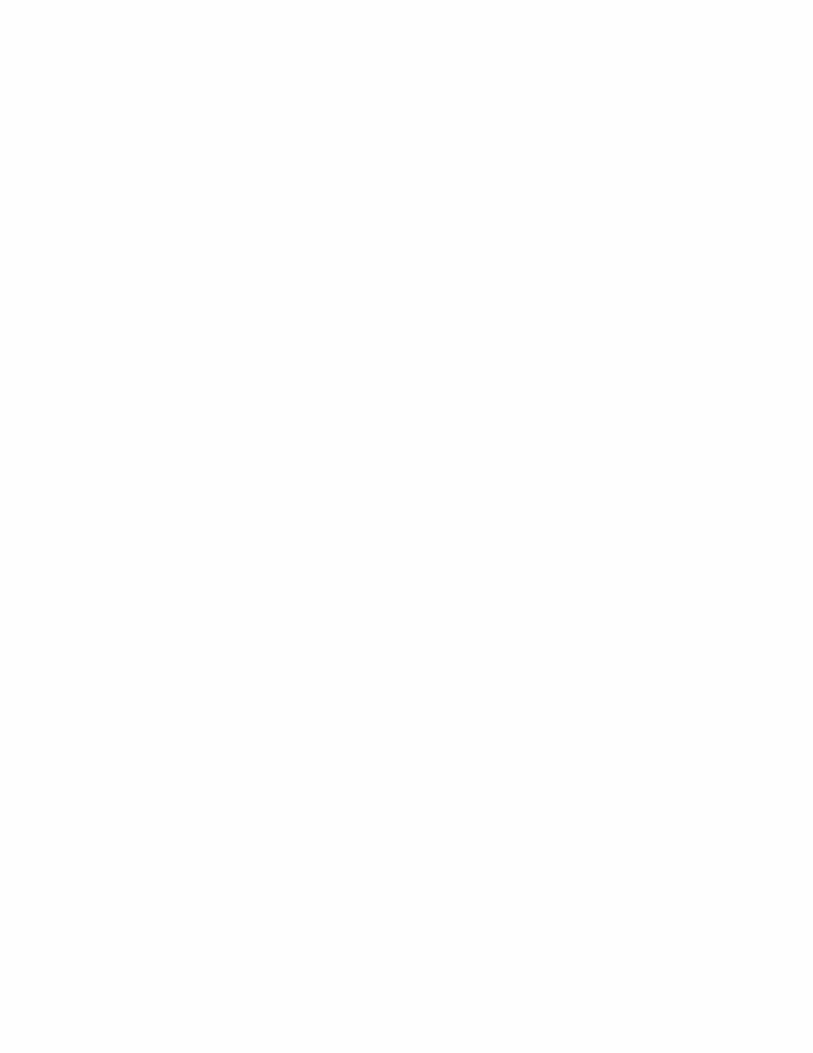
13. Is the employee currently eligible for coverage offered by this employer, or will the employee be eligible inthe next 3 months?
Yes (Continue)13a. If the employee is not eligible today, including as a result of a waiting or probationary period, when is the
employee eligible for coverage? (mm/dd/yyyy) (Continue)No (STOP and return this form to employee)
14. Does the employer offer a health plan that meets the minimum value standard*?Yes (Go to question 15) No (STOP and return form to employee)
15. For the lowest-cost plan that meets the minimum value standard* offered only to the employee (don't includefamily plans): If the employer has wellness programs, provide the premium that the employee would pay if he/ shereceived the maximum discount for any tobacco cessation programs, and didn't receive any other discounts based onwellness programs.a. How much would the employee have to pay in premiums for this plan? $b. How often? Weekly Every 2 weeks Twice a month Monthly Quarterly Yearly
16. What change will the employer make for the new plan year?Employer won't offer health coverageEmployer will start offering health coverage to employees or change the premium for the lowest-cost planavailable only to the employee that meets the minimum value standard.* (Premium should reflect thediscount for wellness programs. See question 15.)
a. How much would the employee have to pay in premiums for this plan? $b. How often? Weekly Every 2 weeks Twice a month Monthly Quarterly Yearly

B U R E A U O F L A B O R A N D I N D U S T R I E S
OregonVal Hoyle, Commissioner
FAMILY LEAVE ACTNOTICE TO
EMPLOYERS AND EMPLOYEES
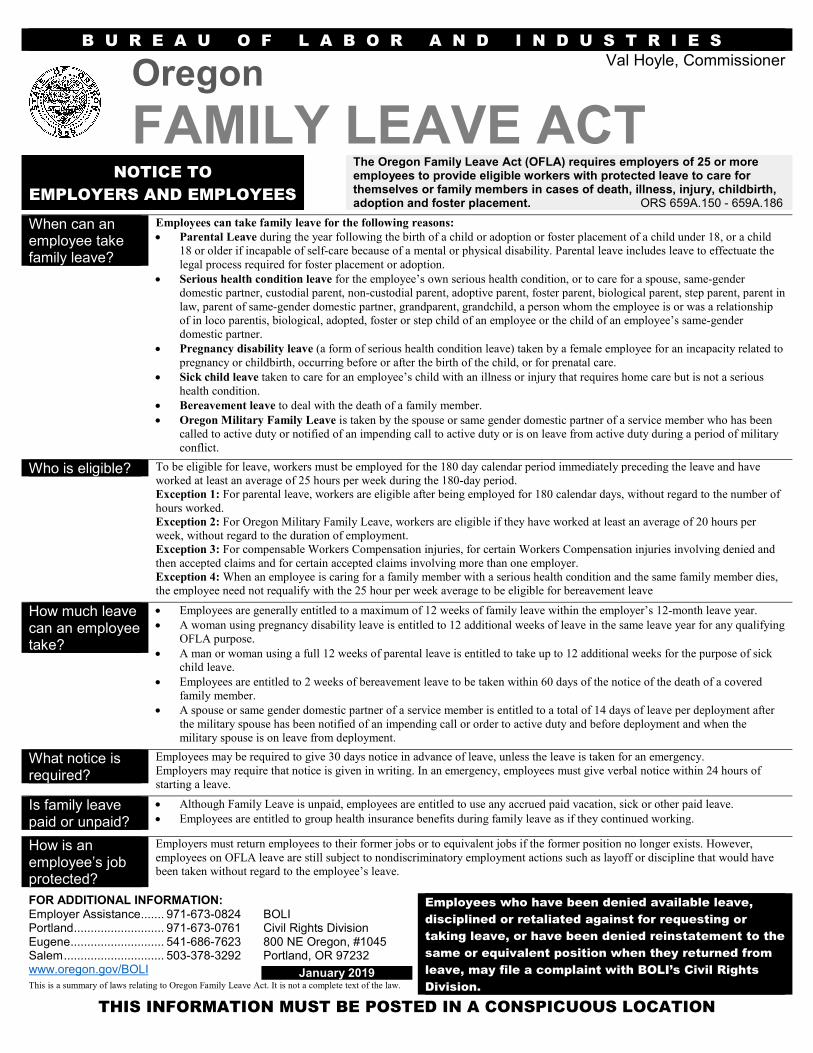
The Oregon Family Leave Act (OFLA) requires employers of 25 or moreemployees to provide eligible workers with protected leave to care forthemselves or family members in cases of death, illness, injury, childbirth,adoption and foster placement. ORS 659A.150 - 659A.186
When can anemployee takefamily leave?
Employees can take family leave for the following reasons: Parental Leave during the year following the birth of a child or adoption or foster placement of a child under 18, or a child
18 or older if incapable of self-care because of a mental or physical disability. Parental leave includes leave to effectuate thelegal process required for foster placement or adoption.
Serious health condition leave for the employee’s own serious health condition, or to care for a spouse, same-genderdomestic partner, custodial parent, non-custodial parent, adoptive parent, foster parent, biological parent, step parent, parent inlaw, parent of same-gender domestic partner, grandparent, grandchild, a person whom the employee is or was a relationshipof in loco parentis, biological, adopted, foster or step child of an employee or the child of an employee’s same-genderdomestic partner.
Pregnancy disability leave (a form of serious health condition leave) taken by a female employee for an incapacity related topregnancy or childbirth, occurring before or after the birth of the child, or for prenatal care.
Sick child leave taken to care for an employee’s child with an illness or injury that requires home care but is not a serioushealth condition.
Bereavement leave to deal with the death of a family member. Oregon Military Family Leave is taken by the spouse or same gender domestic partner of a service member who has been
called to active duty or notified of an impending call to active duty or is on leave from active duty during a period of militaryconflict.
Who is eligible? To be eligible for leave, workers must be employed for the 180 day calendar period immediately preceding the leave and haveworked at least an average of 25 hours per week during the 180-day period.Exception 1: For parental leave, workers are eligible after being employed for 180 calendar days, without regard to the number ofhours worked.Exception 2: For Oregon Military Family Leave, workers are eligible if they have worked at least an average of 20 hours perweek, without regard to the duration of employment.Exception 3: For compensable Workers Compensation injuries, for certain Workers Compensation injuries involving denied andthen accepted claims and for certain accepted claims involving more than one employer.Exception 4: When an employee is caring for a family member with a serious health condition and the same family member dies,the employee need not requalify with the 25 hour per week average to be eligible for bereavement leave
How much leavecan an employeetake?
Employees are generally entitled to a maximum of 12 weeks of family leave within the employer’s 12-month leave year. A woman using pregnancy disability leave is entitled to 12 additional weeks of leave in the same leave year for any qualifying
OFLA purpose. A man or woman using a full 12 weeks of parental leave is entitled to take up to 12 additional weeks for the purpose of sick
child leave. Employees are entitled to 2 weeks of bereavement leave to be taken within 60 days of the notice of the death of a covered
family member. A spouse or same gender domestic partner of a service member is entitled to a total of 14 days of leave per deployment after
the military spouse has been notified of an impending call or order to active duty and before deployment and when themilitary spouse is on leave from deployment.
What notice isrequired?
Employees may be required to give 30 days notice in advance of leave, unless the leave is taken for an emergency.Employers may require that notice is given in writing. In an emergency, employees must give verbal notice within 24 hours ofstarting a leave.
Is family leavepaid or unpaid?
Although Family Leave is unpaid, employees are entitled to use any accrued paid vacation, sick or other paid leave. Employees are entitled to group health insurance benefits during family leave as if they continued working.
How is anemployee’s jobprotected?
Employers must return employees to their former jobs or to equivalent jobs if the former position no longer exists. However,employees on OFLA leave are still subject to nondiscriminatory employment actions such as layoff or discipline that would havebeen taken without regard to the employee’s leave.
FOR ADDITIONAL INFORMATION: Employees who have been denied available leave,
disciplined or retaliated against for requesting or
taking leave, or have been denied reinstatement to the
same or equivalent position when they returned from
leave, may file a complaint with BOLI’s Civil Rights
Division.
Employer Assistance....... 971-673-0824Portland........................... 971-673-0761Eugene............................ 541-686-7623Salem.............................. 503-378-3292www.oregon.gov/BOLI
BOLICivil Rights Division800 NE Oregon, #1045Portland, OR 97232
January 2019This is a summary of laws relating to Oregon Family Leave Act. It is not a complete text of the law.
THIS INFORMATION MUST BE POSTED IN A CONSPICUOUS LOCATION

D E P A R T A M E N T O D E T R A B A J O E I N D U S T R I A S
Ley Val Hoyle, Comisionada
DE LICENCIA FAMILIAR de OregonAVISO A EMPLEADORES Y
EMPLEADOS
La Ley de Licencia Familiar de Oregon (Oregon Family Leave Act: OFLA) requiere que los empleadores que tengan 25 o más empleados otorguen a los trabajadores elegibles licencia protegida para cuidar de su persona o miembros de su familia en caso de muerte, enfermedad, lesión, parto o adopción, y colocación en hogares de crianza. ORS 659A.150 a 659A.186
¿Cuándo puede tomar una licencia familiar un empleado?
Los empleados pueden tomar una licencia familiar por las razones a continuación:
Licencia para padre o madre durante el año siguiente al nacimiento o adopción de un hijo(a) o de la adopción o colocación en
cuidado temporal de un menor de 18 años o de una persona de 18 años de edad o más si es incapaz de cuidarse a sí misma debido a
una discapacidad mental o física. La licencia para padre o madre incluye la licencia para llevar a cabo el proceso legal requerido para
una colocación en cuidado temporal o adopción.
Licencia por condición de salud grave del empleado(a), o para cuidar a un cónyuge, pareja domestica del mismo sexo, padre o
madre con o sin custodia, padre o madre adoptivo(a), padre o madre de crianza, padre o madre biológico(a), padrastro, madrastra,
suegro(a), padre o madre de la pareja domestica del mismo sexo, abuelo(a), nieto(a), cualquier persona con la que el empleado actúe
en lugar de padre o madre, e hijo(a) ya sea biológico(a), adoptado(a), de crianza, o hijastro(a) del empleado(a) o de la pareja
domestica del mismo sexo.
Licencia de discapacidad por embarazo (un tipo de licencia por condición de salud grave) tomada por una empleada debido a una
discapacidad relacionada al embarazo o parto, que ocurra antes o después del nacimiento de un menor o por cuidado prenatal.
Licencia por enfermedad de un menor tomada para cuidar del hijo(a) de un empleado que sufre de una enfermedad o lesión que
requiere del cuidado en el hogar, pero que no es una condición de salud grave.
Licencia por duelo para lidiar con la muerte de un familiar.
Licencia familiar militar de Oregon es tomada por el cónyuge o pareja doméstica del mismo sexo de un miembro del servicio
militar quien ha sido llamado al servicio activo o que ha sido notificado sobre un llamado inminente al servicio activo o que está bajo
licencia del servicio activo durante un periodo de conflicto militar.
¿Quién reúne los requisitos?
Para reunir los requisitos para licencia, los trabajadores deben haber estado empleados por un periodo de 180 días calendario
inmediatamente antes de la licencia y haber trabajado como mínimo un promedio de 25 horas a la semana durante el periodo de 180 días.
Excepción 1: Para la licencia para padre o madre, los trabajadores reúnen los requisitos después de haber estado empleados por 180 días
calendario, sin importar el número de horas trabajadas.
Excepción 2: Para la Licencia familiar militar de Oregon, los trabajadores que califican deben trabajar para un empleador como mínimo
un promedio de 20 horas a la semana, sin importar la duración del empleo.
Excepción 3: Para lesiones aceptadas en el Sistema de Compensación a Trabajadores Lesionados, para ciertas lesiones cuando la queja al
Sistema de Compensación a Trabajadores Lesionados fue primero rechazada y luego aceptada, y para ciertas quejas aceptadas cuando
involucran a más de un empleador.
Excepción 4: Cuando un empleado(a) está cuidando a un familiar con una condición médica seria, si este familiar fallece, el empleado(a)
no tiene que recalificar con un promedio de 25 horas trabajadas por semana para tener derecho a licencia por luto.
¿Cuál es la duración de la licencia que puede tomar un empleado?
Por lo general los empleados tienen derecho a un máximo de 12 semanas de licencia familiar dentro del año de 12 meses de licencia
del empleador.
Una mujer que use la licencia de discapacidad por embarazo tiene el derecho a 12 semanas adicionales de licencia en el mismo año
de licencia para cualquier propósito calificable de OFLA.
Un hombre o una mujer que use una licencia para padre o madre de 12 semanas completas tiene el derecho a tomar hasta 12 semanas
adicionales para el propósito de licencia por enfermedad de un menor.
Los empleados tienen derecho a 2 semanas de licencia por luto a ser tomada dentro de los 60 días siguientes al aviso de la muerte de
un familiar cubierto.
Un cónyuge o pareja doméstica del mismo sexo de un miembro del servicio militar tiene el derecho a un total de licencia de 14 días
laborales por despliegue después de que el cónyuge militar haya sido notificado de un llamado inminente u orden al servicio activo
antes del despliegue y cuando el cónyuge militar esté en un periodo de licencia del despliegue.
¿Qué tipo de aviso es requerido?
Los empleadores pueden requerir que los empleados dan un aviso al empleador con 30 días de anticipación a la licencia, a menos que la
licencia se tome debido a una emergencia. Los empleadores pueden requerir que el aviso sea entregado por escrito. En caso de
emergencia, los empleados deben dar un aviso verbal dentro de las 24 horas de haber empezado una licencia.
¿Se remunera la licencia familiar?
Aunque la licencia familiar no es con goce de sueldo, los empleados tienen el derecho a usar cualquier licencia por enfermedad u otro tipo
de licencia con goce de sueldo o vacaciones con goce de sueldo que hayan acumulado. Los empleados tienen el derecho a la continuación
del seguro médico durante la licencia médica como si hubieran continuado trabajando.
¿Cómo se protege el trabajo de un empleado?
Los empleadores deben regresar a los empleados a sus trabajos anteriores o a trabajos equivalentes si el puesto anterior ya no existe. Sin
embargo, los empleados en licencia de OFLA siguen estando sujetos a medidas de empleo no discriminatorias tales como despido o acción
disciplinaria que se hubiera tomado sin importar la licencia del empleado.
PARA OBTENER INFORMACIÓN ADDICIONAL: Los empleados a quienes se les ha negado una licencia,
que hayan sido disciplinados o que hayan sufrido
represalias por solicitar o tomar una licencia, o a quienes
se les haya negado la reintegración al mismo puesto o a
uno equivalente cuando regresaron de una licencia
pueden presentar una queja ante la División de Derechos
Civiles de BOLI.
Asistencia a empleadores ... 971-673-0824 Portland ............................... 971-673-0761 Eugene ................................ 541-686-7623 Salem .................................. 503-378-3292 www.oregon.gov/BOLI
BOLI Civil Rights Division 800 NE Oregon, #1045 Portland, OR 97232
ENERO DE 2019 El presente es un resumen de las leyes de Oregon pertinentes a la Ley de Licencia Familiar de
Oregon. No es el texto completo de la ley.
ESTA INFORMACIÓN DEBE SER FIJADA EN UN LUGAR VISIBLE

Office of Human Resources 345 North Monmouth Avenue Monmouth, Oregon 97361 Phone: (503) 838-8490 Fax: (503) 838-8144 http://www.wou.edu/hr
FMLA/OFLA Leave Information (Federal Family and Medical Leave Act) / (Oregon Family and Medical Leave Act)
You have a right under FMLA and/or OFLA for up to 12 weeks of unpaid leave in a 12-month period for an FMLA/OFLA reason (It can be paid leave if you have accrued leave to use). Twelve-month period means a rolling twelve-month period measured backward from the date the leave begins and continues with each additional leave day taken. If the leave also qualifies under the Oregon Law or contractual benefit provisions, its use will be counted against both entitlements.
FMLA: An employee must have worked OUS for a total of 1250 hours for a period of 12 months immediately preceding the date leave begins.
OFLA: An employee must have worked for OUS a period of 180 calendar days immediately preceding the date leave begins, and must have worked an average of 25 hours per week during the 180-day period.
A family or medical leave is either requested by the employee directly or the university will invoke family or medical leave for an employee who has a qualifying event.
Examples of qualifying events are:
your own serious health condition,
care of a newborn child, adoption/foster care placement of a child and
care for a family member with a serious health condition
qualifying exigency for an employee whose spouse, child, or parent is on active military duty oris called to active duty status.
The use of leave may be impacted by collective bargaining agreements and personnel rules/policies. It is your responsibility to inquire if you have questions regarding the use of accrued leave or leave without pay.
Unclassified employees must use all accrued sick leave prior to requesting leave without pay while on FMLA/OFLA and may use accrued vacation leave.
Classified employees must use all accrued sick, vacation and personal leave before being placed on leave without pay while on FMLA/OFLA.
Your health benefits must be maintained during any period of unpaid leave under the same conditions as if you continued working, and you must be reinstated to the same or an equivalent job with the same pay, benefits, and terms and conditions of employment on your return from leave. Please note that you have no greater right to reinstatement than you would have had if you had been continuously employed during the FMLA/OFLA period requested.
The University must continue to pay its portion of your core (medical/vision, dental, and employee basic life) benefit premiums while you are on FMLA leave. While you are on leave with pay, you will continue to receive a paycheck and your 5% premium share and any optional benefits you normally pay will be deducted from your paycheck. If you go on leave without pay, the University must continue to pay their portion of your core

medical/vision, dental, and employee basic life) benefit premiums. However, you will be required to self pay your 5% premium share any optional benefits. You will be asked to make arrangements with the Office of Human Resources to continue paying for any optional insurance plans you elect to continue.
If you return to work during the 12 weeks allowed under FMLA leave or the next scheduled working day after the FMLA period ends, active benefit coverage will be reinstated the first day of the next month. If you do not return during or immediately after the 12-week period, coverage reinstatement will depend upon you classification. Classified employees must have at least 80 hours in the pay period in which they return to qualify for benefits for the following month.
You may also be covered by collective bargaining agreements and/or personnel rules/policies that are different than the federal FMLA. In some cases because of these rules/policies, you may be entitled to more leave than is normally available under FMLA. The University must comply with the provisions which are most advantageous to the employee. Leave under collective bargaining agreements and personnel rules/policies will run concurrently with leave available under FMLA.
BENEFITS PROVIDED: FMLA OFLA Job Protection Rights YES YES CORE Benefits YES NO
PROVIDES TIME OFF FOR: FMLA OLFA Care for newborn child, adoption/foster YES YES care placement – both maternal and paternal
Family member serious health condition YES YES Parents-in-law covered: NO YES Same-sex domestic partners covered NO YES
Employee serious health condition YES YES Female employees may take an additional 12 weeks of leave for pregnancy-related health conditions NO YES
Child with minor illness requiring home care NO YES Either parent may take 12 additional weeks for this reason NO YES
ELEGIBILITY FMLA OFLA 180 days of employment; no hours test NO YES*
180 days of employment and must be working NO YES 25+ hours per week
12 months of employment AND YES N/A Exempt employees .50 FTE+ Non-exempt employees 1,250 hours worked in last 12 months
* only for care for newborn child, or adoption/foster care placement.

Office of Human Resources 345 N. Monmouth Ave., Monmouth, OR 97361; Phone: 503.838.8490; Fax: 503.838.8144; wou.edu.hr
Memorandum
To: New Employees
From: Judy Vanderburg Director of Human Resources
Subject: Wolf Web for Employees
The Wolf Web for employees is a secure way (the information is encrypted) for you to see your personal information and payroll data that is kept in the University’s Human Resources Information System.
You can access information about your paycheck, payroll address, benefits and deductions, and W-4 at any time. You and only you will have access to your information.
How Do I Use It? Log on to the WOU Portal
Select the Wolf Web Icon
Additional option would be to:
Go to www.wou.edu/wolfweb
Input username and password
(NOTE: If you have not accessed the Wolf Web in the past and/or have questions or concerns, you may call Human Resources at 503-838-8490 for assistance.)
What if I am having problems using Wolf Web for Employee? You can e-mail us anytime at [email protected].
For assistance with logging on and/or questions regarding the information displayed, callHuman Resources at x88490.
Updated 03/2012


4831-6350-1628.3
IMPORTANT INFORMATION ABOUT YOUR BENEFITS UNDER
THE OREGON PUBLIC EMPLOYEES RETIREMENT SYSTEM
(“PERS”)
You are, or soon will be, eligible to establish membership in the Oregon Public Service Retirement Plan (“OPSRP”), which consists of both a pension program and an Individual Account Program (“IAP”). Once you have established membership in OPSRP, your retirement contributions and benefits are based upon the salary your employer pays you, but only to the extent your salary is taxable in Oregon as determined under Oregon law.
The statutes that establish the rules for OPSRP (ORS Chapter 238A) currently define eligible salary to only include compensation paid by a PERS employer that is taxable in the state of Oregon and paid during a period of qualifying service. Therefore, if your salary is not taxable in the state of Oregon, it will not be counted as eligible salary for contributions to the OPSRP pension and IAP programs, and will not be included in "final average salary" used to calculate retirement benefits under the pension program.
You should carefully review the information in your benefit packet before making any decisions regarding your retirement benefits. If you have any questions about this notice or PERS benefits, please contact Heather Mercer at 503-838-8963. If you have questions about whether your current or future compensation is taxable in the state of Oregon, you should consult with your tax advisor.