new dimensions - fall 2012
DESCRIPTION
New Dimensions - Fall 2012TRANSCRIPT

Fall 2012 Vol. 3, No. 2
Adaptive Athletics >>Page 4
ALSO INSIDE:
Focus on Concussion Prevention, Treatment >>Page 6
Post-polio Pioneer Dr. Lauro Halstead Retires >>Page 9
The Metagenomics of UTI >>Page 10
A first-of-its-kind clinic at MedStar NRH is breaking new ground through a collaborative
approach to aphasia management. The clinic integrates cognitive neurology with speech-
language pathology to produce goal-oriented cutting-edge therapy for people with aphasia.
MedStar National Rehabilitation Network Aphasia Clinic—Unique Collaborative Approach to Aphasia Care
Knowledge and CompassionFocused on You
Aphasia affects more than 1 million Americans—and an estimated 100,000 people in the U.S. acquire the disorder each year. The result of damage to the left hemisphere of the brain from stroke and other brain injury, aphasia can be a debilitating condition that frustrates and isolates people, who struggle to communicate. Many people with aphasia reach a plateau in therapy and discontinue treatment, never fully returning to their active lives.
Today, a better understanding of brain plasticity is opening the door to improvements in treatment, and hope for a fuller recovery. The MedStar NRH Aphasia Clinic is harnessing this new knowledge to help men and women with a recent diagnosis of aphasia—as well as those who want to
improve their communication skills, even years after their illness or injury.
Individualized Neurologic and Speech Assessments
The clinic brings together Director Peter Turkeltaub, MD, PhD, a nationally recognized cognitive neurologist specializing in aphasia diagnosis, evaluation and research, with MedStar NRH speech-language pathologists Denise Frankoff and Brooke Hatfield, who have extensive experience and training in working with people with aphasia. The hallmark of the clinic’s approach is its comprehensive language and medical evaluation of each participant. This unique
Continued on page 2.
Cognitive Neurologist Peter Turkeltaub assesses the neurological aspects of aphasia for a more comprehensive picture of each person’s problem.
2 MedStar National Rehabilitation Network
collaborative assessment helps the clinic team pinpoint the precise areas of the brain affected by stroke or brain injury, and characterize the type of aphasia clients are experiencing.
“We’re the first facility in the region to offer this type of comprehensive care,” says Patricia Fletcher, SLP, director, speech-language pathology. “We know that aphasia can range from mild to profound, and can cause a variety of different specific language and communication problems. Every person is unique and no one therapeutic method is effective for everyone,” she adds. “The best therapy is one that is tailored to the individual, and centered on each person’s goals.”
At the Aphasia Clinic, speech-language pathologists conduct comprehensive speech and language evaluations to identify individual strengths to build upon, as well as impairment areas to target through therapy.
Dr. Turkeltaub evaluates each person’s brain images and medical records to determine the affected systems and the location and degree of damage that has occurred, as well as identify any other significant physical or emotional health issues that may be impacting communication—information that is important in developing an individualized treatment plan.
“I’m looking at the mechanism of the damage—the neurological aspects of aphasia. This will help us paint a more comprehensive picture of each person’s problem,” says Dr. Turkeltaub. “It’s fairly unique for people with aphasia to be evaluated by a cognitive neurologist,” he adds. “Most will be referred directly to speech-language pathologists. As a cognitive neurologist, I focus on disorders of thinking and bring a different perspective
to each person’s evaluation. I can sometimes offer additional options for treatment.”
Tailored, Goal-Oriented Treatment
The team reviews assessment results with each individual “who is at the center of decision-making,” says Fletcher. “The approach puts an emphasis on self-determination, allowing people with aphasia to identify their personal goals.”
A treatment plan may include one-on-one speech-language therapy targeting each client’s unique language challenges.
Continued from page 1
MedStar National Rehabilitation Network Aphasia Clinic
The hallmark of the clinic’s approach is its comprehensive language and medical evaluation of each participant.
Shaking the Stigma of AphasiaFor a disorder long recognized and discussed in medical literature, aphasia still gets no respect, says renowned speech-language pathologist Nancy Helm-Estabrooks, professor emerita at Western Carolina University, who spoke at a recent workshop on aphasia treatment held at MedStar NRH. “Aphasia slips through the cracks in medical school, and is misunderstood by many health professionals and the public,” adds Helm-Estabrooks, who worked with former Congresswoman Gabrielle Giffords after she suffered a critical gunshot wound to the head while conducting a Congress on Your Corner session in Tucson, Ariz., last year.
“My theory is that when you have a disorder that affects communication,
you can’t be your own advocate. So you become isolated and this isolation creates a domino effect that can wreak havoc on lives, of not just patients, but families, as well,” says Helm-Estabrooks.
The lack of understanding about aphasia has created a public awareness void—and some shame and stigma for people with aphasia, she explains. “Sometimes health providers will mislabel a person who has a deficit in language skills as someone with a cognitive disability. Of course, we know that aphasia isn’t a disorder of intelligence, but of communication.
“Still, I’m far more optimistic about the field today than I was 15 years ago.” New approaches to care that integrate
speech therapy with techniques that focus on life participation and self-determination are helping to bring aphasia out of the closet, Helm-Estabrooks adds.
“People with aphasia set priorities such as getting back to work—goals that are built into therapy. I think one-on-one therapy and life participation approaches are mutually beneficial,” she adds. “While this was once regarded with skepticism, we are seeing more combined programs, and that’s helping raise public awareness about aphasia, reduce the stigma and improve opportunities for continued recovery.”
Nancy Helm-Estabrooks
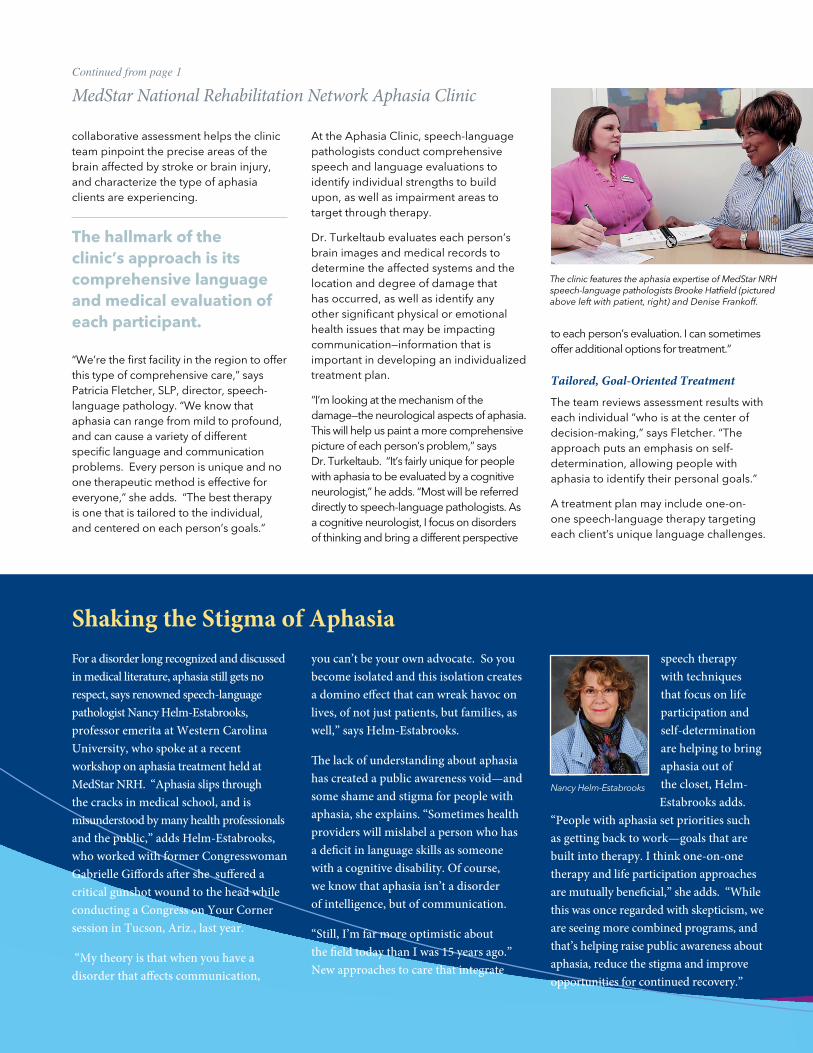
The clinic features the aphasia expertise of MedStar NRH speech-language pathologists Brooke Hatfield (pictured above left with patient, right) and Denise Frankoff.
“And because aphasia can also be very isolating for people, we focus on helping clients identify ways to reintegrate themselves into those activities that are important to their day-to-day quality of life,” she adds. “This may include participation in specialized groups to help them improve communication skills.”
The groups, which include everything from a book club to a computer lab group, give people with aphasia an opportunity to practice communication skills with other people who are experiencing the same issues. “They learn to use research-based strategies and tools to help them communicate more effectively—and this helps boost their confidence,” Fletcher says.
“In addition to traditional therapies and group activity, some people with aphasia may be candidates for medications now used to treat neurological disorders,” says Dr. Turkeltaub. “Other people with aphasia may be eligible to participate in clinical trials now underway at MedStar NRH,” he adds.
Clinical Research Opportunities
Dr. Turkeltaub is principal investigator for several clinical research studies testing new interventions to improve aphasia
recovery. He is a recent recipient of a 2012 Clinical Scientist Development Award from the Doris Duke Charitable Foundation for his groundbreaking work in brain plasticity and its role in reorganizing language following damage to the left hemisphere of the brain.
“One potential avenue of treatment involves an intervention to externally enhance left hemisphere activity, while inhibiting the right,” Dr. Turkeltaub explains. “We know that when the language areas of the brain are damaged, surrounding tissues in the left hemisphere and similar areas in the right hemisphere begin to assume responsibility for communication,” he says. “But there is some debate about whether all of this compensation is beneficial. The right hemisphere simply can’t do as effective a job as the left. We think if we can stimulate the left hemisphere, while inhibiting the right, we may be able to improve recovery.”
In a randomized, double-blinded clinical trial, Dr. Turkeltaub is evaluating the use of Transcranial Direct Current Stimulation (tDCS)—the application of small amounts of electrical current to modify brain function. “We apply safe, low-level constant electrical stimulation to the brain
MedStar NRH Aphasia Mentorship Program matches people living with aphasia with volunteer mentors who have been through the same experience and now have excellent communication skills.
Motor Speech Group utilizes therapies based on the latest research on motor learning for individuals with apraxia of speech, a condition that affects the motor planning abilities required for speech.
Dysarthria Group focuses on techniques to improve voice and speech for individuals with dysarthria, a condition in which the muscles of the mouth and face become weak, move slowly, or don’t move at all, causing distorted speech.
Augmentative and Alternative Communication Clinic provides assessment of appropriate augmentative and alternative (AAC) communication devices, including computer applications with speech output and mobile phone apps.
Support Groups provide support for stroke survivors, family and friends. The newly formed Spanish-Language Stroke Support Group provides education and support for stroke survivors and their caregivers whose primary language is Spanish.
To refer a patient for evaluation by the MedStar NRH Aphasia Clinic or for more information about services, call 202-877-1440.
Additional MedStar NRH Aphasia Services
A one-of-a-kind Aphasia Mentorship Program matches people living with aphasia with volunteers who have had the same experience and now have excellent communication skills.
New Dimensions • Fall 2012 3
through electrodes placed on the scalp,” he explains. “The current flows into the brain through the left hemisphere to stimulate brain cells, and moves out through the right, having the opposite effect and inhibiting brain activity.”
Study participants receive a baseline language assessment, and an optional MRI. Then over a five-day period, they receive speech therapy along with tDCS, or placebo stimulation. At the end of their five sessions, participants undergo another language assessment. Dr. Turkeltaub hopes to enroll 100 patients during the next three years—and ultimately test the procedure through a multi-center clinical trial.
He is also testing the value of transcranial magnetic stimulation (TMS) to inhibit the right hemisphere of the brain and improve language function in people with aphasia. In this study, Dr. Turkeltaub is evaluating TMS in people with differing locations of left hemisphere damage to determine if the technique is more beneficial for one subset of people with aphasia over another. “Our ultimate goal is to fine tune therapy, to provide the therapy that will produce the best result for each person,” Dr. Turkeltaub adds.

The language of sports is morphing, as well, moving away from labels such as “disabled and physically challenged” to the term adaptive athletes, explains Jason De Luigi, DO, director of sports medicine at MedStar NRH. Dr. De Luigi, an internationally recognized leader in adaptive sports, is medical director and head team physician for the U.S. Paralympic Alpine Ski Team, and was medical director of adaptive sports at Walter Reed National Military Medical Center.
MedStar NRH Leads the Way
“In 1960, when the first Paralympics was held in Rome, there were just 40 participants. Sports were not yet part of rehabilitation vernacular. But in the last 50 years, attitudes have been radically altered,” Dr. De Luigi says. “Athletic experiences are becoming routine, not just for a small cadre of elite adaptive athletes, but for all adults and children
who require some type of adaptive equipment to participate. And MedStar NRH has been on the ground floor of this movement. During the last 25 years, it has built one of the strongest adaptive sports programs in the country.”
MedStar NRH is the regional hub for adaptive sports experiences for adults and children. In 2008, it became one of the first Paralympic Sports Clubs in the U.S., and it serves as the D.C. Chapter of BlazeSports America. In addition,
MedStar NRH recently entered into partnership with the D.C. Veterans Health Administration Medical Center to provide handcycling experiences and training for their patients—a program that will likely expand to include other sports, as well.
“We began our program in 1986 with a wheelchair basketball team and now we offer five sports activities for children and adults—basketball, quad rugby,
tennis, sled hockey and handcycling,” says Joan Joyce, CTRS, HFS, coordinator of therapeutic recreation and director, Paralympic Sports Club, Washington, D.C.
“Our weekly sports clinics attract more than 60 athletes. Twice yearly, we hold sports clinics that feature nationally recognized Parathletes. And our teams play in regional and national tournaments. Last April, our nationally-ranked wheelchair basketball team made it to the finals of the National Wheelchair Basketball Association competition held in Denver.”
MedStar NRH also provides competitive opportunities for adaptive athletes through two signature events. The MedStar NRH Celebrating Heroes Triathlon—the first triathlon on the East Coast open to both able-bodied athletes and those using adaptive equipment—attracted more than 1,200 athletes to its first annual outing in June. And the annual Super H 5K Run, Walk & Wheel, now in its 9th year, has become one of the region’s most popular 5Ks. “These events provide athletes with highly competitive experiences, as well as raise funds to support our community program,” Joyce explains.
The Medical Benefit of Sports
“There was a time when exercise and sports involvement were considered dangerous for people with physical challenges,” says Dr. De Luigi. “Now we encourage sports to reduce risk for many secondary conditions, such as skin breakdown, osteoporosis, chronic pain, heart disease, high blood pressure, diabetes and obesity. We look for ways to achieve success within whatever physical constraints they may have.”
When nearly 4,300 Paralympic athletes gathered in London in September, they
stepped into a rapidly evolving competitive environment. Public perceptions
about “challenged athletes” are shifting dramatically—and the line between
athletes who use adaptive equipment and those who don’t is blurring. In August,
double-amputee Oscar Pistorius made history when he crossed that line,
competing with “able-bodied” runners in the 2012 Olympic Games.
Adaptive Athletes: Challenging Themselves and Perceptions
4 MedStar National Rehabilitation Network
Jason De Luigi, DO, (left) with Renie and Harry Freedman, founders of the Super H 5K Run, Walk & Wheel

New Dimensions • Fall 2012 5
There may be some special health issues to manage in the adaptive athlete, such as nerve entrapment, bone ossification, spasticity and autonomic dysreflexia, he explains. “But our research has also shown that adaptive athletes have relatively the same percentage of injuries as their able-bodied counterparts in similar sport activities.
“In fact, people with physical challenges require muscle strength, endurance and energy to perform routine tasks of daily living. Someone with a bilateral amputation, for example, expends 41 percent more energy ambulating than those of us with two limbs. Walking puts a great deal of stress on the heart, so aerobic capacity becomes that much more important.”
This is a lesson the military learned early on, Dr. De Luigi says. “Sports medicine experts are at the bedside of wounded warriors at the very start of acute care. This is increasingly becoming the case outside of the military, as well.”
“At MedStar NRH, all inpatients are introduced to sports activity during their hospitalization,” says Joyce. “Our physicians encourage patients to participate.”
The military has also led the way in the development of adaptive sports technology. “Members of the military and veterans have access to the vast variety of adaptive devices, often prototypes
developed with Department of Defense support. This is a very robust—and expanding—industry,” he adds. “But for the average family, cost of this equipment can be a real deterrent to sports involvement.”
MedStar NRH depends on donations and fundraising events to support its sports program, which is free for participants, and to fund its Adaptive Equipment Lending Library, which loans equipment to patients. “But it is concerning that the cost of increasingly sophisticated technology may become a barrier for participation,” Dr. De Luigi adds.
Still, expansion of Paralympics’ competition and other adaptive athletic programs is likely to continue, Dr. De Luigi explains. As adaptive athletes become more visible, adaptive sports are moving from an “outlier” activity into the mainstream. Even the meaning behind the word Paralympics has evolved over time. “When it was originated, the word was a pun combining ‘paraplegic’ and ‘Olympic,’” Dr. De Luigi adds. “Today ‘para’ stands for the Greek word meaning ‘beside or alongside.’ It recognizes that now the Paralympics parallel the Olympics—equal in value and importance.”
Learn more about the Adaptive Sports Program at medstarnrh.org. For patient referral, contact Dr. De Luigi at 202-877-1621.
“During the last 25 years, MedStar NRH has built one of the strongest adaptive sports programs in the country.” — Jason De Luigi, DO

New information about the dangers of concussion has thrust the issue into
the national spotlight. And government, organized sports, school systems
and healthcare institutions have responded in kind. Measures to decrease the health
impact of mild traumatic brain injury have made their way into legislation, school
and collegiate sports’ practices, and professional athletics. Yet the problem persists.
An estimated 2 million people suffer from concussions every year, and nearly 500,000 of them are children. Because these injuries rarely appear on routine scans, many people go undiagnosed and a brain injury expert never performs an appropriate evaluation until persistent symptoms disrupt a patient’s life, explains Michael Yochelson, MD, MBA, vice president for medical affairs and chief medical officer of the MedStar National Rehabilitation Network.
“We understand now that we need to approach concussion prevention, diagnosis and treatment on multiple
fronts,” he says. “For health care providers, that means developing a continuum of services and a collaborative strategy to deal with the issue. That’s why we have expanded our concussion services to include a more comprehensive MedStar NRH Network Concussion Program, which includes a partnership with Children’s National Medical Center, and participation in the MedStar Sports Medicine Concussion Network’s regional approach to concussion care. This expansion includes research, education and patient advocacy, as well as clinical services.”
Creating the Baseline
While headlines about serious neurological damage—and even death—from repeated concussions have fueled positive action across the country, researchers have well understood the adverse affects of concussion for more than a decade.
Studies conducted in the early 1990s by Joseph Bleiberg, PhD, former director of the Center for Cognitive Neuroscience at MedStar NRH, were among those early critical investigations that clarified the impact of mild brain injury in sports, and helped define concussion management. Dr. Bleiberg was also a pioneer in the development of computerized neuropsychological assessments, which are now widely used in the military and elsewhere.
Baseline cognitive and neurological assessments of athletes are becoming more commonplace in school athletic departments, national professional leagues and the Department of Defense. At MedStar NRH, many of the athletes seen have been baselined with the ImPACT battery, explains William Garmoe, PhD, ABPP-CN, coordinator of neuropsychology services. “We often can easily access baseline-screening scores, and compare the results with post-concussion scores. It’s one tool among many that we use in evaluating symptoms and the recovery process.”
New laws in the District of Columbia, Maryland and elsewhere in the country have helped increase implementation of baseline testing, Dr. Garmoe explains. “Today in many jurisdictions before athletes can return to club or school sports after a concussion, they must receive medical clearance,” he says. “Comparative cognitive screening can help us evaluate a patient’s condition. Still, many individuals we see, especially adults, have not had baseline testing. But this doesn’t impede our ability to effectively manage the recovery process.”
6 MedStar National Rehabilitation Network
Tackling Mild TBI Head On: Introducing the MedStar NRH Network Concussion Program
Young athletes are among those people at higher risk for concussion.

MedStAR NRH NetwoRk CoNCuSSioN PRogRAM in Brief
n Assessment by a physician and/or neuropsychologist (at some sites, other trained healthcare professionals will complete the assessment)
n Complete concussion evaluation including
— Neurologic examination — Balance testing — Review of medications — Neuropsychological assessment — For athletes, if patients had a
previous screening with ImPACT the team may repeat testing
n Development of a treatment plan, which may include referrals for rehabilitation treatments or further medical consultations
n Recommendations regarding: — Return to school, sports and/or work — Accommodations for school or
work, if appropriate — Follow-up care during recovery period — Referral to further treatment, if
appropriate
Services
William Garmoe, PhD, ABPP-CN, coor-dinator of neuropsy-chology services
Michael Yochelson, MD, MBA, vice president for medi-cal affairs and chief medical officer of the MedStar National Rehabilita-tion Network
Leadership
New Dimensions • Fall 2012 7
Earlier Assessment and Treatment
Getting patients appropriately and promptly diagnosed with concussion is the hurdle, says Dr. Yochelson.
“We know that delay in diagnosis and treatment can lead to long-term physical, psychological and cognitive impairments, and increased risk for a more serious repeat concussion.
“Therefore, we are reaching out to schools, ER docs, trainers, teachers and parents to alert them to signs and symptoms. We want them to understand that not everyone who has a concussion loses consciousness, and that concussion can occur from a direct blow to the head, as well as from the force of a blow to the body.
“We are also encouraging people to call our Concussion Clinic at 202-877-1955 to facilitate assessments. Our relationship with the SCORE Concussion Program at Children’s National Medical Center helps patients get the most appropriate treatment available. Our colleagues at Children’s National refer older adolescents to the MedStar NRH Concussion Clinic, and we refer younger patients to the SCORE program. In some cases, we confer with one another.”
Interdisciplinary Team
At MedStar NRH, highly experienced physiatrists, neurologists and neuropsychologists, with specialized training in brain injury, lead the concussion program team. “Because there is often no evidence of concussion on typical imaging, we must depend on a clinical diagnosis. We use a comprehensive assessment that includes a complete medical history, clinical and neurologic exams, and neuropsychological review.
“We have found that these patients can really benefit from an organized therapeutic approach to help relieve symptoms,” says Dr. Yochelson. “An individualized treatment plan may include medical management of symptoms such as headaches, dizziness, sleep disorders and fatigue,” he explains. “It may also include physical or occupational therapy or both. We have expanded the program to a number of our network’s outpatient centers, which are now staffed by physical therapists with experience in concussion so that our patients can continue therapy close to home.”
If patients are experiencing behavioral or cognitive problems, they will be treated by one of the team’s eight neuropsychologists or neuropsychiatrist. “Even mild brain injury can cause changes in mood and cognitive abilities,” Dr. Garmoe says. “These effects can be subtle, and can result from both the direct effects of concussion, as well as secondary effects such as psychological reactions to injury, pain, and stress.
“There is a great deal of misinformation about concussion out there now, and one part of our job in rehabilitation is to reassure patients that they will ultimately recover. We’ve also developed a booklet called “Recovering from a Concussion: Information and Practical Suggestions,” to help patients and parents of children with concussion deal with the recovery process.”
“The good news in concussion is that we are seeing patients earlier in their course of recovery,” Dr. Yochelson says. “Continued education and awareness of the issue is necessary because the culture of ‘playing hard’ in sports isn’t likely to change. But I think we are making inroads in alleviating the more devastating effects of concussion.”
“We understand now that we need to approach concussion prevention, diagnosis and treatment on multiple fronts.” — Michael Yochelson, MD, MBA
For scheduling appointments at the MedStar NRH Concussion Clinic, call 202-877-1955.

8 MedStar National Rehabilitation Network
NoteWorthyRising in Rank—MedStar NRH One of the Nation’s Best For the 18th consecutive year, physicians have ranked
MedStar National Rehabilitation Hospital as one of the
top rehabilitation hospitals in the country in the annual
survey published in U.S. News & World Report.
Southern Maryland Hospital Center Joins MedStar HealthThis past July, MedStar Health announced that Southern Maryland Hospital Center (SMHC), located in Clinton, Maryland, will become the newest member of the regional health care system. MedStar NRH has been a member of the system since it was first launched. SMHC will be MedStar’s 10th hospital and its 7th in the state of Maryland.
Southern Maryland Hospital Center serves Prince George’s County and the Southern Maryland peninsula. It was founded by Dr. Francis P. Chiaramonte 35 years ago, and today is a thriving, 238-bed acute care medical center, providing more than 17,000 inpatient admissions and 65,000 emergency visits annually.
Peter E. Turkeltaub, MD, PhD, Receives Prestigious Doris Duke GrantPeter E. Turkeltaub MD, PhD, received a 2012 Clinical Scientist Development Award from the Doris Duke
Charitable Foundation. The highly competitive grant, totaling $486,000 over three years, supports junior physician-scientists as they transition to independence as clinical researchers. Dr. Turkeltaub is a member of the Center for Brain Plasticity and Recovery, a joint program of Georgetown University
Medical Center (GUMC) and MedStar National Rehabilitation Network that focuses on the study of neural plasticity. He is also assistant professor in the Department of Neurology at GUMC, and director of the Aphasia Clinic at MedStar NRH. His research focuses on brain plasticity and recovery following a stroke, in particular on aphasia, damage in the left hemisphere responsible for language comprehension and speech. [See page 3 for more about Dr. Turkeltaub’s research.]
New Medical StaffJustin Burton, MD, joins the MedStar NRH team as co- director of inpatient pediatric rehabilitation for the National Center for Children’s Rehabilitation at MedStar NRH. Dr.
Burton completed a fellowship in pediatric rehabilitation at Northwestern University Feinberg School of Medicine this year, and his residency in PM&R at the Rehabilitation Institute of Chicago.
Marilyn F. Kraus, MD, joins the MedStar NRH team as program director of the Brain Injury Medicine Fellowship. Dr. Kraus is a neuropsychiatrist who has specialized in the treatment
of patients with traumatic brain injury for more than 20 years. Her research has focused on assessment of neuropathology and neurobehavioral/cognitive function, as well as the role of neuropharmacology in the management of TBI. A graduate of Tulane School of Medicine, Dr. Kraus completed her residency training at Tulane, and fellowships at both Baylor School of Medicine and Johns Hopkins University. Prior to her appointment to the medical staff, Dr. Kraus was medical director of the Traumatic Brain Injury Consult team of the inpatient acute trauma service at Walter Reed National Military Medical Center in Bethesda, Maryland.
The magazine also listed MedStar NRH among the best overall hospitals in the Washington, D.C., region—rising in rank from number four in 2011 to number three this year out of 59 acute care hospitals in the Washington metropolitan region, which includes D.C., Alexandria and Arlington County, Virginia, and Bethesda and Rockville, Maryland.
The magazine recognized just 732 facilities in the U.S. as Best Regional Hospitals from nearly 4,800 hospitals reviewed. The magazine also listed MedStar Washington Hospital Center and MedStar Georgetown University Hospital among the top five ‘best’ regional hospitals in the metropolitan area.
“We are very proud to be recognized by our peers in the medical community for our efforts in providing our patients with high quality health care,” says Michael Yochelson, MD, MedStar NRH vice president of medical affairs and chief medical officer. “This ranking is a testament to the dedication, commitment and experience of our Team Members in the MedStar NRH Network, as well as the support of our community,” he adds. “This recognition inspires us to continue to provide our patients with compassionate care and innovative programs and techniques, which will empower them to lead productive, independent lives.”

New Dimensions • Fall 2012 9
Edna S. Beginning in the early 1980s, patients who had experienced paralytic poliomyelitis decades earlier were beginning to complain of new symptoms, such as unexpected weakness, fatigue and pain. In response to these complaints, several therapists and I at The Institute for Rehabilitation and Research (TIRR) in Houston started a post-polio clinic in 1984. However, none of us was prepared for the multiplicity of medical, functional and psychosocial issues that these individuals were facing. As a result of our inexperience and failure to understand the best way to address these challenges, the clinic drifted, unanchored to a clear vision. Fortunately, all of this changed when I came to Washington. Ed Eckenhoff and John Goldschmidt, MD, had the wisdom to give an interdisciplinary group of clinicians and me the freedom to meet weekly for several months to plan how to organize a comprehensive, innnovative outpatient team to address the multiple needs of these individuals.
Ms. S. was one of the first of several thousand patients who eventually came to the MedStar NRH Post-Polio Clinic from around this country and abroad. She had polio when she was six years old and was in a rehabilitation hospital
for seven months, undergoing three reconstructive orthopaedic surgeries that made it possible for her to walk without the use of assistive devices. Ms. S. had a successful career as a real estate lawyer and with her husband raised two daughters. In 1983, at the age of 42, she began to experience intense generalized fatigue and progressive new weakness in both legs--symptoms that we now recognize as characteristic of post-polio syndrome. Because of the unexpected and inexplicable changes in her health, she took an early retirement. A few years later, in 1987, she was referred to our clinic. Her response to our recommendations was almost miraculous, and not unusual, as we discovered over the years. In addition to other interventions, she started using powered mobility, obtained hand controls for her car and moved to a one-story home. Within two years, she had stopped taking antidepressants and felt strong enough to return to work.
Michael R. Michael had just turned 18 when he sustained a T2 spinal cord injury (SCI) in a motor vehicle accident. He had a girlfriend from high school, but within a short time she left him. We followed him in the outpatient clinic for several years and then one day he
returned for a follow-up visit with Rebecca, his fiancée. Not only did they want to get married, but they wanted to have children! While still at TIRR, Stephen Seager, DVM, a veterinarian from Ireland, and I had been developing a method to obtain semen in anejaculatory men with SCI using rectal probe stimulation. In 1988 we started the Male SCI Fertility Program at MedStar NRH and were looking for couples like Michael and Rebecca. Working with fertility specialists from Shady Grove Fertility Center, we were able to harvest Michael’s sperm and within several months had our first pregnancy. Nine months later a healthy baby boy was born, which helped change forever the future for men with SCI who wanted to have biologic children. Eventually, several dozen babies were born through this program!
Hugh G. Hugh was a friend I met during college. He had respiratory polio as a teenager and used a wheelchair full-time for mobility. He took a graduate degree at Oxford, was a celebrated author and a savant of Capitol Hill politics. In all, probably the brightest person I’ve known. We drifted apart after college, but reconnected when he came to the post-polio clinic one day in the late 1980s. His day job had been legislative assistant for Sen. Bob Bartlett from Alaska and by night he wrote a series of books on Alaskan statehood, the Senate and, finally, a biography of Franklin Delano Roosevelt, which described for the first time the impact polio had on shaping Roosevelt’s personality and presidency. While Hugh was finishing the Roosevelt book, he introduced me to Art Brown who had a publishing firm in Northern Virginia. During that meeting, the idea of a hospital press was born. I mentioned it to Rob Hartmann who became an enthusiastic advocate and the following year MedStar NRH Press published its first volume, Managing Post-Polio. Since then, there have been four additions to the MedStar NRH Press library, including a second edition of the polio book.
Thank you MedStar NRH, for adding joy to my life, and to the lives of countless others.
Of the many wonderful memories I have from my 26 years at MedStar NRH,
here are three along with the patients who helped inspire them.
Adding Joy to Life By Lauro S. Halstead, MD, MPH
Colleagues Edward Healton, MD, MPH, (left) and John Rockwood (right) and former patients bade a heartfelt farewell to Lauro Halstead, MD, MPH, upon his retirement. Dr. Halstead, an internationally respected post-polio pioneer, joined the MedStar NRH staff when it opened its doors in 1986, and wore many hats during the years that followed, including director of the SCI program, the post-polio program, the research center and fertility clinic.

10 MedStar National Rehabilitation Network
Update from the Christoph Ruesch Research Center
Metagenomics—Pathway to Earlier Diagnosis and Treatment of UTI in SCI?
In this pilot study, researchers collected urine from 26 healthy control subjects, and 27 healthy subjects at risk for ABU because of spinal cord injury-related neuropathic bladder (NB). Of these 27 at-risk patients, eight voided normally, eight utilized intermittent catheterization, and 11 utilized indwelling urethral catheterization for bladder drainage.
“We performed urinalysis, urine culture and 16S rDNA sequencing on all samples,” Dr. Groah explains.
Surprising Results
“The findings have been dramatic,” Dr. Groah says. “We found that conventional medical wisdom is incorrect: Healthy urine isn’t sterile. The healthy urine microbiome of the control group consisted of a great deal of bacteria. We also found that the urine microbiome differs by gender: Lactobacillales are found in abundance in women; corynebacterium is found in large quantities in men.
“But the microbiome of the urine of the healthy SCI group was very different,” she adds. “It was characterized by a great deal of virulent bacteria.” There were also differences in urinary microbiome based on the type of bladder management used by the healthy SCI subjects, the type of catheter used, and the duration of catheter use.
Researchers found very little corynebacterium in the urine of healthy men in the SCI group. Results also show the presence of microorganisms, such as enterobacteriales, in these subjects. In healthy women with SCI, lactobacillales were far less abundant than in the control group.
The personal and financial burden of
urinary tract infection (UTI) is well-
recognized. With annual medical
costs of nearly $1 billion, it is the
most common urologic disorder seen
in outpatient settings and the most
common healthcare associated infection.
But the burden for people with spinal cord injury is greater still. They suffer with UTI at a rate 30 times that of the general population—it is the number one complication among SCI patients. In this population, UTI is more likely to lead to other systemic and more serious infections and complications. In spinal cord injured men and women, a simple UTI can become a fatal event.
“The majority of people with spinal cord injury have impaired bladder function and also use some type of catheter for bladder management,” explains Suzanne Groah, MD, director of MedStar NRH
spinal cord injury research and associate professor of rehabilitation medicine at Georgetown University. “As a result, they are at very high risk for both urinary tract infection, as well as asymptomatic bacteriuria (ABU), in which bacteria are present in the urine but patients are asymptomatic.
“Differentiating ABU from UTI is very challenging,” she explains. “But it is also very critical because overtreatment of ABU can perpetuate antimicrobial resistance, while under treatment of UTI can result in increased morbidity and mortality.
“Diagnostic testing by use of urine culture is dependent on growing bacteria that we have already identified, and can take from 48 to 72 hours,” Dr. Groah adds. “That kind of delay in treatment is dangerous. We simply need a better diagnostic tool. And metagenomics has opened up a promising window for exploration.”
First-of-its-Kind Study
Advances in DNA sequencing technologies have created the burgeoning field of metagenomics—the comprehensive examination of microbial communities, including those that can’t be grown in a laboratory. The National Institutes of Health’s Human Microbiome Project is one of several international efforts now underway to characterize the human microbiota and analyze their role in human health and disease.
Now for the first time, researchers at MedStar NRH have characterized the urine microbiome of people with spinal cord injury.
“We hope to use this wealth of information to ultimately create a more effective diagnostic measure of ABU and UTI,” Dr. Groah explains. “Our goal is to identify a bacterial signature in urine that alerts us that a UTI is very likely to occur so we can begin treatment as soon as symptoms appear.
“We collaborated with Children’s National Medical Center and the J. Craig Venter Institute, which have the very sophisticated computational tools and expertise needed to perform comprehensive metagenomic analysis, to conduct a cross-sectional study of 56 subjects,” she adds.
“We found that conventional medical wisdom is incorrect: Healthy urine isn’t sterile.” — Suzanne Groah, MD
Suzanne Groah, MD
“Our goal is to identify a bacterial signature in urine to alert us that a UTI is very likely to occur so we can begin treatment even before symptoms appear.” — Suzanne Groah, MD

“The findings suggest that either increased exposure to a urinary catheter and/or increased severity of neuropathic bladder can influence the ability of lactobacillus to colonize the urinary tract of women with spinal cord injury-related neuropathic bladder,” Dr. Groah says. “And enterobacteriales may be potential indicators of future urinary tract infection in men with SCI.”
Future Implications
While this is preliminary research, the implications of its findings are enormous for the SCI and general population. “First we confirmed earlier research that reputed the commonly held clinical belief that healthy urine is sterile,” she explains.
“Our findings also suggest that corynebacterium may contribute to a healthy urine microbiome in men; and that lactobacillus plays a role in a healthy urine microbiome in women,” Dr. Groah says.
Does this mean that supplementation with probiotics will help prevent urinary infection in women with neuropathic bladder? Will metagenomic analysis of urine for both “good and bad” bacteria become the standard for early detection of UTI?
“It’s too early to tell,” she says. “There is so much more data to gather before a tool for early diagnosis can be developed and tested. Our next step is to study a larger control group for a better understanding of the microbiome of healthy urine.
“But there is no doubt that the new field of metagenomics will have a tremendous effect on public health. For the SCI population, we can envision a future in which a quick and easy urine check will test for infection in just minutes or hours, not days.
“We could one day be able to develop devices for quick diagnoses that are compact. Instead of costing millions of dollars, a device could be produced cheaply enough to make it affordable for routine clinical use, perhaps even so user-friendly that it will be available for home use,” Dr. Groah explains. “And that kind of diagnostic innovation could save lives and money.”
New Dimensions • Fall 2012 11
To Learn More
Check out the recently published article, “Integrated next-generation sequencing of 16S rDNA and metaproteomics differentiate the healthy urine microbiome from asymptomatic bacteriuria in neuropathic bladder associated with spinal cord injury,” in the Journal of Translational Medicine 2012, 10:174 doi: 10.1186/1479-5876-10-174. Also available online: http://www.translational-medicine.com/content/10/1/174.
This chart shows the differences in relative bacterial OTU counts between neuropathic and healthy bladder in males and females. For every individual, the OTU counts were normalized to the individual's total OTU count.

MedStar National Rehabilitation Network 102 Irving Street NWWashington, D.C. 20010-2949202-877-1000medstarnrh.org
James V. Reyes, Chairman, Board of Directors John D. Rockwood, PresidentMichael Yochelson, MD, Vice President and Chief Medical Officer Kenneth A. Samet, FACHE, President and CEO, MedStar Health
New Dimensions is published by Marketing & Strategic DevelopmentRobert S. Hartmann, Vice President Emily R. Turk, Writer-Editor
MedStar NRH is accredited by:
CARF, the Commission on Accreditation of Rehabilitation Facilities
The Joint Commision
ELECTRONIC SERVICE REqUESTED
Become a Fan on Facebook
Connect to uson YouTube
Follow uson Twitter
We are proud that 13 posters and five presentations featuring our residents’ research will be showcased at the meeting, and that several sessions will feature members of our medical staff and residents. I hope you will make special note of these presentations.
I will join my fellow MedStar NRH Team Members on Friday, November 16, from 11 a.m. to 12:30 p.m., for a workshop for residents called “Techniques for
Managing Physical Agitation in the Patient with Brain Injury.” Jason De Luigi, DO, will participate in the educational program “Adaptive Sports Medicine: The Adaptive Athlete, Advances in Adaptive Technology, and Unique Challenges in Regulating Competition” on Sunday, November 18, from 8 to 9:30 a.m.
Gerben DeJong, PhD, will be among presenters on Friday, November 16, from 1:45 to 3:15 p.m., discussing
“The Changing Role of the Rehab Physician in New Delivery System Models.” On Saturday, November 17, from 4 to 5:30 p.m., Dr. Dejong, Christopher Karam, MD, and Cherry Junn, MD, will participate in a panel on “Re-hospitalization following Traumatic Spinal Cord Injury in the First Year following Discharge from Medical Rehabilitation.”
Hope to see you in Atlanta!
Connect to MedStar NRH at medstarnrh.org.
quick Referral to MedStar NRH Expertise Inpatient care: 202-877-1152 • Day treatment: 202-877-1945 • Outpatient services: 202-877-1621
NON-PROFIT ORG.U.S. POSTAGE
PAIDLUTH/TIM, MD
PERMIT NO. 550
It’s time again to network with our colleagues and share innovations in clinical practice
and research at the upcoming AAPM&R Annual Assembly Meeting in Atlanta. I want
to invite you to stop by MedStar NRH booth #301 in the Exhibit Hall, and attend our
MedStar NRH Alumni & Friends Reunion on Friday, November 16, from 7 p.m. to 9 p.m.,
in International 2 at the Atlanta Marriott Marquis.
MedStar NRH Perspectives Michael Yochelson, MD, MBA, VP of Medical Affairs and Chief Medical Officer