neuroradiology of hemorrhagic...
TRANSCRIPT
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
NeuroradiologyNeuroradiology
of Hemorrhagic of Hemorrhagic StrokeStroke
W. Taylor KimberlyHarvard Medical School Year 4
Gillian Lieberman, MD
July 2003
2
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Goals
1. Mechanisms of stroke
2. What neuroimaging
modalities are available
4. Patient presentation to illustrate the decision algorithm for workup of one type of stroke
3. Uses for neuroimaging
modalities
3
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Stroke pathogenesisIschemic stroke (80%) The deficits adhere to vessel territories.
Embolic:
usually cardiogenic
in origin, less commonly artery-to-artery.
Thrombotic:
caused by HTN, arteritides.
Hemorrhagic stroke (20%)Intraparenchymal
hemorrhage:
causes include HTN, trauma, cocaine.Gradual onset, with neurologic findings that may cross vessel territories.
Subarachnoid hemorrhage:
causes include arterial aneurysm and AVM.Sudden onset, excruciating headache and changes in mental status.
Rapid diagnosis and intervention is critical for preservation of
brain function.
4
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Menu of testsHead CT
●
quick ●
sensitive for hemorrhage●
I+ contrast to visualize vascular anatomy●
but cannot detect acute infarction < about 8 hrs old first sign is loss of gray-white differentiation, sulcal
effacementthen decreased attenuation
Brain MR● excellent visualization of anatomy ● sensitive to acute infarct (T2, FLAIR and DWI/ADC sequences) ● can see vessel flow with MRA (better with gadolinium contrast) ● but very slow to acquire images● does not provide vessel anatomy (will overcall tight stenoses)
Cerebral Angiogram● excellent vascular anatomy● permits interventions (clot retrieval, targeted t-PA administration,
coil embolization)
5
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
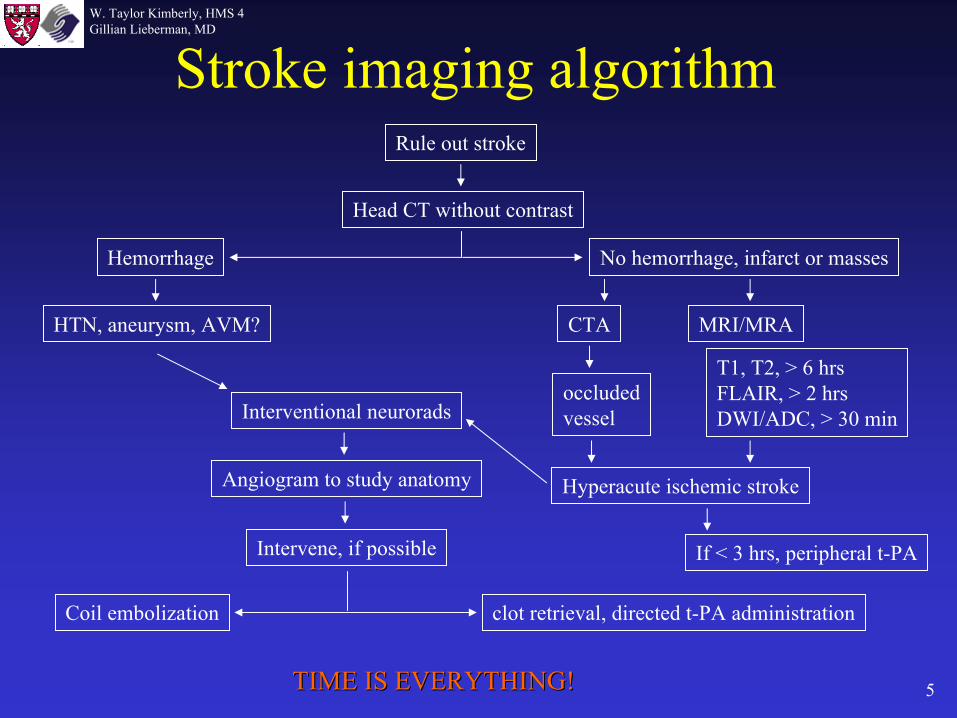
Stroke imaging algorithmRule out stroke
Head CT without contrast
Hemorrhage No hemorrhage, infarct or masses
CTA MRI/MRA
T1, T2, > 6 hrs FLAIR, > 2 hrsDWI/ADC, > 30 min
Angiogram to study anatomy Hyperacute
ischemic stroke
HTN, aneurysm, AVM?
Intervene, if possible If < 3 hrs, peripheral t-PA
TIME IS EVERYTHING!TIME IS EVERYTHING!
Interventional neuroradsoccludedvessel
clot retrieval, directed t-PA administrationCoil embolization
6
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Patient Presentation
J. B. is a 63 year old right-handed female who presents with:-
sudden onset of headache
-
left sided weakness-
rapidly diminishing mental status
What imaging test would you perform first?

7
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Normal neuroanatomy
temporal lobe
cerebellum
pons
frontal lobe
Sylvian
fissure
basal ganglia
corpus callosum
septum pellucidum
caudate nucleuslentiform
nucleus
lateral ventricles
internal capsulethalamus
superior colliculi
falx
cerebri
occipital lobe
gray matter
white matter
Images from BIDMC
8
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Images from BIDMC
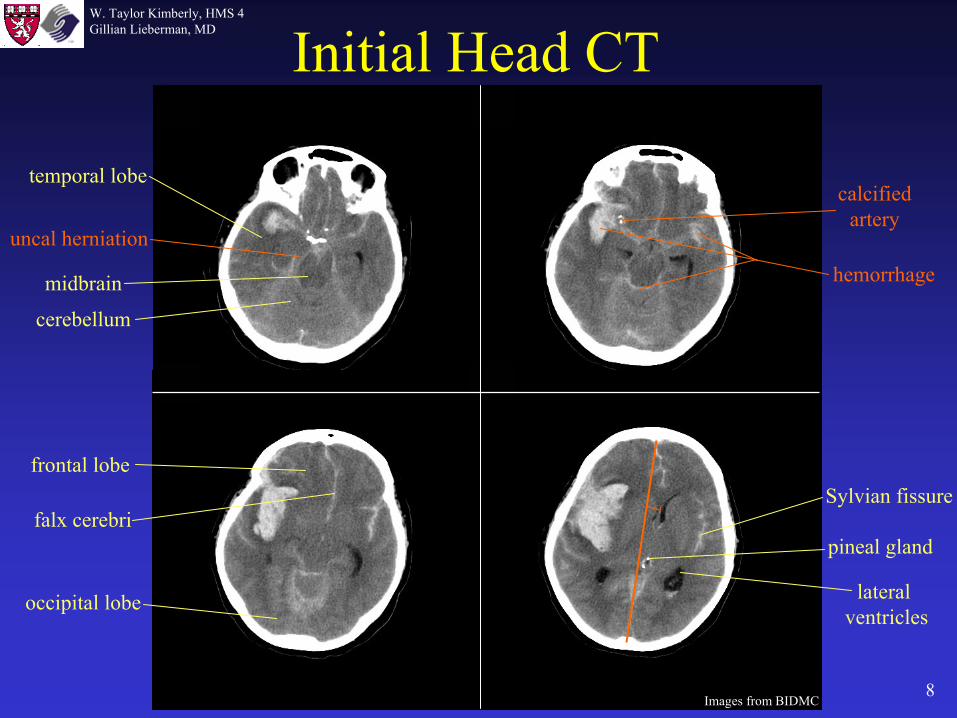
Initial Head CT
temporal lobe
cerebellum
midbrain
falx
cerebriSylvian
fissure
lateral ventricles
pineal gland
occipital lobe
frontal lobe
calcifiedartery
hemorrhage
uncal
herniation

9
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Images from BIDMC
calcified choroid plexus
internal capsule
thalamus
septum pellucidum
corpus callosum
caudate nucleus
lentiform
nucleus
frontal lobe
parietal lobe
occipital lobe
intraparenchymalhemorrhage
Sulci
(withsubarachnoid hemorrhage)
midline shift
Initial Head CT

10
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
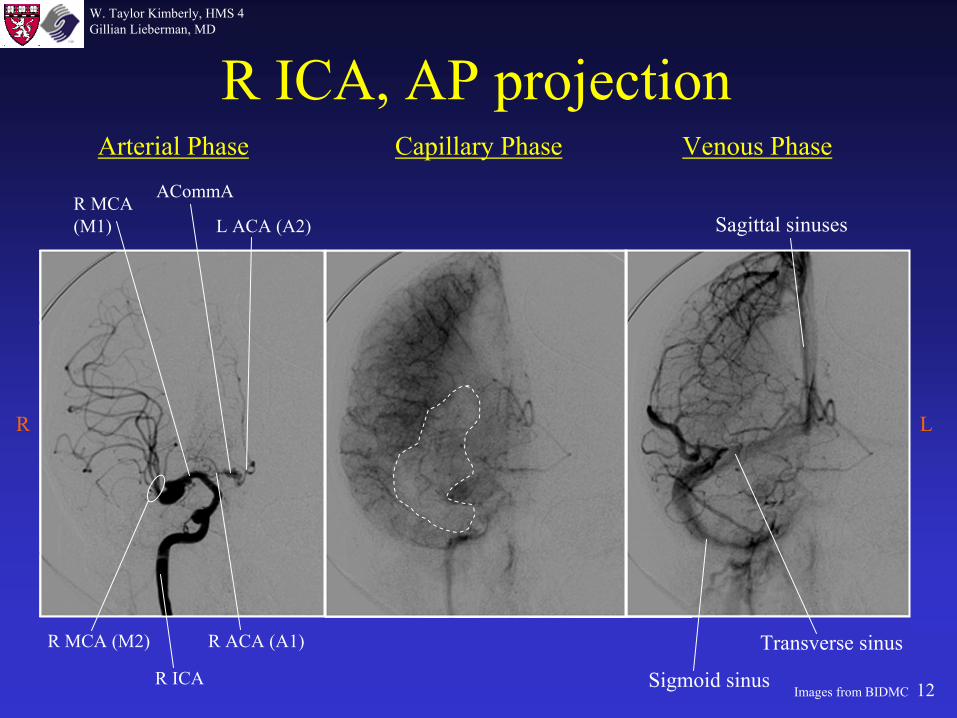
Arterial Phase Capillary Phase Venous Phase
L ICA, AP projection
L ICA
L MCA(M1)
L ACA (A1)
ACommA L ACA (A2)
L MCA (M2)
Sigmoid sinus
Transverse sinus
Sagittal
sinuses
R L
Images from BIDMC
11
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
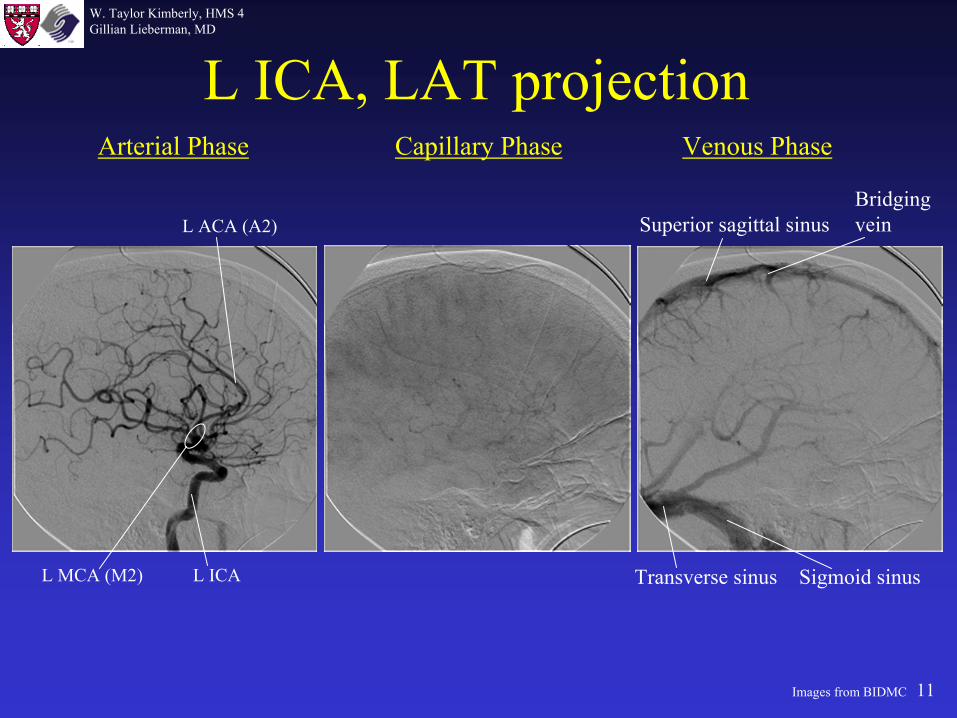
Arterial Phase Capillary Phase Venous Phase
L ICA, LAT projection
L ICA
L ACA (A2)
L MCA (M2) Sigmoid sinusTransverse sinus
Superior sagittal
sinusBridgingvein
Images from BIDMC
12
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
R ICA
R MCA(M1)
R ACA (A1)
ACommA
L ACA (A2)
R MCA (M2)
Arterial Phase Capillary Phase Venous Phase
Sigmoid sinus
Transverse sinus
Sagittal
sinuses
R ICA, AP projection
R L
Images from BIDMC

13
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Arterial Phase Capillary Phase Venous Phase
R ICA, LAT projection
R ICA
L ACA (A2)
R MCA (M2) Sigmoid sinusTransverse sinus
Superior sagittal
sinusBridgingvein
Images from BIDMC
14
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
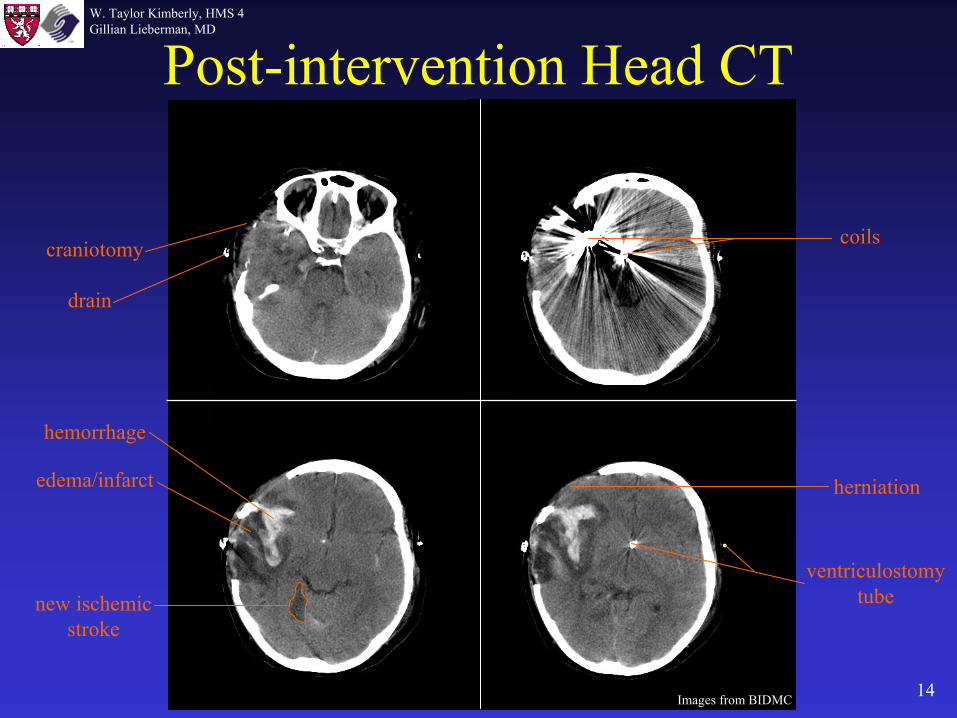
Post-intervention Head CT
Images from BIDMC
coilscraniotomy
herniation
ventriculostomy
tube
hemorrhage
edema/infarct
drain
new ischemic stroke
15
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Images from BIDMC
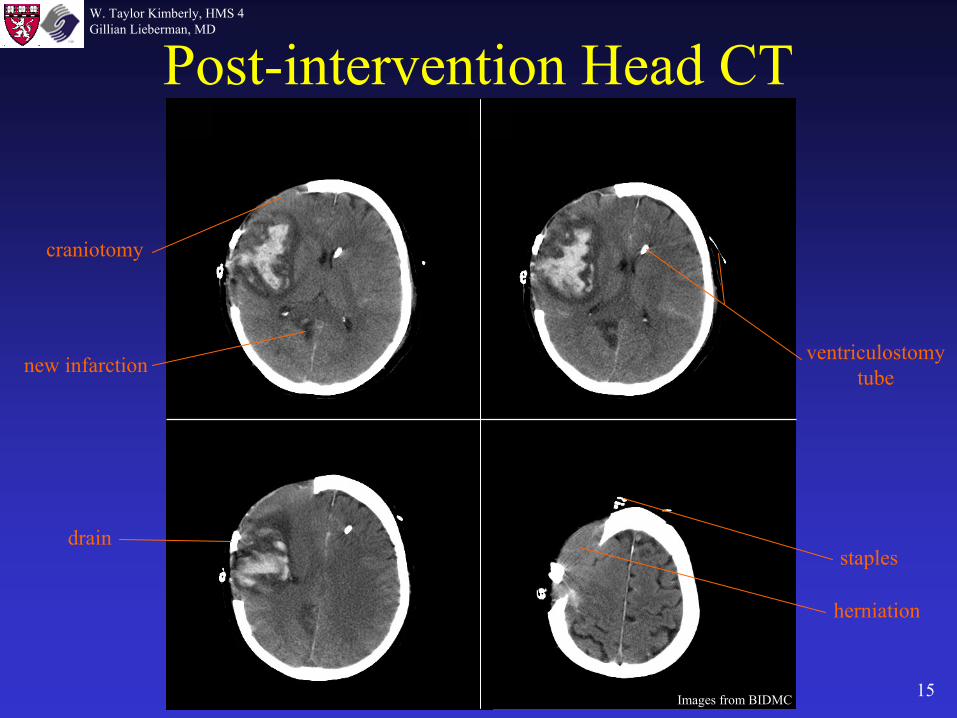
Post-intervention Head CT
craniotomy
ventriculostomy
tube
drainstaples
herniation
new infarction
16
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Summary
Hemorrhage appears as high attenuation regions on CT.
Rapid diagnosis and intervention is critical in stroke patients.
Head CT is the first line imaging in all suspected stroke patients.
Interventional neuroradiology
can offer interventions that minimize bleeding or rebleeding.
Head CT can also detect masses and infarcts > 8-12 hrs old.
17
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
References
•
Hanaway J, Woolsey TA, Gado MH, Roberts MP. The Brain Atlas: A visual guide to the human central nervous system. Bethesda: Fitzgerald Science Press. 1998.
•
Fix JD. High-Yield Neuroanatomy. Philadelphia: Williams & Wilkins. 1995.
•
Flaherty, AW. The Massachusetts General Hospital Handbook of Neurology. Philadelphia: Lippincott Williams & Wilkins. 2000.
•
Novelline RA. Squire’s Fundamentals of Radiology. Cambridge: Harvard University Press. 1997.
18
W. Taylor Kimberly, HMS 4Gillian Lieberman, MD
Acknowledgments
Larry Barbaras Gillian Lieberman, MDPamela Lepkowski