neurobiology of schizophrenia
TRANSCRIPT

NEUROBIOLOGY OF SCHIZOPHRENIAStudent – Dr. Mayuri Mohanty, Dept of Psychiatry, Bharati Hospital

Contents• Introduction• Neuropathology- Macroscopic changes- Functional changes • Neurochemistry- Dopamine- Serotonin- GABA- Glutamate• Genetics• Neurobiological models

Introduction• Schizophrenia actually refers to a group of disorders. There is not
one essential symptom that must be present for a diagnosis. Instead,
patients experience different combinations of the main symptoms of
schizophrenia.
• Subtypes
- Paranoid Type
- Disorganized Type
- Catatonic Type
- Undifferentiated Type
- Residual Type


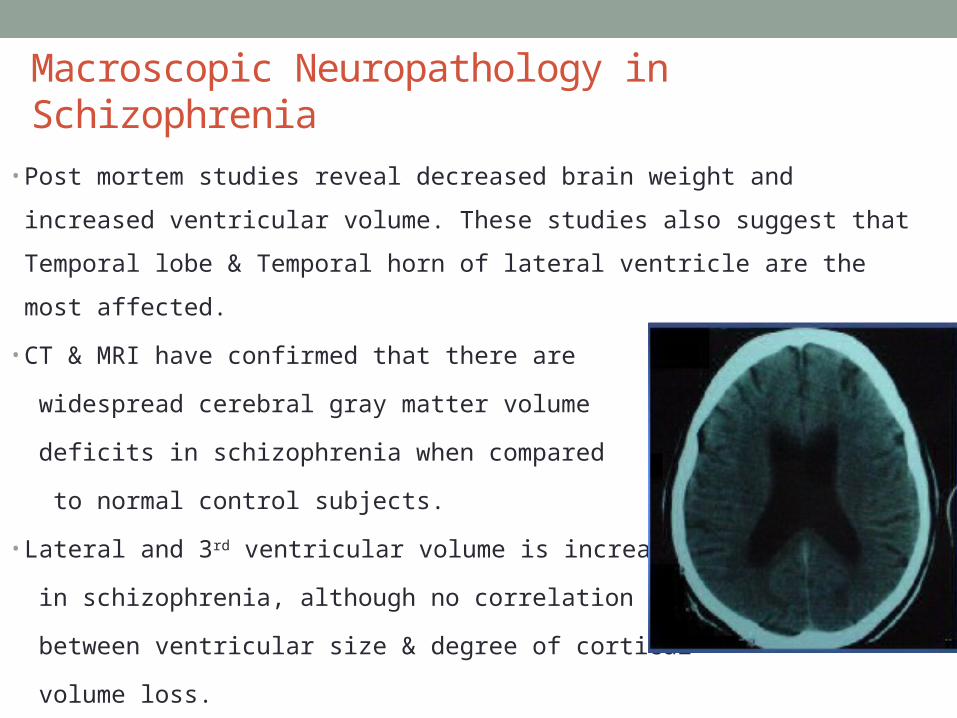
Macroscopic Neuropathology in Schizophrenia
• Post mortem studies reveal decreased brain weight and increased ventricular
volume. These studies also suggest that Temporal lobe & Temporal horn of
lateral ventricle are the most affected.
• CT & MRI have confirmed that there are
widespread cerebral gray matter volume
deficits in schizophrenia when compared
to normal control subjects.
• Lateral and 3rd ventricular volume is increased
in schizophrenia, although no correlation found
between ventricular size & degree of cortical
volume loss.
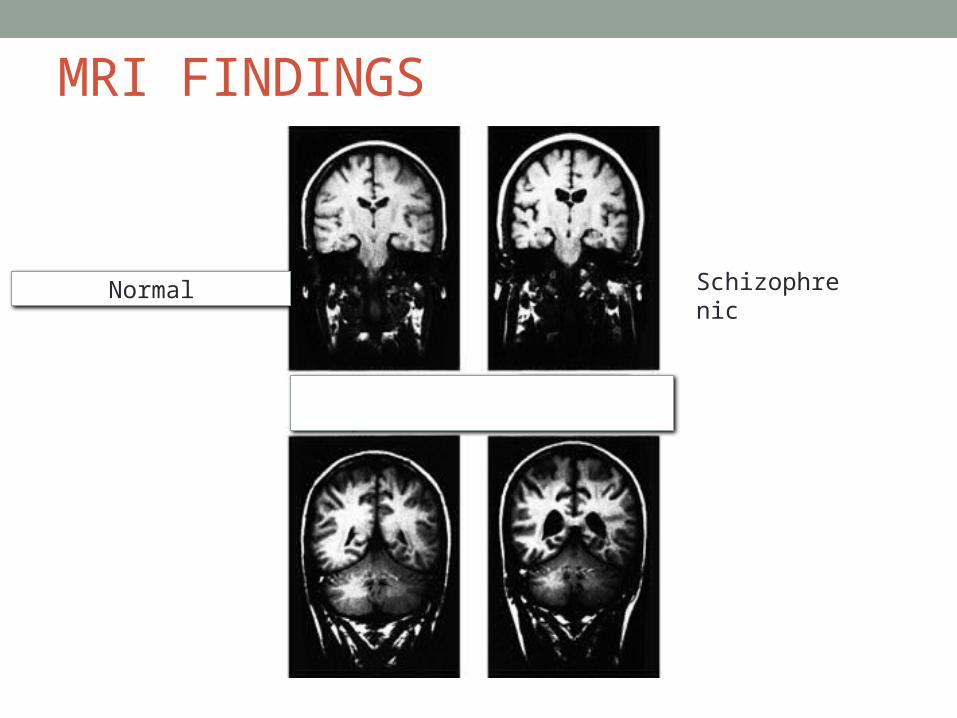
MRI FINDINGS
Normal Schizophrenic

Structural changes in relatives of Schizophrenics
Relatives of schizophrenics also have decreased cortical volumes and enlarged ventricles.These finding suggest that the macroscopic structural changes seen in schizophrenic brain may reflect the underlying genetic vulnerability to the illness and the magnitude of changes are correlated with clinical expression of symptoms

• Reduced Symmetry It is observed in temporal , frontal and occipital lobes of schizophrenics.• Limbic system- Decrease in size of the region including the amygdala, the hippocampus and Para hippocampal gyrus.- MRI imaging studies of patients with Schizophrenia
showed that Hippocampus was not only smaller but also functionally abnormal as indicated by disturbances in glutamate transmission.
- Disordered hippocampal pyramidal cells were also observed in postmortem studies.
- Hippocampus was seen to be smaller in affected twin (static trait)

Disordered hippocampal pyramidal cells

• Prefrontal cortex - Postmortem studies support anatomical abnormalities in
prefrontal cortex in schizophrenics.- Functional deficits in prefrontal region on brain imaging
have been demonstrated.
• Thalamus - Evidence of volume shrinkage or neuronal loss , in
particular subnuclei. The medial dorsal nucleus of the thalamus , which has reciprocal connections with prefrontal cortex, has been reported to have reduced number of neurons.

Structural changes in brain• Increased loss of grey matter in adolescence as seen in
this fMRI image

Functional changes in brain• Hypofrontality hypothesis
• Discordant twins: low frontal blood flow only in affected twin• Wisconsin card sorting task
• Schizophrenics can’t shift attn. to other criterion• Functional imaging: frontal lobe activity lower at rest, esp. in right
hemisphere, does not increase during task.• Drug treatment increased activation of frontal lobes



Neurotransmitters Dopamine theory
- Dopamine is dysregulated; levels may be reduced in
prefrontal cortex and altered complex ways in subcortical
and limbic regions.
- An excess of subcortical dopamine neurotransmission
leads to positive symptoms. ( Hallucinations & Delusions)
- Reduced Dopamine could explain hypofrontality ,
impaired cognition and negative symptoms.

Key dopamine pathways• Mesolimbic dopamine projections from ventral tegmental area
to a number of limbic regions such as Nucleus accumbens and
Temporal lobes.
• Mesocortical pathway projects primarily from ventral tegmental
area to prefrontal cortex.
• Nigrostriatal tract carries nigral dopaminergic projections from
substantia nigra (mainly) & ventral tegmental area to subcortical
motor control areas of striatum ( caudate & putamen).
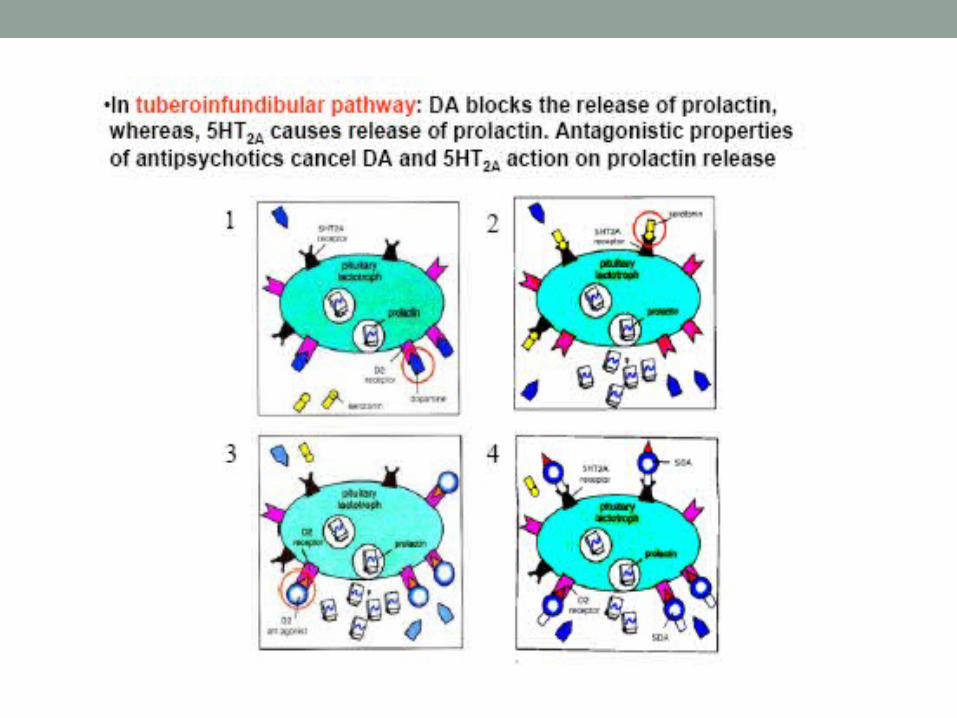
• Tubulofundibular pathway is found entirely in hypothalamus.


Dopamine receptors
• Dopamine has 5 receptors – D1 , D2 , D3 , D4 , D5
• Phenothiazines (incl. chlorpromazine) & all other typical
neuroleptics block D2 receptors and alleviate (+) symptoms.
• Amphetamine (very high doses) <DA agonist> paranoia,
delusions, auditory hallucination
- Also exacerbates symptoms of schizophrenia.
- Effects blocked by DA antagonist chlorpromazine.


Serotonin
• Tryptophan
• Serotonin is said to have seven classes of receptors :
5-HT1 to 5-HT7 .
• 5-HT2 is seen in prefrontal cortex ,striatum and nucleus accumbens; 5-HT3 receptors found in cortical, limbic and subcortical region like amygdala & hippocampus.
• The earliest studies have found increased concentration of serotonin metabolites in plasma & reduced concentration in platelets in schizophrenics.
5-Hydroxyindolic acetic acid
Monoamine oxidase

• In Post mortem studies, Increased levels of serotonin in putamen & globus pallidus.
• The density of reuptake sites for serotonin sites in schizophrenia , particularly in frontal and anterior cingulate cortices.
• Studies looking at mechanism of action of atypical antipsychotics such as clozapine have suggested serotonin’s role in schizophrenia.
• Atypical also reduce parkinsonian side effects and provide enhanced therapeutic efficacy. Atypical antipsychotic have relatively high affinity for 5HT2 receptors
• LSD causes schizophrenia like symptoms , also it blocks serotonin receptors.
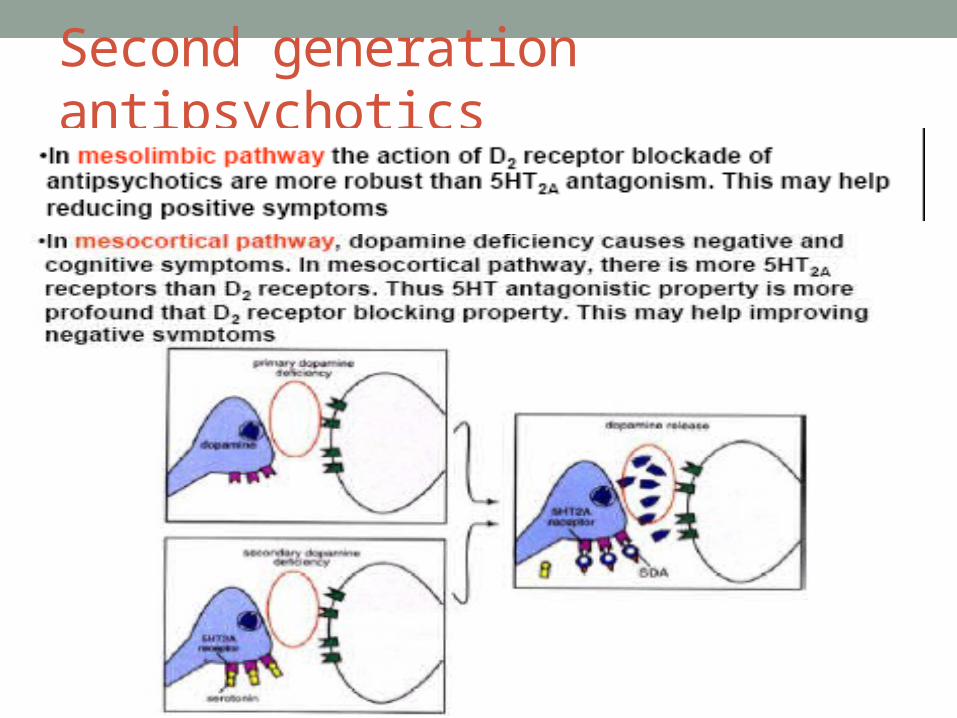
Second generation antipsychotics


GABA • GABA is a major inhibitory neurotransmitter in brain.• GABA has 2 types of receptors : GABA-A & GABA-B• GABA-A is usually seen in CNS , variety of drugs act
here like Benzodiazepines & Barbiturates.• Reduced GABA cortical interneurons , increased GABA-A
receptors are seen in prefrontal cortex , reduced uptake sites in hippocampus are seen in schizophrenia.’
• This shows that GABA cell number or activity is reduced in schizophrenia.
Glutamate• Glutamate is a major excitatory neurotransmitter in the
brain.• Genetic findings pointing at a hypofunction of glutamate
neurotransmission Via NMDA receptors.• Hypothesis is based on observation that NMDA receptor
antagonist such as phencyclidine (pcp) & ketamine produce syndrome similar to schizophrenia.
• PCP and ketamine cause schizophrenia-like psychoses and cognitive deficits in normal subjects and worsens the symptoms of schizophrenia in patients.

Genes• Risk of developing schizophrenia is higher in relatives of a
patient.• Linkage studies have identified loci on chromosomes
1,2,4,5,6,7,8,9,10,13,15,18,22 and X.• Chromosome 22q11-13 has been linked with psychosis
and schizophrenia , several others like 5q , 11q, 18q,19p and 22q.
• Genes – DISC-1 , Neuregulin & dysbindin are said to be linked with schizophrenia.
• DTNBP1 & Neuregulin – negative features
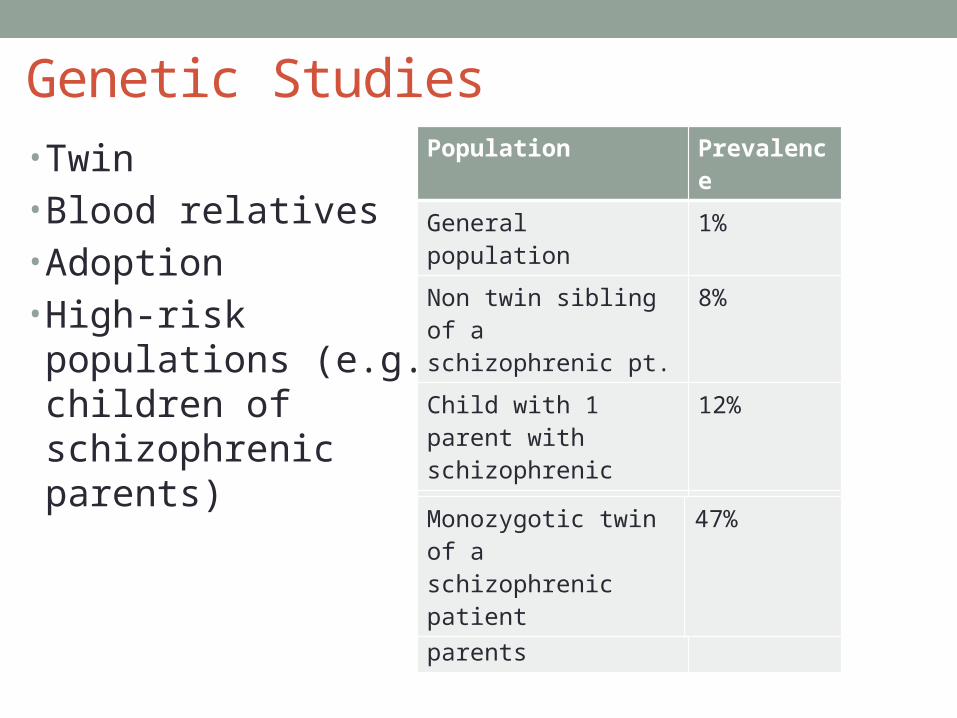
Genetic Studies• Twin• Blood relatives• Adoption• High-risk populations (e.g., children of schizophrenic parents)
Population Prevalence
General population 1%
Non twin sibling of a schizophrenic pt.
8%
Child with 1 parent with schizophrenic
12%
Dizygotic twin of a schizophrenic
12%
Child of 2 schizophrenic parents
40%
Monozygotic twin of a schizophrenic patient
47%

Neurobiological Models
• Genetic factors increase vulnerability to
environmental factors increased risk of
schizophrenia.
• Neuropathological data and studies of obstetric and
perinatal complications support the idea that an
early lesion may account for structural changes.
The apparent lack of gliosis in postmortem studies
is particularly critical and implicates in utero factors.

- Behavioural outcome of subtle abnormalities in early brain development, full effect of which is not manifested till adolescence. Prefrontal cortex matures in late adolescence, the behavioral and cognitive sequelae of subtle structural deficits become manifest . One result is hypofrontality and cognitive impairment.
• Possible insult during gestation, environmental influences• Disturbance in normal brain maturation• Reduced size medial temporal lobe structures - amygdala,
hippocampus• Disturbed cytoarchitecture in hippocampus, entorhinal
cortex

- Genetic and environmental factors produces damage to selected brain areas early in life. Temporal lobe regions like hippocampus are particularly vulnerable. As the prefrontal cortex matures in late adolescence , the behavioral and cognitive sequelae of subtle structural deficits become manifest. One result is hypofrontality and cognitive impairment.
• Possible insult during gestation, environmental influences• Disturbance in normal brain maturation• Reduced size medial temporal lobe structures - amygdala,
hippocampus• Disturbed cytoarchitecture in hippocampus, entorhinal cortex

Summary• Genetically, the disorder is complex, confounding efforts to locate
causative genes. • Similarly, the effects of environment are subtle, with no clear
major factor emerging. Pregnancy, labor, and delivery complications may play a limited role.
• Neurobiological abnormalities include reduced volume of several brain structures, sulcal widening, and increased ventricular size. Cortical abnormalities, particularly in the prefrontal and temporal cortices, have also been implicated by cognitive testing and functional neuroimaging. Postmortem studies have failed to find a major lesion or gliosis that could account for structural abnormalities.
• They have, however, detected a variety of subtle cytoarchitectural changes, perhaps caused by abnormal neurodevelopment. Several neurotransmitters, including dopamine, glutamate, and serotonin, have been implicated.