nephrol. dial. transplant.-1997-nickeleit-1832-8.pdf
TRANSCRIPT

8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 1/7
Nephrol Dial Transplant (1997) 12: 1832–1838
NephrologyDialysis
TransplantationPersonal Opinion
Uric acid nephropathy and end-stage renal disease— Review of a non-disease
V. Nickeleit and M. J. Mihatsch
Institute of Pathology, University of Basel, Kantonsspital, Basel, Switzerland
Key words: gout; nephropathy; renal insuciency; Morphologytophus
Morphological changes seen with the precipitation of uric acid crystals in the kidney can be divided into twomajor groups: (1) chronic (=gouty nephropathy withtophi), and (2) acute. Typically, precipitated crystalsIntroduction
(mainly monosodium urate and less often ammoniumurate [6]) are found in the medulla; (collecting ductsTraditionally, patients suering from gout were
show the highest uric acid concentration of the bodythought to be at high risk for renal complications
[7]).[1,2], in particular the formation of uric acid calculiin the renal pelvis and so-called ‘gouty nephropathy’
Chronic hyperuricaemic nephropathy (Figures 1–4)with tophus formation. Mainly the latter complicationwill be discussed here. This is the ‘classic’ gout kidney with formation of
The precipitation of uric acid in the renal medulla tophi at the cortico-medullary junction and deep inwith formation of characteristic tophi was believed to the medulla. Chronic hyperuricaemia can lead to pre-evoke an inflammatory response leading to fibrosis, a cipitation of uric acid crystals mainly in distal collectingloss of nephrons, and ultimately to chronic irreversible ducts and the interstitium (tophus formation). Therenal failure. Some reports emphasize that nearly 100% exact pathophysiological mechanism is not entirelyof patients with chronic gout also have some renal clear since hyperuricosuria and therefore simple oversa-
involvement [1,2]. Most dramatically, it has been turation of the urine is not a prerequisite (comparestressed by some that renal failure can occur in a high with the acute type) [8]. Quite commonly a decreasepercentage of patients (up to 41%) with chronic gout in renal function (decrease in glomerular filtration,[2,3]. Based on a prevalence of gout (that is to say and/or tubular transport) is an accompanying feature.symptomatic hyperuricaemia with arthritis) of The interstitial uric acid crystals probably originate1.3–3.7% in the general population [4,5], and the from ruptured ducts. The crystals evoke a foreign bodyassumption that renal tophi cause functional deteriora- reaction with central accumulation of crystalloid mat-tion, a significant number of patients should show erial (monosodium urate) surrounded by a rim of gouty nephropathy and renal insuciency. In order to leukocytes, giant cells and fibrosis; this histologicaldetermine the frequency of uric acid deposition in the hallmark is called gout tophus [6,8,9]. In patients withkidney and to correlate the presence of tophi with data a long-standing history of gout, kidneys frequentlyon renal function in a large autopsy series, we screened show not only gouty tophi but also fibrosis, glomerulo-the autopsy files at the Institute of Pathology, Basel, sclerosis, arteriolosclerosis and arterial wall thickeningfrom 1968 to 1976 (n=11 408). Since approximately caused by intimal fibrosis [6,9]. However, these latter45% of all deaths in those years were examined by histological findings are non-specific and can be seennecropsy, data gathered are fairly representative for in various other renal diseases, such as hypertensionthe population in general. In theory (using the figures or interstitial nephritis.mentioned above) in our series around 100 patients(roughly 1%) might be expected to present with gouty
Acute hyperuricaemic nephropathy (Figures 5–8)nephropathy and severe renal insuciency.
Acute hyperuricaemic nephropathy is usually not asso-ciated with gouty arthritis. It is most often (but notexclusively) found in children suering from haemato-
Correspondence and oprint requests to: M. J. Mihatsch MD, Inst.poietic malignancies. Tumour cell necrosis leads to aof Pathology, Kantonsspital, University of Basel, Schoenbeinstrasse
40, CH- 4003 Basel, Switzerland. brisk increase of purine catabolism, to hyperuricaemia,
© 1997 European Renal Association–European Dialysis and Transplant Association

8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 2/7
Uric acid nephropathy and end-stage renal disease 1833
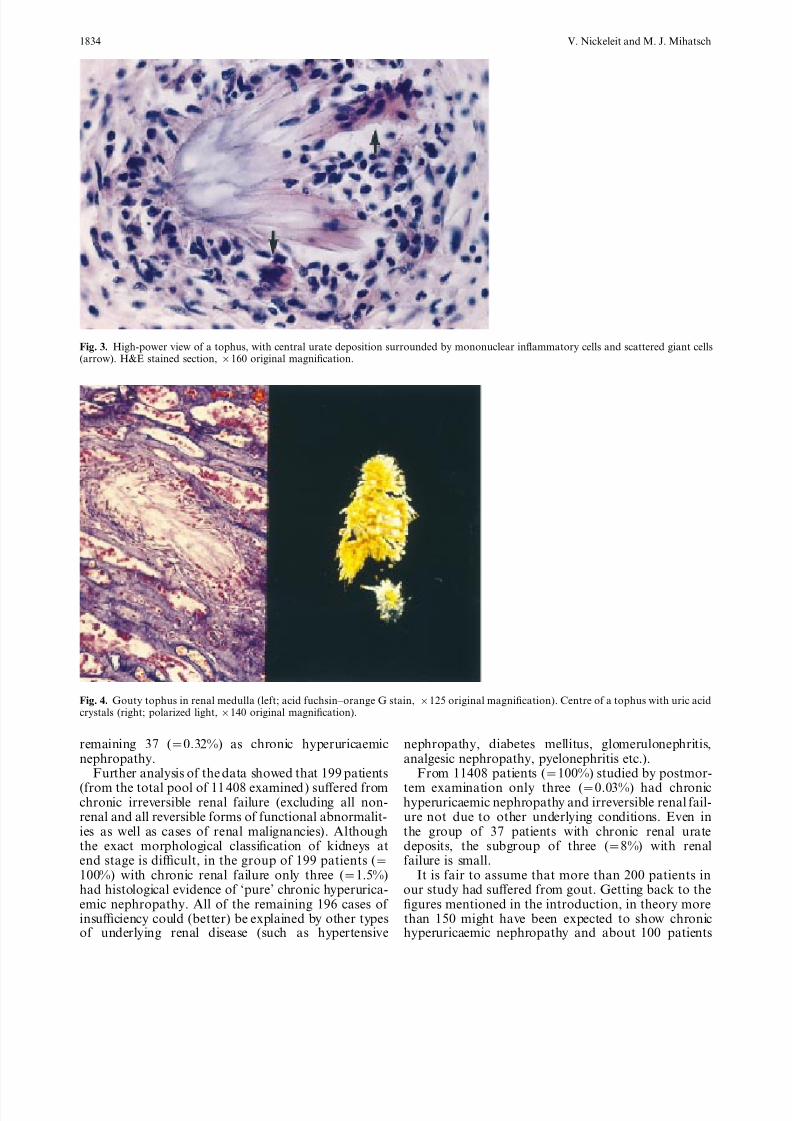
Fig. 1. Gouty tophi in joint and kidney. Chalky white urate deposits are visible in the articular cartilage (right). The corresponding kidney(left) shows yellowish areas in the pyramids (arrow) representing fibrosis and urate deposits.
Fig. 2. Typical gouty tophus in the renal medulla with crystalloid material in the centre surrounded by a narrow rim of fibrosis andinflammation. Note: The tophus probably originated from a ruptured collecting duct (arrow). H&E stained section, ×50 originalmagnification.
and characteristically to hyperuricosuria. Frequently, who were intrigued by the yellow macroscopic appear-ance ‘resembling’ infarcts.)also dehydration and a low pH of the urine are
associated clinical findings. Due to the sudden oversat-uration of uric acid in the urine, uric acid precipitates
as crystals or sludge in tubules and collecting ducts.Prevalence of renal uric acid deposits in the BaselThese precipitates cause obstruction and acute renalseriesfailure [8]. Interstitial fibrosis or tophus formation is
generally not encountered. With appropriate treat-ment, renal function normally recovers, and impair- To determine the overall frequency of urate deposits
in the kidney and to correlate morphological findingsment is therefore mostly transient [5,8]. Also theso-called uric acid renal infarct of the newborn—a with renal function, we evaluated 11 408 consecutive
autopsies performed at the Institute of Pathology inrare, functionally insignificant condition caused bypostnatal lysis of immature red blood cells [6,8]— Basel from 1968 to 1976. Only 39 cases (=0.34%)
displayed renal urate deposits, two of which werebelongs into this category. ( The name ‘uric infarct’represents a misnomer coined by pioneer pathologists classified as acute hyperuricaemic nephropathy and the
8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 3/7
8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 4/7
Uric acid nephropathy and end-stage renal disease 1835
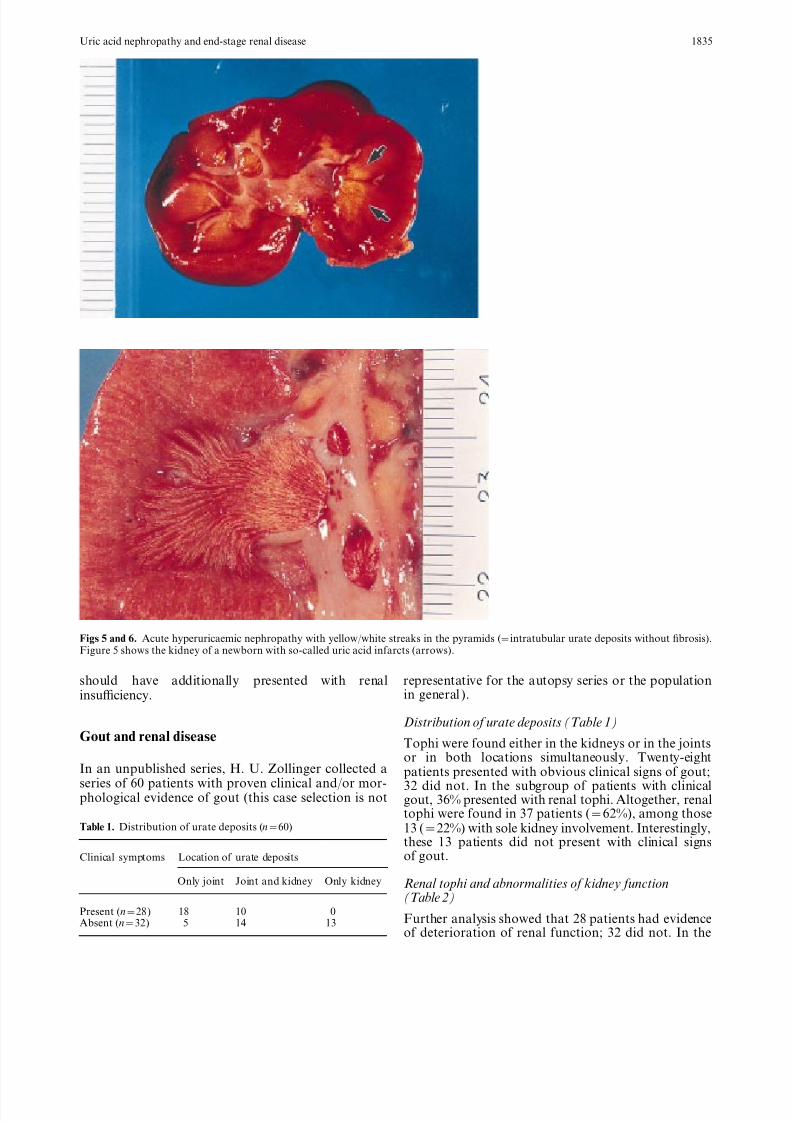
Figs 5 and 6. Acute hyperuricaemic nephropathy with yellow/white streaks in the pyramids (=intratubular urate deposits without fibrosis).Figure 5 shows the kidney of a newborn with so-called uric acid infarcts (arrows).
should have additionally presented with renal representative for the autopsy series or the populationin general ).insuciency.
Distribution of urate deposits (Table 1)Gout and renal disease
Tophi were found either in the kidneys or in the jointsor in both locations simultaneously. Twenty-eight
In an unpublished series, H. U. Zollinger collected a patients presented with obvious clinical signs of gout;
series of 60 patients with proven clinical and/or mor- 32 did not. In the subgroup of patients with clinicalphological evidence of gout (this case selection is not gout, 36% presented with renal tophi. Altogether, renal
tophi were found in 37 patients (=62%), among thoseTable 1. Distribution of urate deposits (n=60) 13 (=22%) with sole kidney involvement. Interestingly,
these 13 patients did not present with clinical signsof gout.Clinical symptoms Location of urate deposits
Only joint Joint and kidney Only kidney Renal tophi and abnormalities of kidney function(Table 2)
Present (n=28) 18 10 0Further analysis showed that 28 patients had evidenceAbsent (n=32) 5 14 13of deterioration of renal function; 32 did not. In the
8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 5/7
V. Nickeleit and M. J. Mihatsch1836
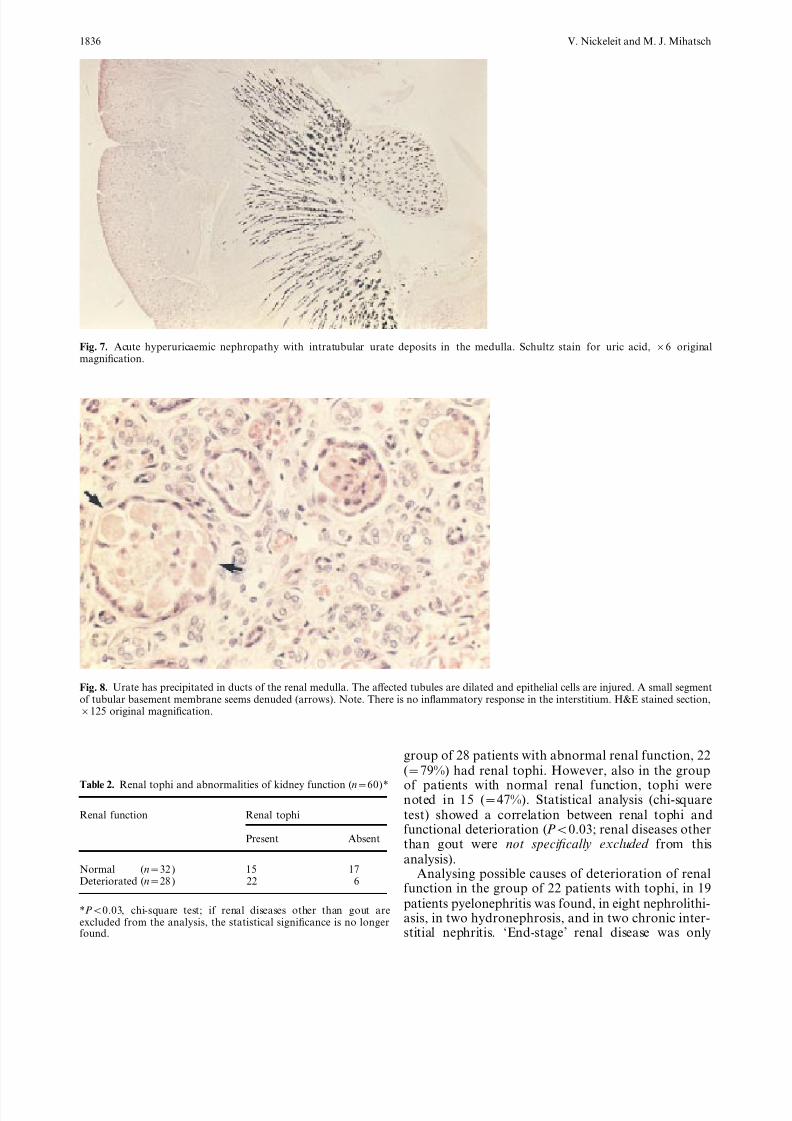
Fig. 7. Acute hyperuricaemic nephropathy with intratubular urate deposits in the medulla. Schultz stain for uric acid, ×6 originalmagnification.
Fig. 8. Urate has precipitated in ducts of the renal medulla. The aected tubules are dilated and epithelial cells are injured. A small segmentof tubular basement membrane seems denuded (arrows). Note. There is no inflammatory response in the interstitium. H&E stained section,×125 original magnification.
group of 28 patients with abnormal renal function, 22(=79%) had renal tophi. However, also in the group
Table 2. Renal tophi and abnormalities of kidney function (n=60)* of patients with normal renal function, tophi werenoted in 15 (=47%). Statistical analysis (chi-square
Renal function Renal tophi test) showed a correlation between renal tophi andfunctional deterioration (P<0.03; renal diseases other
Present Absent than gout were not specifically excluded from thisanalysis).
Normal 15 17(n=32 ) Analysing possible causes of deterioration of renalDeteriorated (n=28 ) 22 6
function in the group of 22 patients with tophi, in 19patients pyelonephritis was found, in eight nephrolithi-
*P<0.03, chi-square test; if renal diseases other than gout areasis, in two hydronephrosis, and in two chronic inter-excluded from the analysis, the statistical significance is no longer
found. stitial nephritis. ‘End-stage’ renal disease was only

8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 6/7
Uric acid nephropathy and end-stage renal disease 1837
found in patients with calculi. Thus, all of these 22 patients were untreated was 6 years). After a meanfollow-up of 6.3 years, only a mild increase in serumcases of functional impairment could be (better)
explained by renal diseases other than gout! creatinine (1.7±0.2 mg/dl) was noted in 10% of patients. The author also tried to predict in a mathem-atical model serum creatinine levels after 40 years of
Summarycontinous serum uric acid levels of either 9.3 or12.9 mg%. He estimated the serum creatinine levels to
Analysis of 11 408 autopsy cases showed that chronic increase to a modest 1.8 or 2.7 mg% respectively.hyperuricaemic nephropathy was found in only 37 Berger and Yu [12], in a study of 524 gouty indi-patients (=0.3%), less frequently than expected. In a
viduals, found in all of their patients abnormalities inselected group of patients carrying the clinical diagnosis renal function explainable by other diseases such asof gout, renal urate depositis were encountered more hypertension, diabetes mellitus, or pyelonephritis.often (=36%). The presence of gouty tophi in the Gouty nephropathy by itself did not seem to causekidney was statistically significantly correlated with renal failure or even impairment of function overabnormal renal function (P<0.03). However, this cor- follow-up periods of up to 12 years. Only renal stonesrelation could no longer be established after exclusion and pyelonephritis had adverse eects on functionalof all cases with other well known causes of renal parameters.disease (in our selected group of 22 patients not a Batuman et al. [13 ] found a high correlation betweensingle one remained). In the entire autopsy series of gout, renal impairment, and increased levels of mobiliz-11 408 cases, only three patients (=0.03%) showed able lead. In their study, gouty patients with normalchronic hyperaluraemic nephropathy and renal failure lead mobilization did not present with renal impair-not otherwise explained. Also in the group of patients ment. In this context it should be mentioned thatpresenting with chronic renal insuciency (n=199) natives in Polynesia were found to have markedly
these three cases (=1.5%) represented a small fraction elevated serum uric acid levels without progression toonly. The same is true for the whole group of patients renal failure [ 14]. Recent publications [ 4,15] also ques-with chronic hyperuricaemic nephropathy (n=37), in tion the rational behind any intervention in cases of which the three cases accounted for barely 10%. And asymptomatic hyperuricaemia, setting the therapeuticeven in these three cases the question remains threshold at 13 mg/dl for men [4 ]. Finally, whetherunanswered whether possibly the renal insuciency renal insuciency encountered in patients with thepreceded the deposition of urate. Furthermore, renal inherited form of familial juvenile gout is definitelytophi were also detected in a significant number of caused by hyperuricaemia, or perhaps by a stillpatients lacking any deterioration of renal function undetermined pathway, remains unknown.(47%, n=37).
Interestingly, renal tophi appeared to be morecommon in patients not presenting with obvious clin- Conclusionical symptoms of gout. Although urate deposits in thekidney were found without accompanying deposits in
Based on our investigation of 11 408 autopsy cases andthe joints, this phenomenon was no longer obvious in the reported data in the literature, we think thatcases with a well-established clinical diagnosis of gout. chronic uric acid deposits in the kidney (=renal tophi)
hardly ever cause terminal irreversible renal failure.Deterioration of renal function can nearly always beGouty renal tophi and renal failure—myth orbetter explained by other well-known risk factors. Inreality?a significant number of cases, renal tophi were alsofound even without evidence of renal malfunction.
Gouty nephropathy and its eect on renal function in aThus, in a patient suering from gout, severe renal
brief review of the literaturedamage with pronounced functional alterations is
Using oxonic acid as a dietary supplement, Bluestone almost invariably due to other diseases such as arterialet al. [10] succeeded in a long-term rat model to hypertension, diabetes mellitus, nephrolithiasis, andproduce hyperuricaemia and hyperuricosuria. After 52 pyelonephritis. Whether renal tophi in association withweeks renal tophi were found in only few animals an underlying kidney disease lead to a more rapid
( 10%), whereas surprisingly early on after only 4 deterioration of renal function remains undetermined.weeks, ~66% of animals had tophus formation. After However, from a practical point of view, gout tophi1 year morphological alterations in the kidneys were in the renal parenchyma do not seem to be of greatminimal and limited to mild interstitial fibrosis. Neither significance for patient management.glomerular nor vascular abnormalities were noted.Over the entire observation period of 52 weeks, renal
Referencesfunction remained normal. The only major complica-tion were renal stones, found in 75% of animals.
1. Gudzent F. Gicht und Rheumatismus. Springer Verlag, Berlin,Fessel [11] studied a group of 72 patients with
1928hyperuricaemia and clinical symptoms of gout, who 2. Talbot JH, Terplan KL. The kidney in gout. Medicine
(Baltimore) 1960; 39: 405–467did not receive any treatment (mean time that the

8/10/2019 Nephrol. Dial. Transplant.-1997-Nickeleit-1832-8.pdf
http://slidepdf.com/reader/full/nephrol-dial-transplant-1997-nickeleit-1832-8pdf 7/7
V. Nickeleit and M. J. Mihatsch1838
3. Barlow KA, Berlin LJ. Renal disease in primary gout. Q J Med 9. Heptinstall RH. Tubular disorders and various metabolic dis-1968; 37: 79–96 eases. In: Heptinstall RH (ed.) Pathology of the Kidney, 4th edn.
4. Becker MA, Roessler BJ. Hyperuricemia and gout. In: Scriver Vol. III. Little, Brown, Boston, 1992; 1989–2043CR, Beaudet AL, Sly WS, Valle D (eds.). The Metabolic and 10. Bluestone R, Waisman J, Klinenberg JR. Chronic experimentalMolecular Basis of Inherited Disease. McGraw-Hill Inc, New hyperuricemic nephropathy—biochemical and morphologicYork, 1995; 1655–1677 characterization. Lab Invest 1975; 33 (3): 273–279
5. Wortmann RL. Gout and other disorders of purine metabolism. 11. Fessel WJ. Renal outcomes of gout and hyperuricemia. AmIn: Isselbacher KJ, Braunwald E, Wilson JD, Martin JB, Fauci J Med 1979; 67: 74–82AS, Kasper DS (eds). Harrison’s Principles of Internal Medicine.
12. Berger L, Yu TF. Renal function in gout. Am J Med 1975;McGraw-Hill Inc, New York, 1994; 2079–2088
59: 605–6136. Zollinger HU. Niere und ableitende Harnwege. In: Doerr DW,
13. Batuman V, Maesaka JK, Haddad B, Tepper E, Landy E,Uehlinger DE (eds.) Spezielle Pathologische Anatomie. Springer
Wedeen RP. The role of lead in gout nephropathy. N Engl Verlag, Berlin, 1966; 282–289J Med 1981; 304 (9): 520–5237. Fineberg SK, Altschul A. The nephropathy in gout. Ann Intern
14. Prior IA, Rose BS, Harvey HP, Davidson F. Hyperuricemia,Med 1956; 44: 1182–1195gout and diabetic abnormality in Polynesian people. Lancet8. Chonko AM, Richardson WP. Urate and uric acid nephropathy,1966: 333–338cystinosis, and oxalosis. In: Tisher CC, Brenner BM (eds) Renal
15. Emmerson BT. The management of gout. N Engl J Med 1996;Pathology—With Clinical and Functional Correlations; Vol. II.Lippincott Company, Philadelphia: 1994, 2nd edn: 1413–1441 334 (7 ): 445–451