neonatal head shape after delivery: an index of molding
TRANSCRIPT

260 Kriewall et al., Neonatal head shape
J. Perinat. Med.6(1977) 260
Neonatal head shape after delivery: An index of molding
Timothy J. KriewaU, Stanley J. Stys, Gregg K. McPherson
University of Michigan, Women's Hospital, Ann Arbor, USA
Molding at parturition, äs perceived subjectively,ranges from no reshaping to marked distortion ofthe infant's head. While clinicians easily recognize,the highly molded head, there are no criteria forquantitating the degree of molding. The purposeof the present study is to describe quantitativelyneonatal skull molding and the restitution of thenewborn's skull from the molded state during theearly neonatal period.
l Literature review
In 1907, STUMPF [13] studied the restitution ofmolding in the neonatal period. Measurements oftwo head circumferences of vaginally deliveredinfants were compared to control infants deliveredby cesarean section, assumed to be unmolded. Heconcluded that the plane of the suboccipito-bregmatic diameter was the presenting plane inlabor, and that molding was a result of interactionof the head with soft tissues rather than the bonypelvis. Both the suboccipitobregmatic and sub-occipitofrontal diameters increased during restitu-tion.HOLLAND [5], in 1922, described cranial stressduring labor and the relationship of excessive stressto tentorial tearsand subdural cerebralhemorrhage.He wrote that tension of the intracranial septa areinevitable äs the head undergoes molding. Moldingwas described äs „an alteration in the position,absolute and relative, and curvature of the cranialbones."Two years later GREENWOOD [4] disputedHOLLAND'S description of the directionof length-
Curriculum vitaeDr. TIMOTHY J. KRIE-WALL was born in 1945.He received a B.S.E. inelectrical engineering fromthe University of Michiganin 1967 and a M.S.E, inelectrical engineering fromStanford University in1968. After working inindustrial research for threeyears, he returned to theUniversity of Michigan toearn a Ph.D. in biomedicalengineering in 1974. He iscurrently an assistant professor at The University ofMichigan'sMedicalSchoolin the Department ofObstetricsand Gynecology.
eningof the molded head stating that it was antero-posterior rather than vertical. Furthermore,restitution of molding in heads which presentedocciput anterior was noted to be faster than inthose which presented occiput posterior.The first radiologic study of molding was reportedin 1942, by MOLOY [8]. Skull films taken immedi-ately after birth compared vaginal deliveries tocesarean sections. A compression binder was alsoused to simulate the forces of parturition in orderto make before and after comparisons. Moloydescribed an increase in the maxillary-verticaldiameter caused by flattening and/or elevation ofthe parietal bones. In contrast to Holland, he alsofeit the occipital plate eleyated.BAXTER [1] in the same year used autopsy speci-mens to describe mechanisms of molding. He
J. Perinat. Med. 5 (1977)
Kriewall et al., Neonatal head shape 261
agreed with many of MOLOY'S observations andconcluded that vertical elevation and flattening ofthe parietals are limited mechanisms affordinglittle margin before compression of cranial contentsbegins.In 1958, BORELL and FERNSTROM [2] performedan intrapartum radiographic study and discoveredthat duringlabor the parietal bones rotate outwardsand are displaced upwards resulting in an increaseof the biparietal diameter of äs much äs 10 mm.Like STUMPF fifty years before, they concludedthat molding of the head is produced by maternalsoft tissues rather than by the bony pelvis.At the same time LINDGREN'S studies [6] broughthim to the same conclusion regarding the structurescausing molding of the fetal head. He made cont-inuous recordings during labor of amniotic pressuresand pressures exerted on the fetal head by theuterine wall. Pressures on the greatest circumferenceof the fetal head were noted to be several timesgreater than amniotic pressures during both uterinecontractions and the resting phase.In 1968, SCHWARCZ et al [12] confirmedLINDGREN'S observation that pressure on theequator of the fetal head during uterine contractionsis greater than amniotic fluid pressure. They alsonoted that cephalic compression during uterinecontractions could lead to transient cerebralischemia resulting in cardiac decelerations.In the same year WILLERMAN [14] reported twostudies on intellectual differences in children bornleft occiput anterior and right occiput anterior.Children delivered from right occiput anteriorhad lower performance IQ than verbal IQ scores.The children delivered from left occiput anteriorhad no difference in performance or verbal IQscores. Assuming that the hemispheres of the brainhave different capacities for verbal or performancefunctions, these studies imply that impairment ofverbal or performance function might occur äs aresult of the presentation of the head during labor.The subjectiveimpressionsof molding that cliniciansuse are understandable considering the literaturejust reviewed. These studies are widely spaced intime and use several vastly different methods. Thequalitative mechanisms of fetal skull molding arestill only poorly defined, and quantitative meas-urements of molding have been nonexistent. There-
fore, this study was undertaken to devise a quan-titative measure of molding.
2 Methods
Thirty-eight infants delivered at the University ofMichigan Medical Center were studied for molding.The study group is representative of the patientpopulation delivered at this medical center.Twenty-three infants were delivered vaginally fromvertex presentations. Fifteen infants were deliveredby elective cesarean section before the onset oflabor; two of these were breech presentations, andthe others vertex. Three infants weighed less than2500 grams, four greater than 4000 grams. Fifteenmothers were primiparas, twenty-three multi-parous. The age ränge of the mothers was 14—35years.Measurements of each infant's skull were madewith obstetrical calipers. The distance was meas-ured to the nearest millimeter. Measurements ofthe biparietal, bitemporal, suboccipitobregmatic,suboccipitofrontal, occipitofrontal, submento-bregmatic and mentovertical diameters were madewithin the first hour after birth and repeated at24,48,72hoursofage.A second group of ten infants was studied formeasurement precision and observer influence.The two groupsof infants were similarly composed.The biparietal, suboccipitofrontal and mentoverti-cal diameters were used to describe an ellipsoidwhich approximates the volume of the infant'shead. The parameter „curvature" from analyticalgeometry was used to derive a molding index.Curvature defines the amount of change in theangle of a tangent to a curve for an incrementalchange in the are length of the curve. To definecurvature in a three-dimensional sense, the geo-metric mean was taken for the curvature in thetwo planes defined by the biparietal and mento-vertical diameters and by the suboccipitofrontaland mentovertical diameters. The molding indexwas made more sensitive by taking the product ofthe geometric mean of the curvatures and thementovertical diameter. Thus, the molding indexused in this study is defined by the followingequation.
J. Perinat. Med. 5 (1977)
262 Kriewall et al., Neonatal head shape
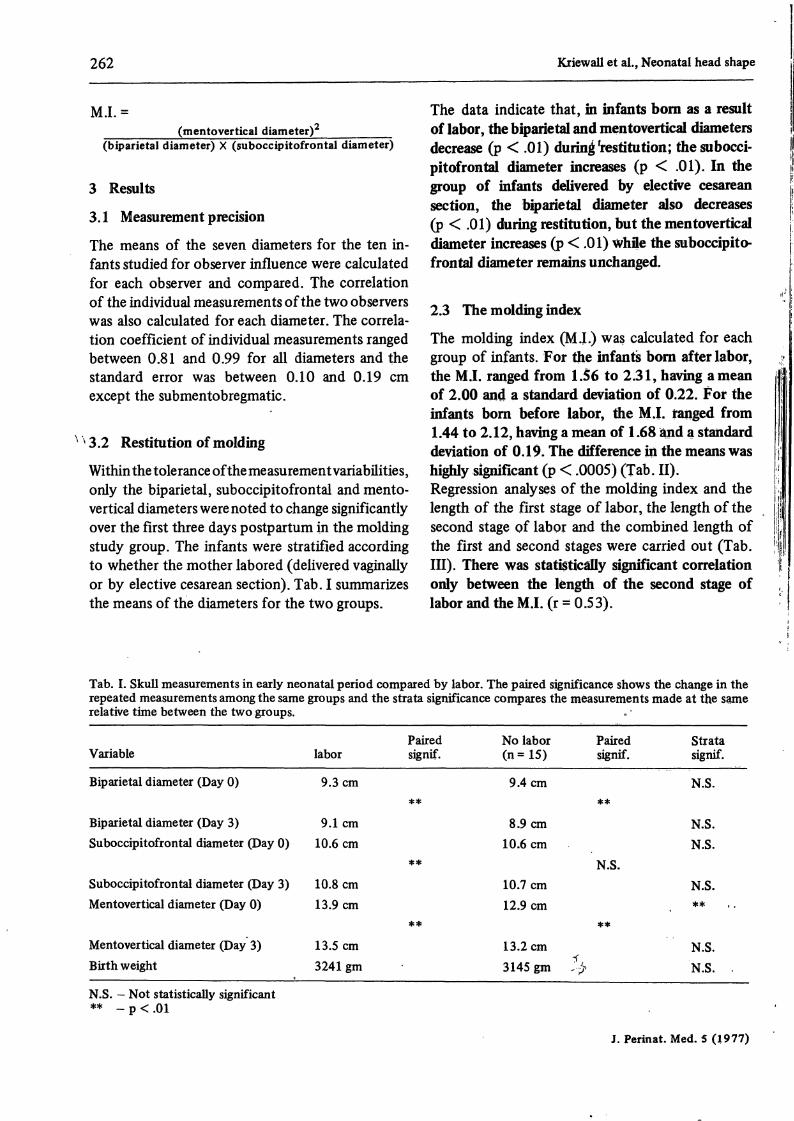
M.I.=(mentovertical diameter)
(biparietal diameter) X (suboccipitofrontal diameter)
3 Results
3. l Measurement precision
The means of the seven diameters for the ten in-fants studied for observer influence were calculatedfor each observer and compared. The correlationof the individual measurements of the two observerswas also calculated for each diameter. The correla-tion coefficient of individual measurements rangedbetween 0.81 and 0.99 for all diameters and theStandard error was between 0.10 and 0.19 cmexcept the submentobregmatic.
13.2 Restitution of molding
Within the tolerance of the measurement variabilities,only the biparietal, suboccipitofrontal and mento-vertical diameters werenoted to change significantlyover the first three days postpartum in the moldingstudy group. The infants were stratified accordingto whether the mother labored (delivered vaginallyor by elective cesarean section). Tab. I summarizesthe means of the diameters for the two groups.
The data indicate that, in infants born äs a resultof labor, the biparietal and mentovertical diametersdecrease (p < .01) during Restitution; the subocci-pitofrontal diameter increases (p < .01). In thegroup of infants delivered by elective cesareansection, the biparietal diameter also decreases(p < .01) during restitution, but the mentoverticaldiameter increases (p < .01) whfle the suboccipito-frontal diameter remains unchanged.
2.3 The molding index
The molding index (M.L) was calculated for eachgroup of infants. For the infants born after labor,the M.I. ranged from 1.56 to 2.31, having ameanof 2.00 and a Standard deviation of 0.22. For theinfants born before labor, the M.I. ranged from1.44 to 2.12, having a mean of l .68 and a Standarddeviation of 0.19. The difference in the means washighly significant (p < .0005) (Tab. II).Regression analyses of the molding index and thelength of the first stage of labor, the length of thesecond stage of labor and the combined length ofthe first and second stages were carried out (Tab.III). There was statistically significant correlationonly between the length of the second stage oflabor and the M J. (r = 0.53).
Tab. I. Skull measurements in early neonatai period compared by labor. The paired significance shows the change in therepeated measurements among the same groups and the strata significance compares the measurements made at the sarnerelative time between the two groups.
Variable
Biparietal diameter (Day 0)
Biparietal diameter (Day 3)Suboccipitofrontal diameter (Day 0)
Suboccipitofrontal diameter (Day 3)Mentovertical diameter (Day 0)
Mentovertical diameter (Day 3)Birth weight
Pairedlabor signif.
9.3cm**
9.1cm10.6 cm
**10.8 cm13.9 cm
**13.5 cm3241 gm
No labor Paired(n = 15) signif.
9.4cm**
8.9cm10.6 cm
N.S.10.7 cm12.9 cm
**13.2cm3145 gm ?·$
Stratasignif.
N.S.
N.S.N.S.
N.S.**
N.S.N.S. .
N.S. — Not statistically significant** -
J. Perinat. Med. 5 (1977)

Kriewall et al., Neonatal head shape 263
Tab. II. Comparison of molding index stratified by labor.
Variable
Molding index (Day 0)
Molding index (Day 3)
Yes Paired(n = 2 3) signif.
2.00**
1.86
No Paired(n = 15) signif.
1.68**
1.82
Stratasignif.
**
N.S.
N.S. - Not statistically significant** - p < .01
The molding Indexes werecomparedforprimiparousand multiparous mothers whose infants were bornvaginally. There were ten primiparous and elevenmultiparous mothers. The mean M.I. for infants ofprimiparous mothers was 2.07 with a Standarddeviation of 0.16. The mean M.I. for infants ofmultiparous mothers was 1.88 with a Standarddeviation of 0.23. The difference was statisticallysignificant (p < 0.05).The M.I. was not correlated t o infant weight ineither group (r = 0.15 and - 0.24 for infants oflaboring and non-laboring mothers, respectively).
Tab. III. Regression analysis of length of labor andmolding index.
Dependent Variable Correlation Coefficient (r)
l st stage of labor 0.21 (N.S.)2nd stage of labor 0.53 (*)Combined l st & 2 nd stage 0.30 (N.S.)of labor
N.S. - Not statistically significant** -p<.05
The molding Indexes were compared for infantsborn after labor stratified by position. Occiputanterior presentations (n = 16) were comparedwith the pooled values of occiput transverse (n = 5)and occiput posterior (n = 2) presentations. Themean M.I. for OA presentations was 1.93 havinga Standard deviation of 0.20. The mean M.I. forthe OT and OP group was 2.05 having a Standarddeviation of 0.24. The difference is not statisticallydifferent.
4 Discussion
4. l Observations on measurement precision
Based on the means, variances and correlationbetween the two observers, the observers makeessentially thesame measurements for the biparietal,suboccipitofrontal and occipitofrontal diameters.Thestandarderror of measurement for the biparietaldiameter was commensurate with ultrasoniccephalometry äs reported by others [7, 10]. Theobservers do not make the same measurementsconsistently for the bregmatic diameters. Thisreflects the difficulty in defining landmarks withinthe bregma and in touching the bregma with thecalipers without deforming the soft tissue.
4.2 Observations on the restitution of molding
In spite of the dramatic visual changes that oftentake place in the shape of the infant's head afterdelivery, only three of the seven diameters meas-ured changed significantly. The four diameterswhich didnot change significantly during restitutionmay contribute to the molding and restitutionprocess, but their effects are either small or simplyobscured by the inability to make precise meas-urements with the methods in this study.Of the three remaining diameters, significantchanges occur in the same direction for the biparietaldiameter for both groups of infants stratified byexposure to labor. The suboccipitofrontal diameterincreased during restitution in both groups, butnot significantly in the group without labor. Theseresidts corroborate the findings only recentlyreported by DESOUZA et al. [3]. The direction ofchange for the mentovertical diameter was differentfor the two groups, decreasing during restitution
J. Perinat. Med. 5 (1977)

264 Kriewall et al., Neonatal head shape
for infants delivered vaginally and increasing ininfants delivered before labor.If restitutional changes are opposite in direction tomolding changes, then, for the fetus delivered fromthe vertex position äs a result of labor, moldingincreases the biparietal and mentovertical diameterswhile decreasing the suboccipitofrontal diameter.STUMPF [13] feit that the plane of the suboccipito-bregmatic diameter presents most often duringlabor. If thisplane's dimensions are to be minimized,the sagittal diameter, approximated by the sub-occipitofrontal diameter, should decrease whilethe transverse diameter, approximated by thebiparietal diameter, should increase. BORELL andFERNSTROM [2] described changes of this type intheir intrapartum radiographic study. Compressionforces on the presenting suboccipitobregmatic planewould lead to mentovertical diameter lengtheningby displacement of parietal, frontal and occipitalbones äs described by BAXTER [1].The changes which occur in the group of infantsdelivered before exposure to labor indicate thatthis group is not an ideal control group äs severalauthors have assumed [9, 13]. Some degree ofmolding occurs merely with positioning of thefetal head within the Uterus prior to labor. Restitu-tional changes in the biparietal and suboccipito-frontal diameters are in the same direction äs ininfants delivered vaginally, although suboccipito-frontal diameter changes are not significantlydifferent during restitution.Mentovertical diameter changes are oppositebetween the two groups of infants. The continuingrepetitive BRAXTON-HICKS contractions through-out pregnancy may be a previously unrecognizedfactor involved in the change of head shape inthose infants born before labor. Environmentaldifferences of intraamniotic and extrauterine lifemay be another factor involved in the dynamicsof head shaping of newborns.
Since the biparietal, suboccipitofrontal and mento-vertical diameters change dramatically in neonatesregardless of their exposure or lack of exposure tolabor, a quantitative index of molding based onthese three diameters might indicate the dynamicsof the process for both groups.
4.3 The molding index
The molding index äs defined in the text wasshown to reflect, on the whole, the shape of theinfant's heads. However, due to the overlap in theindividual values, one cannot infer from this singleindex whether or not the infant has a molded head.A comparison of the two groups indicates that theheads of infants born before labor are äs distortedäs those born after labor, the difference being inthe direction of the shape change. Those infantsborn after labor have more oblong heads whilethose born before labor have rounder heads. Afterthe three days of postpartum restitution, the headshapes of both groups äre the same (Tab. II). Thefact that the heads of infants born before labor aremolded points to the error in such Statements äs„a certain amount of molding is present in everybaby's head, except in those born by electivecesarean section" (MYLES [9]).A statistically significant correlation between themolding index and the length of the second stageof labor may indicate that the greater the dispro-portion between the fetal head and maternal pelvis,the longer the second stage of labor. This assumesa larger disproportion produces a proportionatelyhigher molding index. However, since the squareof the correlation coefficient accounts for the pro-portion of Variation of one variable explained by aregression on the other variable, (REMINGTON andSCHORK [11]) it appears that disproportion is notthe major determinant for the length of labor'ssecond stage (r2 = 0.28).
Summary
The purpose of this study is to describe quantitatively therestitution of the newborn's skull from the molded stateduring the early neonatal period. Measurements of sevenskull diameters of thirty-eight infants were made withinthe fkst hour after birth and repeated at 24, 48 and 72
hours of age. The measurements were made with obstetricalcalipers. The measureMent precision was tested on an in-dependent study groupj> and found to be comparable touitrasoniccephalometry; the Standard error of measurementwas less thanO.19 centimeters for all the diameters critical
J.Perinat. Med. 5 (1977)

Kriewall et al., Neonatal head shape 265
to the study. Within this tolerance of measurement varia-bility, only the biparietal, suboccipitofrontal and mento-vertical diameters were noted to change significantlyover the first three days postpartum. The infants weiestratified according to whether the mother labored. Forinfants born after labor (n = 23), the biparietal andmentovertical diameters decrease (p < .01) during resti-tution, but the suboccipitofrontal diameter increases(p < .01). For infants born by elective cesarean section,the biparietal diameter also decreases (p < .01) duringrestitution, but the mentovertical diameter increases(p < .01). The suboccipitofrontal diameter remains un-changed (Tab. I). The changes which occur in the groupof infants delivered before exposure to labor indicatethat this group is not an ideal control group äs severalauthors have assumed [9, 13]. The infants from the twogroups Start at birth with heads distorted in oppositedirections about the long axis, but subsequently undergohead reshaping toward a common end point secondaryto restitutional and environmental forces.To quantitate the degree of head molding äs a consequenceof the birth process, an index of molding was derived. Theindex of molding is defined äs the square of the mento-
vertical diameter divided by the product of the biparietaland suboccipitofrontal diameters. The mean molding index(M.I.) of the infants born after labor (n = 23) was 2.00with a Standard deviation of 0.22. The mean and Standarddeviation of the infants born before labor (n = 15) was1.68 and 0.19, respectively, The difference in the meansof the two groups was highly significant (p < .0005)(Tab. II). However, after three days of postpartumrestitution, there was no difference in the M.I. of the twogroups. A regression analysis of the molding index on thelength of the first, second and combined stages of labor *showed that a statistically significant correlation (r = 53)existed only for the second stage of labor (p < .05) (Tab.III). The mean M.I. of infants born from laboring primi-parous mothers (n = 10) was significantly greater than theM.I. of infants born from laboring multiparous mothers(n = 11). The M.I. was not correlated with infant weight.A comparison of the two groups that were stratifiedaccording to labor indicates that the heads of infants bornbefore labor are just äs misshapened äs those that are bornafter labor, the difference being in the direction of theshape change.
Keywords: Caput succedaneum, fetal skull, head diameters, labor, molding index, neonatal skull, parturition.
Zusammenfassung
Die neonatale Kopfform nach der Geburt: ein Verfor-mungsindexZiel dieser Studie war es, die Wiederherstellung der Kopf-form des Neugeborenen während der frühen Neonatal-periode quantitativ zu beschreiben. 7 Kopfdurchmesserwurden bei 38 Kindern innerhalb der 1. Stunde nach derGeburt gemessen und die Messungen nach 24, 48 und 72Lebensstunden wiederholt. Die Messungen wurden mitgeburtshilflichen Zirkeln durchgeführt. Die Meßgenauig-keit ist in einer unabhängigen Studie geprüft worden,wobei herauskam, daß sie mit der Ultraschallkephalometrievergleichbar ist; die Standardabweichung der Mittelwertebetrug weniger als 0,19 cm für alle in dieser Studie wich-tigen Durchmesser. Innerhalb dieser Meßtoleranz verän-derten sich nur der bipaiietale, subokzipitofrontale undmentovertikale Durchmesser innerhalb der ersten 3 post-partalen Tage signifikant. Die Kinder wurden in Gruppeneingeteilt, je nachdem ob die Mutter Wehen hatte odernicht. Bei Neugeborenen, die vaginal nach Wehentätig-keit geboren worden waren (n = 23) nahm der biparietaleund mentovertikale Durchmesser während der Restitu-tionsphase ab (p < 0.01), der subokzipitofrontale Durch-messer nahm jedoch zu (p < 0.01). Bei Kindern, diedurch elektive Schnittentbindung zur Welt gekommenwaren, nahm der biparietale Durchmesser ebenfalls ab(p < 0,01) während der Rückbildungsperiode, der mento-vertikale Durchmesser jedoch zu (p < 0,01). Der subok-zipitofrontale Durchmesser blieb unverändert (Tab. I).Die Durchmesserveränderungen, die in der Gruppe vonKindern auftraten, die vor Einsetzen der Wehentätigkeitgeboren worden waren, weisen darauf hin, daß dieseGruppe im Gegensatz zur Meinung verschiedener Autoren[9, 13] kein ideales Kontrollkollektiv darstellt. Die Kinderbeider Untersuchungsgruppen haben nach der Geburt einen
Kopf, der um die Längsachse in Gegenrichtung geformtist, in der Folgezeit dann Jedoch auf einen gemeinsamenEndzustand hin sich verformt, unabhängig von Restitu-tions- und Umweltkräften.Um das Ausmaß der durch den Geburtsprozeß ausgelöstenSchädelverformung zu bestimmen, wurde ein Verformungs-index entwickelt. Der Index ist definiert durch das Quadratdes mentovertikalen Durchmessers dividiert durch dasProdukt aus biparietalem und subokzipitofrontalemDurchmesser. Der mittlere Verformungsindex, der nachWehentätigkeit geborenen Kinder (n = 23) betrug 2,00mit einer Standardabweichung von 0,22. Mittelwert undStandardabweichung der Kinder, die vor regulärer Wehen-tätigkeit geboren wurden (n = 15) betrug 1,68 und 0,19.Die Differenz der Mittelwerte beider Gruppen war stati-stisch hochsignifikant (p < .0005) (Tab. II). Nach einerdreitägigen postpartalen Restitutionsphase fand sich je-doch keine Differenz mehr im Verformungsindex beiderGruppen. Eine Regressionsanalyse des Verformungsindexmit der Dauer der Eröffnungs- und Austreibungsperiodesowie mit einer Kombination beider Abschnitte ergab,daß nur für die Austreibungsperiode eine statistisch sig-nifikante Korrelation (r = 0,53) besteht (Tab. III). Dermittlere Schädelverformungsindex von Neugeborenen, dievon erstgebärenden Frauen nach Wehentätigkeit (n = 10)geboren worden waren, war signifikant größer als jenervon Neugeborenen mehrgebärender Mütter (n = 11). DerVerformungsindex war mit dem Kindsgewicht nicht korre-üert.Ein Vergleich der Köpfe in den beiden Gruppen, die ent-sprechend der Wehentätigkeit gebildet wurden zeigte, daßdie Köpfe von Kindern, die vor Wehentätigkeit geborenwurden, ebenso verformt sind wie jene, die nach Wehen-tätigkeit zur Welt kamen.
Schlüsselwörter: Caput succedaneum, fetaler Kopf, Geburt, Kopfdurchmesser, neonataler Kopf, VerformungsindexWehen. '
J. Perinat. Med. 5(1977)

266 Kriewall et aL, Neonatal head shape
Resume
Forme cränienne neonatale apres Faccouchement: Indexde deformationLe present article se propose de decrire quantitativementla restitution du cräne deforme du nouveau-ne pendant lapremiere periode neonatale. Pour cela, nous avons mesuresept diametres cräniens de 38 bebes durant la premiereheure suivant la naissance, puis 24, 48 et 72 heures apresla naissance. Ces mesures ont ete realisees a Taide decalipers obstetriques. La precision en a ete testee sur ungroupe d'etude independant et trouvee comparable a lacephalometrie ultrasonique; Ferreur type de mesure a eteinferieure a 0.19 cm pour tous les diametres soumis al'etude. Compte tenu de cette Variation toleree de mesure,seuls les diametres biparietal, suboccipitofrontal et mento-vertical ont montre un changement important pendant lestrois premiers jours post partum. Les bebes ont ete stratifiesselon que la mere a ete en travail ou non. Pour les enfantsnes apres le travail (n = 23), nous avons releve une baissedes diametres biparietal et mentovertical (p < .01) pendantla restitution, mais une augmentation du diametre suboc-cipitofrontal (p < .01). Pour les enfants nes par cesarienne^elective, le diametre biparietal decroit aussi (p < .01)pendant la restitution, tandis que le diametre mentoverticalaugmente (p < .01) et quele diametre suboccipitofrontalreste inchange (Tab. I). Les changements observes dans legroupe des enfants nes avant l'exposition au travail prouventque ce groupe ne remplit pas des conditions de controleaussi ideales que Font pretendu divers auteurs [9,13]. Lesenfants des deux groupes ont d'abord a la naissance destetes deformees dans des directions opposees sur Taxe
long, mais ils subissent ensuite une «reformation» de latete vers un point terminal commun secondaire aux forcesrestitutionnelles et environnantes.Afin de determiner quantitativement le degre de deforma-tion cränienne consequente a la parturition, nous avonsderive un index de deformation (molding index: M.I.),defini comme le carre du diametre mentovertical divisepar le produit des diametres biparietal et suboccipito-frontal. L'index de deformation moyen des enfants nesapres le travail (n = 23) a ete de 2.00 avec une deviationtype de 0.22. Les deviations moyenne et type des enfantsnes avant le travail (n = 15) ont ete respectivement de1.68 et 0.19. La difference dans les moyennes des deuxgroupes a ete tres significative (p < .0005). (Tab. II).Cependant, apres 3 jours de restitution post partum, nousn'avons observe aucune difference dans le M.I. des deuxgroupes. Une analyse regressive de l'index de deformationsur la longueur des phases premiere, seconde et cömbirieedu travail a montre qu'il n'existait une correlationd'importance statistique (r = 53) que pour la secondephase du travail (p < .05). (Tab. III). Le M.I. moyen desenfants nes de meres primipares en travail (n = 10) a etebeaucoup plus grand que le M.I. des enfants nes de meresmultipares en travail (n = 11). Nous n'avons releve aucunecorrelation entre Je M.I. et le poids des bebes.Une comparaison des deux groupes qui ont ete stratifiesdependamment du travail indique que les tetes des bebesnes avant le travail sont tout aussi deformees que chez lesbebes nes apres le travail, lä difference portant sur ladirection prise par la deformation.
Mots-cles: Caput succedaneum, cräne foetal, cräne neoriatal, diametres de la tete, index de deformation, parturition.
Acknowledgments: The authors wish to thank Prof. M. ANTHONY SCHORK and Ms. SANDY STEINHORN for theirassistance in the statistical analysis.This work was made possible thrqugh the University of Michigan's Medical School Fund for Com-puting.
Bibliography
[1] BAXTER, J.: Moulding of the fetal head. J. Obstet.Gynaec. Brit. Emp. 53 (1946) 212
[2] BORELL, U., I. FERNSTROM: Die Umformung deskindlichen Kopfes während normaler Entbindung inregelrechter Hinterhauptslage und bei engem Becken.Geburtsh. u. Frauenheilk. 18 (1958) 1156
[3] DESOUZA, S. W, J. ROSS, R. D. G. MILNER:Alterations in head shape of newborn infants aftercaesarean section or vaginal delivery. Arch. Dis.Child.51(1976)624
[4] GREENWOOD, W. O.: Moulding of the foetal headand its consequences. J. Obstet. Gynaec. Brit. Emp.31(1924)611
[5] HOLLAND, E.: Cranial stress in the foetus duringlabor and the effects of excessive stress on the intra-cranial contents. J. Obstet. Gynaec. Brit. Emp. 29(1922)549
[6] LINDGREN, L.: The causes of foetal head mouldingin labor. Acta Obstet. Gynec. Scand. 39 (1960) 46
[7] LUND, R. M., T. CHARD: Reproducibility of meas-urement of fetal biparietal diameter by ultrasoniccephalometry. J. Obstet. Gynaec. Brit. Commonw.81 (1974) 682
[8] MOLOY, H. C.: Studies of head molding duringlabor. Amer. J. Obstet. Gynec. 44 (1942) 762
[9] MYLES, M. D.: A Textbook for Midwives. E. andS. Livingston Ltd., London 1968
[10] POLL, V.: Precision of ultrasonic fetal cephalometry.Brit. J. Obstet. Gynaec. 83 (1976) 217
[11JREMINGTON, R. D., M. A. SCHORK: Statisticswith Applications to the Biological and HealthSciences. Prentice-Hall, Inc., Englewood Cliffs, NewJersey 1970
[12] SCHWARZ, R. L., G. STRADA-SAEN?^ O. ALT-HABE, J. FERNANDEZ-FUNES, L. O.f^LVAREZ,R. CALDEYRO-BARCIA: Compression received bythe head of the human fetus during labor. In: Physi-cal Trauma äs an Etiological Agent in Mental Retar-
J. Perinat. Med. 5 (1977)

Kriewall et aL, Neonatal head shape , 267
dation. U.S. Department of Health, Education and [14] WILLERMAN, L.: Fetal head position duringWeifare, Washington, D.C. 1970 delivery and intelligence. In: Physical Trauma äs an
[13] STUMPF, M.: Beitrag zur Kenntnis der Beeinflussung Etiological Agent in Mental Retardation. U.S. De-der Kopfform durch die Geburtsvorgänge. Arch. partment of Health, Education and Weifare, Washing-Gynaek. 82 (1907) 215 ton, D.C. 1970
Received March 14, 1977. Accepted April 4, 1977.
Timothy J. Kriewall, Ph.D.L-2011 Women's HospitalUniversity of Michigan Medical CenterAnn Arbor, Michigan 48109 U.S.A.
J. Perinat. Med. 5 (1977)