neonatal emergency and common problems in emergency department
TRANSCRIPT
Adib Mursyidi A&E Department

5-day-old boy brought to ED for very poor feeding, lethargy. Full term SVD with unremarkable prenatal and post natal history
What is your next step?
FREAK OUT!!!!


Ill neonate frightening entity for most clinicians
Neonatal = first 28 days of life, but may be expanded to account for gestational age
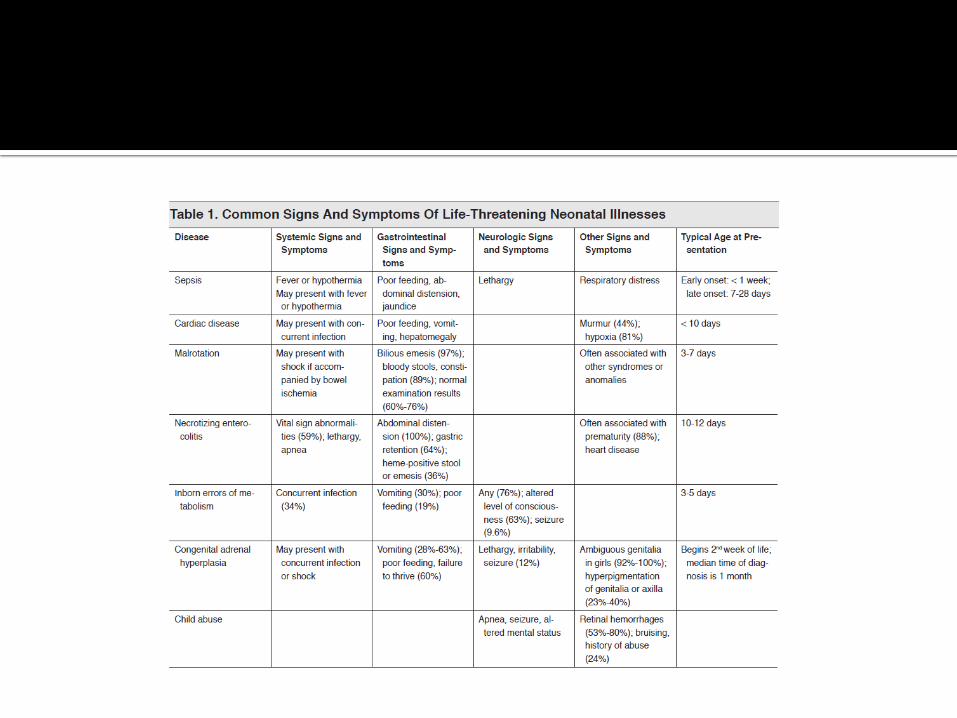
Generally sign and symptoms are vague and non-specific, can be fatal!

Fever / hypothermia Abnormal tone (limping/stiff) Altered mental status (lethargy/irritability) Weak suck Poor feeding Jaundice Abnormal respiration Cyanosis or mottling Vomiting

FEEDING TREND In breast feeding : 1 to 3 hourly, bottle : 6 to 9 in
24hr Lose up to 12% of birth weight during first 3-
7days After this time, gain 20-30g during first 3months
STOOLS Normal BF infants may go 5-7days without
stools OR 6-7 stools per day Color : no significant unless blood is present OR
acholic (white)

RESPIRATORY Range 40-60x per min Periodic breathing (alternating episodes of
rapid breathing with brief <5-10sec pause) usually normal
Healthy infant sleeps median 16.2hr per day


In non accidental head trauma subtle history with no obvious physical finding, non specific
Evaluation including CT Scan, USG, MRI. Skull X-ray might not helpful because infant can have significant injury without skull fracture
X-ray only likely to have positive findings if the were visible sign of injury
Child <2 years old might have occult traumatic head injury and retinal hemorrhage

Evaluation and stabilization of ABC’s Bedside glucose Temperature regulation If bruises or known of ICB Lab should include FBC, PT, APTT
Neuroimaging should be done after stabilization Patient should be admitted to respective
team Skeletal survey and ophthalmologic exam should
be part of evaluation

Always consider the Terrible T’s ▪ Tetralogy of Fallot (TOF) ▪ Tricuspid atresia (TA) ▪ Transposition of great vessels (TOGV) ▪ Total anomalous pulmonary venous return (TAPVR) ▪ Truncus arteriosus (TA)
CHD might not detected in newborn nursery still adequate oxygenated blood through systemic circulation via patent ductus arteriosus (PDA)
PDA closes by 2 weeks of age (delay in detecting)

Boot shaped heart Elevated cardiac apex


“Snowman sign”

Providing 100% O2 can help differentiating between cardiac vs non-cardiac
Non-cardiac at least have 10% increase in pulse oximetry value, where in cardiac have minimal changing in O2 saturation
Hyperoxia test (ABG in room air, then repeat ABG after 10min of 100% O2)
In cardiac minimal change in PaO2

Examination should include BP in 4 extremities Murmur maybe audible, absence does not exclude
cardiac defect CXR, ECG and ECHO is diagnostic Prostaglandin E1 (PGE1) as bolus of IV 0.05mcg/kg
followed by IV infusion 0.05-0.01mcg/kg/min watchout for hypotension, seizure, apnea
Definitive airway management for transportation

Typically present with symptoms of congestive heart failure. Causes: Acyanotic heart disease (ventricular septal defect,
atrial septal defect, patent ductus arteriosus, coarctation of the aorta)
Severe anemia
Trauma
Sepsis
Metabolic abnormalities
Thyrotoxicosis

Classic symptoms: tachypnea, tachycardia, hepatomegaly
History include poor/slow feeding, sweating, color change with feeding, poor weight gain

Stabilization of ABC’s CXR, ECG, FBC, serum electrolyte ECHO diagnostic of heart defect IV Furosemide 1mg/kg IV Dopamine 5-15mcg/kg/min, IV
Dobutamine 2.5-15mcg/kg/min for CVS support
Carefully not to overload this patient Cardiology consultation

Mostly cause by RSV, adenovirus, influenza Classic symptoms : rhinorrhea, cough,
congestion, apnea, significant respiratory distress and wheezing
Depending on symptoms In severe, prolonged apnea accompanied by
bradycardia, unresponsive to O2 therapy, may required intubation
Nebulization with corticosteroid therapy Sepsis evaluation should be consider Admission in premature and other comorbid
(reactive airway disease)

Present in the 1st week with vomiting, hypoglycemia or shock
Common cause in CAH : deficiency in 21 hydroxylase enzyme
CAH diagnosed at birth by routine newborn screening, but missed due inadequate blood, lab error, inability to contact family
Hypotension that unresponsive to fluids and inotropes leads to suspicion of CAH

Stabilization of ABC’s Bedside glucose, serum electrolytes (usually
had hyponatremia and hyperkalemia) IV Hydrocortisone 25-50mg/m2, imperative
to treat hypoglycemia HyperK in this patient response to fluids,
however in symptomatic with ECG changes, calcium chloride, sodium bicarbonate, insulin and glucose may be needed

Develop in infant born to mother with Grave’s disease
Cause by transmission of maternal TS immunoglobin
Present with poor feeding, failure to thrive, tachycardia, irritability, hyperthermia, vomiting, diarrhea, jaundice, thrombocytopenia, respiratory distress, heart failure and shock

Diagnosis is difficult without clear history of Grave’s disease from mother
Evaluation should include Thyroid function test
Stabilization with ABC’s IV Propranolol 0.25 mg/kg for the tachycardia IV Propylthiouracil (PTU) 1.25 mg/kg followed Lugol's solution 1-5 drops by mouth
Given 1 hour after the PTU
This will help to control the hypermetabolic state
Admit with endocrine consultation


Delay/unrecognized/uncommon and not part of routine screening and symptoms
Non specific symptoms such as poor feeding, vomiting, failure to thrive, tachycardia, tachypnea, or irritability
Occasionally symptoms of seizures, lethargy, hypoglycemia, apnea, temperature instability, and acidosis.
Physical exam findings are usually normal

Stabilization with ABC’s Bedside glucose FBC, serum electrolytes, pH, lactate,
ammonia, LFT, urinalysis for reducing substances and ketones
Main goal : stop exposure to protein that maybe converted to toxic metabolic and clear the body of toxic byproduct


In any rectal temperature >38 C Sign and symptoms : poor feeding, irritability,
apnea, hypothermia, jaundice, rashes, increased sleeping, seizures, or vomiting
Maternal and fully physical exam might help

Stabilization with ABC’s Full septic evaluation : CBC, blood culture,
urinalysis, urine culture, cerebral spinal fluid [CSF] culture and analysis, and CXR
To administer broad spectrum antibiotic in sepsis / life threatening symptoms
In neonatal herpes early recognition and treat with acyclovir may decrease mortality

IV Ampicillin 50-100mg/kg and IV Gentamicin 2mg/kg OR
IV Cefotaxime 50-100mg/kg IV Acyclovir 20mg/kg


Inappropriate mixing of water and powdered formula
Overdilution of concentrated liquid of premixed formula
This may result life threatening electrolyte disturbances or failure to thrive
Hyponatremia may present as seizures and immediate correction to stop seizure

Malrotation caused by abnormal rotation of bowel in utero result in an unfixed portion of bowel that may later twist on itself resulting volvulus and bowel ischemia/death
Diagnoses as early in 1st month of life Symptoms include bilious emesis and poor
feeding, lethargy and shock in advanced state

Stabilization of ABC’s Fluids resuscitation,
NGT placement, surgical consultation
AXR might normal, sign of bowel obstruction or classic double bubble sign

Life threatening, might unrecognized History of constipation, with additionally
history of unable to pass meconium in 1st 24hours of life
Poor feeding, vomiting, irritability, abdominal distention, hematochezia and shock
Stabilization of ABC’s Fluid resuscitation Administration of broad spectrum antibiotic AXR : enlarged or dilated section of colon Need surgical consultation

Classical disease of premature neonates Similar presentation with Hirschsprung
enterocolitis Management includes stabilization of ABC,
fluid resuscitation, NGT placement AXR demonstrate pneumatosis intestinalis /
portal air Administration of broad spectrum antibiotic
and surgical consultation

Most common, neonate may represent normal healthy baby
Evaluation depend on presentation ED management include stabilization, lab
evaluation Based on hospital protocal


Uncommon in this group, can be result from maternal ingestion in BF mother, homeopathic remedies, drug overuse
Most common “teething gel” ED management primarily supportive and
based on clinical presentation Hospitalization might required for
observation and monitoring

Neonate suspect with seizure difficult to diagnose
History can include their newborn not acting right or more somnolent
Neonate had immature cortical development, seizure activity might not tonic-clonic
Symptoms include lip-smacking, abnormal eye or tongue movement, pedaling, apnea


Describing event “frightening to the observer and is characterized by some combination of apnea, color change, marked change in muscle tone, choking, or gagging”
ED management : depending on historical information provided by observer and examination
Hospitalization maybe appropriate for observing and monitoring

Common differential diagnosis of ALTE Sepsis/Meningitis/Encephalitis
Pneumonia/RSV
Hypothermia/hypoglycemia
Anemia
ICB
Acid base disturbance/Electrolyte abnormalities/IEM
Seizures
GERD
Child abuse

Further history
Feeding well previously, 2oz every 2hours
Starting to sucking poorly and taking less than half oz every feeding
On examination difficult to arouse, slightly jaundiced and mottled, other examination unremarkable
Temp 35.5, HR 190, RR 50, BP 66/38, CRT >2sec
IV access obtained via scalp FBC : WCC raise, electrolyte normal. UFEME
clear. Infant was given IV NS 20ml/kg bolus and
started on maintenance fluids IV Ampicillin and IV Gentamicin was initiated LP was performed : no evidence of meningitis Blood C&S showed Group B Strep

Antibiotic was changed to penicillin in view of sensitivity and continue for 10days
Infant was discharge well after 12 days of hospitalization

Neonatal emergencies may provoke anxiety in ED clinician
Mnemonics “THE MISFITS” is a helpful tools Infant rare entity Sign and symptoms are non specific To treat unstable neonate narrow down
diagnosis begin life-sustaining treatment ensure safe disposition

References
Evidence Based Review of Neonatal Emergencies in Pediatrics, Aug 2010
Medscape Emergency Medicine : Neonatal Emergencies
Pediatric Protocol 3rd edition, 2013