national latino aids awareness day cultural competency workshop conceptual overview
TRANSCRIPT

National Latino AIDS Awareness Day
Cultural Competency WorkshopConceptual Overview
Objectives
• Define and understand key terminology
• Discuss the implications of demographic trends for health disparities
• Explain how cultural beliefs shape clinical encounters
• Describe effective techniques for working with minority patients

Latino or Hispanic?• Latino Population
• Many cultures that include people from:• North America ∙ Central America • South America ∙ Caribbean
• Languages: English, Spanish, Portuguese, Mayan, Guarani
• Diverse background of individuals indigenous of:• African, European, Anglo, Asian, Middle Eastern descent
• “Hispanic” inclusive of only Iberian Peninsula in Spain
• Guyana, French Suriname, & some non-Spanish speaking indigenous groups not consider themselves “Latino”
Culture Is…?
A. Things: Tools, clothing, buildings, art
B. Ideas: Thoughts, beliefs, values, expectations
C. Behaviors: Traditions, rituals, manners, roles, language
D. Taught/Learned
E. Passed from generation to generation
F. All of the above

Culture• A concept (an idea; something formed by
mentally combining all of the characteristics or particulars related to that subject)
• An integrated pattern of knowledge, beliefs, behaviors, whose soul purpose is to transmit this knowledge to succeeding generations
• A unification process, which combines customary beliefs, shared attitudes, and values

Health as a Cultural Construct
• Culture Defines:• How health care information is received
• How rights and protections are exercised
• What is considered to be a health problem • How symptoms and concerns are expressed
• Who should provide treatment for the problem
• What type of treatment should be given
• In Latin America health is• “the perfect harmony between your internal and external
world”
• In the U.S. health is• “the absence of illness”

Cultural Competency is…?
A. The ability to work effectively in cross-cultural
situations
B. A course offered at UNO
C. Knowledge of every cultural norm and more
D. Both A and C
E. All of the above
How would a Culturally Competent Health Care Facility Operate?
• The facility is capable of delivering the highest quality care to every patient regardless of race, ethnicity, culture, or language proficiency
• The facility is engaged in an intentional and continuous process of learning about and integrating cultural knowledge into every facet of what they do to better serve culturally diverse communities
• Staff hold a deep respect for cultural differences and are eager to learn, and are willing to accept, that there are many ways of viewing the world

BE SAFE Model
•Barriers to Care – real or perceived gaps
•Ethics – principles determining “right” or “wrong”
•Sensitivity – cultural awareness by provider
•Assessment – collecting data in context of pt culture
•Facts – understanding of pts beliefs and values
•Encounters – awareness of communication cultural norms

Barriers to Care
• Linguistic Issues
• Access to Care and HIV Testing
• Constructs of Culture and Gender
• Stigma
• Bias of Health Care Provider
Ethics• Principles that should guide health care facilities
1.Autonomy- information necessary for an informed decision
2.Beneficence – putting the patient’s best interest first
3.Non-malfeasance – “above all, do no harm”
4.Justice – all individuals treated equally regardless of culture, race, ethnicity, or language barriers
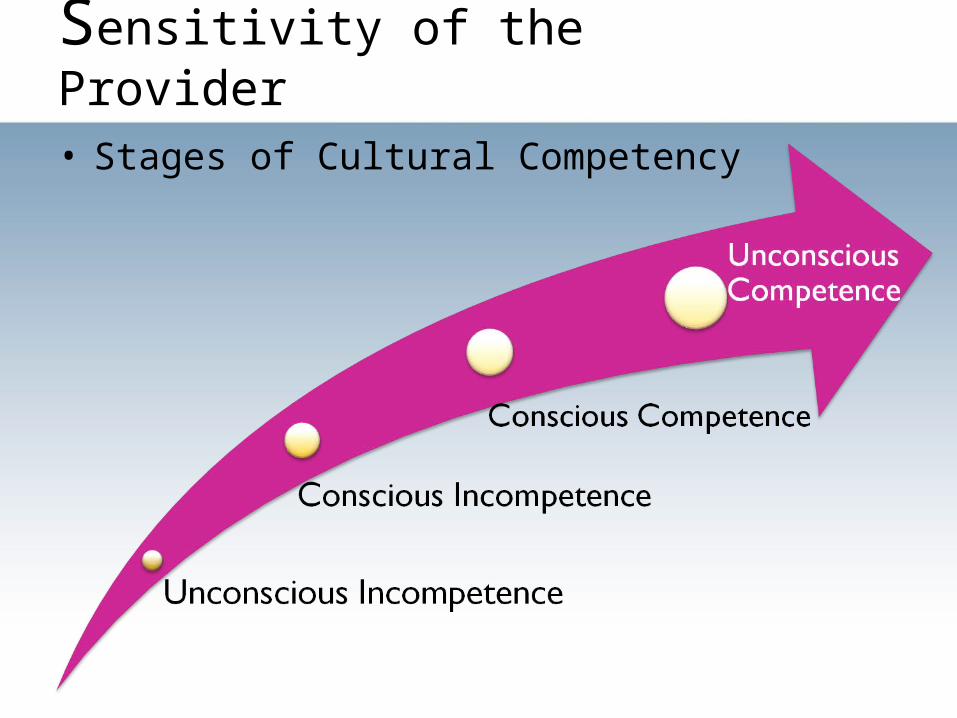
Sensitivity of the Provider• Stages of Cultural Competency
Unique Issues
• Low tolerance for anything that involves time
• Facilitation of translation through use of family or friends as translators
• + more multilingual signs are now used in health care settings
• Heavy accents are associated with poverty, lower socio-economic levels, etc

Unique Issues
• No 15 minute “one size fits all” model• Physicians usually meet patients in their office
before exam
• Often treat the whole family and ask about them
• Eyesight problems or illiteracy?
• Folk Medicine• Using herbs & oils allows a sense of control
• Consider an active coping process

Assessment• Culturally Based Assessments and Treatment Plans
• ETHNIC Model
• Explanation – “Why do you think you have these symptoms?”
• Treatment – “What kinds of medicines have you tried?”
• Healers – “Have you sought advice from folk healers?”
• Negotiation of treatments plan
• Determine the Intervention
• Collaborate to make possible the optimal and holistic
treatment

Assessment• Explanatory Model
• “What do you think caused your problem?”
• “Why do you think it started when it did?”
• “What do you think your sickness does to you?”
• “How severe is it?”
• “What kind of treatment do you think you should receive?”
• “What are the most important results you hope to
achieve?”
• What are the chief problems your sickness has caused?”
• What do you fear most about your sickness?”

Facts• Cultural Beliefs and Values
• Fatalismo• Familismo• Simpatia• Confianza• Respeto• How can these affect the clinic
visit?
• Gender Roles• Marianismo & Machismo
• Use of Folk Medicine
• Fatalism• Family• Friendly, Humble, &
Vulnerable • Trust• Respect

Encounters
• Eye contact – demonstrates respect
• Facial Expression – an unexaggerated, friendly smile
• Gestures – stand up, walk to, & greet patient
• Touch – greet with handshake and offer handshake upon completion of the encounter
• Voice Intonation – speaking loudly will not
understanding
• Addressing Latino Patients – the use of titles
• The Use of Interpreters

Demographic Changes and Health Disparities
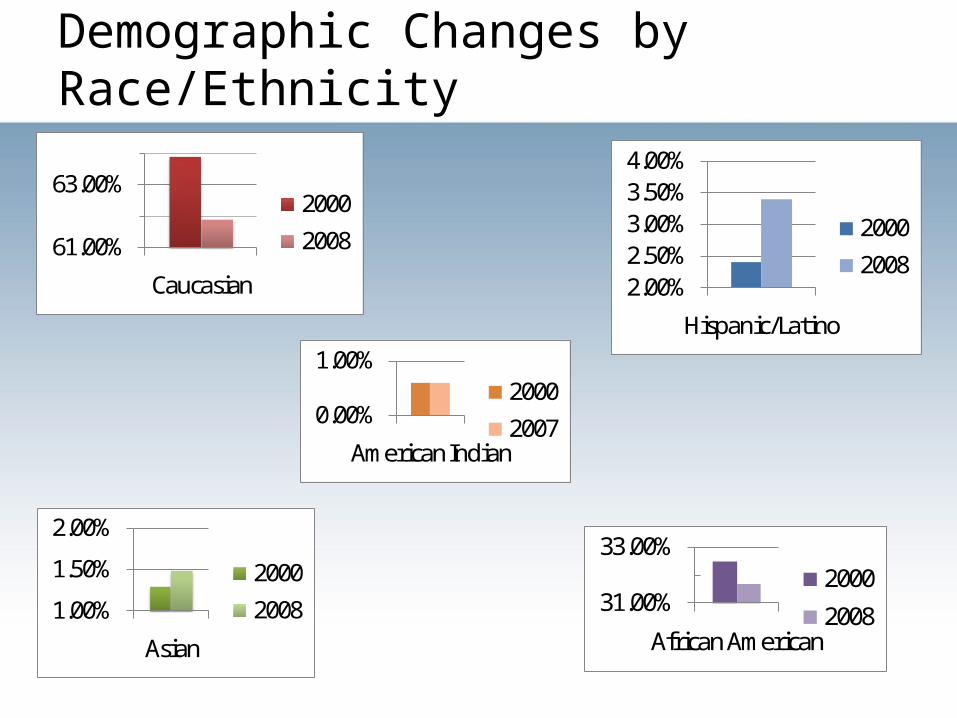
Demographic Changes by Race/Ethnicity
31.00%
33.00%
African American
2000
2008
61.00%
63.00%
Caucasian
2000
2008
2.00%2.50%3.00%3.50%4.00%
Hispanic/Latino
2000
2008
1.00%
1.50%
2.00%
Asian
2000
2008
0.00%
1.00%
American Indian
2000
2007
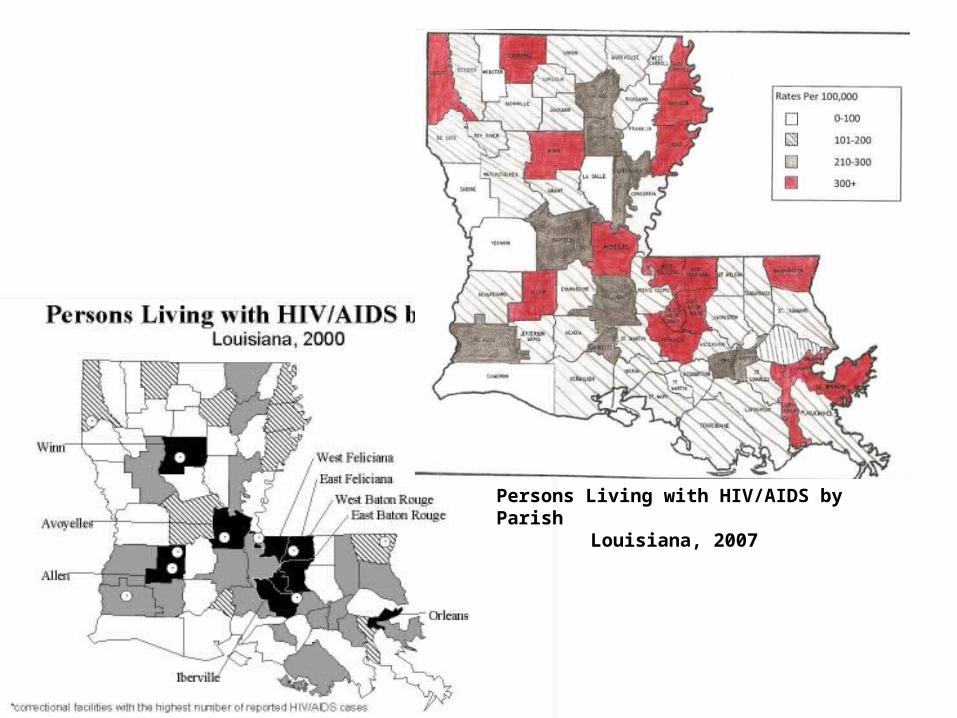
Persons Living with HIV/AIDS by ParishLouisiana, 2007

Latino Population Map Key
>9%
7-9%
4-7%
<4%

Nationwide
• Latinos comprise 15% of the US population, but accounted for 17% of all new HIV infections in 2006
• Incidence of HIV/AIDS 3X the rate for Whites
• Latino males accounted for 18% of all males living with HIV/AIDS
• Latina females accounted for 15% of all females living with HIV/AIDS
• In 2005, HIV/AIDS was the fourth leading cause of death among Latino men and women aged 35–44
• Most common methods of HIV transmission were: • For males: 1) MSM sexual contact 2) Injection drug use
3) High-risk heterosexual contact
• For females: 1) High-risk heterosexual contact 2) Injection drug use
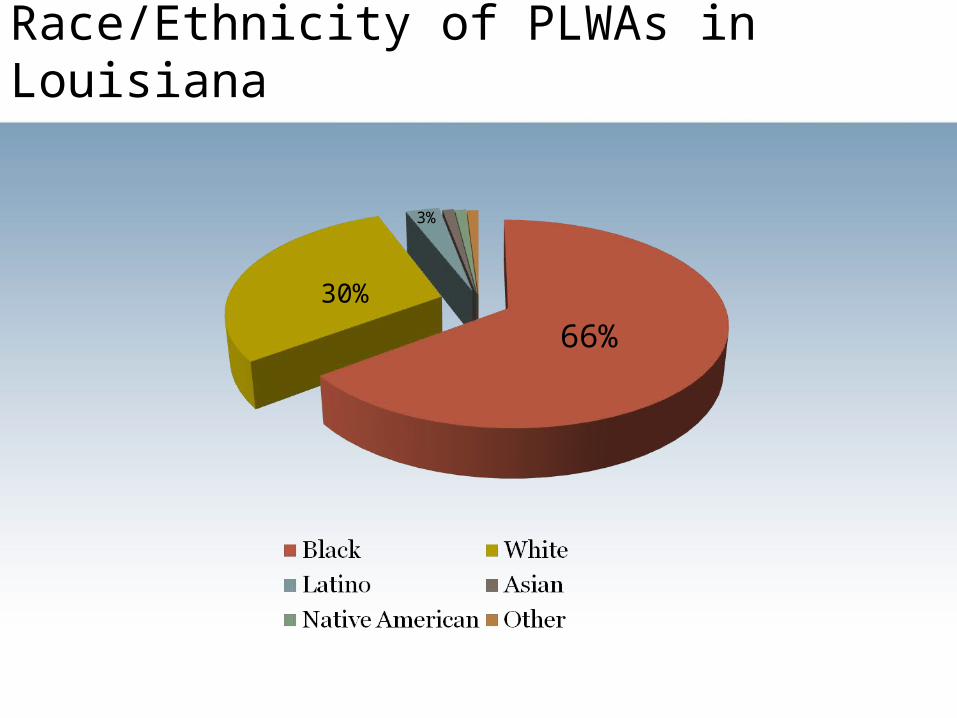
Race/Ethnicity of PLWAs in Louisiana
66%
3%
30%

Southern Region of Louisiana Rates Among Latino/Hispanics• There are a reported 579 Cases of HIV/AIDS in
Louisiana Among Latinos/Hispanics
Region: Region 1New Orleans Area
Region 2Baton Rouge Area
Region 3Houma Area
Region 4Lafayette Area
Region 5
# of HIV/ AIDS:
305 43 17 45 80
Percent: 5% 1% 3% 4% 9%

Latino Population• Many languages, many cultures
• The Effects of Hurricanes• Pre-K: substantially Honduran and other Central
American professionals• Clustered, well educated, well paying jobs in health
care, business, and government
• Post K:• Influx of less educated largely male laborers• Mexico, Nicaragua, Brazil• Some undocumented, limited knowledge of foreign
culture • Dispersed

Health Disparities Defined
• Population-specific differences in the presence of
• Disease
• Health outcomes
• Access to health care

Latino Population• Implications for healthcare
• Language & Health Care Expectations• “Latino physicians show a friendliness to
patients, and ask about the family”
• Pre-natal care for undocumented/Spanish speaking women
• Documentation• Domestic & Occupational Barriers to Care• Acculturation conflicts• Educational difficulties

Barriers to Care• Linguistic Issues – English, Spanish, Portuguese, Guarani, etc.
• Access to Care and HIV Testing• Under/uninsured – lack of citizenship, job characteristics, poverty• Education – 50% Latinos not completing high school• Transportation, no childcare, excessive waiting times, can’t miss work
• Constructs of Culture and Gender• Religious beliefs• Gender roles• Fatalistic views of life – “que sera, que sera”
• Stigma – greater than in U.S. culture
• Bias of Health Care Provider

Tragic Consequences:
Cases of Inadequate Communication
• Misinterpretation of a single word led to a patient's delayed care and preventable quadriplegia

Tragic Consequences:
Cases of Inadequate Communication
• After 36 hours of work up for a drug overdose, comatose patient reevaluated
• Diagnosis: Intracerebellar hematoma with brain-stem compression and a subdural hematoma secondary to a ruptured artery
• Hospital paid $71 Million settlement
Tragic Consequences Case #2
Misinterpretation• Spanish speaking
woman told a resident that her two-year old had “hit herself” when she fell off her tricycle
• Resident misinterpreted two words
• W/O interpreter present, mother signed over custody of her two children

Conclusions
• All patients have the right to fair and competent care
• Race, ethnicity, language, and culture must be included when planning care for the patient
• Cultural competency in health care is the ability to work cross-culturally in order to address the needs of the patient.
Resources• Delta AETC archives (1999-2009) PowerPoint
Presentations
• National Minority AIDS Education and Training Center (2002) BE SAFE: A Cultural Competency Model for Latinos. Washington D.C., Howard University
• Louisiana Department of Health and Hospitals Office of Public Health (2009).Louisiana HIV/AIDS Surveillence Quarterly Report (6/30/09)
• Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520–529.
• CDC. WISQARS [Web-based Injury Statistics Query and Reporting System] Leading causes of death reports, 2005 [2005 reports re Hispanic/Latinos]. Accessed March 18, 2008.