national audit of intermediate care national conference birmingham, sept 12 th 2012 professor...
TRANSCRIPT

National Audit of Intermediate Care
National ConferenceBirmingham, Sept 12th 2012
Professor Finbarr C. MARTIN Geriatrician
Guys and St Thomas’ Hospitals & King’s College LondonPresident, British Geriatrics Society

Intro
Well done !
• Starting data informed discussion is good• Linking organisational and patient level
data is good• This was a vital first step

How did we get here?(and what might we have lost sight of on route?)
• Damon has given the policy context and aspiration
• The aspirations are at many levels
– Improved experience for patients
– ?? For carers
– Better outcomes for patient?
– More sustainable public services (ie efficiency)
– Reducing inequity and inequalities
• Being integrated or even being the glue in the system is proving a challenge
• Are the 10, 20 and social care building blocks the problem?

Key considerations
What service problem are we trying to solve ?
- a system level diagnosis is needed JSNA
What is the clinical nature of the work ?
- necessary to define the skills needed
Who are the right patients/users ?
- need evidence of ability to benefit
How is it done best
- dearth of evidence on this
What are the success parameters ?
- at system and individual levels

What are JSNA may wish to consider(From DH guidance)
● the number and occupancy of beds in acute and community
● incidence rates of emergency admissions for people over 75
● the average length of stay for certain index conditions
● the rates of new admissions to care homes
● the pattern of repeat admissions
● discharge locations from acute care eg. of people over 75
● the locations of people 3 and 12 months after leaving IC
● the number of people receiving intensive home care.

Key considerations
What service problem are we trying to solve ?
- a system level diagnosis is needed JSNA
What is the clinical nature of the work ?
- necessary to define the skills needed
Who are the right patients/users ?
- need evidence of ability to benefit
How is it done best
- dearth of evidence on this
What are the success parameters ?
- at system and individual levels

Some Clinical issues
• Criteria for acceptance
– Medically stable
– Ability to benefit from rehab
– Needing significant mental health input
• Does it matter that geriatricians were hardly involved in this service largely for older people?
• Should post acute care be an opportunity for systematic CGA based care?
• What is in the black box (ie patients as well as the interventions!)
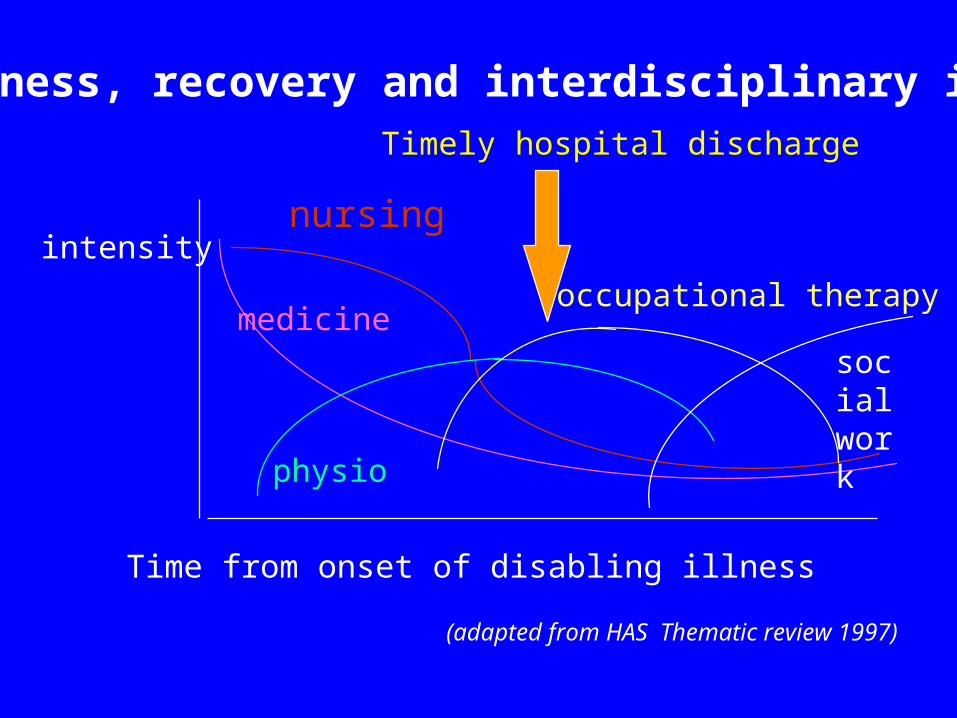
Illness, recovery and interdisciplinary inputs
intensity
Time from onset of disabling illness
nursing
medicine
physio
occupational therapy
socialwork
(adapted from HAS Thematic review 1997)
Timely hospital discharge

Vicious Cycle of Dependency
Incomplete recovery
Readmissions and LTC increased dependency
Vulnerable to change
This is what IC is trying to impact

Some Clinical issues
• Criteria for acceptance
– Medically stable
– Ability to benefit from rehab
– Needing significant mental health input
• Does it matter that geriatricians were hardly involved in this service largely for older people?
• Should post acute care be an opportunity for systematic CGA based care?
• What is in the black box (ie patients as well as the interventions!)

Does the evidence from RCTs help ?
RCTs can clarify causality,
ie treatment x given to patient y produces outcome z(more commonly than chance or placebo, but not
always)-------------------------------------------------so what is treatment x ?and who is patient y ?what is the importance of the context ?what else affects outcome and individual variation ?

Who is patient y
eg. Supported discharge teams
Lambeth Gloucester
Bartel 15 (11-18) 16 (15 -17)
Cognitive impairment mild/moderate nil/mild
morale low low
functional change slight slight
Controls at home 40% 66%(at 6 months) Impact of intervention significant not significant
What does success imply?
Low morale or high discharge related anxiety may :– predict those most likely to benefit– predict those with higher rate of adverse
outcomes
Δ Risk adverse schemes miss the point !!

What is treatment x ? –eg duration
Supported/Early discharge teams costs
Kettering (acute) orthopaedic 4-6 days same or less
West London (rehab) orthopaedic 9 days more
Kettering (acute) chest disease etc 9 days same or less
Bristol (mixed rehab) 15 days same
Lambeth (mixed older people) 22 days less
Nottingham (mixed older people ) less
So we need to know the nature of the problem to be solved, and for whom, to interpret the LOS and resources etc

How might audit help?
• Later presentations make good suggestions
• Encourage commissioners to be strategic• Encourage services to combine clinical
governance across sectors
• Encourage clarity of purposes • Be holistic rather than functional