myocardial infarction
DESCRIPTION
Myocardial InfarctionTRANSCRIPT
Myocardial InfarctionTutorial group #3
Tutorial group #3: Members• Presenter: Angeline Maranata (0961050048)• Slider/time keeper: Alfonsina C. Pentury (0961050090)• Sources:
– Anastasia Febrianti (0961050001)– Ayunita Permata (0961050022)– Irvan R. Amanu (0961050031)– S. Dian Tanjung (0961050134)– Michael R. Marampe (0961050144)– Meylani Bith (0961050125)– Marsha D. Sari (0961050140)– Basten J. Siahaan (0961050167)
Case Report• ♂ 71y.o complained: dyspneau with
chest pain since morning• History: hypertension (the onset has not
been known yet), smoker, obese,physical inactivity
• Analysis findings:– BP: 180/100mmHg– BW: 80kg– Glucose plasma: 265mg/dl– Elevation of CPK, CK-MB, and Troponin T/I– ECG result: ST elevationExplain this phenomenone and plan themanagement of this case.
Difficult medical terms
• CPK: Creatine Phosphokinase. An enzyme which found inbrain, skeletal muscle, and heart. Non-spesific marker ofcardiology disorder. It rises within 4-8h after infarct andreturn to normal after 48-72h post-infarct and also can berisen by brain injury, convulsion, and myopathy
• CK-MB: one of the isoenzymes of CreatinePhosphokinase, which is found in cardiac tissues. It ismore spesific than CPK although can be risen by cardiacsurgery, cardioversion, myocarditis.
• Troponin T/I: protein that is restricted in cardiac muscle. Itis most spesific and sensitive marker to identify cardiacmuscle necrosis. It is elevated within 1-3h after infarct andremain elevated after 7-10 days post-infarct.
• ST elevation: The elevation of segment ST inelectrocardiogram, which indicates the necrosis of cardiacmuscle.
(Harrison’s Principle of Internal Medicine 18th edition)

Hypothesis
Aging, hypertension, obesity,smoking, and physical inactivity arerisk factors of Coronary Heart Disease

Hypertension
Aging
Smoking
Obesity
Physical
inactivity
Mind Mapping
Cardiac musclehypertrophy
Cardiaccompensation
Heart failure dyspneau
AtherosclerosisTotal occlusionof coronaryartery
Cardiacmuscleinfarction
ST elevation
CPK enzym >>
CK-MB enzym >>
Troponin T/I >>
Glucose plasma >>
Chest pain
Presipitating factors:muscle spasm,thrombus embolism

Working Diagnosis
• Accoding to WHO:– Characteristic chest pain– Significant elevation of Biochemical
Markers of MI– ST segment, T wave, and Q wave
abnormalities2 out of 3: MI (Myocardial Infarction)

Outlines• Definition of Myocardial Infarction (MI)• Etiology and Predisposing Factors of MI• Cardiovascular system changes in
Elderly• Pathophysiology of MI• Clinical Manifestations of patient with MI• Management of patient with MI• Complications of MI• Differential diagnosis of MI• Outcomes of patient with MI• Prevention to avoid MI

Definition of MI
Myocardial Infarction:Cell death of cardiac myocytescaused by ischemia, which is theresult of a perfusion imbalancebetween supply and demand.
Universal Definition of MyocardialInfarction: American Heart
Association. 2007
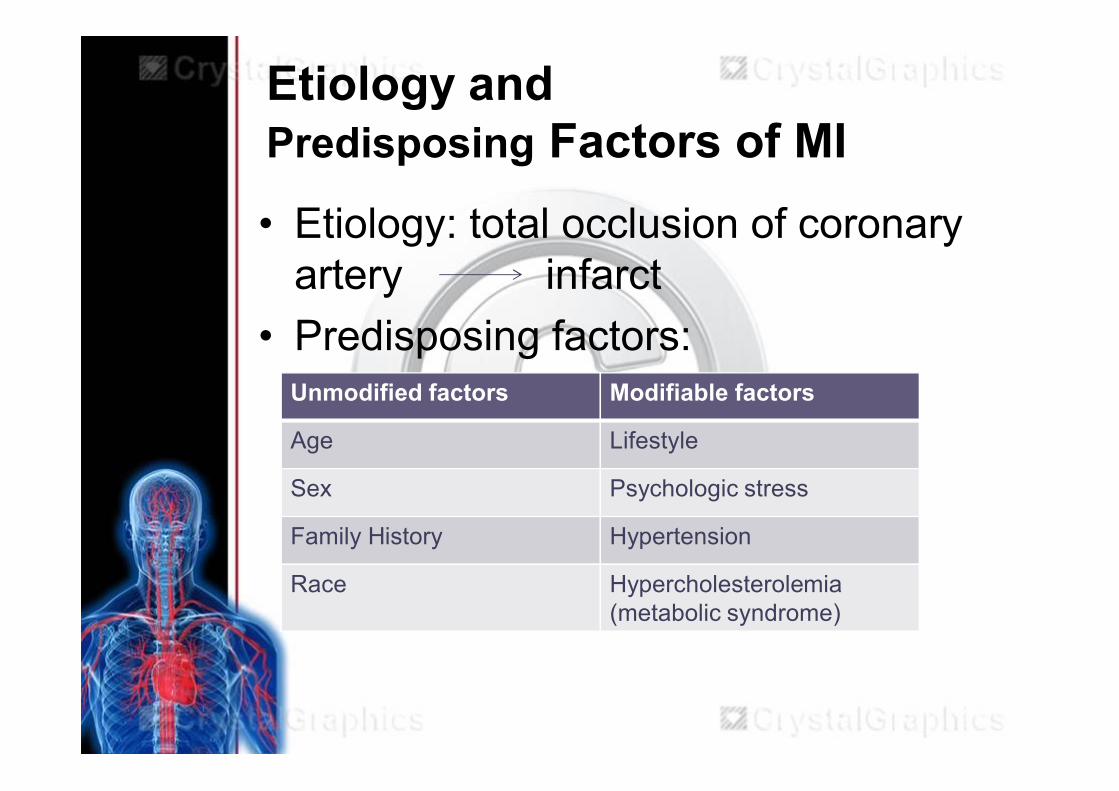
Etiology andPredisposing Factors of MI• Etiology: total occlusion of coronary
artery infarct• Predisposing factors:
Unmodified factors Modifiable factors
Age Lifestyle
Sex Psychologic stress
Family History Hypertension
Race Hypercholesterolemia(metabolic syndrome)
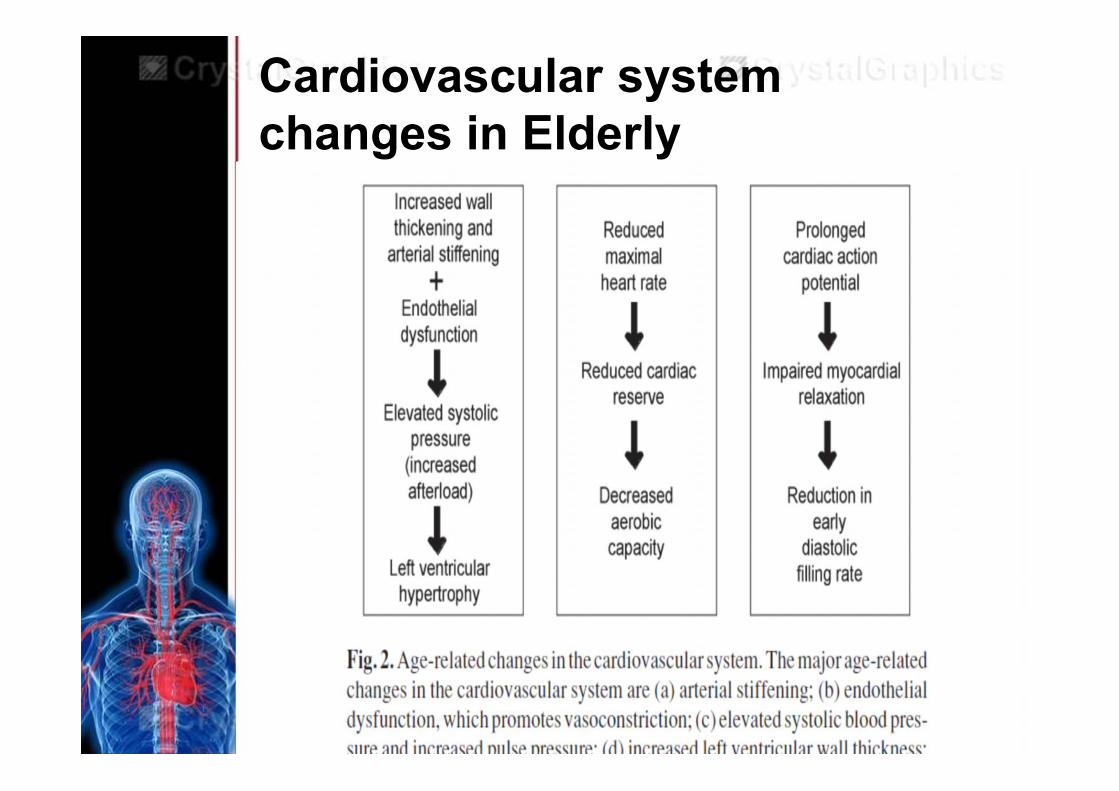
Cardiovascular systemchanges in Elderly

Pathophysiology of MI

Clinical Manifestations ofpatient with MI
Characteristic pain:• Pressure• Tightness• Heaviness+ palpitation+ heartburn+ persistent shortness of breath+ weakness, dizziness, loss ofconsciousness
Radiates to neck, jaw, back, leftarm, or both arm, possible toepigastrium: visceral pain
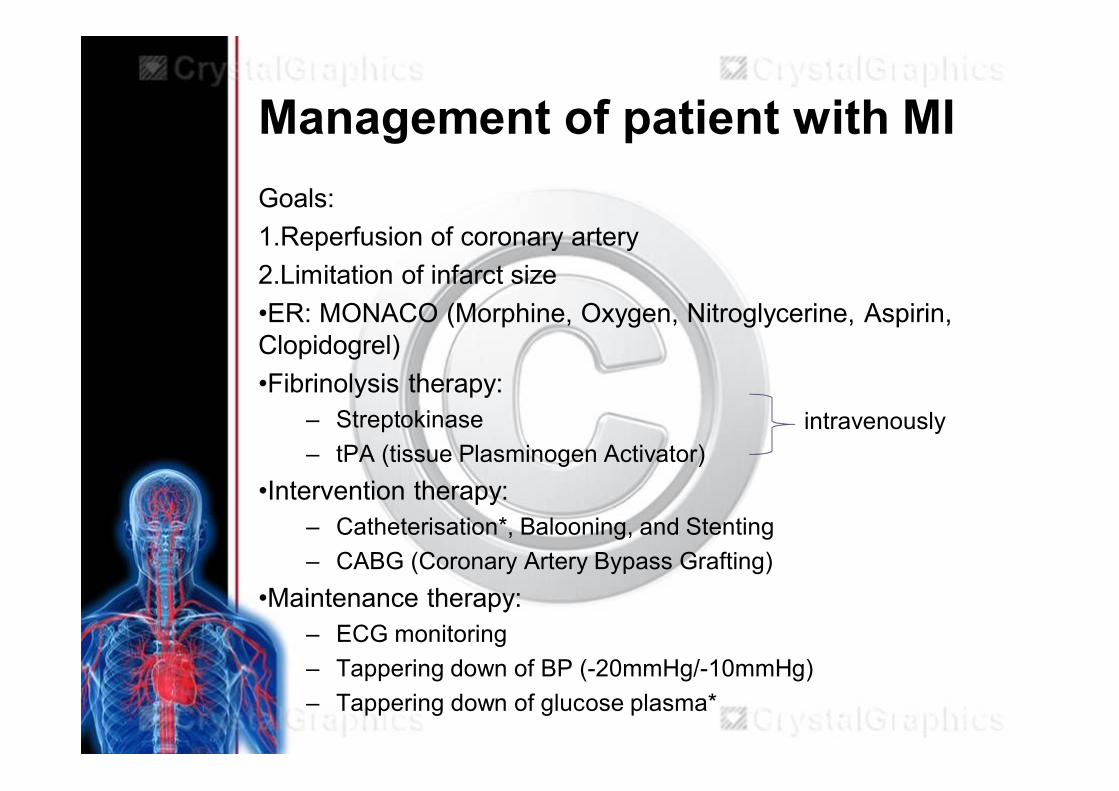
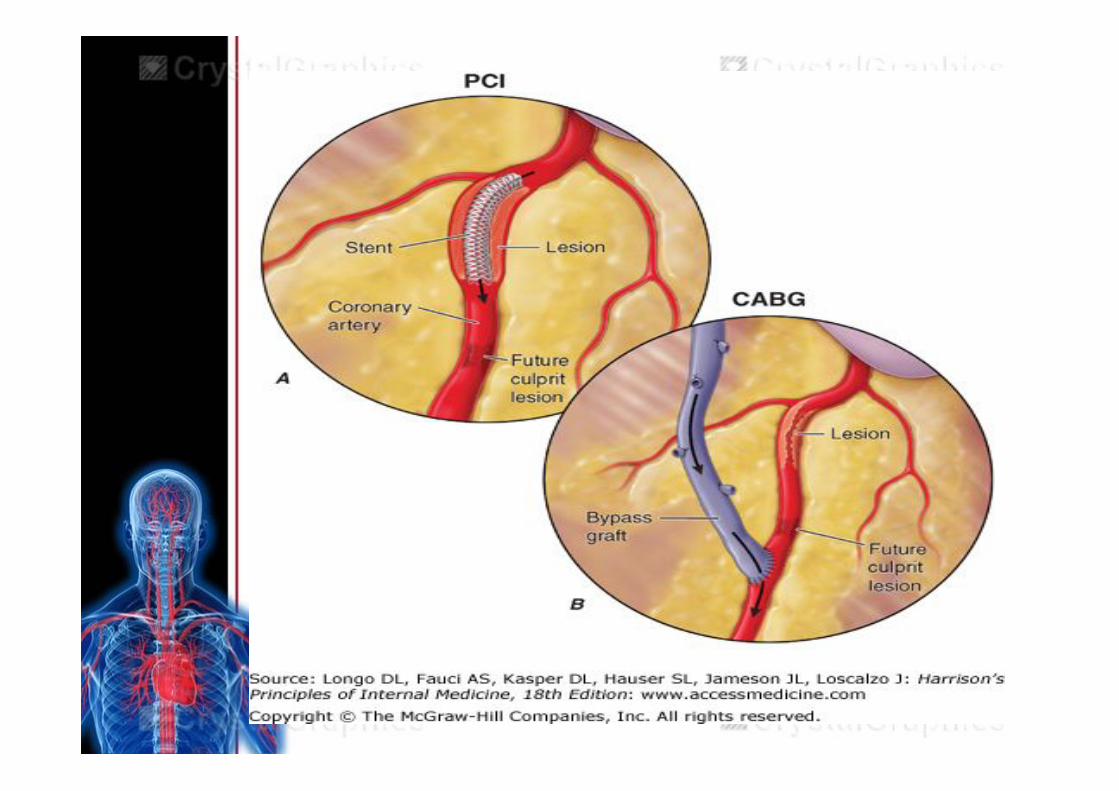
Management of patient with MIGoals:1.Reperfusion of coronary artery2.Limitation of infarct size•ER: MONACO (Morphine, Oxygen, Nitroglycerine, Aspirin,Clopidogrel)•Fibrinolysis therapy:
– Streptokinase– tPA (tissue Plasminogen Activator)
•Intervention therapy:– Catheterisation*, Balooning, and Stenting– CABG (Coronary Artery Bypass Grafting)
•Maintenance therapy:– ECG monitoring– Tappering down of BP (-20mmHg/-10mmHg)– Tappering down of glucose plasma*
intravenously
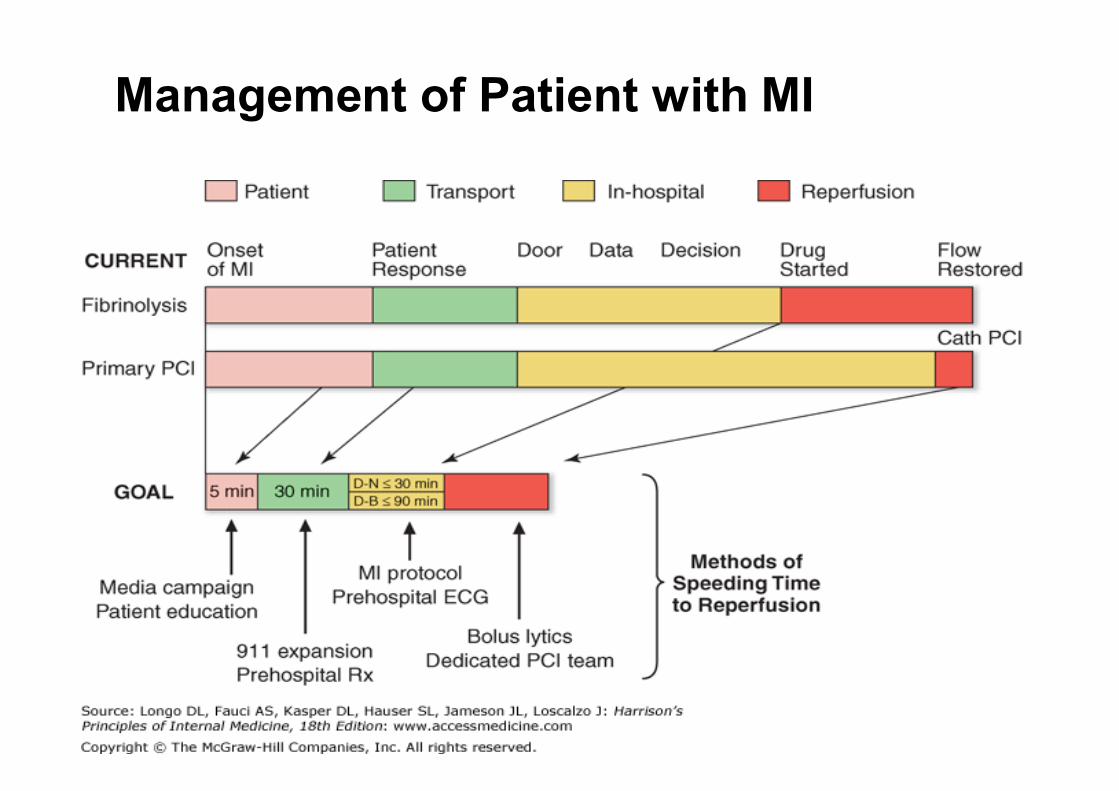
Management of Patient with MI
Complications of MI• Reperfusion injury• Acute heart failure• Aneurysm of heart• Cardiac muscle cells rupture• LBBB or RBBB• Ventricular arrhytmias:
– Fibrilation– bradhyarrhytmia
• Cardiogenic shock
• Hypovolemia

Differential Diagnosis of MI
System Disease Symptoms Key distinguishingfeatures
Cardiac Pericarditis Sharp, pleuritic painaggravated by changesin position
Pericardial friction rub
Gastrointestinal GERD(GastroesophagealReflux Disease)
Burning substernal andepigastric discomfort, 10-60 minutes in duration
Aggravated by large mealand postprandialrecumbency; relieved byantacid
Vascular Pulmonary Embolism Sudden onset of dyspneaand pain, usually pleuriticwith pulmonary infarction
Dyspnea, tachypnea,tachycardia, and signs ofright heart failure
Infectious Herpes Zooster Prolonged burning pain indermatomal distribution
Vesicular rash,dermatomal distribution
Symptom: Acute Chest Pain
Outcomes of Patient with MI
• Dubia et bonam: the treatment hasbeen completed under the goldenhour
• Dubia et malam: the necrotic areahas been extended heart failure

Prevention to avoid MI• Primary prevention: Healthy Lifestyle and
do exercise• Secondary prevention:
– Prevent another heart attack:• Antithrombotic agents + enteric formulation• healthy diet for heart:
– Control eating portion– Eat more vegetables and fruits– Select whole grains– Limits unhealthy fats and cholesterol
• Do exercise safely: involves large muscle groupsand maintain regular breathing pattern
– Daily walking in 30mins – 60mins regulary– Cycling
References1. Auntman EM. ST elevation Myocardial Infarction.
Braunwald Heart’s Disease. 8th edition. In editor: Libby.Saunders Elsevier. 2007. p: 1207-24, 1234-1289
2. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL,Loscazio J: Harrison’s Principle of Internal Medicine 18th
edition: www.accessmedicine.com3. Phibbs, Brendan. Coronary Artery Disease. The Heart: The
Basic Guide to Heart Disease. 2nd edition. In editor: FranDestefano. Lippincot William and Wilkins. 2007 p: 42-52
4. Webb RC, Inscho RW. Age-related changes inCardiovascular system. Clinical hypertension and Vasculardiseases. In editor: LM Prissant. Springer. 2008 p: 11-21
5. Van Camp SF, Cantwell DJ, Fletcher GF, Smith K,Thompson PD. Exercise for Patient with Coronary ArteryDisease. American College of Sports Medicine. 1994.downloaded from:http://www.healthsystem.virginia.edu/pub/renal-services/exercise/position-stand-on-exercise-and-cad.pdfon November 10, 2012