musculoskeletal medicine course - university of manitoba · few if any standardized notes package...
TRANSCRIPT
Musculoskeletal Medicine Course Dr. Jason Peeler
MSK Course History Part of a very busy Block #5 (also Neuro & Optha)
Historically, a very poorly rated course (17% student approval rating prior to 2010)
Cited during the last accreditation review (ED-47: Use of student evaluation data in program improvement)
Host of problems identified by students: ◦ Extraordinary large # of instructors ◦ Poor sequence / organization ◦ Few if any standardized notes package or reference / support materials ◦ Dominated by the “specialist” approach ◦ etc
Ongoing Renewal Since 2010 What’s changed? ◦ New Course Director ◦ Reorganize, re-sequence & re-format. ◦ Established “educational leaders” for each section. ◦ Standardized notes package and reference materials. ◦ Establish global learning objectives for whole course, as well as each
individual sessions. ◦ More small group and case-based learning sessions. ◦ Ongoing and consistent formative evaluation for students ◦ Ongoing and specific student feedback and input for educational
leaders and course director.
Focus became the Generalist!

MSK Modules & Leaders 1. Fundamental Concepts - Dr. Jason Peeler 2. Upper Extremity - Dr. Neil Craton 3. Lower Extremity - Dr. Jason Peeler 4. Spine - Dr. Hillel Sommer 5. Rheumatology - Dr. David Robinson 6. MSK as a System - Dr. David Robinson

Other Professionals Strategically Involved (determined by course director and/or module leader)
Basic scientists (anatomy/pathology/human development) Family medicine Orthopaedics Rheumatologists Physical medicine & rehabilitation Radiology Genetics Allied health professionals (OT/PT/AT, etc) Residents / graduate students (small group learning, labs,
etc)

Consistent Approach Organization, Sequence & Format
1. Anatomy - lecture, lab & case study
2. Pathology - lecture & case presentation
3. Medical imaging – lecture, tutorial & case study
4. Common conditions of region ◦ eg. Lower extremity module - broken down by region: hip & thigh
/ knee / lower leg, ankle & foot. ◦ Lecture, tutorial & case study
5. Pediatrics – lecture
6. Surgery – lecture
7. Clinical skills – lecture and “hands-on” tutorials
8. Instructional exam – take home test and review session
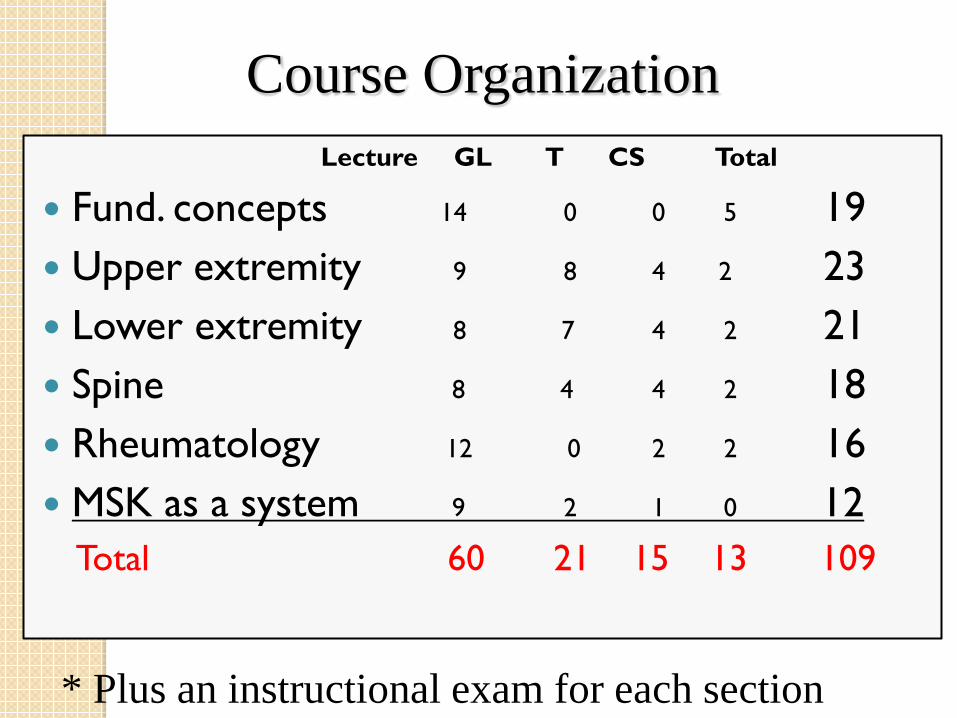
Course Organization Lecture GL T CS Total
Fund. concepts 14 0 0 5 19 Upper extremity 9 8 4 2 23 Lower extremity 8 7 4 2 21 Spine 8 4 4 2 18 Rheumatology 12 0 2 2 16 MSK as a system 9 2 1 0 12
Total 60 21 15 13 109
* Plus an instructional exam for each section

Course Goals & Objectives Focus on Preparation for Clerkship and FM Residency
Goal: To develop a clinical approach to musculoskeletal conditions which includes differential diagnosis, investigations, management options and burden of illness. Objective: Upon completion of the MSK course, the student will be able to…… Describe the normal structure and function of the MSK system, and define unique aspects of bone, joints and muscle structure/function.
Explain how macroscopic, microscopic and metabolic aspects of bone, joint (including connective tissues), and muscle structure relate to function/dysfunction of the MSK system.
Describe normal patterns of growth / development and regeneration of the MSK system.
Describe the principles and practices of injury prevention as they relate to common MSK conditions.
Describe the principles and practices used in the conservative and/or surgical management of common MSK conditions.
Explain the importance of interdisciplinary and inter-professional care in the management of common MSK conditions.
Describe the physical, psychological, financial and quality of life consequences associated with living with a common MSK conditions.
Describe the common traumatic, inflammatory, infectious, degenerative, metabolic, and congenital diseases of the MSK system. For each describe:
◦ Prevalence and age distribution
◦ Patho-anatomical and biomechanical mechanisms, and common structures and locations involved.
◦ Clinical manifestations, differential diagnosis, and natural history
◦ Role of imaging and other tests in the diagnosis and management
◦ Various management options ranging from pharmacology, physiotherapy, alternative therapies, psychotherapies and surgery.
◦ Associated disability, morbidity and mortality.
◦ Red flags in MSK care.
Describe and perform a MSK history and physical examination to determine anatomic location, differential diagnosis and management urgency.

Student Approval Rating now at 80%. Course is going in the right direction!
MSK Course Moving Forward Within CuRe

What we are building is not changing……
1. Student successful in MSK course. 2. Student to acquire knowledge and skills
required for success in clerkship. 3. Success on Medical Council of Canada –
MCCQE and LMCC 4. Success in FM clinical practice

….. How we are building it is! Course divided into M1 / M2 modules. Revised methods of delivery & evaluation. Novel methods and opportunities for delivery
of clinical skills portion of course. Integration of new ideas - Expansion of steering
committee Evolution / adaptation of course
materials, small group and case-based learning methods.
Further integration of MSK course. • Longitudinal courses • Complex patient • OSCE & PR evaluations.

M1 Course 2 weeks (Jan 6 – 17th) 34 contact hrs. Content: Fundamental concepts Anatomy Pathology Human Development Medical Imaging Baseline CS
Formative Evaluation Summative Evaluation
M2 Course • 4 weeks (Feb 16 – March 13th) • 68 contact hrs. • Content: Common conditions
of…… Upper extremity Lower extremity Spine Rheumatology Region specific CS
• Formative Evaluation • Summative Evaluation
M1 Course 2 weeks (Jan 6 – 17th) 34 contact hrs. Content: Fundamental concepts Anatomy Pathology Human Development Medical Imaging Baseline CS
Formative Evaluation Summative Evaluation
M2 Course • 4 weeks (Feb 16 – March 13th) • 68 contact hrs. • Content: Common conditions
of…… Upper extremity Lower extremity Spine Rheumatology Region specific CS
• Formative Evaluation • Summative Evaluation
Focus will continue to be the Generalist!
Current Challenges within CuRe 14 week course now condensed into 6 weeks ◦ Delivery of “normal” in 2 weeks. ◦ Availability of preceptors for small group sessions. ◦ Reliable / Valid methods of evaluation / remediation.
Selection of appropriate tutorial cases ◦ Simple vs. Complex ◦ Pediatric vs. Geriatric ◦ Congenital vs. Development vs. Acquired
Linking with longitudinal courses ◦ Clinical skills, problem solving, etc.

CuRe Course Steering Committee Jason Peeler – Athletic Therapy / Anatomy Neil Craton – Sports Medicine Hillel Sommer – Phys Med David Robinson – Rheumatology James Koenig – Radiology Susan Thompson – Orthopaedics / Pediatrics Jennifer Salter – Phys Med Kyle Perry - Pathology James Pierce - 3rd year student rep Sam Victos - 4th year student rep

Questions