muscle sparing thoracotomy
DESCRIPTION
To be well exposed, it is half the success of a surgical procedure.With adequate deflation of underlying lung, most thoracic procedures can be performed safely through a limited incision. Muscle sparing thoracotomy is easy to perform with appropriate attention to chest wall anatomy. The take home message is: BIG SURGEONS NOT NECESSARILY DO BIG INCISIONS.TRANSCRIPT
MUSCLE SPARING THORACOTOMY
Prof. Abdulsalam Y Taha
School of MedicineUniversity of Sulaimani
Iraq
https://sulaimaniu.academia.edu/AbdulsalamTaha
INTRODUCTION Thoracic Surgery in Sulaimani Teaching
Hospital was began in 2003 Thoracic Surgeons in 2009: 3 The standard technique: Posterolateral
thoracotomy. Occasionally: partial muscle sparing
thoracotomy.
10/15/14 2Prof. Abdulsalam Y Taha
OUR PROJECT To introduce and popularize MUSCLE
SPARING THORACOTOMY. WHY? Good impact on patient care. Realistic. Team of Surgeons & Anaesthetists.
10/15/14 3Prof. Abdulsalam Y Taha
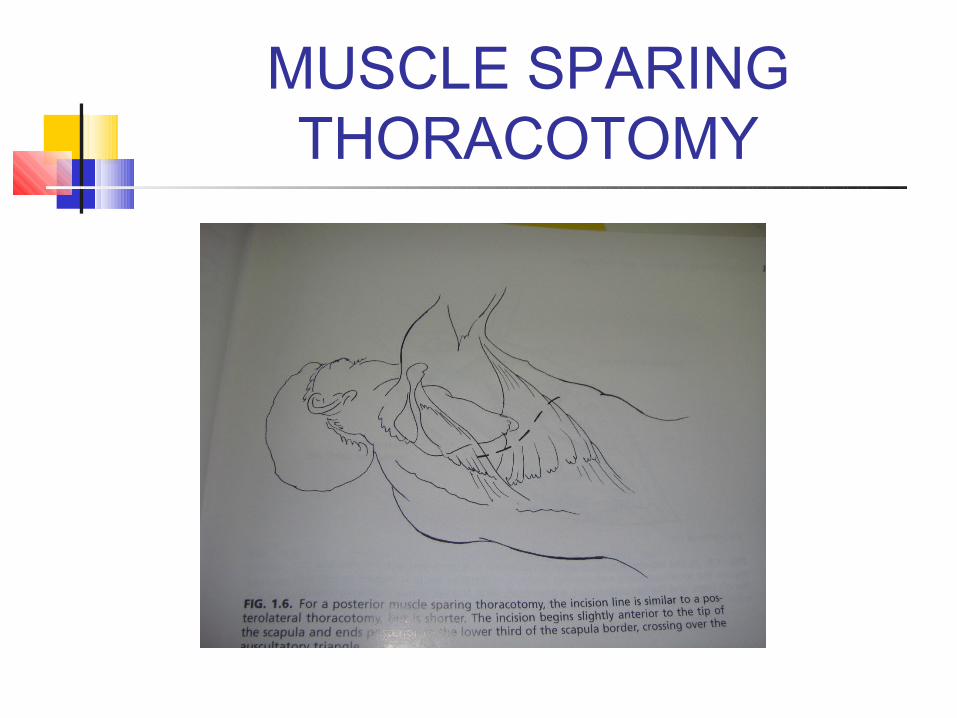
MUSCLE SPARING THORACOTOMY

MUSCLE SPARING THORACOTOMY
FEATURES:● Small.● No muscle cutt ing.● No impairment of shoulder or arm mobil i ty.● Less painful.● Less postop Resp complications.● Shorter hospital stay.● Better cosmetic result.● Preserved Latissimus dorsi m.□ Limited Exposure.

TECHNIQUES OF ONE LUNG VENTILSTION
10/15/14 6Prof. Abdulsalam Y Taha

VASCULAR & BRONCHIAL STAPLERS
10/15/14 7Prof. Abdulsalam Y Taha

STAPLED STRUCTURES
10/15/14 8Prof. Abdulsalam Y Taha

POSTEROLATERAL THORACOTOMY
FEATURES:1. Big2. Muscle cutting3. Time consuming4. Severely painful5. Impaired arm & shoulder movement6. Bad cosmetic result7. Longer hospital stay8. Increased cost9. No lattisimus dorsi available for flap in future.10. Postop scolioses in children.11. Excellent exposure.
10/15/14 9Prof. Abdulsalam Y Taha

STAKEHOLDERS Powerful but less
interested Administration.
Powerful & Interested
SURGEONS.+_ ANAESTHETISTS.
+_ Manufacturing Co. + Little Interest &
Power Nursing Staff.
Interested but less powerful
Patients.+
10/15/14 10Prof. Abdulsalam Y Taha
PLAN OF IMPLEMENTATION Time table: 3 months. Communication with stakeholders:
surgeons, anaesthetists, administrator & companies.. different messages.
Equipments to be requested & made ready in reasonable time.
Training: surgeons & anaesthetists. Audit.
Surgeons Familiar with the technique. welcome it.
Share their experience. Unfamiliar with it: motivated to do it. Training: observing a colleague or
visiting a specialized centre. Selecting uncomplicated case to start
with..

Anaesthetists The short supply of equipments should
be solved. Meanwhile: consolidating the
experience of the trained..DLT for every adult pt.
Training the junior anaesthetists. Motivating them: training course
abroad.
ADMINISTRATION & Companies
In view of anticipated improvement in patient's care & cost saving; should be interested.
Role: to get the equipments & training opportunities..
Co.. Best deals to provide the best products for best prices & training of staff.

THREATS Reluctant training.. Motivation. Equipments may not be ready in time.. Complications: bleeding. Patient's
safety should not be compromised. Whenever
exposure is inadequate, never hesitate to extend the incision.
CONCLUSIONS To be well exposed, it is half the success of a
surgical procedure. With adequate deflation of underlying lung,
most thoracic procedures can be performed safely through a limited incision.
Muscle sparing thoracotomy is easy to perform with appropriate attention to chest wall anatomy.
Evidence from Literature
1. M Ashour. Modified muscle sparing posterolateral thoracotomy. Thorax 1990; 45: 935-938.
2. Posterior ( auscultatory triangle) Muscle sparing thoracotomy.
3. A. J. Jawad. Experience with modified posterolateral muscle-sparing thoracotomy in neonates, infants, and children.Paediatric Surgery International. Volume 12, Numbers 5-6/ July, 1997.
4. Nicolas Dürrleman and Gilbert Massard. Posterolateral thoracotomy. MMCTS (August 10, 2006).

TAKE HOME MESSAGE
BIG SURGEONS NOT
NECESSARLY DO
BIG INCISIONS.