multiple hereditary osteochondromatosis with spinal cord...
TRANSCRIPT

1 23
Child's Nervous System ISSN 0256-7040Volume 34Number 3 Childs Nerv Syst (2018) 34:565-569DOI 10.1007/s00381-017-3645-1
Multiple hereditary osteochondromatosiswith spinal cord compression: case report
Oscar García-González, J. NicolásMireles-Cano, Natalia Sánchez-Zavala,Miguel A. Chagolla-Santillan, SegioM. Orozco-Ramirez, et al.

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer-
Verlag GmbH Germany. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.
CASE REPORT
Multiple hereditary osteochondromatosis with spinal cordcompression: case report
Oscar García-González1,2 & J. Nicolás Mireles-Cano1 & Natalia Sánchez-Zavala3 &
Miguel A. Chagolla-Santillan1& Segio M. Orozco-Ramirez1 & Pedro Silva-Cerecedo1 &
Mario Murguia-Perez1 & Fernando Rueda-Franco4
Received: 7 March 2017 /Accepted: 18 October 2017 /Published online: 11 November 2017# Springer-Verlag GmbH Germany 2017
AbstractObjective The purpose of the report is to describe a patientwith hereditary osteochondromatosis and spinal cord com-pression at the thoracic level.Clinical features An 8-year-old patient with hereditaryosteochondromatosis inherited from his father presentedparaparesis in the left foot, leading to complete paralysis inboth legs.Intervention In a CT scan, a bony tumor rising from the pos-terior wall of the T3 body narrowing the spinal canal, and theMRI spinal cord compression at the same level and thehydrosyringomyelic cavity extended to the conus medullaris;with an anterior thoracic approach to T2–T4, the fibro-cartilaginous tumor was removed, and the stabilization wascompleted with bone graft and a plate. Two months after sur-gery, the patient recovered strength in both legs.Conclusions A detailed family history through examination-guided advanced imaging and biopsy provides useful infor-mation for diagnosis and appropriate management ofoccupative lesions in patients affectedwithmultiple hereditaryexostosis.
Keywords Multiple hereditary exostosis . Spinal cordcompression . Transsternal approach
Introduction
Osteocartilaginous exostosis or osteochondroma is the mostcommon benign tumor of the bone, comprising 9% of all bonetumors [1, 2]. Many osteochondromas are asymptomatic; com-plications can involve the bones, nerves, and tissues via intrinsicchange or mass effect. Both genders can be affected, but there isa slight male predominance with an incidence of 1 in 50,000 [3].
Most osteochondromas arise in the appendicular skeleton,occurring as solitary or multiple entities;10% of patients withosteochondroma possess multiple exostoses. This entity is aninherited autosomal dominant condition called hereditary mul-tiple exostosis (HME) [4, 5] which is characterized by the pres-ence of multiple osseous prominences, arising most commonlyfrom the metaphysis of a long bone. These exostoses can alsobe found on the diaphysis of long bones, on flat bones, and/oron vertebrae [6, 7]. Whether solitary or HME, these lesionsseldom occur along the vertebral column, with an incidenceof approximately 3% [8]. Spinal cord compression resultingfrom osteochondroma is an extremely serious complication ofHME. It occurs more frequently in the cervical spine, C2 beingthe vertebra most affected [9–11]. The thoracic vertebrae are thesecond in frequency. The neurological presentation is slow dueto the growth characteristics of the tumor. The symptoms aremyelopathy and paralysis [8, 12–15].
Case description
An 8-year-old boy was diagnosed with HME, inherited fromhis father whowas diagnosedwith a biopsy of one appendicular
* Oscar García-Gonzá[email protected]
1 Hospital Regional de Alta especialidad del Bajío, León, Guanajuato,Mexico
2 Department of Pediatric Neurosurgery, Hospital Regional de AltaEspecialidad del Bajío, Blvd. Milenio 130, 37660 León, Guanajuato,Mexico
3 Universidad de Guanajuato, León, Guanajuato, Mexico4 Instituto Nacional de Pediatría, México City, Mexico
Childs Nerv Syst (2018) 34:565–569https://doi.org/10.1007/s00381-017-3645-1
Author's personal copy
skeleton tumor, with no genetic mutation studies available. Thepatient presented bony prominences in both wrists, shoulders,ribs and knees, with 2 months of progressive weakness in theleft extremity, leading to complete paralysis in both legs.
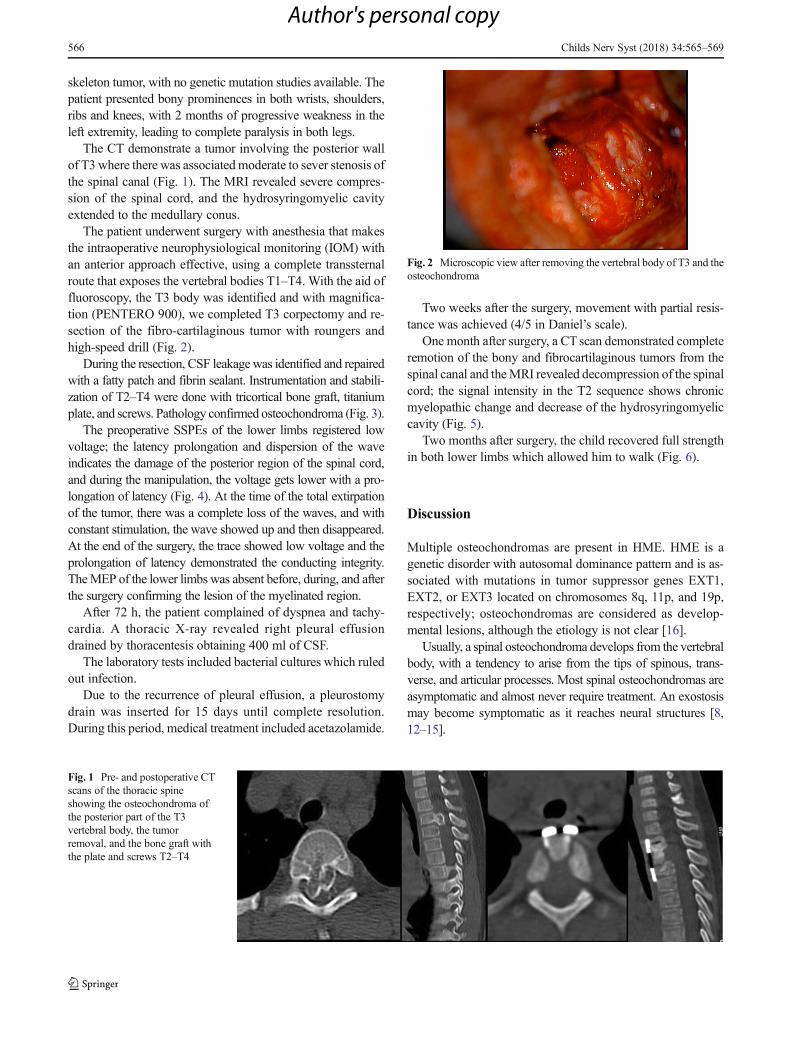
The CT demonstrate a tumor involving the posterior wallof T3 where there was associatedmoderate to sever stenosis ofthe spinal canal (Fig. 1). The MRI revealed severe compres-sion of the spinal cord, and the hydrosyringomyelic cavityextended to the medullary conus.
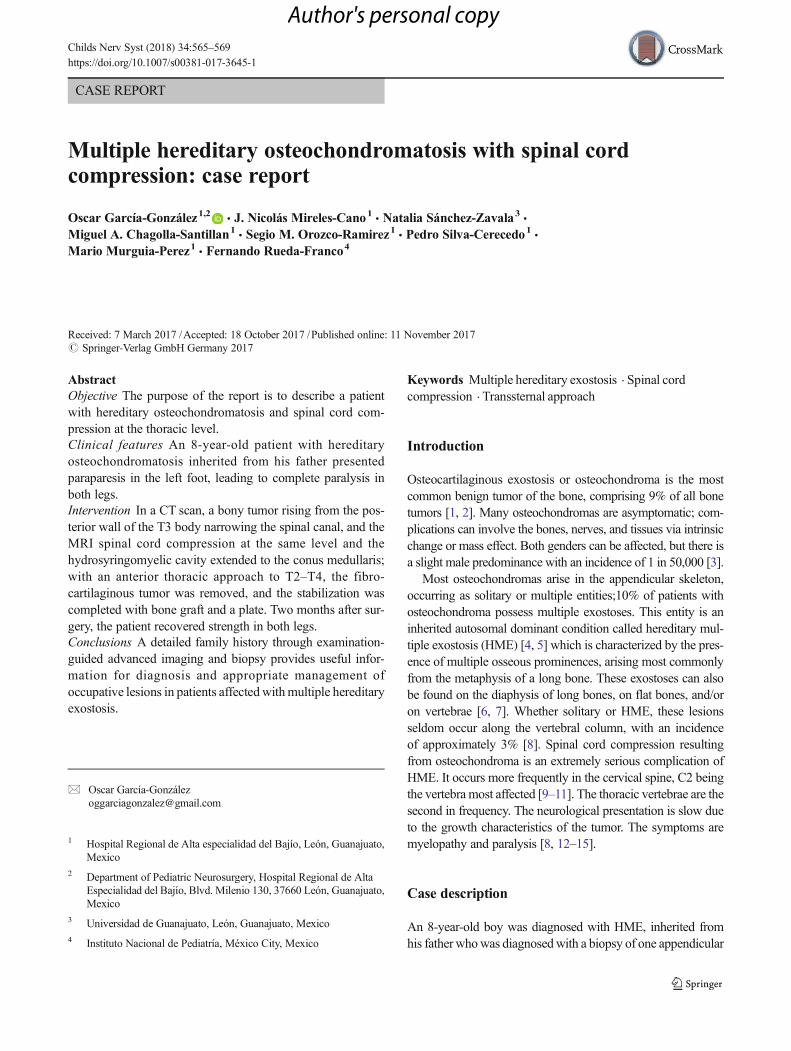
The patient underwent surgery with anesthesia that makesthe intraoperative neurophysiological monitoring (IOM) withan anterior approach effective, using a complete transsternalroute that exposes the vertebral bodies T1–T4. With the aid offluoroscopy, the T3 body was identified and with magnifica-tion (PENTERO 900), we completed T3 corpectomy and re-section of the fibro-cartilaginous tumor with roungers andhigh-speed drill (Fig. 2).
During the resection, CSF leakage was identified and repairedwith a fatty patch and fibrin sealant. Instrumentation and stabili-zation of T2–T4 were done with tricortical bone graft, titaniumplate, and screws. Pathology confirmed osteochondroma (Fig. 3).
The preoperative SSPEs of the lower limbs registered lowvoltage; the latency prolongation and dispersion of the waveindicates the damage of the posterior region of the spinal cord,and during the manipulation, the voltage gets lower with a pro-longation of latency (Fig. 4). At the time of the total extirpationof the tumor, there was a complete loss of the waves, and withconstant stimulation, the wave showed up and then disappeared.At the end of the surgery, the trace showed low voltage and theprolongation of latency demonstrated the conducting integrity.TheMEP of the lower limbs was absent before, during, and afterthe surgery confirming the lesion of the myelinated region.
After 72 h, the patient complained of dyspnea and tachy-cardia. A thoracic X-ray revealed right pleural effusiondrained by thoracentesis obtaining 400 ml of CSF.
The laboratory tests included bacterial cultures which ruledout infection.
Due to the recurrence of pleural effusion, a pleurostomydrain was inserted for 15 days until complete resolution.During this period, medical treatment included acetazolamide.
Two weeks after the surgery, movement with partial resis-tance was achieved (4/5 in Daniel’s scale).
One month after surgery, a CTscan demonstrated completeremotion of the bony and fibrocartilaginous tumors from thespinal canal and theMRI revealed decompression of the spinalcord; the signal intensity in the T2 sequence shows chronicmyelopathic change and decrease of the hydrosyringomyeliccavity (Fig. 5).
Two months after surgery, the child recovered full strengthin both lower limbs which allowed him to walk (Fig. 6).
Discussion
Multiple osteochondromas are present in HME. HME is agenetic disorder with autosomal dominance pattern and is as-sociated with mutations in tumor suppressor genes EXT1,EXT2, or EXT3 located on chromosomes 8q, 11p, and 19p,respectively; osteochondromas are considered as develop-mental lesions, although the etiology is not clear [16].
Usually, a spinal osteochondroma develops from the vertebralbody, with a tendency to arise from the tips of spinous, trans-verse, and articular processes. Most spinal osteochondromas areasymptomatic and almost never require treatment. An exostosismay become symptomatic as it reaches neural structures [8,12–15].
Fig. 1 Pre- and postoperative CTscans of the thoracic spineshowing the osteochondroma ofthe posterior part of the T3vertebral body, the tumorremoval, and the bone graft withthe plate and screws T2–T4
Fig. 2 Microscopic view after removing the vertebral body of T3 and theosteochondroma
566 Childs Nerv Syst (2018) 34:565–569
Author's personal copy

For an optimal study of the spinal column, CT imaging ispreferred, to evaluate the anatomic details and evidence ofneuroforaminal intrusion. MRIs are also used to detect asso-ciation with damage in adjacent tissues (e.g., spinal cord nerveroots) [8, 17, 18].
Several surgical approaches to the cervicothoracic junctionhave been described, including posterior, posteolateral, ante-rior, or anterolateral approaches. Posterior approaches providepoor exposure of the anterior spinal elements, have limited usein the management of complex spinal disease states, and may
Fig. 4 Intraoperative neuromonitoring. Upper row: preoperative SSPEs from the right and left limbs. Lower row: postoperative SSPEs from the rightand left limbs
Fig. 3 Pathological findingsshowed many fragments ofosteocartilaginous matrix ofmixoid aspect. Condrocytes ofregular size with abundantbasophilic cytoplasm with smallcentral nuclei surrounded by aclear pericellular space; many ofthese chondrocytes showedintracytoplasmic vacuoles andothers nuclear pyknosis. Alsoendochondral ossification withbone matrix with trabeculae. Nomalignancy findings (H&E × 100)
PreOp PosOp
Fig. 5 Pre- and postoperativeFLAIRs and T2 sequences ofMRI
Childs Nerv Syst (2018) 34:565–569 567
Author's personal copy

further destabilize the spine. The first description of a postero-lateral approach to the cervicothoracic junction was of acostotransversectomy, described in 1894 by Ménard [19] forPott disease. A purely anterior approach to the cervicothoracicjunction was initially described in 1923 and was mainly asupraclavicular approach [20]. Because the clavicle was leftintact, the exposure of the upper thoracic area was limited.Further limitations with this approach can be encountered inpatients with short necks or large shoulders. In 1957,Cauchoix and Binet [21] enhanced the exposure by combiningthe supraclavicular approach with a median sternotomy. Sincethe 1980s, various modifications to the sternum-splitting ap-proach have been made to reduce perioperative mortality andmorbidity while maintaining exposure [22]. Darling et al. re-port the experience regarding a modified anterior approach.Standard cervical approach was combined with a partial me-dian sternotomy and transverse osteotomy through the synos-tosis between the manubrium and the body of the sternum; itprovided excellent exposure from C3 to T4. There was noassociated morbidity related to the division of the manubriumor the innominate vein [23]. Comey et al. describe an ap-proach to the anterior upper thoracic spine that obviates theneed for sternotomy to access the superior end plate of T3.With adequate soft-tissue dissection and retraction, however,T3 and perhaps even T4 are easily accessible [24].
Postoperative recurrence of solitary osteochondromas(mostly non-spinal) is reported in 2–5% of cases with an in-complete resection [2, 4, 8, 10, 19, 20, 22, 25].
Conclusions
Overall, surgical approaches to the cervicothoracic junction willbe guided by the tumor’s location, extent of involvement, andhistological features, as well as the surgeon’s familiarity withthe approach. In younger patients with more benign lesions, wehave favored the transsternal approach as the best route to gainaccess to lesions localized within vertebral bodies of the upperthoracic spine allowing for their resection, interbody fusion, andreplacement with bone graft. It is technically simple to performthe approach for a trained thoracic surgeon and is safer as itprovides better exposure of the mediastinum, and thus, suffi-cient control of great vessels, including subclavian ones, givesbetter exposure of T3, T4, and even T5 vertebral bodies,allowing perpendicular sight and attack to the anterior surfaceof the upper thoracic spine and therefore good visualizing of theposterior longitudinal ligament and dura. Furthermore, newerinstrumentation materials and techniques have facilitated thesurgeon’s ability to stabilize the cervicothoracic junction. Inour case, a dural tear during the resection of the firmly attachedosteochondroma led to CSF leakage and pleural effusionrepresenting a life-threatening complication that was promptlyidentified and treated with complete resolution in the next.
Compliance with ethical standards
Conflict of interest No conflicts of interest.
References
1. Fiechtl JF, Masonis JL, Frick SL (2003) Spinal osteochondromapresenting as atypical spinal curvature. Spine 28:252–255
2. Moon KS, Lee JK, Kim YS, Kwak HJ, Joo SP, Kim IYet al (2006)Osteochondroma of the cervical spine extending multiple segmentswith cord compression. Pediatr Neurosurg 42:304–307
3. Zoboski Robert J. (2016) Compression in a patient with hereditarymultiple exostostoses: a case report J Chiropr Med
4. Kiymaz N, Dogan A, Yilmaz N, Mumcu C (2005) A giant cervicalosteochondroma. Eur J Gen Med 2:120–122
5. Shane Tubbs R, Maddox GE, Grabb PA, Jerry Oakes W, Cohen-Gadol AA (2010) Cervical osteochondroma with postoperative re-currence: case report and review of the literature. Childs Nerv Syst26:101–104
6. Küçükesmen Ç, Özen B, Akçam M (2007) Multiple hereditaryosteochondromatosis: a case report. Eur J Dent 1(3):183–187
7. Faik A, Filali SM, Lazrak N, El Hassani S, Hajjaj-Hassouni N(1995) Spinal cord compression due to vertebral osteochondroma:report of two cases. Jt Bone Spine 72:177–179
8. Khosla A, Martin DS, Awwad EE (1999) The solitary intraspinalvertebral osteochondroma. An unusual cause of compressive mye-lopathy: features and literature review. Spine 24:77–81
9. Jackson A, Hughes D, St. Clair Forbes W, Stewart G, CummingsWJK, Reid H (1995) A case of osteochondroma of the cervicalspine. Skeletal Radid 24:235–237
10. Scher N, Panje WR (1988) Osteochondroma presenting as a neckmass. A case report. Laryngoscope 98:550–553
Fig. 6 Eight-year-old boy with T3 osteochondroma 2 months aftersurgery
568 Childs Nerv Syst (2018) 34:565–569
Author's personal copy

11. Prasad A, Renjen PN, Prasad ML (1992) Solitary spinalosteochondroma causing neural symptoms. Paraplegia 30:678–680
12. García-Ramos CL, Buganza-Tepole M, Obil-Chavarría CA, Reyes-Sánchez AA (2015) Spinal osteochondroma: diagnostic imagingand treatment. Case reports. Cir Cir 83(6):496–500
13. Cherubino P, Benazzo F, Castelli C (1991) Osteochondroma of thecervical spine. Ital J Orthop Traumatol 17:131–134
14. Cooke RS, Cumming JK, Cowie RA (1994) Osteochondroma ofthe cervical spine: case report and review of the literature. Br JNeurosurg 8:359–363
15. George B, Atallah A, Laurian C, Tayon B, Mikol J (1989) Cervicalosteochondroma (C2 level) with vertebral artery occlusion and sec-ond cervical nerve root irritation. Surg Neurol 31:459–464
16. Upadhyaya GK, Jain VK, Arya RK, Sinha S, Naik AK (2015)Osteochondroma of upper dorsal spine causing spastic paraparesisin hereditary multiple exostosis: a case report. J Clin Diagn Res9(12):RD04–RD06
17. Eaton BA, Kettner NW, Essman JB (1995) Solitary osteochondromaof the cervical spine. J Manip Physiol Ther 18:250–253
18. Tang WM, Luk KD, Leong JC (1998) Costal osteochondroma. Arare cause of spinal cord compression. Spine (Phila Pal 1976)23(17):1900–1903
19. Ménard V (1894) Causes de la paraplégie dans le mal de Pott. RevOrthop:47–64
20. Kim DH, Beck CE, Dietze DD Jr et al (2000) Surgical approachesto the cervicothoracic junction. In: Schmidek HH (ed) Schmidek &Sweet operative neurosurgical techniques: indications, methods,and results, 4th edn. WB Saunders, Philadelphia, pp 2107–2121
21. Cauchoix J, Binet JP (1957) Anterior surgical approaches to thespine. Ann Roy Coll Surg Engl 21:237–243
22. Le H, Balabhadra R, Park J, Kim D. (2003) Surgical treatment oftumors involving the cervicothoracic junction. Neurosurg Focus 15(5):Article 3
23. Darling GE, McBroom R, Perrin R (1995) Modified anterior ap-proach to the cervicothoracic junction. Spine (Phila Pa 1976)20(13):1519–1521
24. Comey CH, McLaughlin MR, Moossy J (1997) Anterior thoraciccorpectomy without sternotomy: a strategy for malignant disease ofthe upper thoracic spine. Acta Neurochir 139(8):712–718
25. Pecker J, Valle B, Desplat A (1980) Lateral interscalenic approachfor tumors of the cervical intervertebral foramina. Neurochirurgie26:165–170
Childs Nerv Syst (2018) 34:565–569 569
Author's personal copy