multicystic dysplastic kidney
TRANSCRIPT
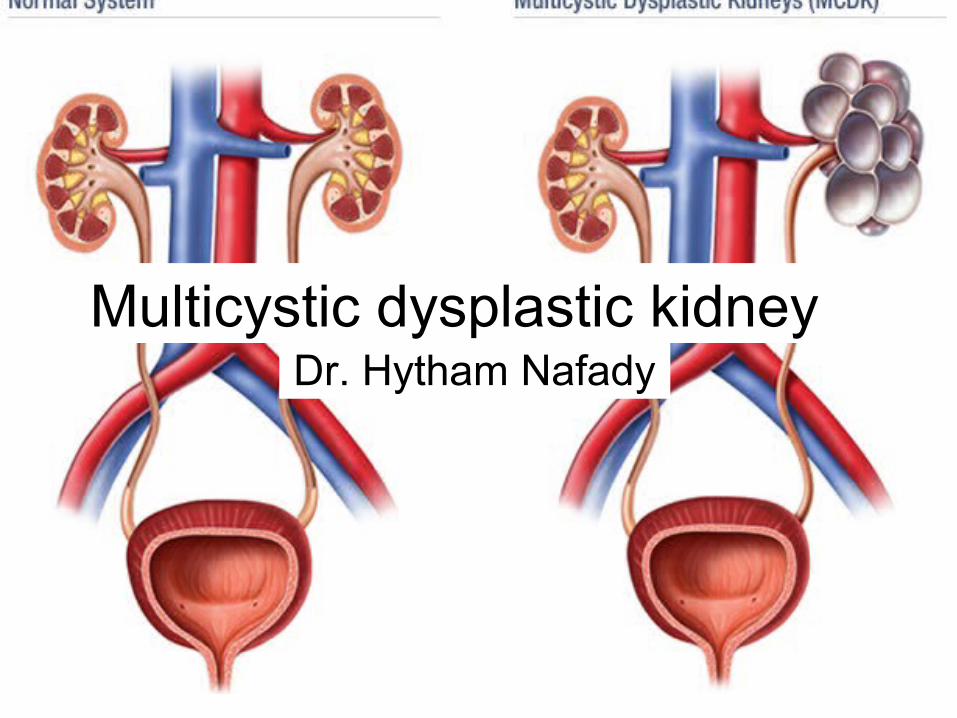
Multicystic dysplastic kidneyDr. Hytham Nafady
• Replacement of the renal parenchyma by multiple cysts & non functioning dysplastic tissue.

Etiology
• Atresia of the proximal ureter or PUJ during the metanephric phase of intrauterine development.
Pathology
• The kidney is enlarged & replaced by multiple cysts & undifferentiated mesenchymal tissue.
• The ureter is atretic.• The renal vessels are small or atretic.
Contralateral associated abnormalities.• PUJ obstruction.• Vesicoureteric reflux.Bilateral multicystic dysplsatic kidney is
incompatible with life.

Demographics
• Fetus (antenatal diagnosis).
• Neonate.
• Sex: M>F.

C.P
• MCDK is the 2nd most common cause of abdominal mass in infancy.
• Congenital hydronephrosis is the 1st most common cause of abdominal mass in infancy.

PUT
• Large mass with displacement of the gas shadows.
• Ring like densities due to cyst wall calcification.

IVP
Non functioning kidney.
Contralateral kidney:
Compensatory hypertrophy.
Associated anomalies:
• PUJ obstruction.
• Vesicoureteric reflux.

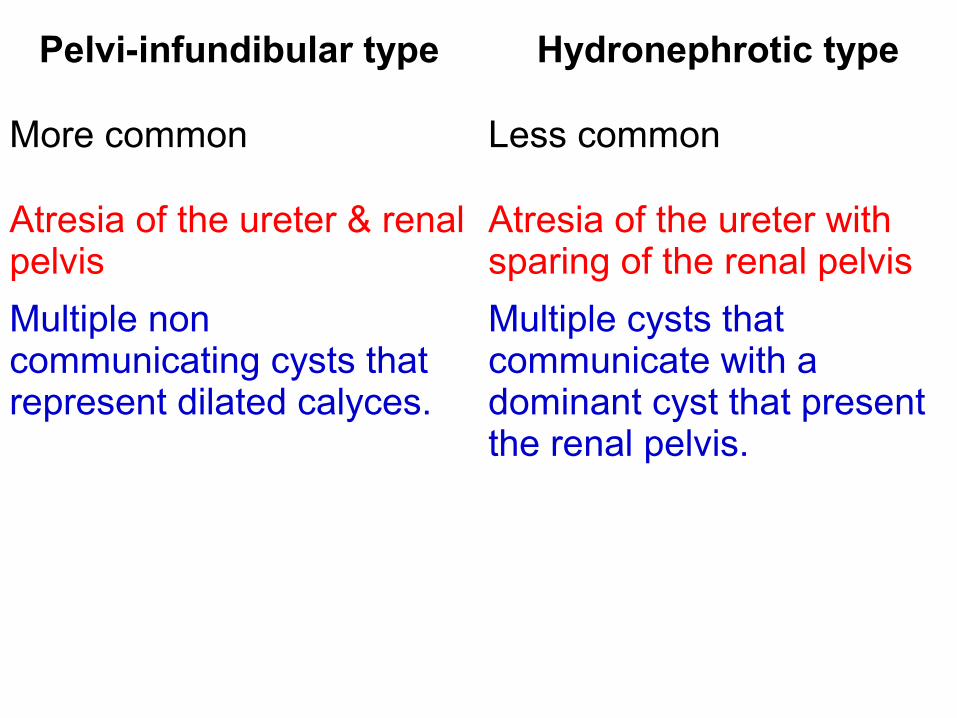
Pelvi-infundibular type Hydronephrotic type
More common Less common
Atresia of the ureter & renal pelvis
Atresia of the ureter with sparing of the renal pelvis
Multiple non communicating cysts that represent dilated calyces.
Multiple cysts that communicate with a dominant cyst that present the renal pelvis.
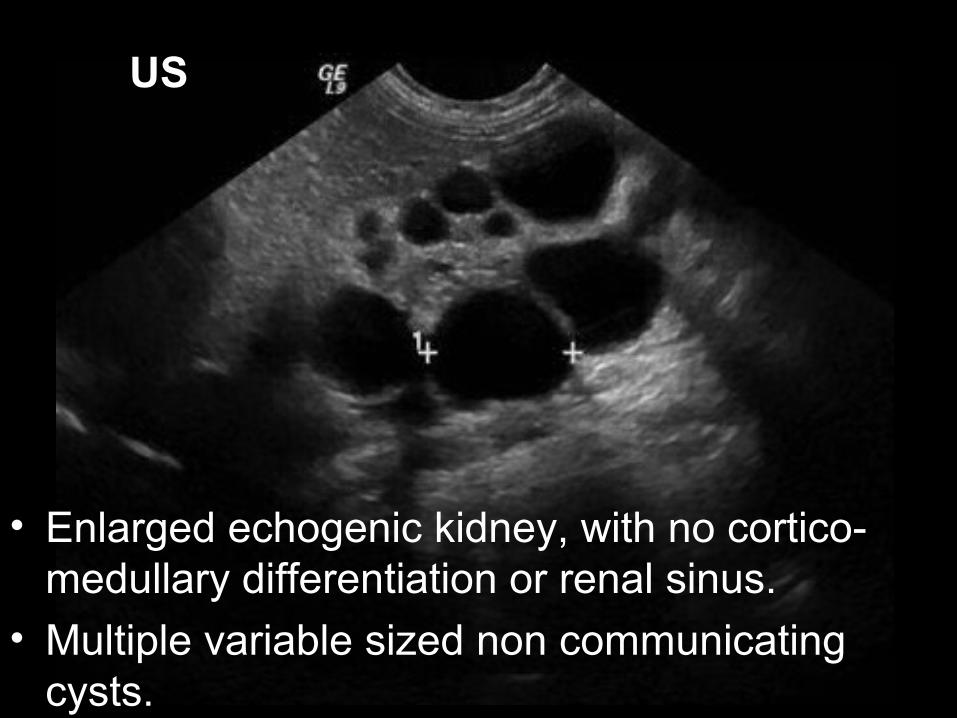
• Enlarged echogenic kidney, with no cortico-medullary differentiation or renal sinus.
• Multiple variable sized non communicating cysts.
US

Duplex
• Minimal flow in the parenchyma.
• Small or absent renal vessels.
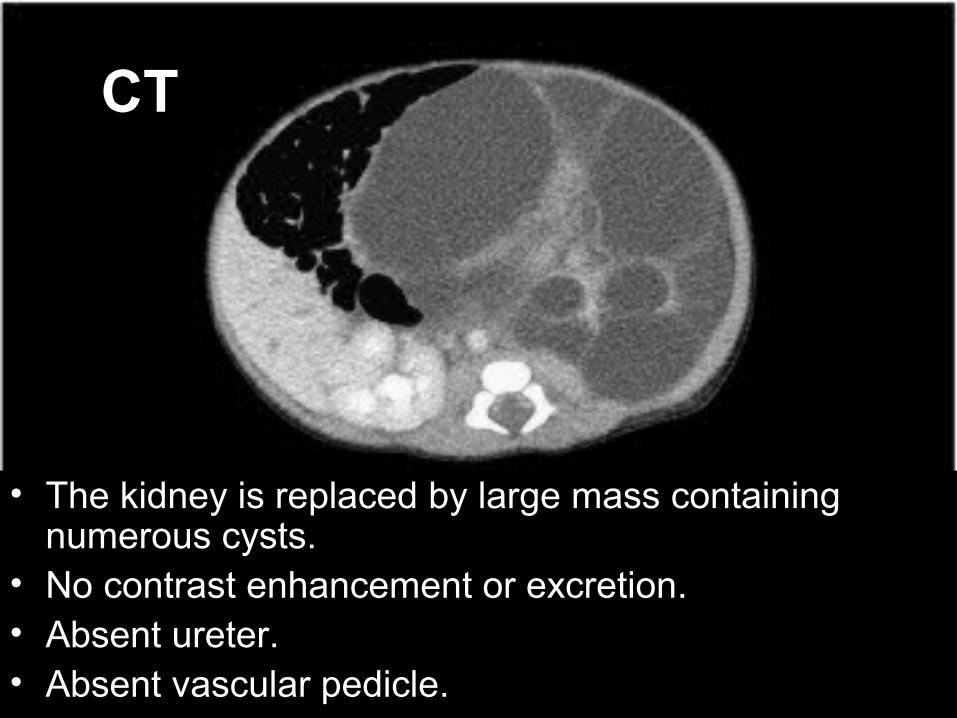
CT
• The kidney is replaced by large mass containing numerous cysts.
• No contrast enhancement or excretion.• Absent ureter.• Absent vascular pedicle.
Nuclear medicine
• MAG3 or DTPA:
• May show some flow to the kidney & may be cortical uptake, however, there is no contrast excretion.


DD of pediatric cystic renal disease
1. Multicystic dysplastic kidney.
2. Autosomal recessive polycystic kidney.
3. Multilocular cystic nephroma.
4. Nephronophthosis (medullary cystic disease).