mrcpuk - membership of the royal colleges of …uk)-annual-review-2015.pdf about mrcp(uk) the...
TRANSCRIPT

ANNUAL REVIEW 2015
MRCPUKMembership of the Royal Colleges of Physicians of the United Kingdom

About MRCP(UK) 1
Welcome from the medical director 2
Opening our doors to quality: inviting external scrutiny 4
Commitment to fairness: equality and diversity 6
International partnerships: examinations and training around the world 8
Support for training: benefits for candidates and their trainers 10
Our people: clinical leadership, appointments and thank you 12
Contents
MRCP(UK) 11 St Andrews Place, Regent’s Park, London NW1 4LE www.mrcpuk.org

About MRCP(UK)The Federation of Royal Colleges ofPhysicians of the United Kingdom setsinternationally acknowledgedstandards in medicine, building on a proud tradition of professionalexcellence, established over centuriesby British physicians.
The Federation is a partnershipbetween:
n The Royal College of Physicians ofEdinburgh
n The Royal College of Physicians andSurgeons of Glasgow
n The Royal College of Physicians ofLondon.
Working together, the Colleges developand deliver membership and specialtyexaminations that are recognised aroundthe world as quality benchmarks.
The Federation is responsible for thefollowing postgraduate medicalexaminations.
The Membership of the Royal College ofPhysicians (UK) Diploma tests the skills,knowledge and behaviour of doctors intraining. The MRCP(UK) Diploma hasbeen approved by the General MedicalCouncil (GMC) as the summativeassessment for core medical training andthe successful completion of the entirethree-part examination is a requirementfor physicians wishing to undergo trainingin a medically related specialty in the UK.
Internationally, the MRCP(UK) Diploma isalso a valued professional distinction inmany other countries.
The Specialty Certificate Examinations(SCEs) have been developed in closecollaboration with the UK specialistsocieties. Physicians in training must passthe appropriate SCE in order to gainadmission to the GMC Specialist Register.Success in the SCE certifies physicians ashaving sufficient knowledge of theirspecialty to practise safely andcompetently as consultants. The SCEs area requirement for specialist physicians inthe UK and they provide an internationalbenchmark for postgraduate medicaleducation.
1ABOUT MRCP(UK)
MRCP(UK) works with the examinationteams in the three Colleges and isaccountable to the Federation. Staffprocess applications, coordinate logisticsand communicate results to candidates.The teams also work closely with theexamining boards to:
n develop the content of the tests
n set the standards required to pass theexaminations
n guide academic development of theexaminations ensuring that theyremain the best.
MRCP(UK) monitors performance in allthe examinations and generates statisticalanalyses, which are crucial to maintainingacademic quality. MRCP(UK) alsocollaborates with academics in medicaleducation and psychometrics, who usethe data to publish work in their field.

The focus over the past year has been on systematic qualityreview, the fairness of ourexaminations and the relevanceof their content ...
2 MRCP(UK) ANNUAL REVIEW 2015

At a time of considerable change inhealthcare and medical education, onething at least remains constant – theneed for high quality assessments ofthe knowledge and bedside skills ofour doctors in training.
MRCP(UK) is proud to continue toprovide such assessments and in 2014more than 20,000 aspiring generalphysicians or specialists sat ourexaminations in over 40 countries.
The focus over the past year has beenon systematic quality review, thefairness of our examinations and therelevance of their content.
We held our first external quality reviewmeeting, in which lay people, traineesand representatives of diverse candidategroups gathered to interrogate ourprocesses, our pass standards and ourpass rates. Internally, we continued torestructure our monitoring and reportingof key performance indicators.
Everyone wants assessment to be fair.We have continued to collaborate with
stakeholders to ensure that ourexaminations do not unfairlydisadvantage specific candidates orcandidate groups. We have publishedresearch, which shows no evidence ofunfair ethnic or gender bias within ourclinical examinations, and we continue toseek and research other factors that maycontribute to differences in performance.It is increasingly clear that support andguidance for trainees in the workplace,be that in preparation for high-stakesexaminations, their training in general, ortheir integration into UK medical orbroader social culture, is a vital part ofthe solution.
High-stakes examinations are powerfuleducational tools and it is often saidthat assessment drives learning. Thisbrings a responsibility to ensure that thecontent of our examinations directsyoung doctors towards the knowledgeand skills that our patients desire andneed. The imminent changes topostgraduate training in the UK,outlined in the Shape of Training reportled by Professor Greenaway, present areal opportunity to tailor curricula andtheir linked assessments to modernmedical practice. We will ensure thatMRCP(UK) examinations arecomplementary to the more formativelearning experiences that occur in theworkplace.
WELCOME FROM THE MEDICAL DIRECTOR 3
Welcome from themedical director
International uptake of our examinationscontinues to develop. However, werecognise that international employersand regulators increasingly seek evidenceof high quality training in addition topassage through stand-aloneexaminations when considering youngdoctors for promotion, employment orfurther training opportunities. Therefore,we are working with our sisterorganisation the Joint Royal Colleges ofPhysicians Training Board, and ourinternational partners, to adapt andextend our model of postgraduatemedical training to benefit doctors andpatients in other countries.
MRCP(UK) seeks to deliver examinationsthat are fair, relevant and of the highestpossible quality. Achieving this requirescommitment, enthusiasm, effort andexpertise. I thank all the clinicians and staffwho have worked together to create anddeliver a suite of examinations that arevital in maintaining standards of care foran inestimable number of patients aroundthe world.
Dr Andrew ElderMedical Director, MRCP(UK)

Opening our doors to quality: inviting externalscrutiny
Academic quality is our top priority, because our qualificationsare trusted by so many people. The career stakes are high forcandidates. Employers need toknow they are hiring safe andcompetent doctors. Above all,patients have a right to expectthe highest standards of care,from doctors who areknowledgeable, skilled anddedicated to their welfare.
To meet this responsibility, we make it a matter of routine to consult widely,share our data, and listen to ideas forcontinuous improvement.
We also believe that assessments are anintegral part of training. Therefore weseek to influence our peers, for examplethrough representation on key working
Asking
groups organised by the Academy ofMedical Royal Colleges. We are alsoworking with the Joint Royal Colleges ofPhysicians Training Board (JRCPTB) to stayabreast of, and have an impact on, thetraining agenda (please see page 10).
Voices at the tableOne of our key advances this year wasto invite external representatives to joinour MRCP(UK) Standards AdvisoryReview Group (MSARG), which met forthe first time in February 2015. Thepurpose of the group is to gain anobjective, outside view of MRCP(UK)quality management, and the passstandards required in our Diplomaexaminations.
Invitations were accepted by a widevariety of stakeholders, including theConference of Postgraduate MedicalDeans (COPMeD), NHS Employers, andsome of the individual deaneries. Wewere also pleased to welcome others
representing the interests of trainees,the public, and diverse groups ofcandidates, including internationalmedical graduates. An independentexpert on psychometrics and arepresentative from JRCPTB completedthe group.
The pass standards and pass rates for allcomponents of the MRCP(UK) Diplomawere agreed to be appropriate.
Recommendations from the meetingincluded:
n reviewing the Part 1 examination toensure its scientific content remainsclinically relevant (although theemphasis on clinical science, and theformat, should remain)
n considering ways to reduce thenumber of papers and the length ofthe Part 2 Written examination
n increasing patient involvement in thePart 2 Clinical examination (PACES).
A pilot project to test active involvementof surrogates in assessing candidates hasalready been conducted, and analysis ofthe data is underway.
Inviting
4 MRCP(UK) ANNUAL REVIEW 2015
Academic quality is our top priority ...
Educational value
Fairness
Culture
RecruitmentPatient needs
Candidateconcerns
Fitness forpurpose
Externalviewpoints
Developing
Listening
The group confirmed that PACESremains a good test of core bedsideclinical skills, and that the scoring systemand passing standards should remain asthey are.
Members were impressed by the workundertaken to investigate the issue ofdifferential attainment (where somegroups of candidates, for example froma particular gender or ethnicbackground, achieve higher scores thanothers – please see page 6). Theyencouraged us to develop this further.
OPENING OUR DOORS TO QUALITY 5
‘I was very pleased to have been invited to attend the recent MSARGmeeting. It was good to see the Colleges being so willing to be open to discuss and receive feedback on their quality. It shows a genuinedesire to ensure that the MRCP(UK) examinations remains fit-for-purposeand an international benchmark of academic and clinical knowledge and skills.’
Dr Inam HaqDirector of Undergraduate Studies and Reader in Medical Education and Rheumatology,Brighton and Sussex Medical School
‘Maintaining the standards of key examinations such as MRCP(UK) isessential to achieving and maintaining the highest quality healthcarethat the NHS can deliver. However, it is also important that thosestandards meet the needs of employers within the NHS, ensuring thatwe are training the right number in the right specialties, and deliveringfully-trained doctors with the right skills to meet the healthcare needs oftoday’s patients. It was therefore an excellent opportunity that, as thevoice of employers for the NHS in England, I was able to contribute tothe annual standards review. With all parts of the examinationconsidered, it truly was a thorough review and I look forward toparticipating again in the future.’
Sarah ParsonsMedical Workforce Manager, NHS Employers
Getting it right To ensure that we are testing theright things, we use the coding inour question bank to map ourexaminations to the UK trainingcurricula and demonstrate whichparts of our examination testthem. From time to time, we alsoneed to adjust the pass mark foran examination, to ensure itremains at the right standard. Wedid this in 2015 for the MRCP(UK)Part 1 examination, raising thepass mark from 521 to 528.
Members were impressed by the work undertaken ...

Commitment tofairness: equality and diversity
Understanding
If any examination is to have realvalue, it must be fair. This is particularlyimportant for our postgraduatemedical examinations, where thestakes for safe patient care andsuccessful medical careers are so high.
Differential attainment – meaning thatsome candidate groups perform lesswell in examinations than other groups– has been recognised in the UK forsome time in a range of disciplines,including medicine, from performance inmedical school through to competitionfor training posts and beyond.1
Mindful of this, we take seriously ourresponsibility to ensure that no aspectof the generation or delivery of any ofour examinations could contribute tothe issue.
Understanding the issuesTo solve a problem, we first need tounderstand it. For several years, wehave been gathering detailed self-
Listening
Training
declared data about candidatecharacteristics such as gender andethnicity, and relating these factors toperformance in our examinations.2
These data are published openly on ourwebsite. We gather similar informationabout our examiners, through ourannual census, and ultimately we wantto monitor all protected characteristicsfor candidates and examiners alike. Inaddition to enabling comparison ofoutcome for different candidate groups,this will allow us to ensure that nobarriers exist to the participation ofexaminers from any specificbackground.
Our approach has allowed us to publishpeer-reviewed research on fairness andequality in examinations. A recentpublication found no evidence ofsystematic ethnic or gender bias in ourclinical skills examination, PACES.3
Our data also informed the GeneralMedical Council’s 2015 report4 on
progression of doctors in training, andwas presented at the British MedicalAssociation (BMA) Symposium onEnsuring Fairness in Clinical Training andAssessment.
We are also committed to promotingunderstanding on an individual level.Although equality and diversity trainingis widely available, some of ourexaminers have indicated difficulty inaccessing it in their workplace, and weare now developing a bespoke onlineprogramme to meet this need.
Listening to stakeholdersTo achieve genuine equality andfairness, we work to establishrelationships with our stakeholders,hear their views, and act to address anyconcerns they hold. We meet regularlywith representatives from the BMAJunior Doctors Committee and theBritish Association of Physicians ofIndian Origin (BAPIO) and have gainedmany insights, particularly into howculture and language can affectlearning styles. We have revised ourwebsite to make it more accessible forinternational medical graduates (IMGs),and appointed representatives of bothIMGs, and candidates from black andminority ethnic backgrounds to our key
6 MRCP(UK) ANNUAL REVIEW 2015
1 Woolf K, Potts HW, McManus IC. Ethnicity and academicperformance in UK trained doctors and medical students: systematicreview and meta-analysis. BMJ 2011;342:d901.
2 Dewhurst NG, McManus C, Mollon J, Dacre JE, Vale AJ. Performancein the MRCP(UK) Examination 2003-4: analysis of pass rates of UKgraduates in relation to self-declared ethnicity and gender.BMC Med 2007;5:8.
4 See the GMC report about factors affecting progression of doctorsthrough training on the GMC website: www.gmc-uk.org/education/25495.asp
3 McManus IC, Elder AT, Dacre J. Investigating possible ethnicity and sexbias in clinical examiners: an analysis of data from the MRCP(UK) PACESand nPACES examinations. BMC Med Educ 2013;13:103. To see ourextensive portfolio of academic publications, including research ondifferential attainment, please visit our website atwww.mrcpuk.org/about-mrcpuk/research
Reviewing
Monitoring
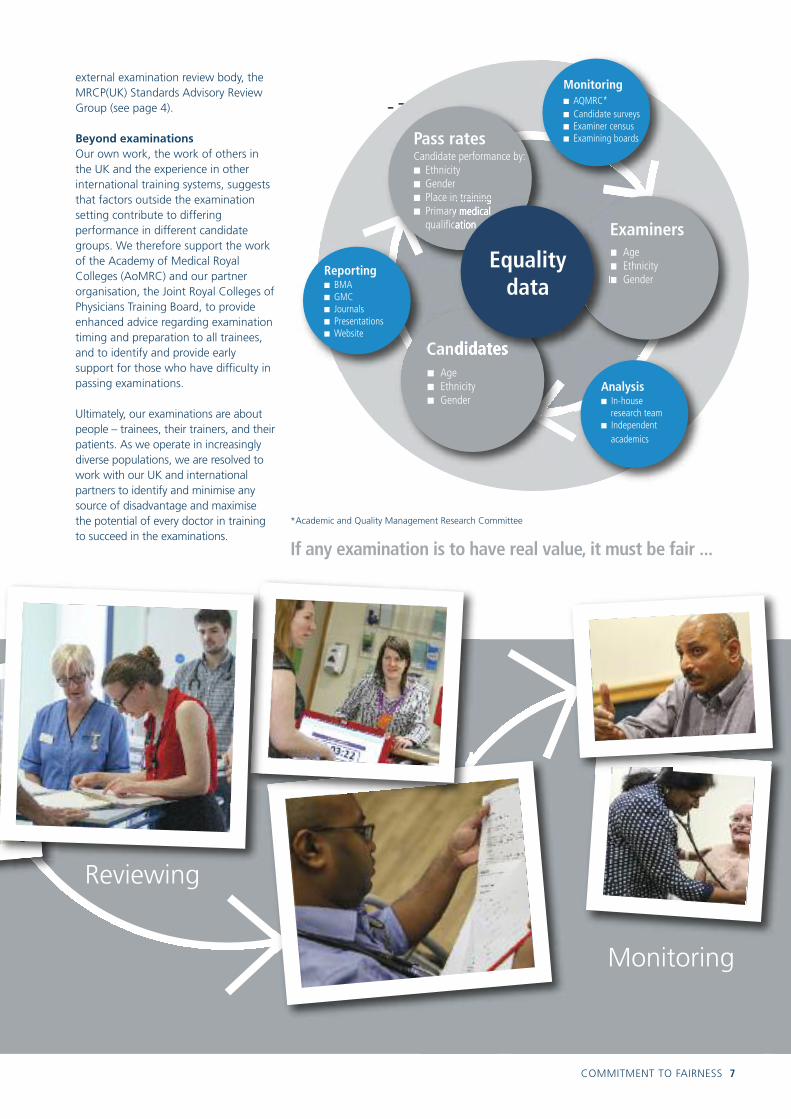
external examination review body, theMRCP(UK) Standards Advisory ReviewGroup (see page 4).
Beyond examinationsOur own work, the work of others inthe UK and the experience in otherinternational training systems, suggeststhat factors outside the examinationsetting contribute to differingperformance in different candidategroups. We therefore support the workof the Academy of Medical RoyalColleges (AoMRC) and our partnerorganisation, the Joint Royal Colleges ofPhysicians Training Board, to provideenhanced advice regarding examinationtiming and preparation to all trainees,and to identify and provide earlysupport for those who have difficulty inpassing examinations.
Ultimately, our examinations are aboutpeople – trainees, their trainers, and theirpatients. As we operate in increasinglydiverse populations, we are resolved towork with our UK and internationalpartners to identify and minimise anysource of disadvantage and maximisethe potential of every doctor in trainingto succeed in the examinations.
If any examination is to have real value, it must be fair ...
COMMITMENT TO FAIRNESS 7
Candidate performance by: n Ethnicityn Gender n Place in trainingn Primary medical
qualification
Pass rates
Examinersn Agen Ethnicityn Gender
n Agen Ethnicityn Gender
Candidates
Equality data
Monitoringn AQMRC*n Candidate surveysn Examiner censusn Examining boards
Analysisn In-house
research teamn Independent
academics
Reportingn BMAn GMCn Journalsn Presentationsn Website
*Academic and Quality Management Research Committee

Internationalpartnerships:examinations andtraining aroundthe world
We are increasingly delivering ourexaminations outside the UK, andinternational candidates tell us howmuch they value this educationalopportunity, and the qualifications inwhich they take great pride. Oursenior colleagues confirm how muchthe examinations are respected byeducators and employers.
Encouraged by this success, we are nowtaking our international activities to ahigher strategic level, with the aim ofintegrating our examinations within localpostgraduate medical trainingprogrammes. In Europe, we are alsoexploring specialist medical qualificationsthat cross borders. Meanwhile, wecontinue expanding internationalcapacity for the delivery of our written
and clinical skills examinations, and weare harnessing communicationstechnology to stay in touch with ourvalued international partners.
Integrated training partnershipsWe believe that examinations to assessknowledge and clinical skills, along withteaching, supervision, and workplaceevaluation, form an integral part oftraining that prepares competentphysicians for independent practice.
That is why we have teamed up with oursister organisation, the Joint RoyalColleges of Physicians Training Board, to explore comprehensive training andexamination partnerships beyond the UK.
In the past year we met with colleaguesfrom Iceland and Sri Lanka, at an eventhosted at the Royal College of Physiciansof London, to explore the developmentof accreditation programmes in thesecountries. The focus was on core medicaltraining (CMT), and the three Diplomaexaminations (Part 1, Part 2 Written andPACES) would be part of this completepackage.
Similar discussions are underway inother countries, and we look forward toa very exciting year ahead.
European initiativesMany physicians work across borders inEurope, and this year has seen progresstowards common qualifications that cantravel with them.
In a two-year pathfinder project, wehave been providing a specialtyexamination on behalf of the BritishSociety of Gastroenterology (BSG) andthe European Board ofGastroenterology and Hepatology(EBGH). Representatives of the EBGHhave contributed extensively to theexamining board meetings and questionwriting and standard setting groups.
Candidate numbers nearly doubled inthe second year of the pathfinder: 50candidates sat the examination in 2014and this increased to 95 in 2015.
The examination has already beenadopted as a mandatory element ofhigher specialist training in Switzerland,a welcome move that is in line with ourvision of an integrated approach totraining and assessment.
8 MRCP(UK) ANNUAL REVIEW 2015
CollaboratingExpanding
exam attemptsin 2014255more international
PACES places
‘Preparing for PACES is an exciting experience. I havelearned a lot and after passing the exam, I started to helpand teach my junior colleagues. Passing PACES will pavemy way to higher training opportunities.’
Dr Hala Ibrahim AbuElhassan AbdAllaIbn Sina Hospital, Ahfad University for Women, Khartoum, Sudan – achieved full marks in PACES.

‘MRCP(UK) is an internationally respected examination of clinicalknowledge, skills and communication. Increasingly this is linked to arequirement to demonstrate a period of recognised training in internalmedicine. MRCP(UK) is working with regulators to facilitate thisintegration.’
Dr Donald Farquhar, International Associate Medical Director, MRCP(UK)
Virtual conferencesWorking side by side with our PACES hosts provides a valuableopportunity to build relationshipsand a sense of common purpose.However, it is a busy time, andeveryone is focused on deliveringthe examination. In order to learnmore about what our partners need,and discuss practical improvements,we have launched a series ofteleconferences with ourinternational PACES hosts. Thisallows for conversations outside thehustle and bustle of examinationdays, and it is proving to be a usefulnew activity. Teleconferences withour colleagues from Oman, Brunei,Chennai and Hong Kong havealready taken place, and we lookforward to talking with all of ourpartners on a regular basis.
We are increasinglydelivering ourexaminations outsidethe UK ...
INTERNATIONAL PARTNERSHIPS 9
‘MRCP(UK) is a very highly respectedqualification in Oman and othercountries. There is great demand forthe examination all over the world. Itis well respected by employers whenthey recruit doctors for training postsor senior jobs.’
Dr Seif Salem Al-AbriLead PACES Examiner in Oman
44countriesworldwide
Inspiring
Hospital, hosted by Professor Aye AyeChit. This centre will offer 45 places ineach examination cycle.
Partnerships in the Middle East have alsobeen fruitful, with the opening of a newPACES centre at Hamad General Hospitalin Doha, Qatar. The hosts there areDr AA Gehani and Dr Wanis Ibrahim, andtheir dedicated team was assisted on siteby senior staff from the Royal College ofPhysicians of Edinburgh. A pathfinder inOctober 2014 was very successful, theexamination went live in December anda second diet took place in April 2015.
Launching these new centres has beencharacterised by a strong sense ofcamaraderie and shared learning –which is what our internationalpartnerships are all about.
Now that the initial pathfinder hascome to an end, we are talking to ourpartners about next steps.
In addition we are exploring thepossibility of pan-Europeanqualifications in other specialtiesincluding neurology and nephrology.
Expanding capacityAlongside these new initiatives, we arealso expanding our capacity to bring theMRCP(UK) Diploma within reach ofmore doctors, in more countries.
An inspiring example has beenMyanmar, where partnerships areblossoming. In 2013, the first PACESexamination was held in New YangonGeneral Hospital. Interest has beenkeen, and in 2015, an additional PACEScentre opened at Mandalay General

Development
Quality
Training
The quality criteria were inspired byfeedback from trainees, who toldJRCPTB that the pressures of their servicecommitments were crowding out timefor educational activities.The criteriawere developed with input from trainersand trainees, after broad consultation.
The CMT quality criteria cover fourdomains:
n structure of the training programme
n delivery and flexibility
n supervision and support for trainees
n good communication.
Among the detailed recommendations,the criteria call for bleep-free coverarrangements to allow protectedlearning time. This will give traineesmore opportunities to attend outpatientclinics and other learning events,including clinical skills development forPACES. We are very encouraged by thisreminder that hard-working juniordoctors need time in their working livesto learn and progress with their training.
Support and monitoringLocalities are being encouraged to reviewwhat they are providing for trainees, andreflect on ways to enhance the learning
Our examinations are woven intothe fabric of medical training. They assess the desired skills andknowledge, guide doctors in theirstudies, and tell us how wellindividuals – and even entirecohorts – are progressing.
This is why we work with medicaleducators to ensure a close match withthe curricula, and provide data that cansupport training on an individual andlocal level. We also use our influence topromote national policies to benefittraining and patient care.
Data for developmentWe collect a wealth of data oncandidate performance, and analysisfrom our research team gives it context.We share these analyses with variousstakeholders so they can spot trends,see how training in their localitymeasures up, and identify areas wheretrainees may need more input andsupport.
To give one example, as part of ourcommitment to transparency in ourprocesses, and in the spirit of helpingcandidates prepare for theirexaminations, we have recentlypublished data on performance by topicfor each of our Specialty CertificateExaminations. This information may alsobe of interest to deaneries andeducational supervisors as they helptheir trainees prepare for theexamination, and will help informexamining board members inmaintaining the examination standards.We have prepared similar data for theDiploma examinations, and thisinformation has now been provided inour regular examination performanceupdates for the Local Education andTraining Boards in England, and thedeaneries in Wales and Scotland.
Quality standards for trainingWe also work with the Joint RoyalColleges of Physicians Training Board(JRCPTB), which sets and maintainsstandards for training on behalf of thethree colleges in the Federation. One ofJRCPTB’s recent achievements has beenthe introduction of quality criteria forCore Medical Training (CMT). Theseclear standards are designed to improvethe educational experience for trainees,and drive up the quality of the trainingenvironment.
Support fortraining: benefitsfor candidates andtheir trainers
10 MRCP(UK) ANNUAL REVIEW 2015

Supporting
environment and the opportunities onoffer. To this end, JRCPTB produced acomprehensive package of resourcesdesigned to support implementation ofthe quality criteria, which was sent to allheads of school for local discussion anddistribution.
Implementation of the criteria will alsobe monitored through the GeneralMedical Council’s annual trainee survey.
Simply asking the question shouldencourage trainees to find out moreabout what is available locally, and giveextra thought to their experience oftraining and how it could be improved.Publication of the overarching findingswill indicate where there are strengthsto build on, and weaknesses to address.
Ultimately, a supportive environment fortraining will benefit patient safety and
care. In the immediate term, for example,skills learned in a simulation workshopcarry over onto the wards and give juniordoctors more confidence. Looking furtherahead, this initiative is about training theconsultants of the future and ensuringthey have the skills, sensitivity andjudgment to lead their own teamseffectively and with assurance.
SUPPORT FOR TRAINING 11
Quality criteria for CMT – overviewThe diagram here gives an overview of the elements covered within each domain of the CMT quality criteria. The aim is to ensurethat trainees have ongoing support and sufficient exposure to learning opportunities that will allow them to become well-rounded,confident and proficient consultant physicians. For more details, please visit www.jrcptb.org.uk
Structure of theprogramme
Delivery and flexibilityof the programme
Supervision and otherongoing support
Communicationwith trainees
A B C D
Core criteria:n Information about rotationsn Advance notice of rotas
Core criteria: n Time on the acute take
Best practice:n Additional placements
2 year programme
Core criteria:n Ward rounds and handoversn Outpatient clinicsn Protected learning timen Procedural skills trainingn Examinations teaching time
Best practice: n On-call in blocksn Acting up arrangementsn Regional teaching programmes
Core criteria:n Committee representationn Information about assessmentn Named College tutor in
all Trusts/Health boardsn Pre-ARCP reviewsn MRCP(UK) support
Best practice:n Regional inductionn UK orientation programmen Local survey/placement evaluation

Medical training in the UK is due forsignificant changes in the next fewyears, and we are actively involvedin shaping and implementing thistransformation. Meanwhile, ourinternational work is opening newdoors around the world, andmaintaining our high academicstandards is becoming anincreasingly complex task.
To stay ahead of these challenges, wehave restructured and strengthened ourclinical leadership roles. This includesthe creation of a new post, AssociateMedical Director (AMD) for Quality. The physician in this role will build onthe capabilities of our in-house researchand policy teams, and ensure thatacademic quality remains embedded inall our work.
With the new appointments, the teamis structured as above.
Three highly valued medical leadersdemitted from their posts this year:*
n Dr Lawrence McAlpine, InternationalAMD
n Dr John Mucklow, AMD for WrittenExaminations (see right)
n Professor Trudie Roberts, AMD forAcademic Quality.
We would like to thank them all fortheir years of outstanding service.
Our people: clinical leadership, appointments and thank you
Medical Director,MRCP(UK)Dr Andrew Elder
Associate MedicalDirector for WrittenExaminationsDr Derek Waller
InternationalAssociate MedicalDirectorDr Donald Farquhar
Associate MedicalDirector for QualityProfessor Phil Smith
Associate MedicalDirector for ClinicalExaminationsDr Kenneth Dagg
12 MRCP(UK) ANNUAL REVIEW 2015
Outstanding contributionsIn recognition of his contributionto the MRCP(UK) examinationsover the years Dr John Mucklow isdue to receive the President’sMedal from the Royal College ofPhysicians of London. It is a rarehonour, and the Medal will bepresented at the HarveianOration on 15 October 2015.
*You can read profiles of our demitting AMDs on the website, and biographies of our new AMDs are in progress for publication on the same page. Please visit: www.mrcpuk.org/about-us/publications/newsletters
Professor Jane Dacre, President of theRoyal College of Physicians of London,who worked alongside Dr Mucklow onthe examinations said, ‘Dr Mucklow hasprovided an extraordinary contributionto UK medicine, in particular via hissupport for the MRCP(UK) examinations.His strategic thinking has shaped severalinnovations to the examinations overmany years. He has been a wonderfulcolleague, and loyal friend to the RoyalCollege of Physicians of London.’

Appointments and thank you
Thanks are due to our demittingofficers and board members, for theirhard work and contributions. A warmwelcome is also extended to our newboard members.
MRCP(UK) Part 1 Examining Board
Thank youDr Ray Fox (Chair)Dr Nigel Reynolds (Medical Secretary)Dr Tom BrownProfessor Sue CarrDr Ken LimDr John Murphy
WelcomeProfessor Albert Ferro (Chair)Dr Karen Adamson (Medical Secretary)Dr Richard D’SouzaDr Nicholas HeaneyDr Ramasharan LaxminarayanDr Malcolm Locke
MRCP(UK) Part 2 WrittenExamining Board
Thank youDr Derek Waller (Chair)Professor Anthony Nicholls (Medical Secretary)Dr Charles HindDr Adrian StanleyDr Catherine Stirling
WelcomeDr Rob Wright (Chair)Professor Rudy Bilous (Medical Secretary)Dr Peter AndrewsDr Ian BealesDr Paul LambertDr Fraz MirDr Ananthakrishnan RaghuramDr Catherine Sargent
Scenario Editorial Committee (PACES)
Thank youDr Jon GoldmanDr Derek GordonDr Andrew InnesDr Michael RudolfDr Udi Shmueli
WelcomeDr Parijat DeDr Arthur DunkDr Sara FairbairnDr Michael Flower (trainee representative)Dr Ellon McGregorDr Laura-Jane Smith (trainee representative)
Academic, Quality Management andResearch Committee
Thank youDr Iain Drummond (trainee representative)
WelcomeDr Daniel Furmedge (trainee representative)Dr Chris Wilkinson (trainee representative)
Acute Medicine SCE Examining Board
Thank youDr Deepak Bhatia (Chair)Dr Philip Dyer
WelcomeDr Nick Scriven (Chair)Dr Nicola Cooper (Medical Secretary)Dr Suresh ChandranDr Mark Cranston
Acute Medicine SCE Standard SettingGroup
WelcomeDr Ruth McEwan
Dermatology SCE Standard SettingGroup
Thank youDr Richard Meyrick-Thomas
Endocrinology & Diabetes SCE Examining Board
Thank youProfessor Jayne FranklynDr Dinesh Nagi
WelcomeDr John Miell
Gastroenterology SCE Examining Board
Thank youDr Elizabeth AlsteadDr Geoff Sandle
WelcomeDr Safa Al-ShammaDr Ian Beales
Gastroenterology SCE Standard Setting Group
Thank youDr Simon Campbell
Geriatric Medicine SCE ExaminingBoard
Thank youDr Julia Newton
Infectious Diseases SCE ExaminingBoard
Thank youDr Nick BeechingDr Mark Melzer
WelcomeDr Brian AngusDr Elinor MooreDr Catherine Sargent
Infectious Diseases SCE Standard Setting Group
WelcomeDr Sani AliyuDr Julia Greig
Medical Oncology SCE Standard Setting Group
WelcomeDr Cathryn Brock
Nephrology SCE Examining Board
Thank youDr Ellon McGregorDr David ReaichDr Chris Winearls
WelcomeDr Richard D’SouzaDr Stephen KardaszDr Edward Kingdon
Nephrology SCE Standard SettingGroup
Thank youProfessor Neil Sheerin
WelcomeDr Catherine Stirling
Palliative Medicine SCE StandardSetting Group
Thank youDr Fiona Hicks
Respiratory Medicine SCE ExaminingBoard
Thank youDr William Kinnear
Respiratory Medicine SCE StandardSetting Group
Thank youDr Ian Coutts
Rheumatology SCE Examining Board
Thank youDr Tom LawsonDr Sophia Steer
WelcomeDr James MartinDr Karen Walker-Bone
Rheumatology SCE Standard Setting Group
Thank youDr Oliver Duke
Copywriting: Colleen Shannon, Freelance medical writerDesign: Chris Hewitt, WLG DesignPhotography: Jonathan Perugia and Christina KernohanProduction: Ruth LorimerPrinted by: Latimer Trend
Published for the Federation of Royal Colleges of Physiciansof the UK by MRCP(UK)
© Royal Colleges of Physicians 2015

MRCPUKMembership of the Royal Colleges of Physicians of the United Kingdom