mp32-20 recovery of erectile function after radical prostatectomy: identification of trajectory...
TRANSCRIPT

Vol. 191, No. 4S, Supplement, Sunday, May 18, 2014 THE JOURNAL OF UROLOGY� e337
Systolic blood pressure decreased from 141.95�13.02 to 123.71�5.45mmHg, diastolic blood pressure from 83.08�10.27 to 78.41�3.89 mmHg(p<0.0001 for all).
CONCLUSIONS: Normalising testosterone in obese hypo-gonadal men resulted in weight loss and improvement of all compo-nents of the metabolic syndrome. These improvements wereprogressive over the full 5 years of the study.
Source of Funding: none
MP32-18TESTOSTERONE REPLACEMENT THERAPY IMPROVES THEQUALITY OF LIFE OF HYPOGONADAL MEN DIAGNOSED WITH“LATE ONSET HYPOGONADISM” e ASSESSED BY VALIDATEDQUESTIONNAIRES
Dany-Jan Yassin*, Braunschweig, Germany; Aksam Yassin,Norderstedt, Germany; Peter Hammerer, Braunschweig, Germany
INTRODUCTION AND OBJECTIVES: Physiologic testosteronemaintains libido, nocturnal tumescence and a good erectile function.Studies have shown that sub-physiologic testosterone levels affect thepsychosomatic and psychomotor domains. We hypothesized thattestosterone causes sustained long-term health related quality oflife (HRQoL).
METHODS: 261 patients (mean age 58 years) diagnosed withlate onset hypogonadism (LOH) were treated with long-acting intra-muscular testosterone undecanoate (TU). Treatment was startedapproximately 3 weeks after the diagnosis and continued at three monthintervals after a “loading dose” interval of six weeks. Patients wereentered into a cumulative registry database once they had receivedtreatment for at least one year and followed for up to five years. In thisanalysis, we followed health quality indicators over time since thebeginning of testosterone replacement therapy (TRT). The outcomesstudied were the International Prostate Symptom Score (IPSS), theInternational Index of Erectile Function-5 (IIEF-5), the Aging Males’Symptoms (AMS) scale, and joint and muscle pain. Concomitantly totaltestosterone levels were measured. Joint and muscle pain was recor-ded in a binary fashion. The rest of the parameters were continuousparameters. Means of the IPSS, IIEF-5, AMS, and testosterone werecalculated in every visit (Tx). The percentage of patients reporting jointand muscle pain was also calculated at every Tx. Barographs wereused to report the percentages of those who answered “yes” to “pres-ence of joint and muscle pain”. Linear plots were used to represent thetrend of the means of the continuous variables over time.
RESULTS: Means of IPSS and AMS decreased with a steepslope within the first 3 months. Means of IIEF-5 and total testosteroneincreased with an equal slope during the same period. All 4 parametersreached a plateau at around 3-6 months. Muscle pain percentagedecreased steeply over the first year and continued to decrease with asmaller coefficient until the last follow-up date.
CONCLUSIONS: This descriptive analysis shows a clearimprovement in the psychomotor, psychosomatic, urinary and sexualdomains. As physiologic total testosterone is reached and maintained,IIEF, IPSS, and AMS plateau at a normal level. In addition, joint andmuscle pain shows a sustained continuous improvement.
Source of Funding: none
MP32-19PENILE DOPPLER ULTRASOUND IN YOUNG MEN WITHERECTILE DYSFUNCTION: A SINGLE-CENTER EXPERIENCE
Blake Wynia*, Shpetim Telegrafi, Joseph Alukal, New York, NY
INTRODUCTION AND OBJECTIVES: One in four men seekingmedical help for new onset erectile dysfunction (ED) is under the age of40; the root cause of ED in these men is often assumed to be psy-chogenic in nature. Among those where an organic cause is suspected,hypogonadism, medical and/or surgical comorbidity, prescription med-ications, or illicit drug use are presumed causes. However, a significant
proportion of young men with ED exist who have demonstrable vascularabnormalities. Penile doppler ultrasound is a valuable tool in diagnosingthese abnormalities. We sought to characterize our experience withyoung men presenting for evaluation of ED, and to quantify the numberof anatomic abnormalities discovered in this population.
METHODS: We performed a retrospective review of 120consecutive men aged 18 to 35 evaluated at a tertiary care center forerectile dysfunction. Baseline clinical parameters including duration ofED, nature of symptoms, use of medical therapy, history of pelvic orperineal trauma, and medical comorbidities were collected. In thosewhom penile Doppler ultrasound was performed, cavernosal and dorsalartery flow parameters were recorded as well as the presence orabsence of venoocclusive dysfunction. As well, abnormality of thedorsal or cavernosal arteries was recorded in addition to quality oferection. All dopplers were performed by a single radiologist afterintracavernosal injection of 0.10 mL standard Trimix (30 mg/ml papav-erine, 2 mg/ml phentolamine, 10 mcg/ml prostaglandin E2).
RESULTS: Mean patient age was 30.5 (range 20 to 35). Peniledoppler was offered to all patients; it was performed on 32 of the 120patients (26.7%). Among those who underwent doppler, 15 were foundto have a significant anatomic abnormality (46.9% of dopplers, 12.5% ofthe cohort as a whole); these included absent or hypoplastic cavernosalarteries on one or both sides. Among patients with these abnormalities,mean quality of erection during the test was 2.2 (scale 0-4); meanerection quality among those without these abnormalities was 3.9(p<0.01). Findings consistent with Peyronie’s disease were found in 3of the studies (9% of dopplers, 2.5% of cohort).
CONCLUSIONS: Among young men with referred to a tertiarycare center for evaluation of erectile dysfunction, a significant proportionwill have anatomic abnormalities in vasculature contributing to their ED.This finding supports increased utilization of penile doppler in youngmen with erectile dysfunction, where a large population of patients withthese abnormalities may currently be undiagnosed.
Source of Funding: none
MP32-20RECOVERY OF ERECTILE FUNCTION AFTER RADICALPROSTATECTOMY: IDENTIFICATION OF TRAJECTORYCLUSTER GROUPS
Catherine J. Harris*, Nashville, TN; Christopher B. Anderson, New York,NY; Mary S. Dietrich, Daniel A. Barocas, Sam S. Chang, Nashville, TN;Michael S. Cookson, Oklahoma City, OK; Joseph A. Smith Jr.,Peter E. Clark, S. Duke Herrell, Melissa R. Kaufman, Nashville, TN
INTRODUCTION AND OBJECTIVES: Post-prostatectomyerectile dysfunction (ED) can impact health related quality of life inmen treated with radical prostatectomy for prostate cancer. Predictingrecovery patterns after prostatectomy can inform counseling pre-operatively and post-operative treatment. Using trajectory clusteringanalysis we identified predictors of post-prostatectomy erectiledysfunction and recovery patterns.
METHODS: In a five-year period health related quality of lifewas evaluated in patients treated with radical prostatectomy usingUCLA-PCI pre-operatively, and 3, 6 and 12 months postoperatively. Weused a novel cluster modeling technique to identify unique group tra-jectories of erectile function recovery with time.
RESULTS: Group based modeling of the UCLA-PCI sexualfunction scores identified 4 distinct post-prostatectomy erectile functionrecovery patterns. The 70 group 1 patients had significant ED atbaseline and attained only 9.4% of optimum erectile function at 12months. The 202 group 2 patients had a baseline UCLA-PCI sexualfunction score of 78.1 (IQR 65.6, 84.4) with 20.3% on treatment for EDand 7.4% impotent. Group 2 patients reached 18.9% of optimumerectile function at 12 months. The 88 group 3 patients had a baselineUCLA-PCI sexual function score of 84.4 (IQR 78.1, 90.6) with maximumloss of function at 3 months and a strong trend toward recovery at 12months. Of these patients, 10.2% required ED treatment pre-operativelyand 2.3% were impotent. The 43 group 4 patients maintained strongsexual function scores from baseline 87.4 (IQR 78.1, 93.8) to 12 months
e338 THE JOURNAL OF UROLOGY� Vol. 191, No. 4S, Supplement, Sunday, May 18, 2014
78.1 (71.9, 84.4). Patients in groups 1 and 2 were older (p¼0.009) andmore likely to have ED requiring treatment (p¼0.028) or to be impotent(p¼0.01) at baseline than those in groups 3 or 4. On multivariateanalysis, patients’ age and pre-operative erectile function significantlypredicted inclusion in groups 1 or 2. Patients’ comorbidities, D’Amicorisk group and degree of nerve sparing were not significant predictors ofpost-operative erectile function recovery.
CONCLUSIONS: A novel modeling approach identified 4distinct post-prostatectomy erectile function recovery patterns. Patientage and pre-operative erectile function were most predictive of recoverypatterns. These findings can assist in pre-operative counseling andpost-prostatectomy interventions, such as identifying those that maybenefit from penile rehabilitation programs.
Source of Funding: None
Urodynamics/Incontinence/Female Urology:Incontinence Therapy I
Moderated Poster
Sunday, May 18, 2014 10:30 AM-12:30 PM
MP33-01RETROSPECTIVE EVALUATION OF EFFICACY AND SAFETY OFARGUS SLING FOR TREATMENT OF MALE STRESS URINARYINCONTINENCE: THE CANADIAN EXPERIENCE
Genevieve Nadeau*, Quebec, Canada; Michael-Wadih Sourial,Sherbrooke, Canada; Michel Bureau, Quebec, Canada; Le-Mai Tu,Sherbrooke, Canada; Greg Bailly, Halifax, Canada; Stephen S. Steele,Kingston, Canada; Kevin Carlson, Richard Baverstock, Calgary,Canada; Neil Dwyer, Moncton, Canada; Luc Valiquette, Montreal,Canada; Jean-Guy V�ezina, Quebec, Canada; Sender Herschorn,Toronto, Canada
INTRODUCTION AND OBJECTIVES: The Argus trans-obturator bulbourethral silicone male sling for stress urinary inconti-nence (SUI) can be performed after radiation and is adjustablepostoperatively through superficial skin incisions if required. To date,only a few reports from South America and Europe have described itsperformance. We aim to report the efficacy and safety in a series ofCanadian patients following implantation.
METHODS: The records of 96 patients treated at 8 Canadianinstitutions since 2010 were reviewed. Continence status and compli-cations were recorded.
RESULTS: Of the 96 patients 25 had mild (1-2 pads), 57 hadmoderate (3-5 pads) and 14 had severe (> 5 pads) incontinence. Ninetypatients had undergone radical prostatectomy, four had had TURP andtwo had a neurogenic bladder. The sling tension was set to a meanintra-operative retrograde urethral pressure of 36 cm H2O. With a meanfollow-up of 13.1 months (range 1.5-37.9), improvement in continencestatus was noted in 90%, with 54% being completely dry. There was asignificant reduction in daily pad use from 3.8 to 1.1 (p<0.0001).Twenty-three (24%) men had had previous radiation and their outcomeswere similar to those who did not. Adjustment was necessary in17 (18%) cases - loosening (1/96) or tightening (16/96) at an average of192 days.
No device erosion was seen. The overall complication rate was64%, the most common of which was early postoperative perinealdiscomfort, in 38%. This resolved in most but 7 patients had persistentpain. Other complications included 3 intraoperative urethral/bladderperforations, 8 de novo OAB symptoms, 4 UTIs, 3 wound infections, 2de novo erectile dysfunction, 21 patients with transient urinary retentionand 2 with chronic retention. Eleven patients required Argus removalbecause of persistent or recurrent incontinence (4), sling breakage (3),sling infection (2), chronic retention (1), or chronic scrotal pain (1).
CONCLUSIONS: In this first North American series, the Argussling was found to be highly effective to treat male SUI, even after ra-diation therapy. Although mostly minor and self-limited, a non-negligiblecomplication rate was seen, which raises concerns especially aboutpostoperative perineal pain. Further studies are required and we plan tocontinue to report outcomes after extended follow-up.
Source of Funding: None
MP33-02PROSPECTIVE MULTICENTER DOUBLE-BLIND PLACEBO-CONTROLLED TRIAL OF THE EFFICACY AND SAFETY OFLIPOSOMAL BOTULINUM TOXIN-A INSTILLATION VS.PLACEBO IN TREATMENT OF PATIENTS WITH REFRACTORYOVERACTIVE BLADDER
Yao-Chi Chuang*, Kaohsiung, Taiwan; Jonathan Kaufmann,David Chancellor, Pittsburgh, PA; Michael Chancellor, Royal Oak, MI;Hann-Chorng Kuo, Hualien, Taiwan
INTRODUCTION AND OBJECTIVES: Intradetrusor injection ofbotulinum toxin has been shown to be effective for the treatment ofrefractory overactive bladder (OAB), however, the treatment requires acystoscopic procedure with 20-30 needle injections and risk of urinaryretention. We studied the safety and efficacy of a single instillation ofliposomal OnabotulinumtoxinA (LP-09) 200 U solution.
METHODS: A two-center, double-blind, prospective, random-ized, placebo-controlled, study enrolled male and female patients withidiopathic OAB who were inadequately managed by antimuscarinics.Subjects were randomized to either LP-09 or saline administered as50 ml solution. The primary end point was mean change from baselinein the number of micturitions per day at 4 weeks post treatment. Addi-tional end points included mean change of urgency and incontinenceepisodes, OAB symptom score (OABSS), and urgency severity score(USS). Safety assessments included adverse events and post voidresidual (PVR) urine volume.
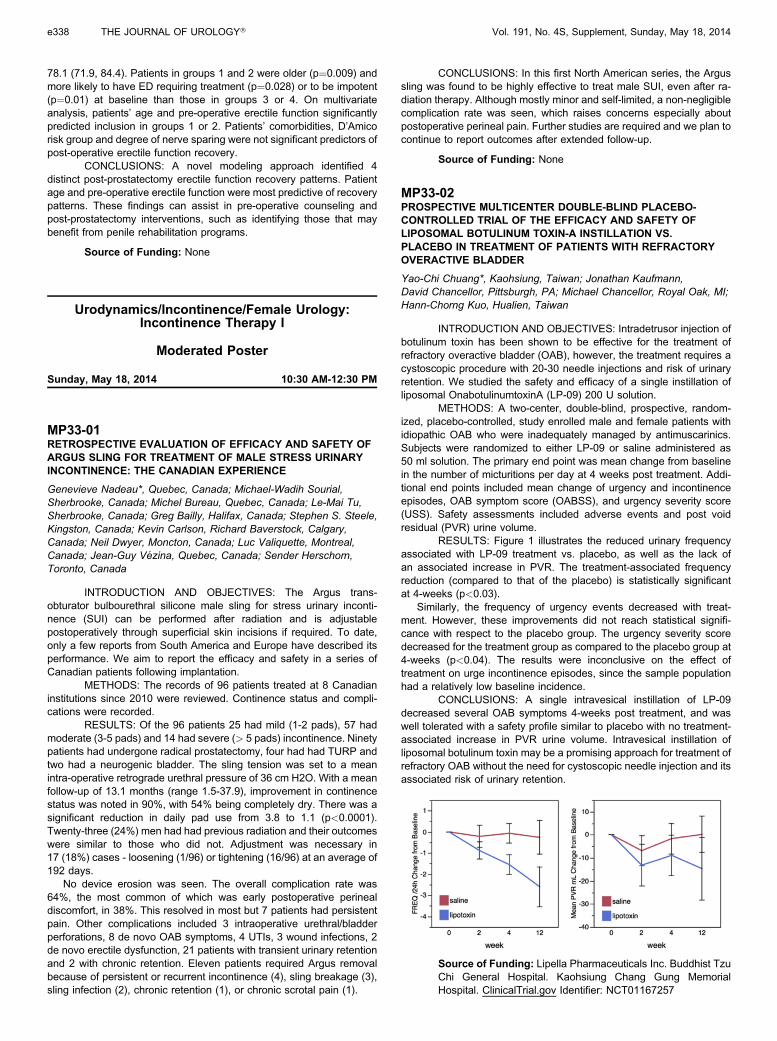
RESULTS: Figure 1 illustrates the reduced urinary frequencyassociated with LP-09 treatment vs. placebo, as well as the lack ofan associated increase in PVR. The treatment-associated frequencyreduction (compared to that of the placebo) is statistically significantat 4-weeks (p<0.03).
Similarly, the frequency of urgency events decreased with treat-ment. However, these improvements did not reach statistical signifi-cance with respect to the placebo group. The urgency severity scoredecreased for the treatment group as compared to the placebo group at4-weeks (p<0.04). The results were inconclusive on the effect oftreatment on urge incontinence episodes, since the sample populationhad a relatively low baseline incidence.
CONCLUSIONS: A single intravesical instillation of LP-09decreased several OAB symptoms 4-weeks post treatment, and waswell tolerated with a safety profile similar to placebo with no treatment-associated increase in PVR urine volume. Intravesical instillation ofliposomal botulinum toxin may be a promising approach for treatment ofrefractory OAB without the need for cystoscopic needle injection and itsassociated risk of urinary retention.
Source of Funding: Lipella Pharmaceuticals Inc. Buddhist TzuChi General Hospital. Kaohsiung Chang Gung MemorialHospital. ClinicalTrial.gov Identifier: NCT01167257