morehouse pediatrics em lecture series november 23,2009 taryn r taylor, md
TRANSCRIPT
Morehouse Pediatrics EM Lecture SeriesNovember 23,2009Taryn R Taylor, MD

Epidemiology Tooth Eruption & Shedding Schedule Clinical Evaluation Dental Concussion & Subluxation Avulsion Injuries Tooth Displacement Tooth Fractures Dental Abscesses
Epidemiology◦ 30% of children experience dental injuries◦ Peak period of trauma to primary teeth is 18 to 40
months of age◦ Trauma to permanent teeth
School aged boys suffer trauma twice as frequently as girls
Upper (maxillary) central incisors are most frequently injured

Tooth Eruption & Shedding Schedule

Clinical Evaluation◦ Medical History
Assess need for SBE prophylaxis Determine if child has a bleeding disorder or is
immunocompromised Record current medications and medication allergies Obtain history of previous surgeries Determine if tetanus immunization is up to date Determine if child lost consciousness due to injury
◦ Dental History How the injury occurred: provides info regarding severity When injury occurred: prognosis for injured tooth worsens with
every minute of delay in treatment Where injury occurred: helps determine whether tetanus
prophylaxis is warranted

Clinical Evaluation◦ Physical Examination
General assessment includes review of vital signs, evaluation of potential head and cervical spine injury as well as ocular damage
Extra oral evaluation Palpate mandibular condyles, maxilla, zygoma & TMJ
Anterior open bite, malocclusion or limited mandibular opening suggests condylar fractures or dislocation
Note extra oral lacerations, bruises or swelling Lacerations must be inspected for foreign bodies i.e.
gravel or tooth fragments & be debrided if foreign body present

Physical Exam cont.◦ Intra oral evaluation
Remove all clots and debris Palpate alveolus to detect fractures Have patient clench teeth to detect dental occlusion Examine each tooth for damage or mobility Examine labial mucosa, maxillary frenulum, gingival
tissues and tongue for bruising or lacerations Lacerations must be cleaned & explored for presence of
foreign body Frenulum will heal without long term consequences Most tongue lacerations will heal on their own, unless
tissue edges are not self-approximating

Dental Concussion & Subluxation◦ Concussion: Mild injury to periodontal ligament without
tooth mobility or displacement◦ Subluxation: Significant injury to periodontal ligament
resulting in some tooth mobility◦ These injuries may result in tooth discoloration◦ Initial management
Tylenol as needed for pain Ice as needed for swelling Soft diet Follow up with dentist
◦ Dental office management Radiographs of primary tooth to evaluate for root fracture Splinting of permanent tooth if extremely mobile

Avulsion Injuries◦ Occurs when a tooth is completely displaced from the dental
socket◦ Radiographs may be necessary if tooth cannot be found◦ Primary Teeth
Not reimplanted, as the risk of injury to developing permanent tooth bud is high
◦ Permanent Teeth Best way to preserve an avulsed tooth is to replace it in its socket
as quickly as possible Periodontal ligament is protective layer surrounding the root, which
suffers irreversible damage if allowed to dry Do not touch root of tooth, handle by crown only Rinse only if there is dirt covering it, don’t scrub or scrape tooth Gently dislodge any clots, & reintroduce tooth into the dental socket
slowly

Avulsion Injuries cont.◦ Post Reimplantation care
Dental consult immediately for splinting & tooth stabilization
10 day course of prophylactic penicillin Tetanus vaccination if wound is dirty or vaccination
requires updating Chlorhexidine gluconate rinses, oral hygiene & soft
diet instructions Analgesics for pain control Dental follow up within one week

Tooth Displacement◦ Luxation: Displacement of tooth in any direction,
while remaining in the socket Lateral luxation is usually associated with fracture of
alveolar bone Primary teeth: analgesia, proper dental hygiene,
prompt dentist follow Permanent teeth: gently reposition tooth, additional
care similar to primary teeth

Tooth Displacement◦ Extrusion: tooth is only partially removed from
socket Care similar to other luxation injuries
◦ Intrusion: tooth is impacted into alveolar bone with associated fracture Intrusions of up to 3 mm have excellent prognosis Care similar to other luxation injuries

Tooth Fractures◦ Crown fractures are described by Ellis Classification
Ellis class I: involves enamel only, rarely painful, cosmetic implications only
Ellis class II: involves enamel as well as dentin Sensitivity to cold air & fluids Emergency treatment aimed at protecting the pulp by applying
calcium hydroxide product Dentist follow up in 48 hours
Ellis class III: dental pulp involved, often appears red Exposure of nerve endings causes extreme pain Exposure of pulp will lead to pulpal necrosis from bacterial
infection if left untreated Emergency treatment aimed at protecting the pulp by applying
calcium hydroxide product Dentist follow up within 24 hours

Dental Abscess◦ Results when inflammation of the pulp is left
untreated◦ Pain, tenderness, red, swollen gingiva with areas of
fluctuance◦ Complications include localized cellulitis, fistula
formation◦ Emergency management includes pain control and
oral penicillin◦ Prompt dental follow-up◦ Emergent ENT consultation for patients requiring
incision and drainage due to severe pain or with extension of infection into deeper tissues

Landmarks of the eye Different types of eye injuries Emergency care for eye injuries Orbital Cellulitis
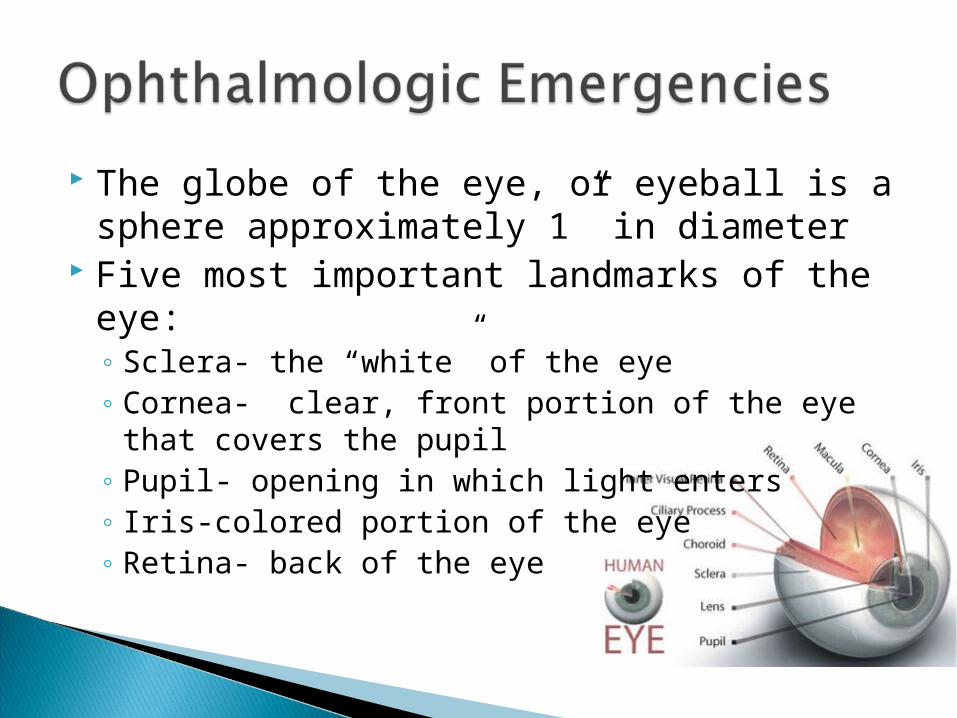
The globe of the eye, or eyeball is a sphere approximately 1” in diameter
Five most important landmarks of the eye:◦ Sclera- the “white” of the eye◦ Cornea- clear, front portion of the eye that covers
the pupil◦ Pupil- opening in which light enters◦ Iris-colored portion of the eye◦ Retina- back of the eye
Ocular trauma is the leading cause of noncongenital unilateral blindness in children younger than 20
Most eye trauma occurs during sports activities
Clinical Assessment◦ Mechanism: blunt or sharp object, foreign body
present◦ Symptoms: pain, photophobia, eye movements,
visual acuity◦ Exam: Pupil size, shape, reaction to light: orbital
rims, floor, extra ocular motion
Eye injuries are usually not life-threatening Time is of the essence in your treatment Six different types of eye injuries:
◦ Foreign object in the eye◦ Corneal Abrasions◦ Lid injury◦ Injury to the globe◦ Injury to the orbits◦ Chemical burn to the eye

Extra ocular Foreign Objects◦ Dust, dirt, sand or fine pieces of metal can be
blown into the eye & lodged on conjunctiva or cornea Signs & Symptoms
Pain, foreign body sensation Excessive tearing Reddening of conjunctiva Decreased visual acuity

Extra ocular Foreign Body◦ Flush eye for at least 20
minutes◦ If object cannot be flushed,
attempt to remove◦ Evaluate for possible corneal
abrasion
To remove object:Pull down lower lid while patient looks up, or evert upper lid while patient looks downRemove object with sterile gauze
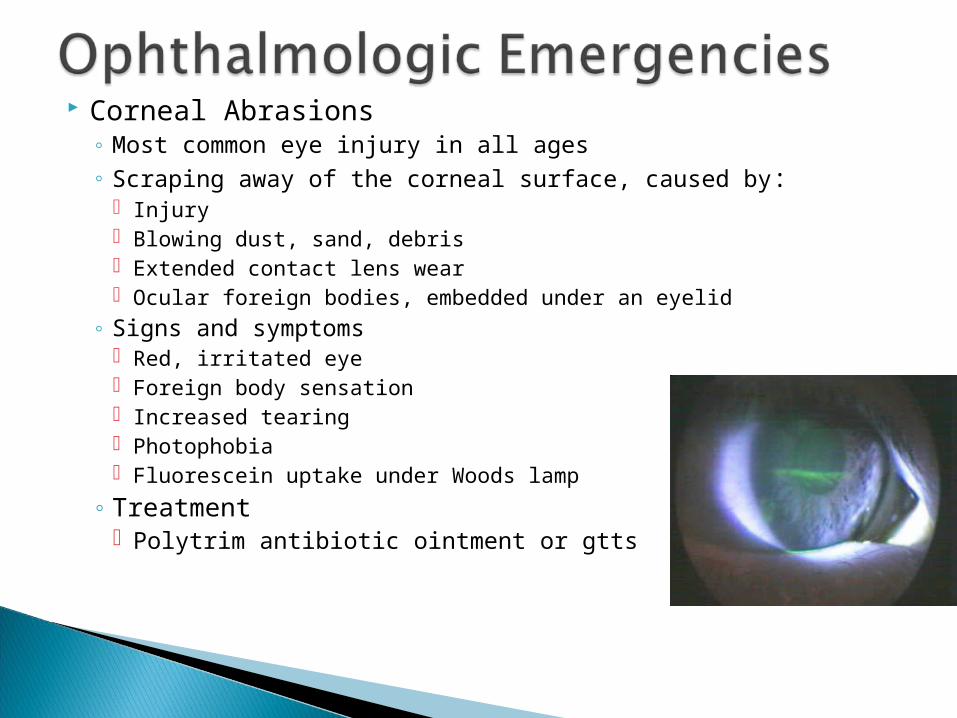
Corneal Abrasions◦ Most common eye injury in all ages◦ Scraping away of the corneal surface, caused by:
Injury Blowing dust, sand, debris Extended contact lens wear Ocular foreign bodies, embedded under an eyelid
◦ Signs and symptoms Red, irritated eye Foreign body sensation Increased tearing Photophobia Fluorescein uptake under Woods lamp
◦ Treatment Polytrim antibiotic ointment or gtts

Eyelid Lacerations◦ Control bleeding with LIGHT pressure◦ Ocular injury should always be suspected◦ Lids should be everted and conjunctival surface
examined◦ Orbital CT if suspected ocular penetration ◦ Laceration repair with 6-0 nonabsorbable suture◦ Optho referral for repair:
Lacerations involving nasolacrimal duct Full thickness lacerations Eyelid margin lacerations
◦ Lacerations from animal or human bites require tetanus prophylaxis

Injuries to Globe◦ Subconjunctival Hemorrhage
Blood between conjunctiva & sclera, stops at cornea Not an emergency Heals like any other bruise
◦ Hyphema Accumulation of blood in the anterior chamber Complications include inflammation and increased IOP
Patients with sickle cell disease or trait & thalassemia are at risk for central retinal artery and optic nerve damage
Patients are at risk for rebleeding 3-5 days after initial injury Initial treatment: bed rest, elevation of head of bed 30 degrees,
optho referral Hyphemas > 50% should be admitted Avoid aspirin & NSAIDS
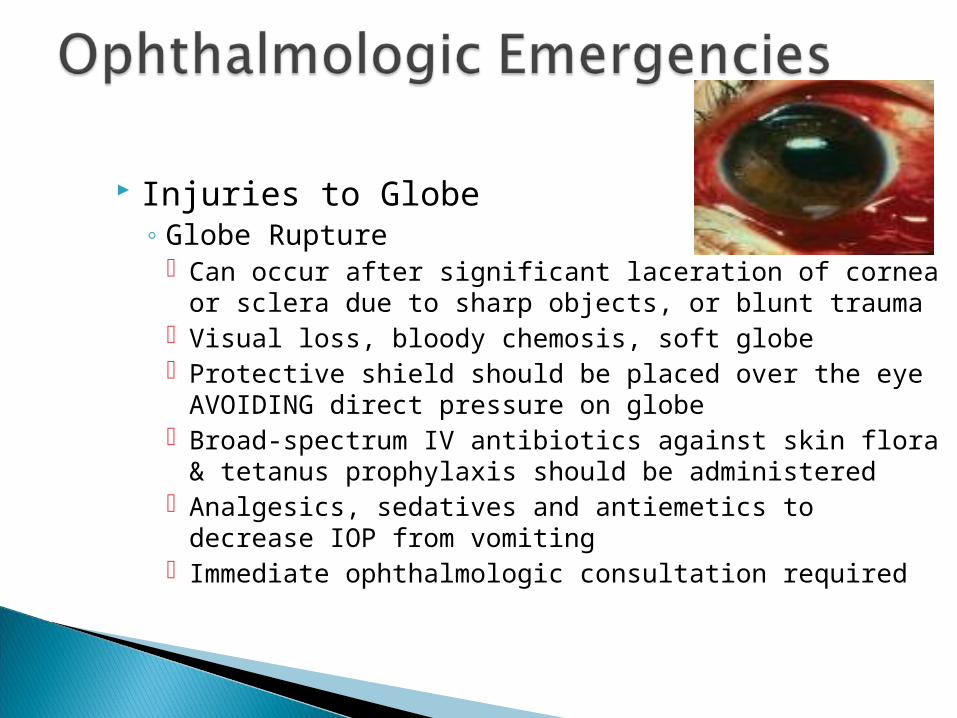
Injuries to Globe◦ Globe Rupture
Can occur after significant laceration of cornea or sclera due to sharp objects, or blunt trauma
Visual loss, bloody chemosis, soft globe Protective shield should be placed over the eye
AVOIDING direct pressure on globe Broad-spectrum IV antibiotics against skin flora &
tetanus prophylaxis should be administered Analgesics, sedatives and antiemetics to decrease
IOP from vomiting Immediate ophthalmologic consultation required

Orbital Fractures◦ “Blowout” Fracture
Following blunt trauma, eye is pushed through floor of orbit, causing fracture of orbital wall
Trapping of intraocular muscle prevents movement of eye away from fracture site
Facial asymmetry, sunken eye, paralysis of upwards gaze, double vision
◦ Orbital roof fractures Occur mostly in children under 5 years Possibility of communication between orbit & intracranial
cavity Pulsating proptosis
◦ CT scan with immediate ophthalmologic consultation

Chemical Burns◦ Represent a DIRE emergency◦ Permanent damage can occur within seconds◦ Burning and tissue damage will continue to occur
as long as substance is left in eye◦ Signs and Symptoms
Irritated, swollen eyelids Redness of the eye Blurred/diminished vision Irritated, burned skin around the eyes

Chemical Burns◦ Emergency Care
Immediately begin irrigation with NS or LR Continuously irrigate for a minimum of 20 minutes Remove contact lenses-may trap chemicals Wash your hands afterward to prevent contamination
to yourself Contact Poison Control Center for further information Referral to ophthalmologist
Orbital Cellulitis◦ An infection of the orbit itself, which occurs
As a complication of sinusitis with extension of the infection to the orbit
Secondary to penetrating trauma As an extension of a nearby facial infection
◦ Signs & Symptoms Erythema, edema, induration and tenderness to peri
orbital tissues Decreased eye movement Proptosis, chemosis, decreased visual acuity and
papilledema

Orbital cellulitis◦ CT scan of orbit ◦ Prompt treatment with IV antibiotics◦ Inpatient admission for frequent monitoring ◦ Ophthalmologic consultation

Questions?