molmed presentation - jefferies conference nyc 2013 … s.p.a. | jefferies global healthcare...
TRANSCRIPT
Company presentationJefferies Global Healthcare Conference
New York, June 6, 2013
Claudio BordignonChairman and CEO

2MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Forward-looking statements
The presentation contains certain forward-looking statements. Although the Company believes its
expectations are based on reasonable assumptions, these forward-looking statements are subject to
numerous risks and uncertainties, including scientific, business, economic and financial factors, which could
cause actual results to differ materially from those anticipated in the forward-looking statements.
The Company assumes no responsibility to update forward-looking statements or adapt them to future
events or developments.
This presentation is not an offer of securities for sale in any country or jurisdiction, including the United
States. Securities may not be sold to the public in the United States, in Australia, in Canada, in Japan, or in
other relevant jurisdictions without complying with local registration requirements and other legal restrictions.
Declaration by the official Corporate Financial Reporting Manager:
The undersigned herewith attests, pursuant to Article 154-bis, paragraph 2 of the Italian Consolidated Law
on Finance (Legislative Decree 58/1998), that the accounting disclosure contained in this presentation
matches documentary evidence, corporate books, and accounting records.
Enrico Cappelli, Chief Financial Officer, official Corporate Financial Reporting Manager

3MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Listed on the Milan Stock Exchange (MLM)
Company Focus: oncology and genetic orphan diseases
112 employees, 2/3 staff scientists
Net financial position: € 16.9 million (March 31, 2013)
Company core competencies:
NGR-hTNF: tumor vascular targeting agent – pivotal Phase III results in 3Q 2013
TK: cell therapy product – expected filing for conditional approval in EU in 2013
CMO activities for third parties: growing revenues
MolMed: at a glance
Recombinant proteins
Cell and gene therapies
4MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
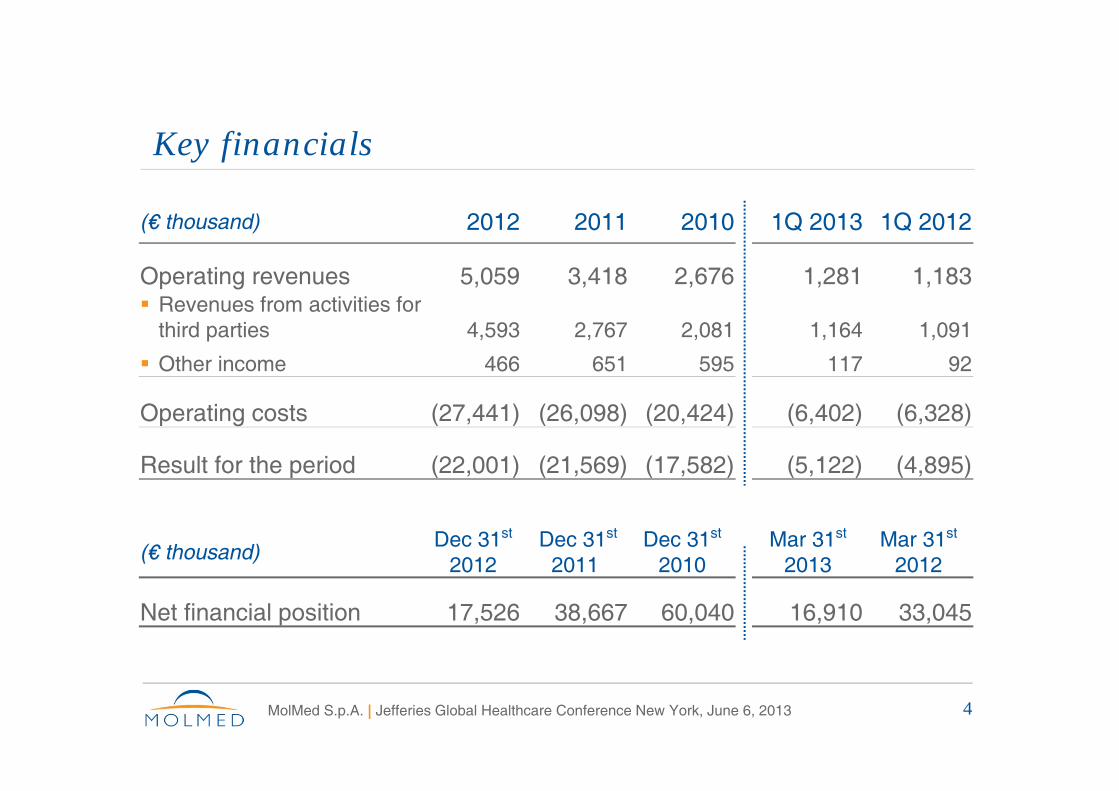
(€ thousand) 2012 2011 2010 1Q 2013 1Q 2012
Operating revenues 5,059 3,418 2,676 1,281 1,183 Revenues from activities for
third parties 4,593 2,767 2,081 1,164 1,091
Other income 466 651 595 117 92
Operating costs (27,441) (26,098) (20,424) (6,402) (6,328)
Result for the period (22,001) (21,569) (17,582) (5,122) (4,895)
Key financials
(€ thousand)Dec 31st
2012 Dec 31st
2011Dec 31st
2010Mar 31st
2013 Mar 31st
2012
Net financial position 17,526 38,667 60,040 16,910 33,045

5MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Shareholders’ structure
Market cap (end of May 2013): ~ €130 million
Daily traded volume (average 3 months): ~ 1,400,000 shares
Shareholders as of 22/04/2013:
Others (<2%)44.15%
Science Park Raf 9.91%
Airain 6.49%
Fininvest 24.90%
H-Equity 4.06%
Delfin 4.06%H-Invest 4.06%
Lombard 2.36%
Free float Strategic investors

6MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed business model:innovation and risk mitigation
Two innovative platforms with different business strategies
Cell and gene therapyRecombinant proteins

7MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed business model:innovation and risk mitigation
Two innovative platforms with different business strategies
Cell and gene therapyRecombinant proteins
Partnering for largerindications
NGR-hTNF
Tumour vascular targeting Potential blockbuster

8MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed business model:innovation and risk mitigation
Two innovative platforms with different business strategies
Cell and gene therapyRecombinant proteins
Partnering for largerindications
Own commercialisation vs partneringopportunities
NGR-hTNF TK
Tumour vascular targeting Potential blockbuster
Patient-specific product for high-risk leukaemia

9MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed business model:innovation and risk mitigation
Two innovative platforms with different business strategies
Cell and gene therapyRecombinant proteins
Partnering for largerindications
Own commercialisation vs partneringopportunities
R&D & production for third parties
NGR-hTNF TK GMP Solutions
Tumour vascular targeting Potential blockbuster
Patient-specific product for high-risk leukaemia
Patient-specific cell & gene therapies

10MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
NGR bindingto tumor blood vessels
hTNF
PeptideNGR
CD13on tumor neo-
vasculature TNF-Receptor
Recombinant fusion protein
Endothelium marker (green) + NGR (red)
NGR-hTNF: a selective vascular targeting agent
Doses of 0.8 µg/sqm systematically show antitumor activity

11MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Selective binding to angiogenic tumour vessels
Human colon carcinoma Normal human colon
Endothelium marker (green) + NGR (red)Endothelium marker (green) + NGR (red)
NGR binds to tumour vessels of CRC and not to those of normal intestine
Whole mount analysis of tissues obtained from the same patient (N=3)
12MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
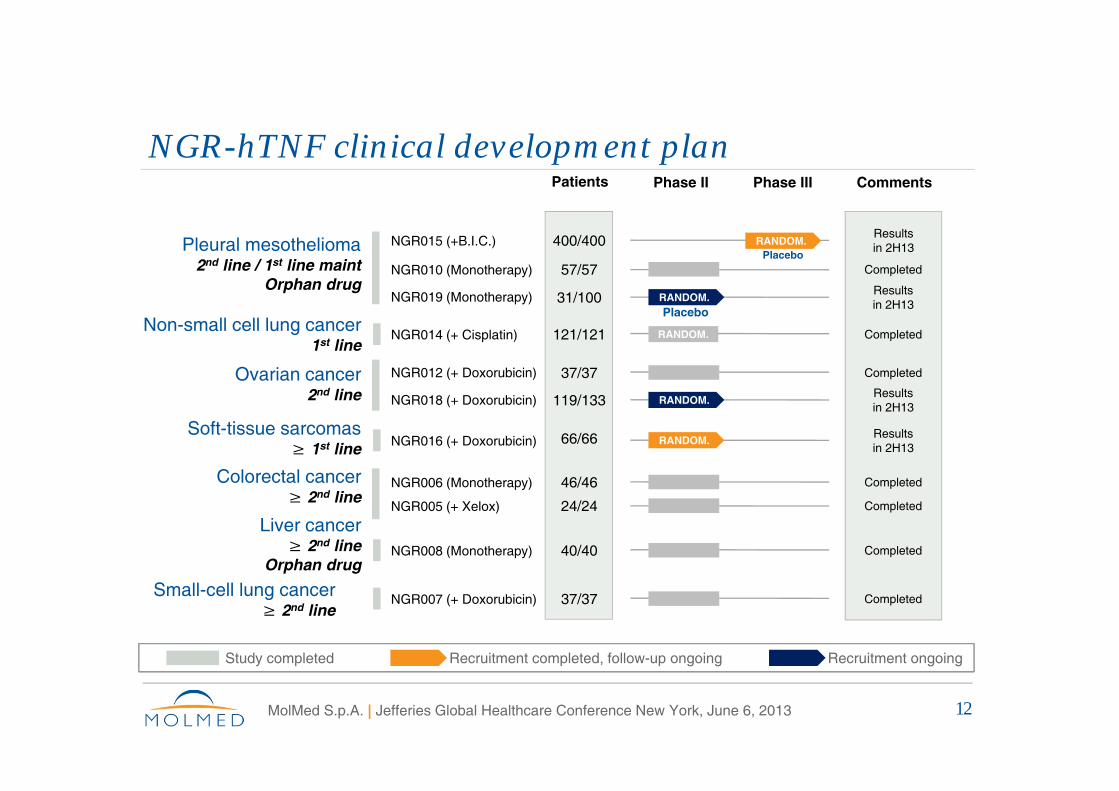
NGR-hTNF clinical development plan
NGR006 (Monotherapy)
NGR005 (+ Xelox)
NGR008 (Monotherapy)
NGR014 (+ Cisplatin)
NGR007 (+ Doxorubicin)
NGR012 (+ Doxorubicin)
NGR018 (+ Doxorubicin)
NGR015 (+B.I.C.)
NGR010 (Monotherapy)
NGR019 (Monotherapy)
NGR016 (+ Doxorubicin)
Phase II Phase III
RANDOM.
RANDOM.
RANDOM.
RANDOM.
Comments
Results in 2H13
Results in 2H13
Completed
Completed
Results in 2H13
Completed
Results in 2H13
Completed
Completed
Completed
Completed
Liver cancer≥ 2nd line
Orphan drug
Colorectal cancer≥ 2nd line
Soft-tissue sarcomas ≥ 1st line
Pleural mesothelioma2nd line / 1st line maint
Orphan drug
Ovarian cancer2nd line
Small-cell lung cancer≥ 2nd line
Non-small cell lung cancer1st line
Patients
400/400
31/100
121/121
37/37
119/133
57/57
66/66
46/46
24/24
40/40
37/37
Placebo
Placebo
Study completed Recruitment completed, follow-up ongoing Recruitment ongoing
RANDOM.

13MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
NSCLC: final data show statistically significant survival improvement in squamous subset1
Decrease in tumour size over treatment
Phase II Randomized + Cisplatin and Gemcitabine 1st line
After a 2.5-year follow-up time, there is a more than 50% relative reduction in the risk of death
Overall survival (n=35)
Time (months)0 6 12 18 24 30 36
2nd 4th 6th (cycle)0
-10
-20
-30
-40
-50
-60
100
80
60
40
20
0
Su
rviv
al p
rob
abili
ty
Med
ian
ch
ang
e fr
om
bas
elin
e (%
)
Note: 1 Predefined per protocol

14MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Soft tissue sarcomas: preliminary data showstatistically significant clinical benefit
Phase II Randomized + Doxorubicin (60mg/sqm) ≥ 2nd line
Low-dose NGR-hTNF plus doxorubicin significantly improve the clinical benefit in sarcoma patients
Progression free survival (n=69) Overall survival (n=69)

15MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Mesothelioma:pivotal Phase III trial as 2nd line therapy (NGR015)
Design: double-blind, placebo-controlled, with a 1:1 randomization ratio
Primary endpoint: survival (N=390; 80% power; 0.05 alpha level; HR=0.72)
Status: enrolment completed (400 pts in EU, US, Canada and Egypt)
Primary efficacy analysis: 3Q 2013
Patients pre-treatedwith pemetrexed-based
regimen (n=390)Randomization 1:1
NGR-hTNF (0.8 µg/sqm q1w) +
Best Investigator’s Choice
Placebo+
Best Investigator’s Choice
N=195
N=195

16MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Mesothelioma: doubled median survival duration versus historical controls
Phase II Single arm Monotherapy ≥ 2nd line
Comparison with Phase III data recently reported in the same setting suggests superior clinical benefit of NGR-hTNF
NGR-hTNFPh II (n=57)
Placebo vs Monochemoth.Ph III (n=660)*
Median PFS (months) 2.8 1.4 vs 1.4
Median OS (months) 12.1 6.2 vs 7.1
*Krug LM et al. EMCC 2011
Comparison with historical controls in 2nd line treatment

17MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Mesothelioma: treatment intensification leads to longer patient benefit
Phase II Single arm Monotherapy ≥ 2nd line
3-year follow-up results strongly confirm the benefit of dose intensification and convincingly support the statistical hypothesis testing of Phase III trial
OS by schedule in patients with disease control

18MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
NGR-hTNF: gearing up for marketing authorization in mesothelioma as first indication
Enrolment completed in pivotal Phase III (400 patients), results expected by 2H 2013, and registration planned as first indication
High unmet medical need and low competition scenario: no drugs registered for second-line treatment or in Phase III development
Orphan Drug designation + patent protection up to 2029
Development of commercial-scale manufacturing ongoing for liquid and lyophilised formulations:
Low COGS: obtained by fermentation in E.coli (one single gene construct)
Strong margin, also in case of price pressure or intense competition
19MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Very low toxicity profile
More than 700 patients treated so far:
No grade 3-4 drug-related toxicity
No cumulative toxicity
No worsening of chemo-associated toxicities
No pulmonary hemorrhage or bleeding events
No treatment discontinuations due to toxicity
Suitable for long-term maintenance treatment

20MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
NGR-hTNF: data from 5 randomised studies (on 800 patients) available over the next 7 months
4Q12 1H13 2H13
MPM Ph III (2nd line) Accrual completion
Primaryresults
MPM Ph II (1st line maint) Accrual completion
NSCLS Ph II (1st line) Accrual completion
Complete results
OC Ph II (2nd line) Accrual completion
24 pts added(weekly dose)
Primaryresults
STS Ph II (1st and 2nd line) Accrual completion
Primaryresults

21MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
NGR-hTNF: well positioned to become a potential blockbuster
Proposed mechanism of action confirmed by clinical observations
Optimal dosing regimen robustly defined
Compelling results presented at ASCO from randomised studies confirm the antitumor activity of NGR-hTNF observed in key indications
Favourable tolerability profile confirmed in more than 700 patients
Easy-to-use predictors of drug efficacy identified
22MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
TK: addressing high unmet need to treat high-risk leukemia
Indication: haematopoietic stem cell transplants (HSCT) for high-risk leukaemia
Unmet need:
~50% of patients candidate to HSCT miss a fully matched donor
Without a transplant, high-risk leukaemia patients have extremely low survival rate
TK technology enables HSCT from partially matched donor without post-transplant immune-suppression

23MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
TK therapy
Technological innovation within HSCT, the oldest & most consolidated celltherapy (>50 years of clinical practice)
Genetic engineering of donor T cells
Day 21+Protection frominfections
Protection fromleukaemia relapse
No immune-suppression needed(prompt abrogation ofGvHD by administrationof ganciclovir)
DonorT cells
TK cellsDay 0
T cells
Haemat.stem cells
TK cells
Donorhaematopoietic
stem cells
HSV-TK
Haplo-identical
donor
Hospital
MolMed GMP facility
24MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
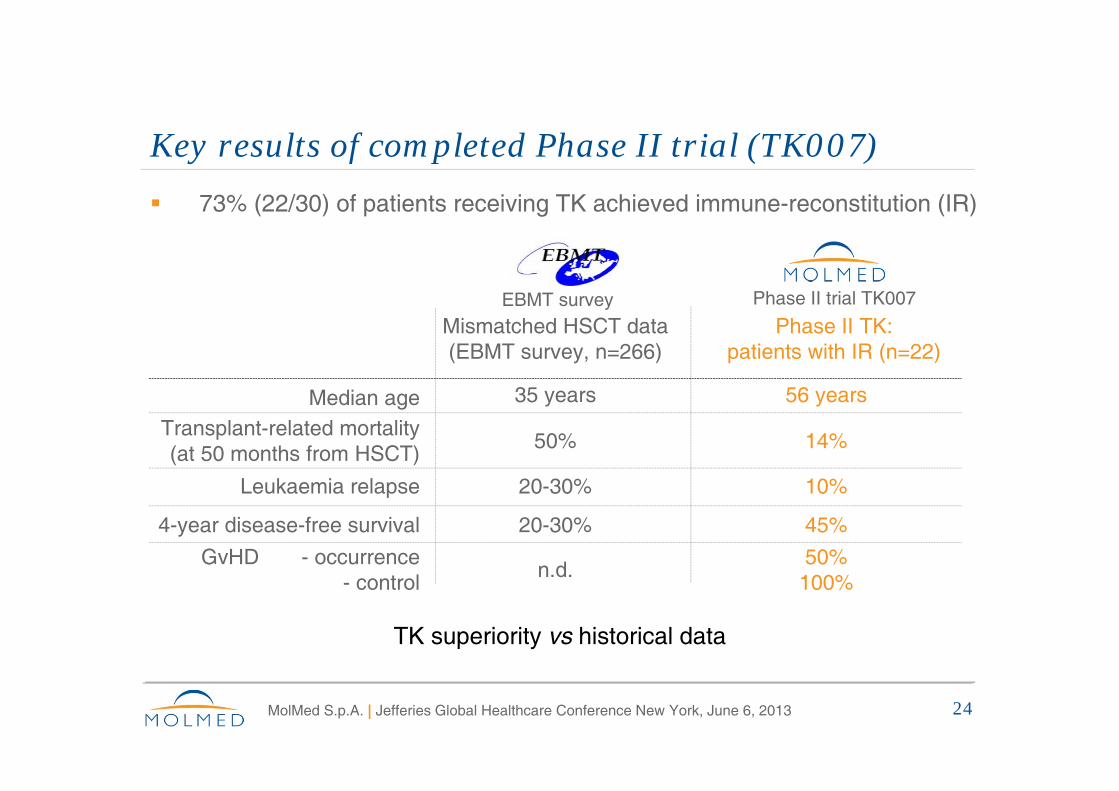
Key results of completed Phase II trial (TK007) 73% (22/30) of patients receiving TK achieved immune-reconstitution (IR)
TK superiority vs historical data
Mismatched HSCT data (EBMT survey, n=266)
Phase II TK:patients with IR (n=22)
Median age 35 years 56 years
Transplant-related mortality(at 50 months from HSCT)
50% 14%
Leukaemia relapse 20-30% 10%
4-year disease-free survival 20-30% 45%
GvHD - occurrence- control
n.d.50%100%
EBMT survey Phase II trial TK007

25MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
The TK technology in haploidenticaltransplants
2 years 5 years 10 years0
20
40
60
80
100O
vera
ll Su
rviv
alHAPLOMRDMUD
p ns
The use of TK has enabled the execution of haploidentical donor transplants, with an overall survival similar to transplants from fully compatible donors

26MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Ongoing pivotal Phase III trial (TK008)
Enrolment planned: 170 patients, randomisation 3:1 in favour of TK
Primary endpoint: disease-free survival
Ongoing in Europe and US
Recent improvements to the TK Phase III trial:
Enlargement of study population to relapsed patients
New treatment option in the control arm to perform an unmanipulated HSCT followed by cyclophosphamide, as GvHD prophylaxis
Modifications already implemented in the majority of clinical centers

27MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
TK: getting ready for the market
Orphan Drug designation + patent protection (with SPC) up to 2030
Phase II long-term data available and pivotal Phase III trial under way
Planned application for Conditional Approval in EU in 2013 based on:
Proof of efficacy
Established long-term safety data
High unmet medical need for patients lacking HLA-matched donor
Automation of cell manufacturing process ongoing
Small dedicated sales force required

28MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed, the pioneer in gene-modified cell therapy
MolMed’s pioneering TK technology: ex vivo genetically-engineered T cells
Telethon’s ADA-SCID (bubble boy) project: developed by MolMed on the same technology platform
12 children suffering from ADA-SCID were treated
8 of 10 first treated patients no longer require enzyme-replacement therapy*
All 10 lead a normal life with significantly improved physical conditions*
ADA-SCID gene therapy was in-licensed by GlaxoSmithKline from Telethon in 2010
Source: *N Engl J Med 2009; 360:447-458
29MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
MolMed, the leader in cell and gene therapy
ADA-SCID success has placed MolMed among the top players in the field of cell and gene therapy
GlaxoSmithKline signed an agreement for the development of the ADA-SCID commercial production process (€ 5.5 million in two years)
Telethon Foundation signed an agreement for the development of six gene therapies for rare genetic diseases (€ 8.3 million in four years)
Opportunity for further industrial partnerships

30MolMed S.p.A. | Jefferies Global Healthcare Conference New York, June 6, 2013
Summary
NGR-hTNF Statistically significant clinical benefit demonstrated in randomised studies Phase III enrolment completed, results expected in 3Q 2013 Manufacturing process on track, IP protection granted
TK Planned application for Conditional Approval to EMA in 2013 Proof of efficacy achieved and long-term safety data established High unmet medical need for patients lacking HLA-matched donor
GMP solutions Successful development of ADA-SCID therapy Important contract signed with big pharma Opportunity for further industrial partnership

Thanks for your attention