molecular targets in bladder cancer: pd-1 and beyond … · imvigor 210 study design cohort 1 to be...
TRANSCRIPT
Molecular Targets in Bladder Cancer: PD-1 and Beyond
Sumanta Kumar Pal, M.D.
Assistant Professor,
Department of Medical Oncology &
Experimental Therapeutics
Co-Director, Kidney Cancer Program
City of Hope Comprehensive Cancer
Center
August 20, 2016

Disclosures
• Consulting: Pfizer, Novartis, Genentech, GSK, Astellas,
Medivation
• Honoraria: Genentech
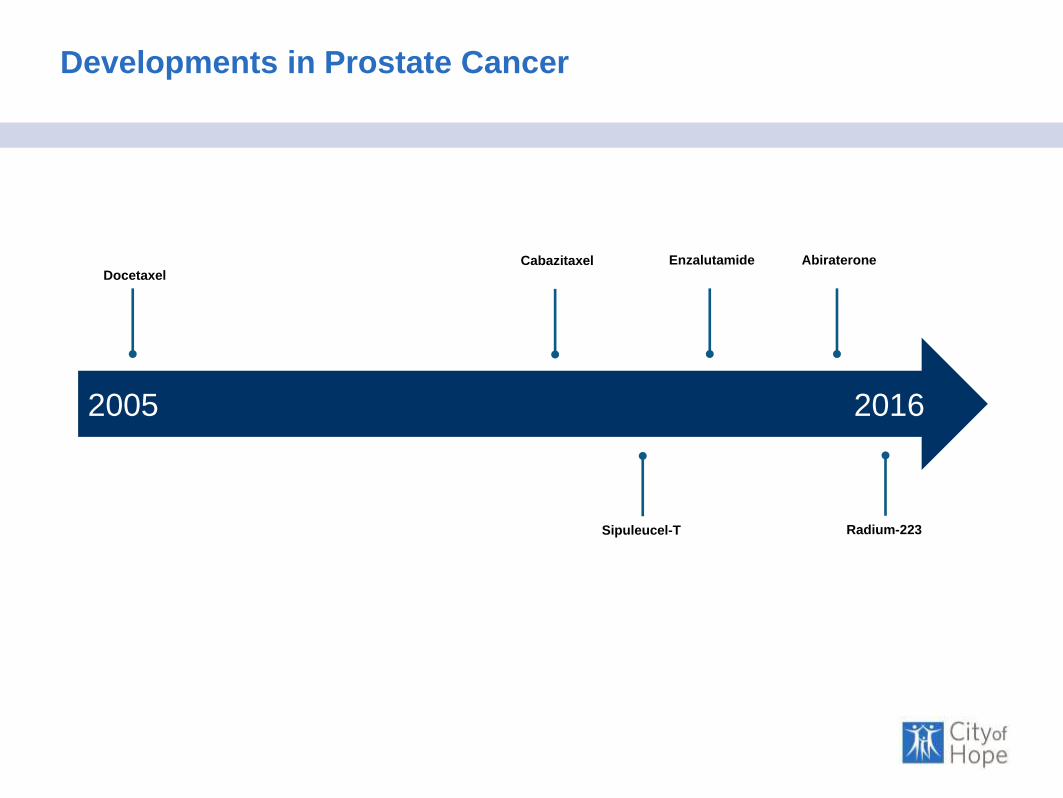
Developments in Prostate Cancer
2005 2016
DocetaxelCabazitaxel Enzalutamide Abiraterone
Sipuleucel-T Radium-223

Developments in Renal Cell Carcinoma
2005 2016
Sorafenib Temsirolimus Bevacizumab Axitinib
Everolimus LenvatinibSunitinib NivolumabPazopanib
Cabozantinib
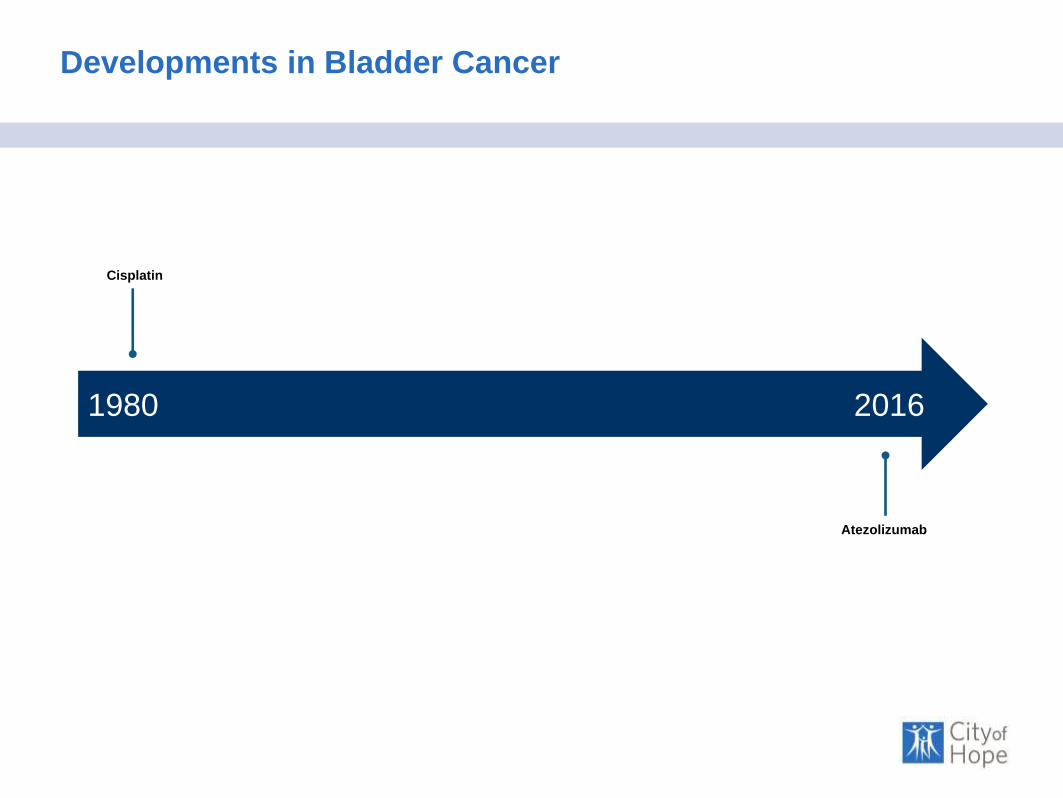
Developments in Bladder Cancer
1980 2016
Cisplatin
Atezolizumab

Overview
Topic
Nature of Treatment
Disease Bladder Cancer
Immune
MOAPD-1-
Directed Therapy
Targeted
MOAFGFR and
HER2 inhibition

Overview
Topic
Nature of Treatment
Disease Bladder Cancer
Immune
MOAPD-1-
Directed Therapy
Targeted
MOAFGFR and
HER2 inhibition
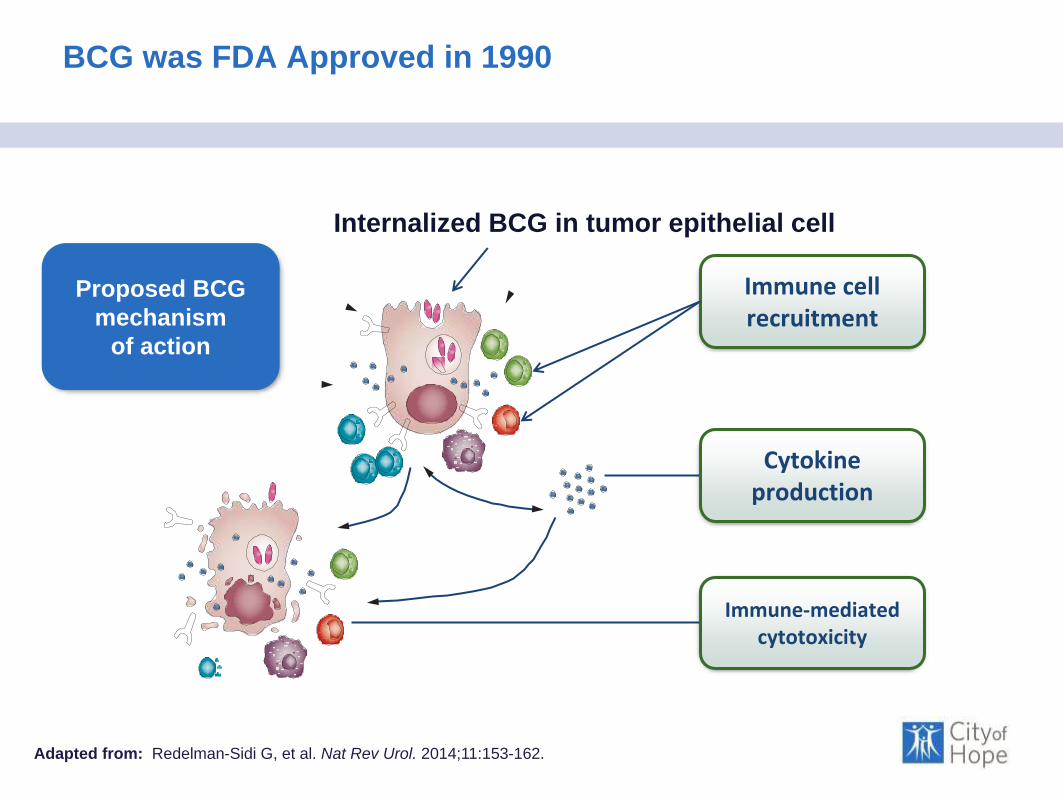
BCG was FDA Approved in 1990
Adapted from: Redelman-Sidi G, et al. Nat Rev Urol. 2014;11:153-162.
Immune cell recruitment
Cytokine production
Immune-mediated cytotoxicity
Internalized BCG in tumor epithelial cell
Proposed BCG
mechanism
of action
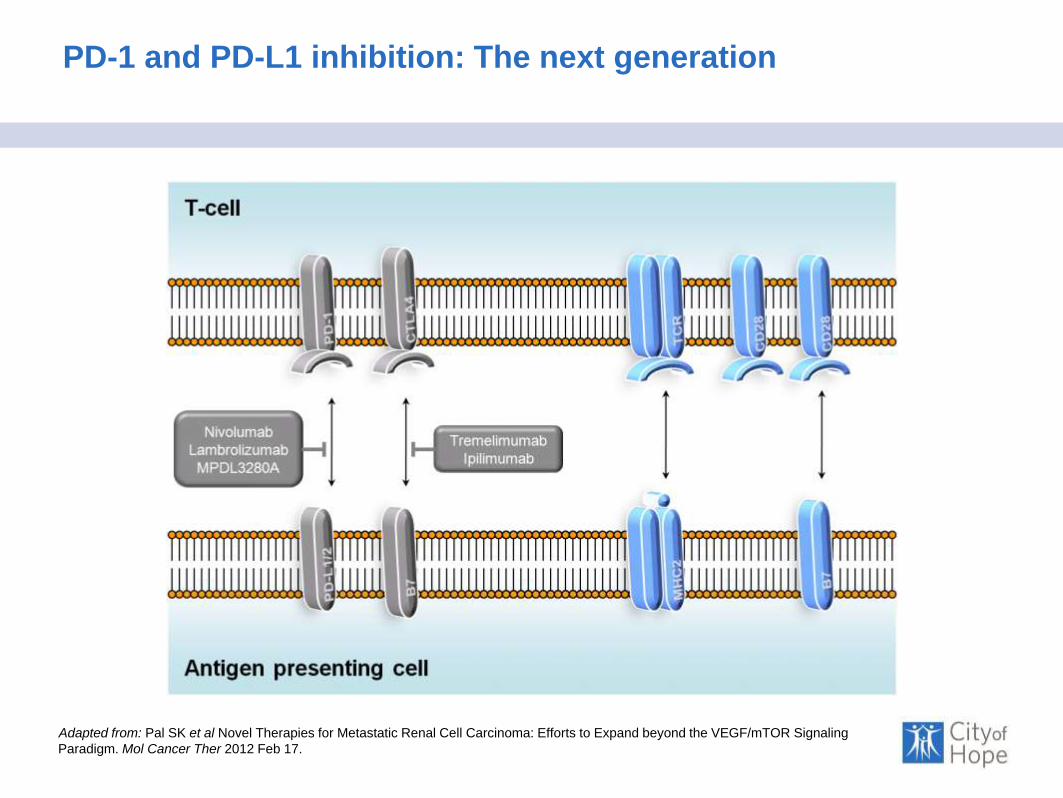
PD-1 and PD-L1 inhibition: The next generation
T-cell
Antigen
Presenting
Cell
Adapted from: Pal SK et al Novel Therapies for Metastatic Renal Cell Carcinoma: Efforts to Expand beyond the VEGF/mTOR Signaling
Paradigm. Mol Cancer Ther 2012 Feb 17.

Genomic diversity in bladder cancer
Lawrence MS et al . Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013 07/11/print;499(7457):214-8.
FDA approved the use of atezolizumab

•Locally advanced or metastatic urothelialcarcinoma.•Predominantly urothelialhistology•Tumor tissue for PD-L1 testing
Cohort 1 (N=119)11 Cisplatin Ineligible
Cohort 2 (N-310)Platinum-treated nUC
Co-primary endpoints:
•ORR (confirmed) per RECIST v1.1 by central review
•ORR per immune-modified RECIST by investigator
Key secondary endpoints
•DOR, PFS, OS, safety
Key exploratory endpoints
•Intratumoral biomarkers
Imvigor 210 Study Design
Cohort 1 to be shown later
Atezolizumab 1200 mg IV q3w until
Loss of Benefit
Cohort 2-Specific Inclusion Criteria
• Progression during/following platinum
(no restrictions on # prior lines of
therapy)
• ECOG PS 0-1
• CrCl ≥ 30 mL/min
Median follow-up: 17.5 months (range, 0.2 to 21.1+ mo)
Dreicer R et al. IMvigor210: Atezolizumab in platinum-treated mUC. ASCO 2016

Atezolizumab Response Rates (by PD-L1 status)
IC2/3n = 100
IC1/2/3n = 207
Alla
N = 310
IC1n = 107
IC0n = 103
ORR: confirmed IRF RECIST v1.1 (95% CI)28%
(19, 38)
19%(14, 25)
16%(12, 20)
11%(6, 19)
9%(4, 16)
CR rate: confirmed IRF RECIST v1.1 (95% CI)15%(9, 24)
9%(6, 14)
7%(4, 10)
4%(1, 9)
2%(0, 7)
• Responses were seen in all IC subgroups, but ORR was enriched with higher
PD-L1 status
• Complete responses accounted for nearly half of the observed responses
– CRs were observed in all PD-L1 subgroups, with the highest rate in IC2/3
patients
a Includes 46 patients with missing/unevaluable responses. b CR + PR + SD ≥ 24-wk rate per IRF RECIST v1.1. Treated patients had measurable disease at baseline per investigator-assessed RECIST v1.1. Data cutoff: Mar. 14, 2016.
Dreicer R et al. IMvigor210: Atezolizumab in platinum-treated mUC. ASCO 2016

Duration of Response to Atezolizumab
• Responses were durable, with mDOR not reached in any PD-L1 subgroup
(range, 2.0+ to 13.7+ mo)
• Ongoing responses were seen in 38 of 45 responding patients (84%)
• Median follow-up time: 11.7 mo (range, 0.2+ to 15.2 mo)
50
0
‒100
0 9 18 27 36 45 54 63
Time on Study, weeks
SLD
Chan
ge
Fro
m B
aselin
e, %
0 9 18 27 36 45 54 63 0 9 18 27 36 45 54 63
IC2/3 IC0IC1
♦ Discontinued
▲ New lesion
Patients with CR or PR per IRF RECIST v1.1
Hoffman-Censits et al. GU ASCO 2016. Abstr 355.
Data cutoff: September 14, 2015.
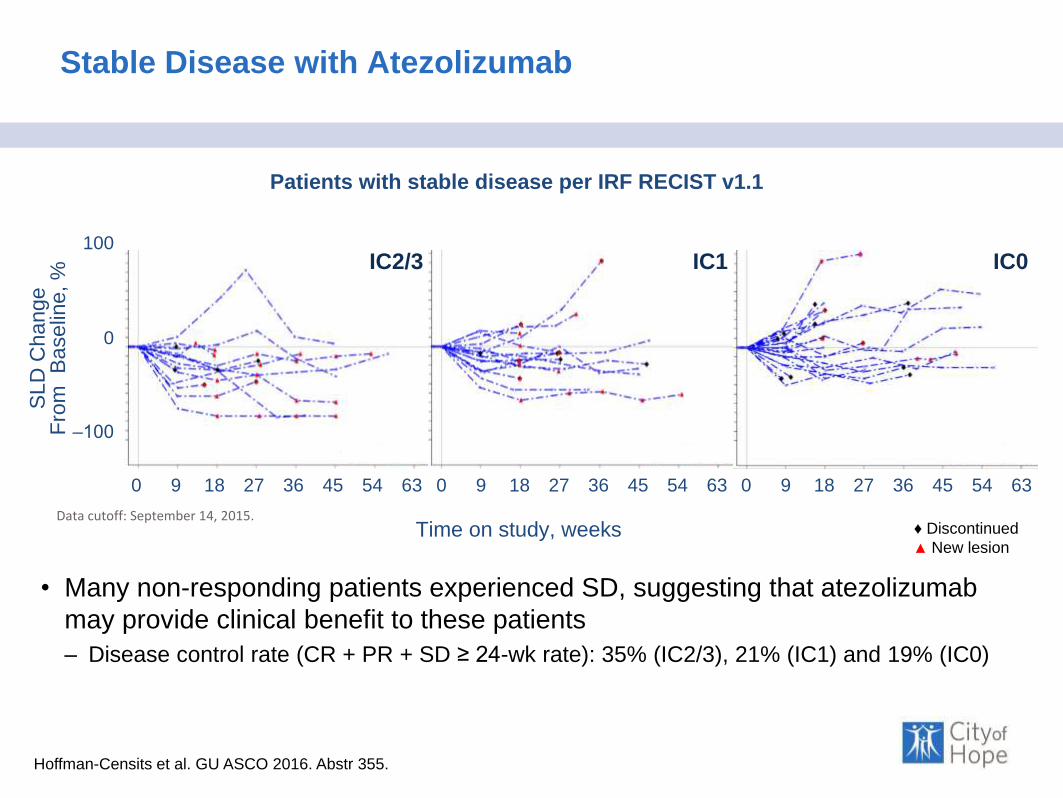
Stable Disease with Atezolizumab
• Many non-responding patients experienced SD, suggesting that atezolizumab
may provide clinical benefit to these patients
– Disease control rate (CR + PR + SD ≥ 24-wk rate): 35% (IC2/3), 21% (IC1) and 19% (IC0)
Hoffman-Censits et al. GU ASCO 2016. Abstr 355.
Data cutoff: September 14, 2015.
100
0
‒100
0 9 18 27 36 45 54 63
Time on study, weeks
0 9 18 27 36 45 54 63 0 9 18 27 36 45 54 63
IC2/3 IC0IC1
Patients with stable disease per IRF RECIST v1.1
♦ Discontinued
▲ New lesion
SL
D C
ha
ng
e
Fro
m
Ba
se
line, %
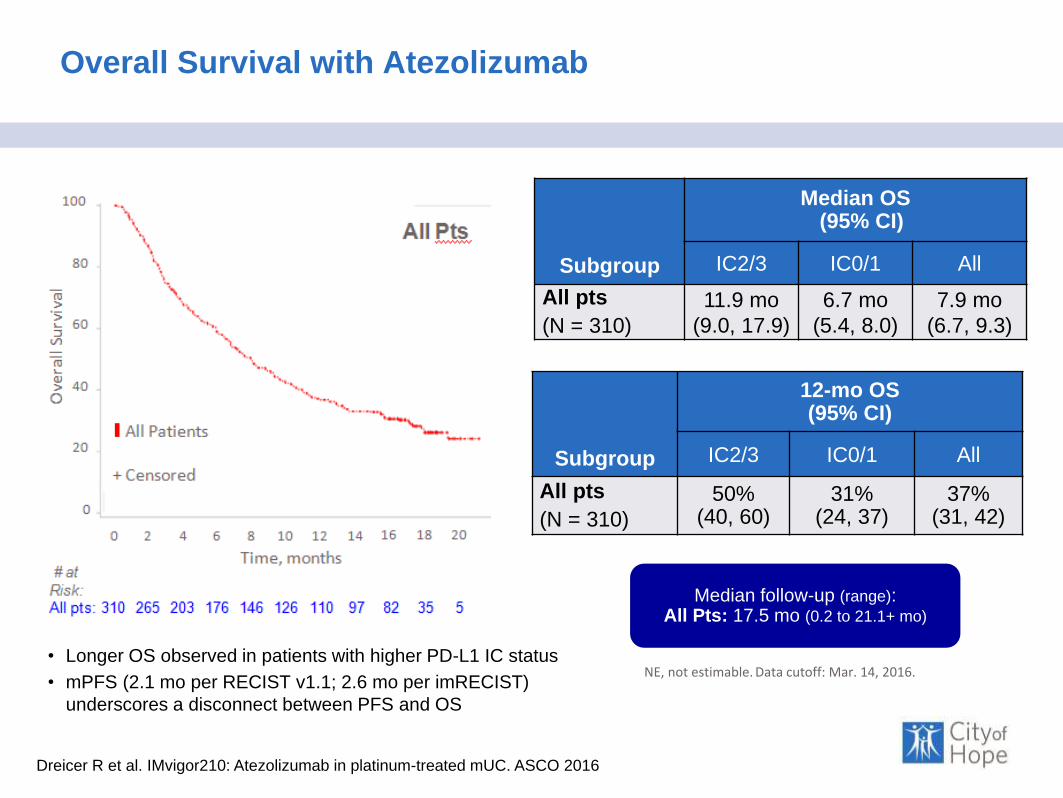
Overall Survival with Atezolizumab
• Longer OS observed in patients with higher PD-L1 IC status
• mPFS (2.1 mo per RECIST v1.1; 2.6 mo per imRECIST)
underscores a disconnect between PFS and OS
Subgroup
Median OS(95% CI)
IC2/3 IC0/1 All
All pts
(N = 310)
11.9 mo
(9.0, 17.9)
6.7 mo
(5.4, 8.0)
7.9 mo
(6.7, 9.3)
Subgroup
12-mo OS(95% CI)
IC2/3 IC0/1 All
All pts
(N = 310)
50% (40, 60)
31% (24, 37)
37% (31, 42)
Median follow-up (range): All Pts: 17.5 mo (0.2 to 21.1+ mo)
Dreicer R et al. IMvigor210: Atezolizumab in platinum-treated mUC. ASCO 2016
NE, not estimable. Data cutoff: Mar. 14, 2016.
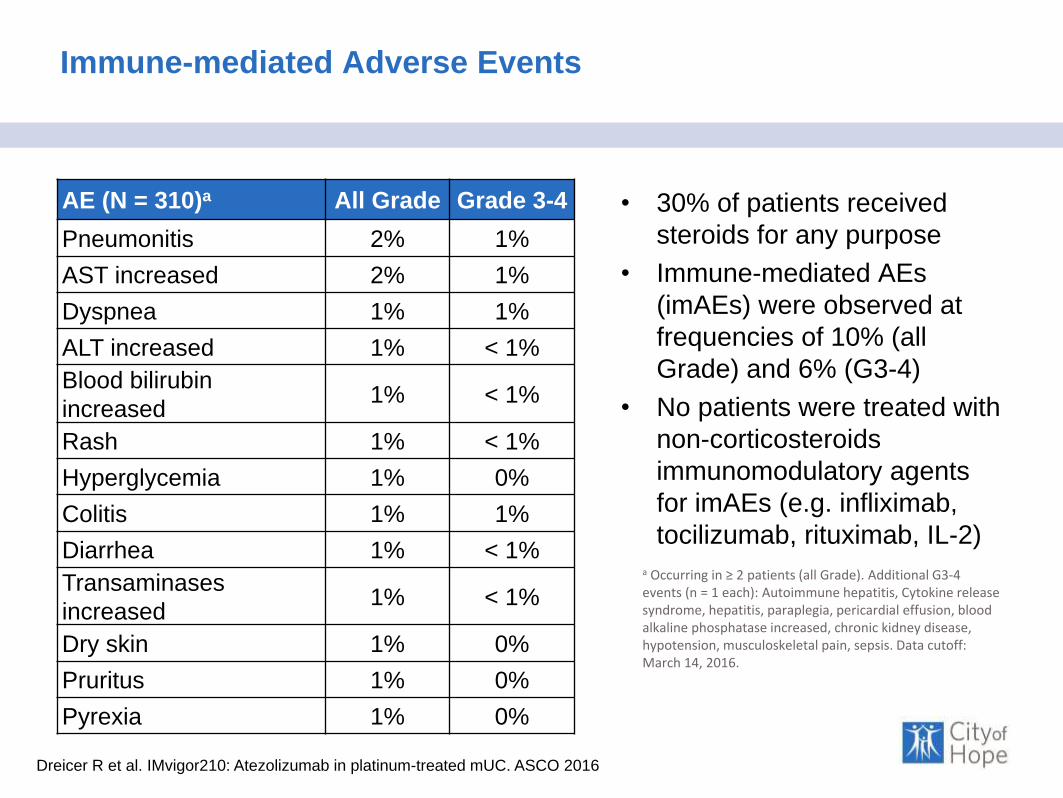
Immune-mediated Adverse Events
AE (N = 310)a All Grade Grade 3-4
Pneumonitis 2% 1%
AST increased 2% 1%
Dyspnea 1% 1%
ALT increased 1% < 1%
Blood bilirubin
increased1% < 1%
Rash 1% < 1%
Hyperglycemia 1% 0%
Colitis 1% 1%
Diarrhea 1% < 1%
Transaminases
increased1% < 1%
Dry skin 1% 0%
Pruritus 1% 0%
Pyrexia 1% 0%
• 30% of patients received
steroids for any purpose
• Immune-mediated AEs
(imAEs) were observed at
frequencies of 10% (all
Grade) and 6% (G3-4)
• No patients were treated with
non-corticosteroids
immunomodulatory agents
for imAEs (e.g. infliximab,
tocilizumab, rituximab, IL-2)
a Occurring in ≥ 2 patients (all Grade). Additional G3-4 events (n = 1 each): Autoimmune hepatitis, Cytokine release syndrome, hepatitis, paraplegia, pericardial effusion, blood alkaline phosphatase increased, chronic kidney disease, hypotension, musculoskeletal pain, sepsis. Data cutoff: March 14, 2016.
Dreicer R et al. IMvigor210: Atezolizumab in platinum-treated mUC. ASCO 2016
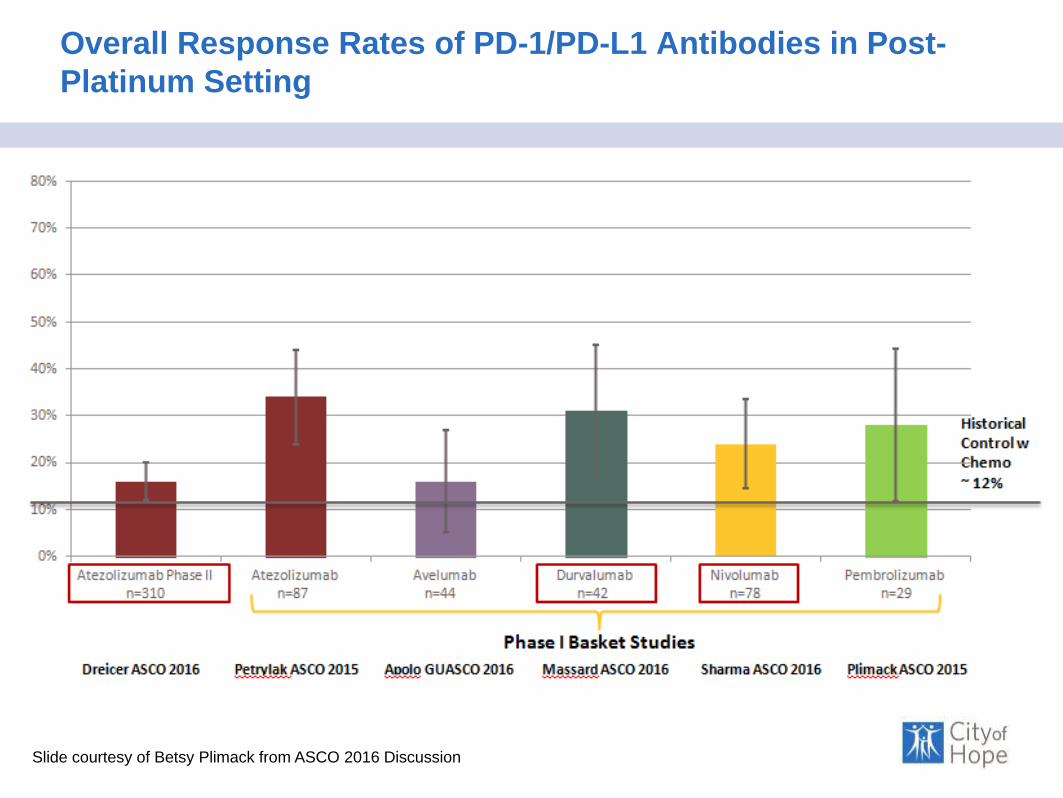
Overall Response Rates of PD-1/PD-L1 Antibodies in Post-
Platinum Setting
Slide courtesy of Betsy Plimack from ASCO 2016 Discussion
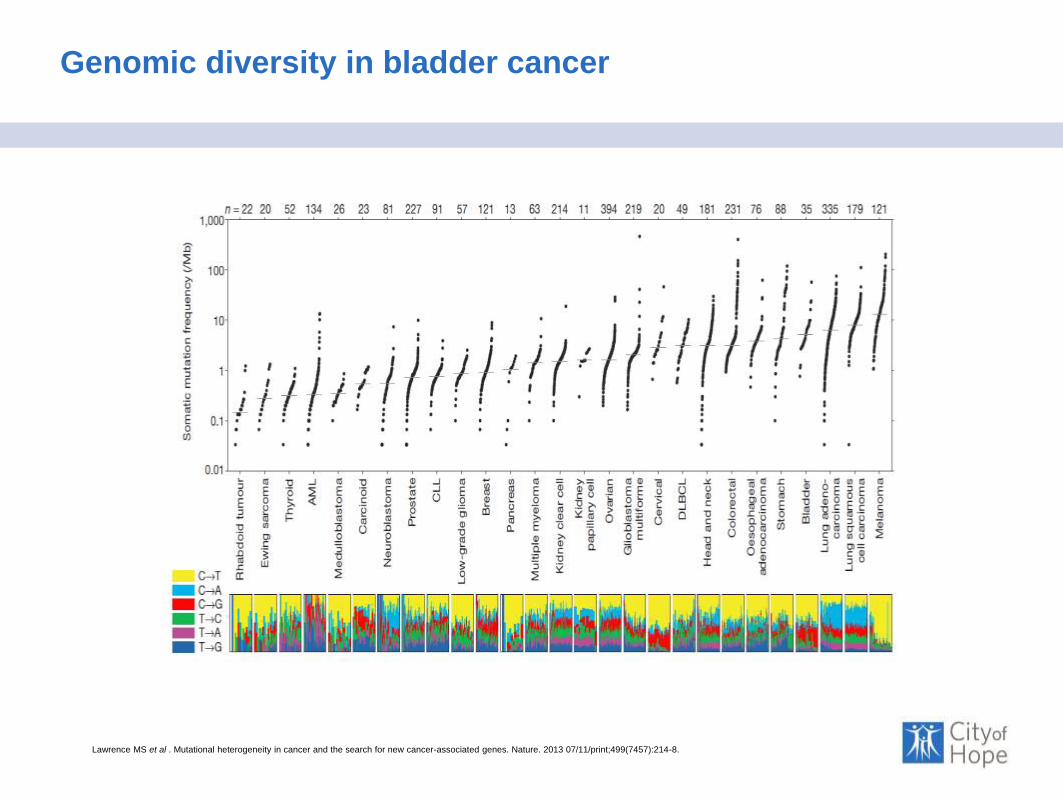
Genomic diversity in bladder cancer
Lawrence MS et al . Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013 07/11/print;499(7457):214-8.

Atezolizumab in bladder cancer
Rosenberg JE et al Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm,
multicentre, phase 2 trial. The Lancet.
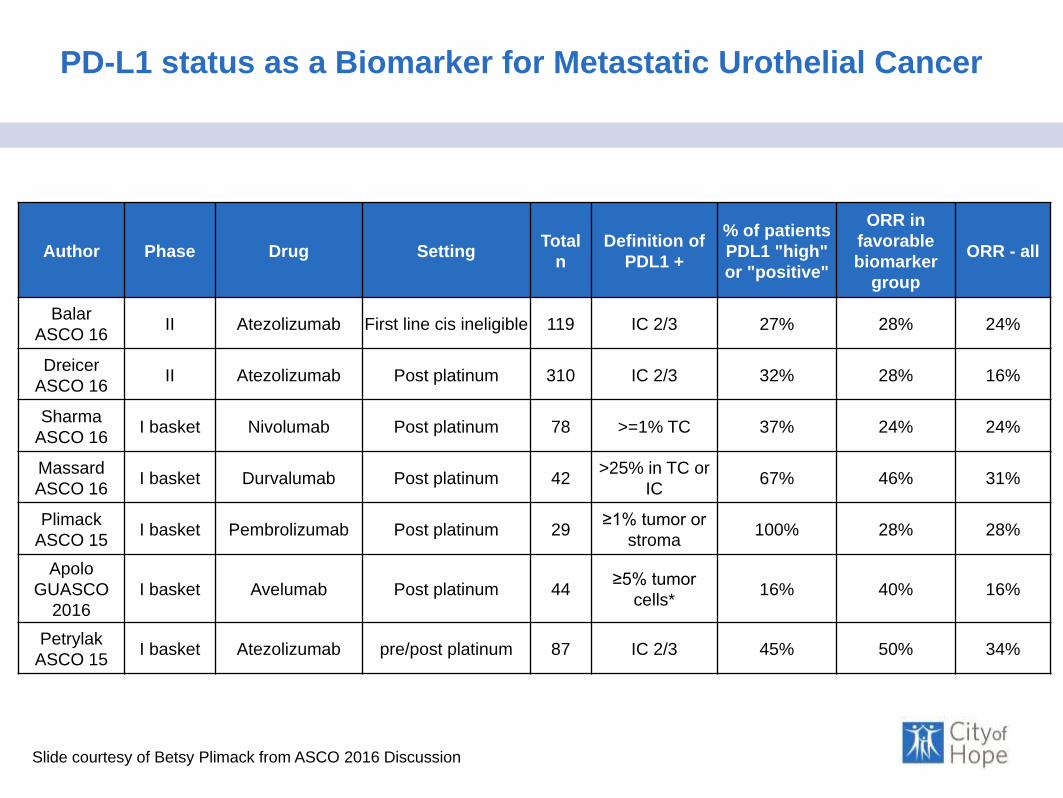
PD-L1 status as a Biomarker for Metastatic Urothelial Cancer
Slide courtesy of Betsy Plimack from ASCO 2016 Discussion
Author Phase Drug SettingTotal
n
Definition of
PDL1 +
% of patients
PDL1 "high"
or "positive"
ORR in
favorable
biomarker
group
ORR - all
Balar
ASCO 16II Atezolizumab First line cis ineligible 119 IC 2/3 27% 28% 24%
Dreicer
ASCO 16II Atezolizumab Post platinum 310 IC 2/3 32% 28% 16%
Sharma
ASCO 16I basket Nivolumab Post platinum 78 >=1% TC 37% 24% 24%
Massard
ASCO 16I basket Durvalumab Post platinum 42
>25% in TC or
IC67% 46% 31%
Plimack
ASCO 15I basket Pembrolizumab Post platinum 29
≥1% tumor or
stroma100% 28% 28%
Apolo
GUASCO
2016
I basket Avelumab Post platinum 44≥5% tumor
cells*16% 40% 16%
Petrylak
ASCO 15I basket Atezolizumab pre/post platinum 87 IC 2/3 45% 50% 34%

•Locally advanced or metastatic urothelialcarcinoma.•Predominantly urothelialhistology•Tumor tissue for PD-L1 testing
Cohort 1 (N=119)11 Cisplatin Ineligible
Cohort 2 (N-310)Platinum-treated nUC
Co-primary endpoints:
•ORR (confirmed) per RECIST v1.1 by central review
•ORR per immune-modified RECIST by investigator
Key secondary endpoints
•DOR, PFS, OS, safety
Key exploratory endpoints
•Intratumoral biomarkers
Imvigor 210 Study Design
Cohort 1 to be shown later
Atezolizumab 1200 mg IV q3w until
Loss of Benefit
Cohort 2-Specific Inclusion Criteria
• Progression during/following platinum
(no restrictions on # prior lines of
therapy)
• ECOG PS 0-1
• CrCl ≥ 30 mL/min
Median follow-up: 17.5 months (range, 0.2 to 21.1+ mo)
Dreicer R et al. IMvigor210: Atezolizumab in platinum-treated mUC. ASCO 2016

Imvigor 210 Cohort 1 Data from ASCO
IC2/3
(n = 32)
IC1/2/3
(n = 80)
All Patients
(N = 119)
IC1
(n = 48)
IC0
(n = 39)
ORRa (95% CI) 28% (14, 47) 25% (16, 36) 24% (16, 32) 23% (12, 37) 21% (9, 36)
CR 6% 6% 7% 6% 8%
PR 22% 19% 17% 17% 13%
Subgroup ORRa 95% CI
Demographics and prior treatment
Age ≥ 80 years (n = 25) 28% 12, 49
Perioperative chemob (n = 22) 36% 17, 59
Primary tumor sites
Bladder/urethra (n = 85) 17% 9, 26
Upper tract (n = 33) 42% 25, 61
Metastatic sites at baseline
Lymph node only (n = 31) 32% 17, 51
Visceralc (n = 78) 15% 8, 25
Liver (n = 25) 12% 3, 31
Cisplatin ineligibility criteria
Impaired renal function (n = 83) 27% 17, 37
ECOG PS2 (n = 24) 25% 10, 47
Renal impairment and ECOG PS2 (n = 8) 25% 3, 65 Balar AV et al. ASCO 2016; LBA4500.
Key Demographics
• 28% with upper tract disease
• 70% with Cr Cl 30-60
• 20% ECOG 2
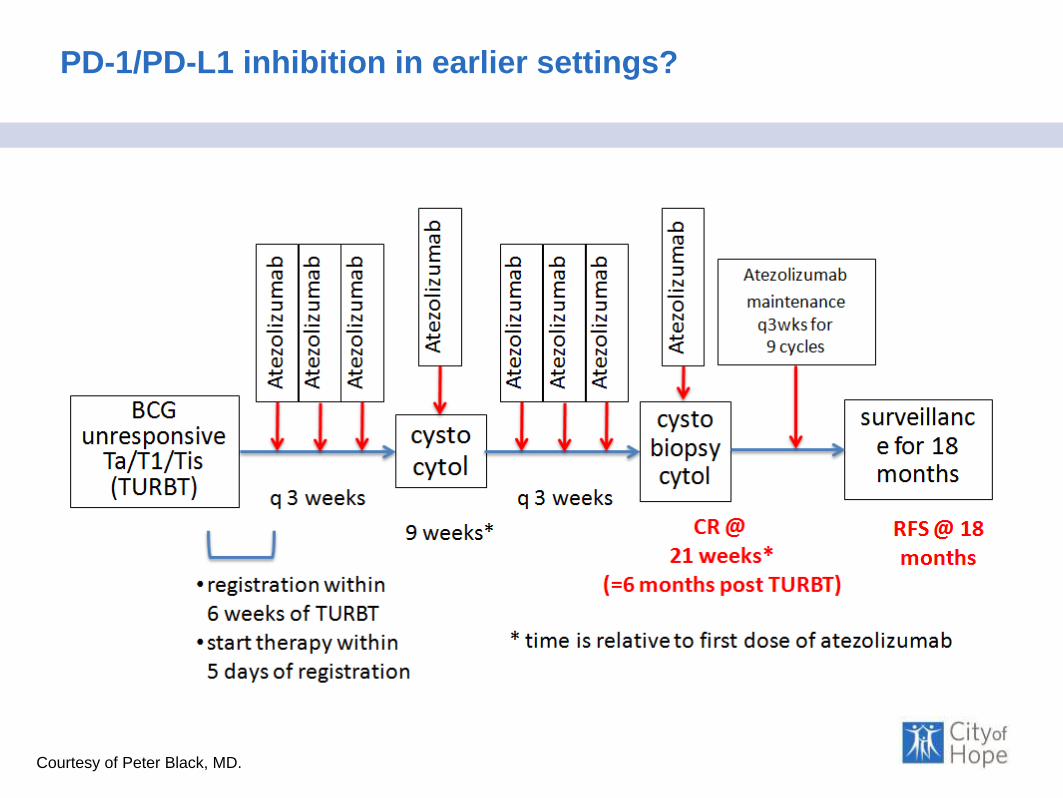
PD-1/PD-L1 inhibition in earlier settings?
Courtesy of Peter Black, MD.
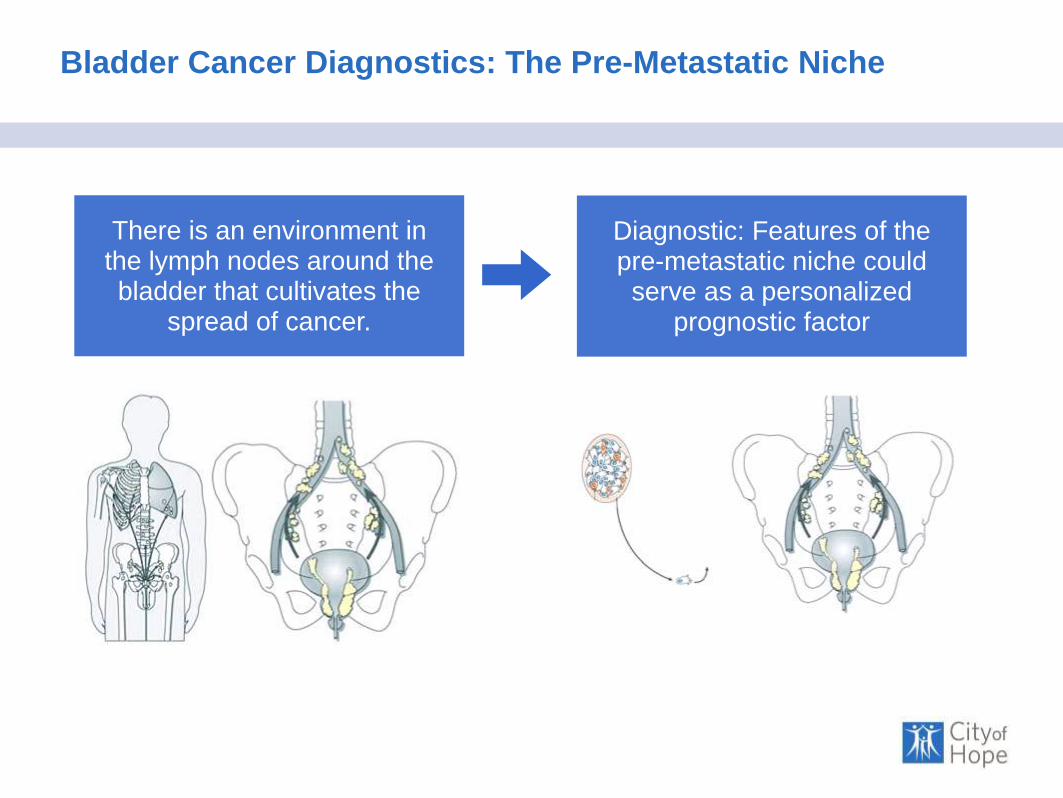
Bladder Cancer Diagnostics: The Pre-Metastatic Niche
There is an environment in the lymph nodes around the bladder that cultivates the
spread of cancer.
Diagnostic: Features of the pre-metastatic niche could serve as a personalized
prognostic factor
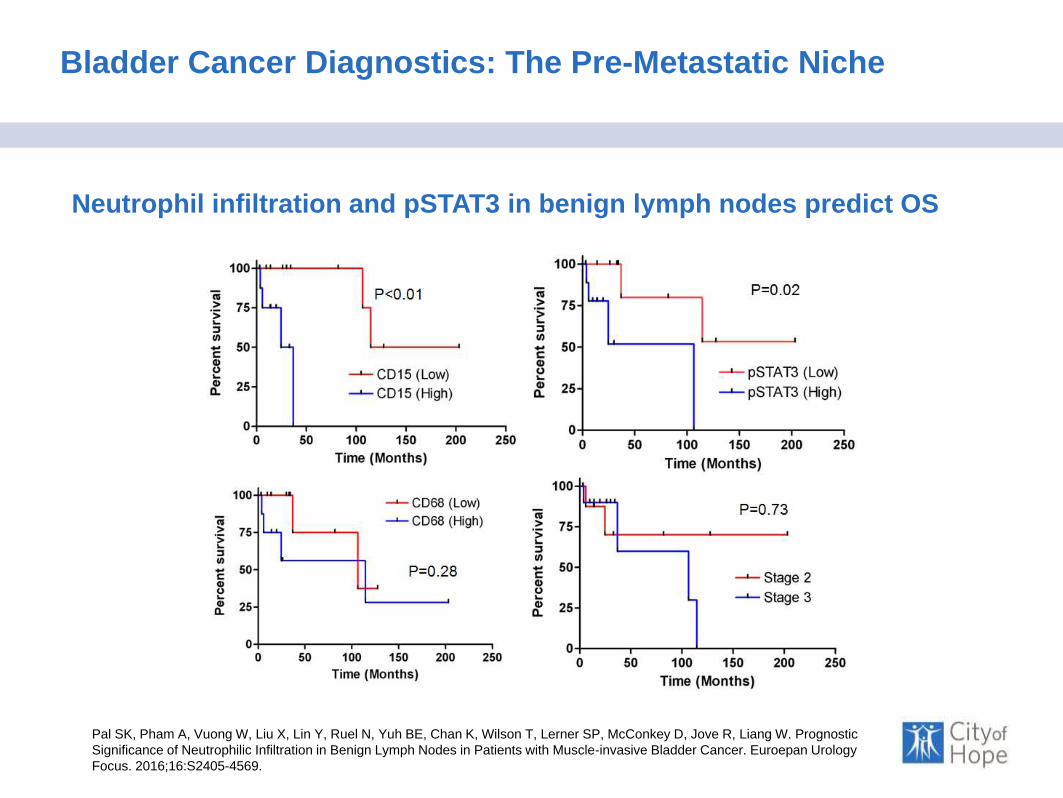
Bladder Cancer Diagnostics: The Pre-Metastatic Niche
Pal SK, Pham A, Vuong W, Liu X, Lin Y, Ruel N, Yuh BE, Chan K, Wilson T, Lerner SP, McConkey D, Jove R, Liang W. Prognostic
Significance of Neutrophilic Infiltration in Benign Lymph Nodes in Patients with Muscle-invasive Bladder Cancer. Euroepan Urology
Focus. 2016;16:S2405-4569.
Neutrophil infiltration and pSTAT3 in benign lymph nodes predict OS
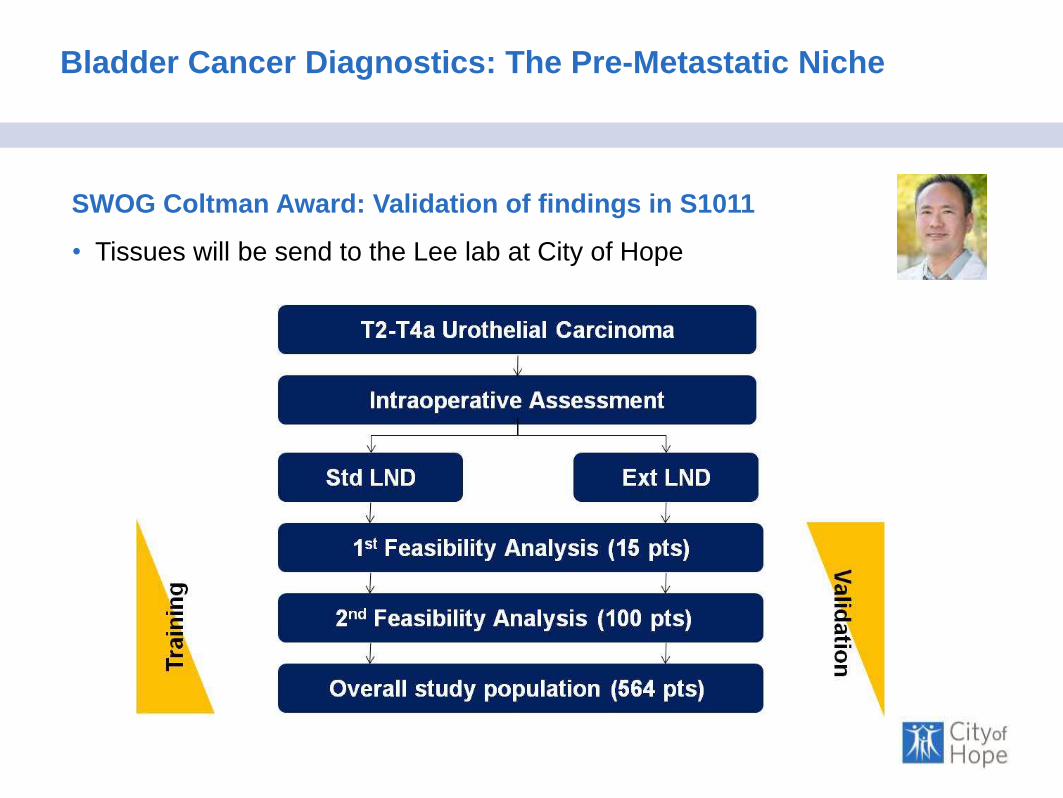
Bladder Cancer Diagnostics: The Pre-Metastatic Niche
SWOG Coltman Award: Validation of findings in S1011
• Tissues will be send to the Lee lab at City of Hope

Overview
Topic
Nature of Treatment
Disease Bladder Cancer
Immune
MOAPD-1-
Directed Therapy
Targeted
MOAFGFR and
HER2 inhibition
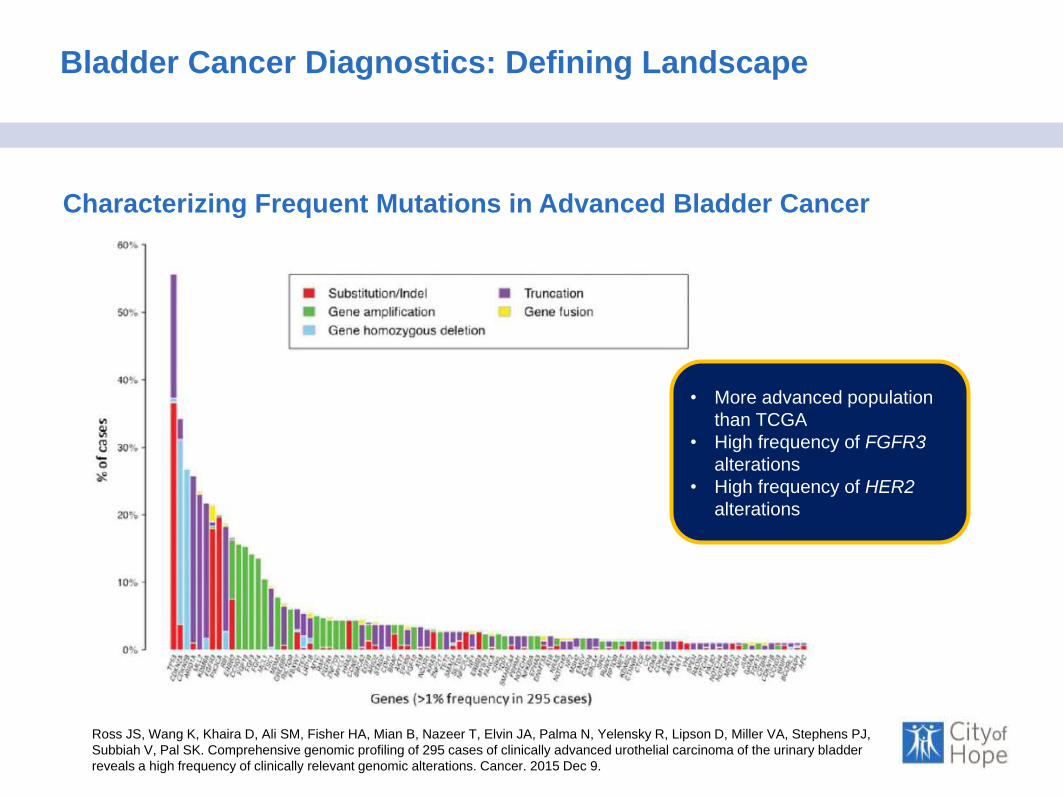
Bladder Cancer Diagnostics: Defining Landscape
Characterizing Frequent Mutations in Advanced Bladder Cancer
Ross JS, Wang K, Khaira D, Ali SM, Fisher HA, Mian B, Nazeer T, Elvin JA, Palma N, Yelensky R, Lipson D, Miller VA, Stephens PJ,
Subbiah V, Pal SK. Comprehensive genomic profiling of 295 cases of clinically advanced urothelial carcinoma of the urinary bladder
reveals a high frequency of clinically relevant genomic alterations. Cancer. 2015 Dec 9.
• More advanced population
than TCGA
• High frequency of FGFR3
alterations
• High frequency of HER2
alterations
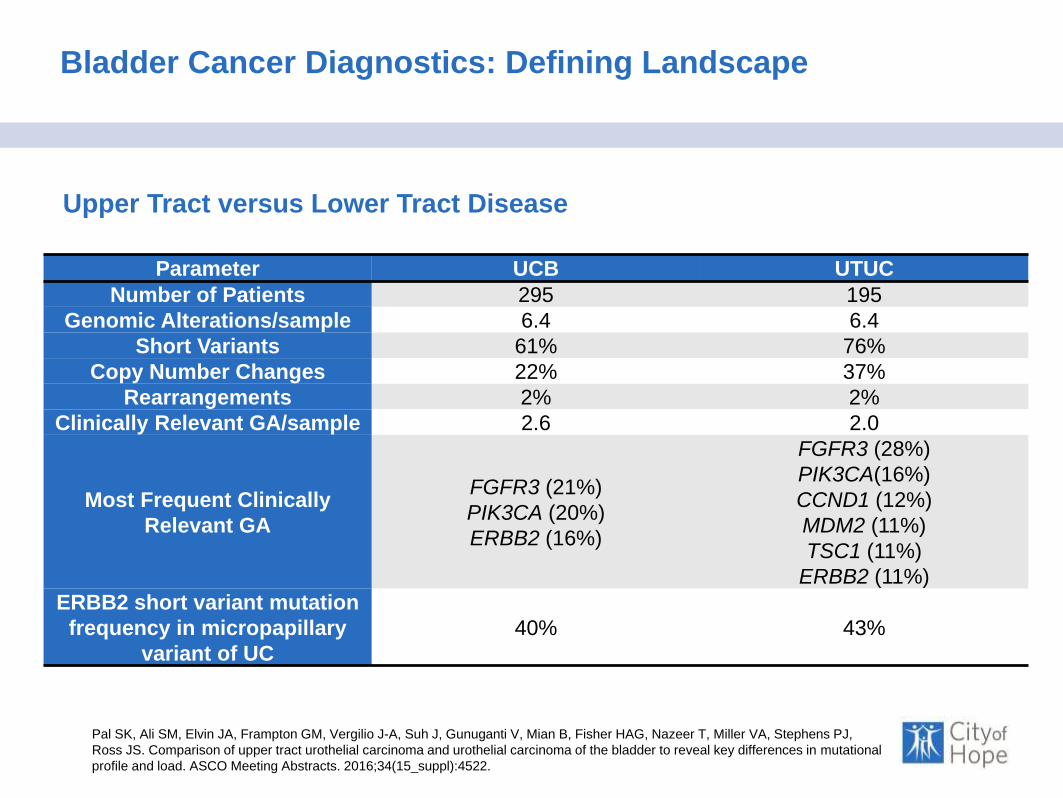
Bladder Cancer Diagnostics: Defining Landscape
Upper Tract versus Lower Tract Disease
Pal SK, Ali SM, Elvin JA, Frampton GM, Vergilio J-A, Suh J, Gunuganti V, Mian B, Fisher HAG, Nazeer T, Miller VA, Stephens PJ,
Ross JS. Comparison of upper tract urothelial carcinoma and urothelial carcinoma of the bladder to reveal key differences in mutational
profile and load. ASCO Meeting Abstracts. 2016;34(15_suppl):4522.
Parameter UCB UTUC
Number of Patients 295 195
Genomic Alterations/sample 6.4 6.4
Short Variants 61% 76%
Copy Number Changes 22% 37%
Rearrangements 2% 2%
Clinically Relevant GA/sample 2.6 2.0
Most Frequent Clinically
Relevant GA
FGFR3 (21%)
PIK3CA (20%)
ERBB2 (16%)
FGFR3 (28%)
PIK3CA(16%)
CCND1 (12%)
MDM2 (11%)
TSC1 (11%)
ERBB2 (11%)
ERBB2 short variant mutation
frequency in micropapillary
variant of UC
40% 43%

Bladder Cancer Diagnostics: Defining Landscape
Smoking vs Non-Smoking
Joshi M, Vasekar M, Grivas P, Emamekhoo H, Hsu J, Miller VA, Stephens PJ, Ali SM, Ross JS, Zhu J, Warrick J, Drabick JJ, Holder
SL, Kaag M, Li M, Pal SK. Relationship of smoking status to genomic profile, chemotherapy response and clinical outcome in patients
with advanced urothelial carcinoma. Oncotarget. 2016 May 18.
• Never, current and ex-smokers have a distinct
genomic profile
• GAs in NSD1 were more frequent in CS as
compared to other groups (P < 0.001)
Bladder Cancer Diagnostics: Setting Guidelines
Pal SK, Agarwal N, Boorjian SA, Hahn NM, Siefker-Radtke AO, Clark PE, Plimack ER. National Comprehensive Cancer Network
Recommendations on Molecular Profiling of Advanced Bladder Cancer. J Clin Oncol. 2016 Jul 25.
• There is a dearth of available therapies
• Even immunotherapy approaches are non-curative
• Broader use of genomic profiling will facilitate studies of targeted
therapy in this disease
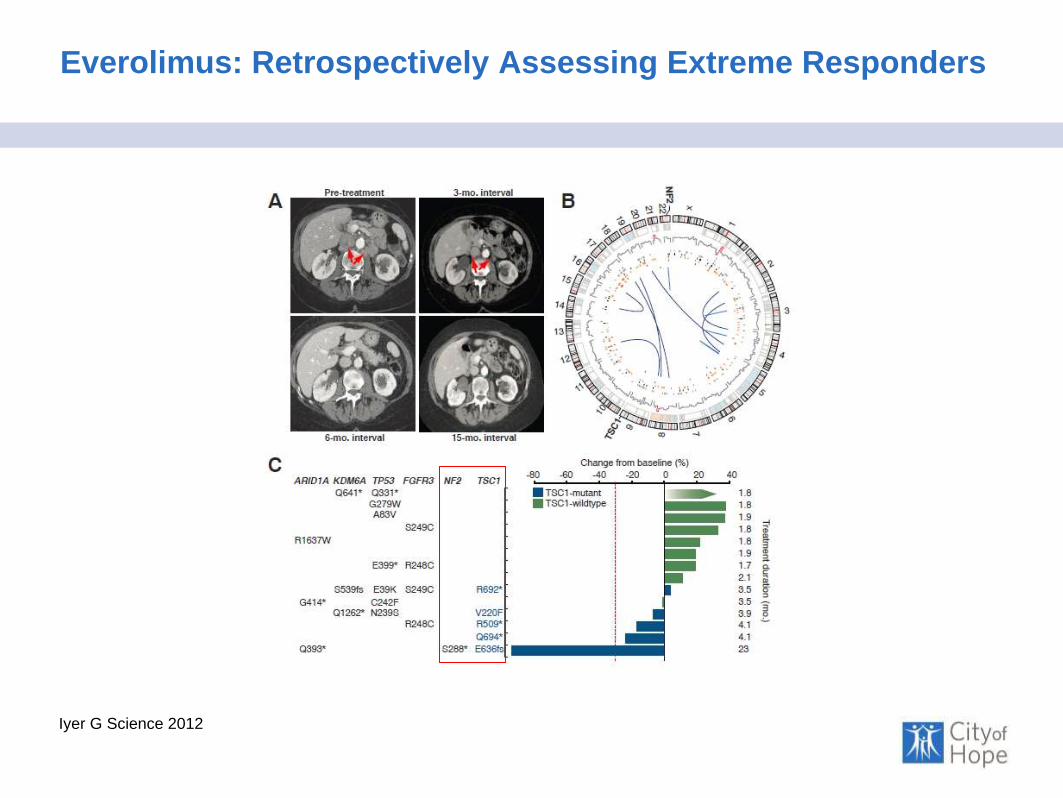
Everolimus: Retrospectively Assessing Extreme Responders
Iyer G Science 2012

Everolimus: Applying FM Results to an Individual Case
Ali S (Submitted)
AuthorTiming of Genomic
Profiling
mTOR Pathway
Alternations
Other Genomic
Alterations
Iyer et al Retrospective after
treatment
TSC1/NF2 Unknown
Wagle et al Retrospective after
treatment
MTOR E2014k,
E2419K
CTNNB1, TP53
Ali et al Prospective and
guided treatment
NF2 TP53, ATRX,
ATM

Targets To Explore …
Pal SK, Milowsky MI, Plimack ER. Optimizing systemic therapy for bladder cancer. Journal of the National
Comprehensive Cancer Network : JNCCN 2013 Jul 1;11(7):793-804.

Dovitinib
Milowsky ASCO GU 2013
FGFR3 mut
Group 1: FGFR3 mut
~20 patients
Group 1: FGFR3 mut
~ 20 patients
FGFR3 WT
Group 2: FGFR3 WT
~20 patients
Group 2: FGFR3 WT
~ 20 patients
Stratification / Study Entry
Treatment with Dovitinib500 mg p.o. 5 days on / 2 days off, cycle: 28 days
Study EndpointsPrimary: ORR (CR, PR)
Secondary: PFS, DCR, Safety, PK Profile
Stage 1
Stage 2

Dovitinib
Milowsky ASCO GU 2013
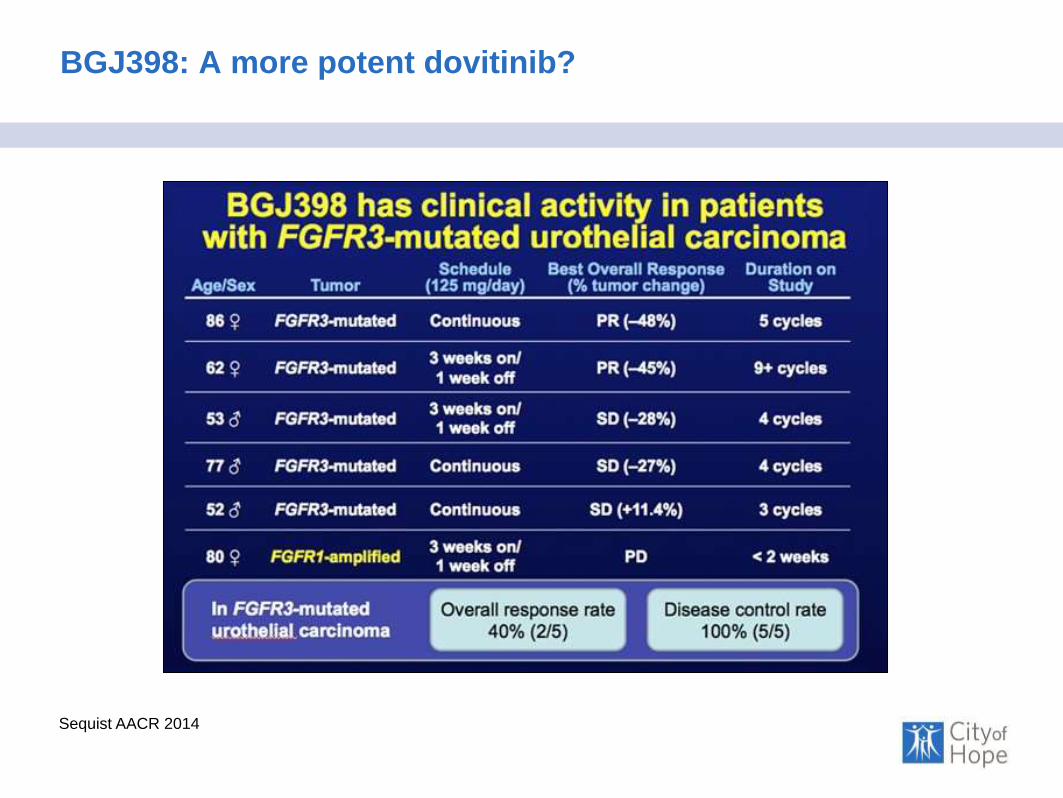
BGJ398: A more potent dovitinib?
Sequist AACR 2014

FGFR3 inhibition in bladder cancer
Bladder Cancer Therapeutics: Targeted Therapies
Ross JS, Wang K, Khaira D, Ali SM, Fisher HA, Mian B, Nazeer T, Elvin JA, Palma N, Yelensky R, Lipson D, Miller VA, Stephens PJ,
Subbiah V, Pal SK. Comprehensive genomic profiling of 295 cases of clinically advanced urothelial carcinoma of the urinary bladder
reveals a high frequency of clinically relevant genomic alterations. Cancer. 2015 Dec 9.

FGFR3 inhibition in bladder cancer
Bladder Cancer Therapeutics: Targeted Therapies
Pal SK, Rosenberg JE, Keam B, Wolf J, Berger R, Dittrich C, Hoffman-Censits JH, Quinn D, van der Noll R, Burris HA, Galsky MD,
Gravis G, Lee J-L, Medioni J, Mortazavi A, Maroto P, Parker K, Chen X, Isaacs R, Bajorin DF. Efficacy of BGJ398, a fibroblast growth
factor receptor (FGFR) 1-3 inhibitor, in patients (pts) with previously treated advanced/metastatic urothelial carcinoma (mUC) with
FGFR3 alterations. ASCO Meeting Abstracts. 2016;34(15_suppl):4517.

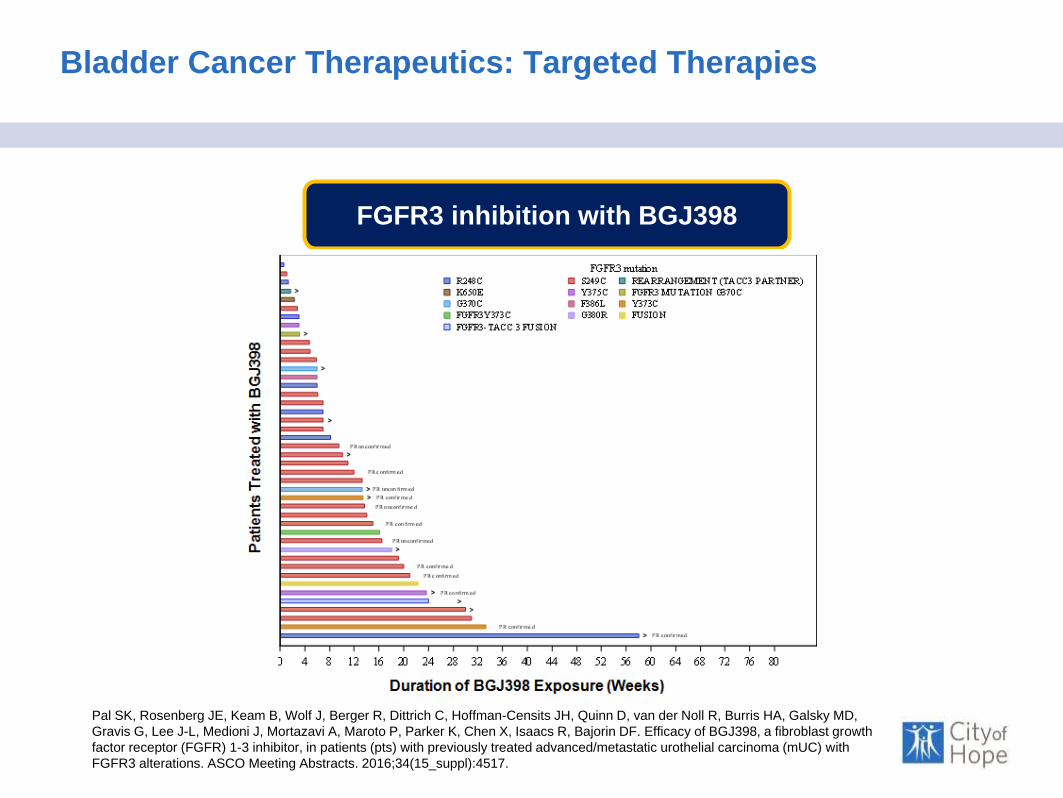
FGFR3 inhibition with BGJ398
Bladder Cancer Therapeutics: Targeted Therapies
Pal SK, Rosenberg JE, Keam B, Wolf J, Berger R, Dittrich C, Hoffman-Censits JH, Quinn D, van der Noll R, Burris HA, Galsky MD,
Gravis G, Lee J-L, Medioni J, Mortazavi A, Maroto P, Parker K, Chen X, Isaacs R, Bajorin DF. Efficacy of BGJ398, a fibroblast growth
factor receptor (FGFR) 1-3 inhibitor, in patients (pts) with previously treated advanced/metastatic urothelial carcinoma (mUC) with
FGFR3 alterations. ASCO Meeting Abstracts. 2016;34(15_suppl):4517.
FGFR3 inhibition with BGJ398
Bladder Cancer Therapeutics: Targeted Therapies
Pal SK, Rosenberg JE, Keam B, Wolf J, Berger R, Dittrich C, Hoffman-Censits JH, Quinn D, van der Noll R, Burris HA, Galsky MD,
Gravis G, Lee J-L, Medioni J, Mortazavi A, Maroto P, Parker K, Chen X, Isaacs R, Bajorin DF. Efficacy of BGJ398, a fibroblast growth
factor receptor (FGFR) 1-3 inhibitor, in patients (pts) with previously treated advanced/metastatic urothelial carcinoma (mUC) with
FGFR3 alterations. ASCO Meeting Abstracts. 2016;34(15_suppl):4517.

Bladder Cancer Therapeutics: Targeted Therapies
DNA Repair Pathways Remain Essential in Bladder Cancer
• VX-970 is a first-in-class ATR inhibitor and may synergize with cisplatin
Adapted from Jackson SP, Bartek J. The DNA- damage response in human biology and disease Nature (2009) 461, 1071
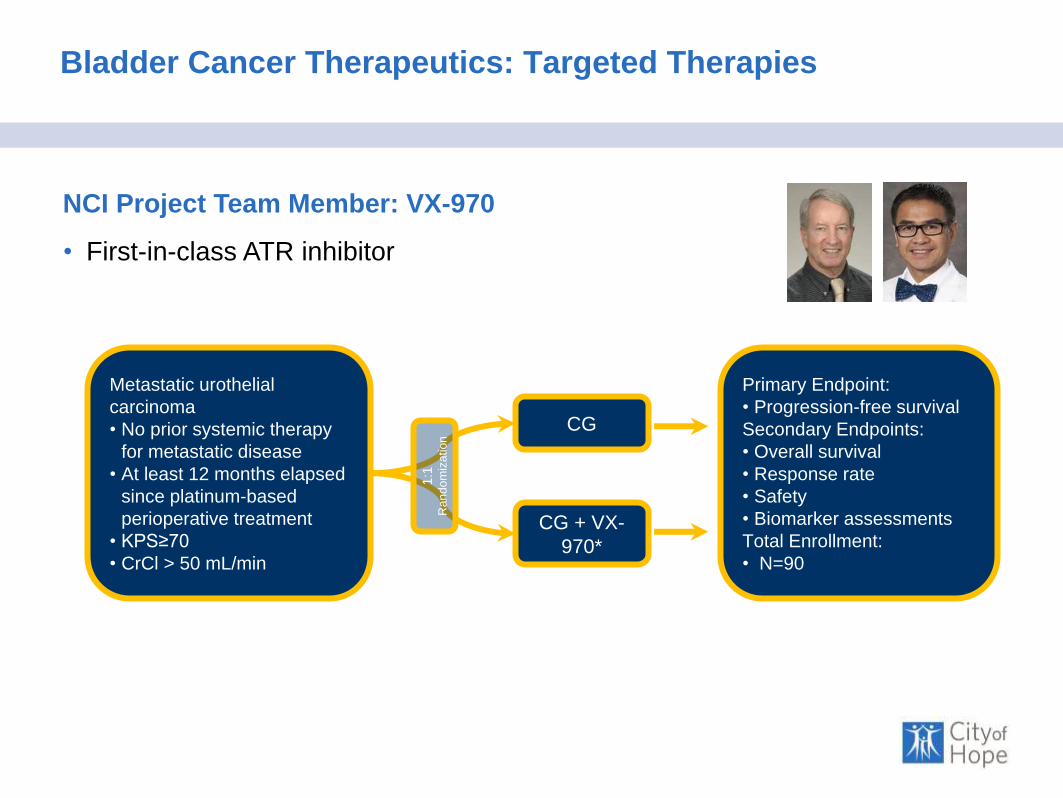
Bladder Cancer Therapeutics: Targeted Therapies
NCI Project Team Member: VX-970
• First-in-class ATR inhibitor
Metastatic urothelial
carcinoma
• No prior systemic therapy
for metastatic disease
• At least 12 months elapsed
since platinum-based
perioperative treatment
• KPS≥70
• CrCl > 50 mL/min
CG
CG + VX-
970*
1:1
R
andom
iza
tion
Primary Endpoint:
• Progression-free survival
Secondary Endpoints:
• Overall survival
• Response rate
• Safety
• Biomarker assessments
Total Enrollment:
• N=90

Bladder Cancer Therapeutics: Chemo as targeted therapy?
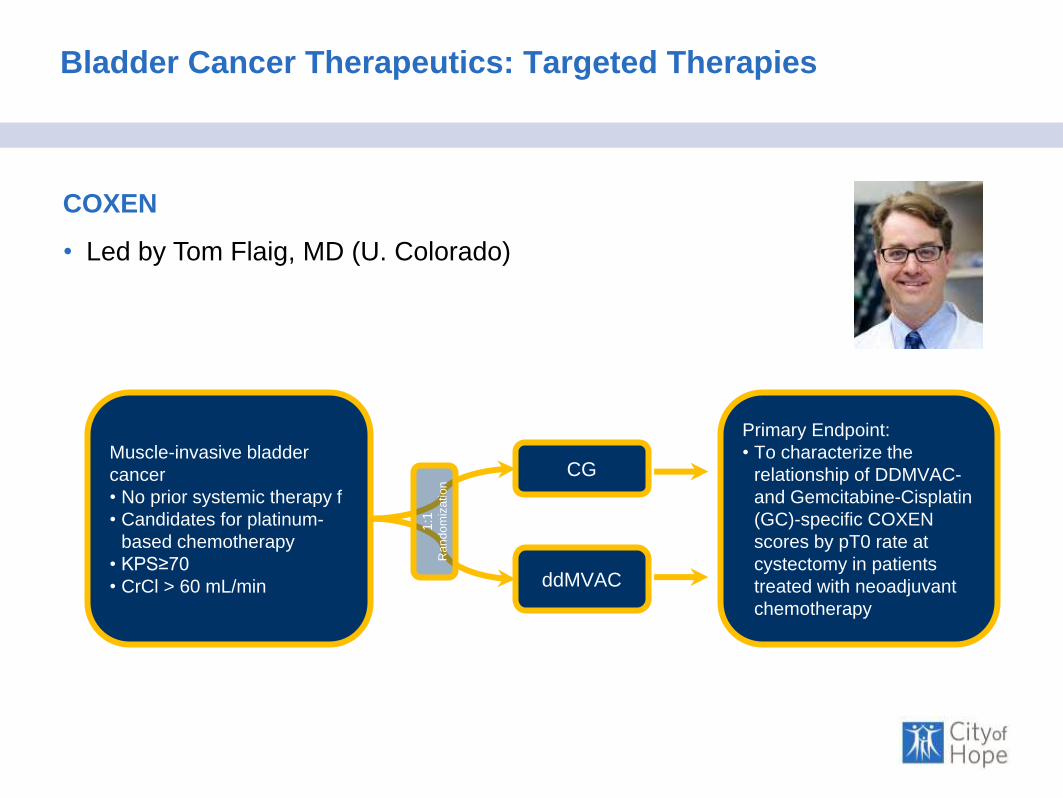
Bladder Cancer Therapeutics: Targeted Therapies
Muscle-invasive bladder
cancer
• No prior systemic therapy f
• Candidates for platinum-
based chemotherapy
• KPS≥70
• CrCl > 60 mL/min
CG
ddMVAC
1:1
R
andom
ization
Primary Endpoint:
• To characterize the
relationship of DDMVAC-
and Gemcitabine-Cisplatin
(GC)-specific COXEN
scores by pT0 rate at
cystectomy in patients
treated with neoadjuvant
chemotherapy
COXEN
• Led by Tom Flaig, MD (U. Colorado)