mn nurses strike advances hospital safety, quality debate, need for new system
DESCRIPTION
MN Nurses Strike Advances Hospital Safety, Quality Debate, Need for New System. By Joel Albers health economist, clinical pharmacist Universal Health Care Action Network-MN 612-636-3838, [email protected] July 12, 2010. Hospital Safety,Quality of Care. Deterioration in Quality of Care. - PowerPoint PPT PresentationTRANSCRIPT

MN Nurses Strike Advances Hospital Safety, Quality Debate, Need for New
System
By Joel Albershealth economist, clinical pharmacist
Universal Health Care Action Network-MN612-636-3838, [email protected]
July 12, 2010

Hospital Safety,Quality of Care

Deterioration in Quality of Care
• 1999 Institute of Medicine landmark report found medical errors in hospitals kill up to 98,000 people/yr,8 th leading cause of death in U.S.
• IOM “Care W/out Coverage report found 44,000 unnecessary deaths every year in U.S.
• WHO: Health System Rating US Ranks 37th in the World in quality of care who.int/whr/2000/en/report.htm
• ER Waiting time is 1 hr before seeing a M.D., up from 38 minutes in 1997.

Mandated Nurse:Patient Ratios Calif
• Associated w/ significantly lower mortality• Less nurse burnout• Greater job satisfaction• 22,336 hospital staff nurses surveyed, cross-sectional• Data supporting this association growing; 90 studies
Source: Implications of the California nurse staffing mandate for other states. Health Services Research,pp1-18, http://tinyurl.com/y7rdzys



Nurse Staffing Improves Care
• Increased hours of nursing care is associated with better care of hospitalized patients
Needleman et al NEJM 2002
VA: Highest quality care
• Outperformed other providers by 20% in prevention
• Significantly better in chronic disease,overall quality
• Coordinated approach to care
• Systemwide electronic health record
• Excellent quality measurement tools
• Source: Elizabeth McGlynn, RAND Health



MN Hospital Financial Trends

Hospitals are Largest Component of Health Care Spending, 2005:
15%
12%
15%
3%
3%
22%
29%
17%
11%
9%
5%
3%
23%
33%
0% 5% 10% 15% 20% 25% 30% 35%
Other Spending
Prescription Drugs
Long Term Care (includingHome Care)
Dental Services
Other Professional Services
Physician Services
Hospital Care
Minnesota U.S.
Note: Some spending included in hospital services in the national estimate is defined as long term care spending in the Minnesota estimates.Sources: MDH Health Economics Program and Centers for Medicare and Medicaid Services (estimated spending for health services and supplies).
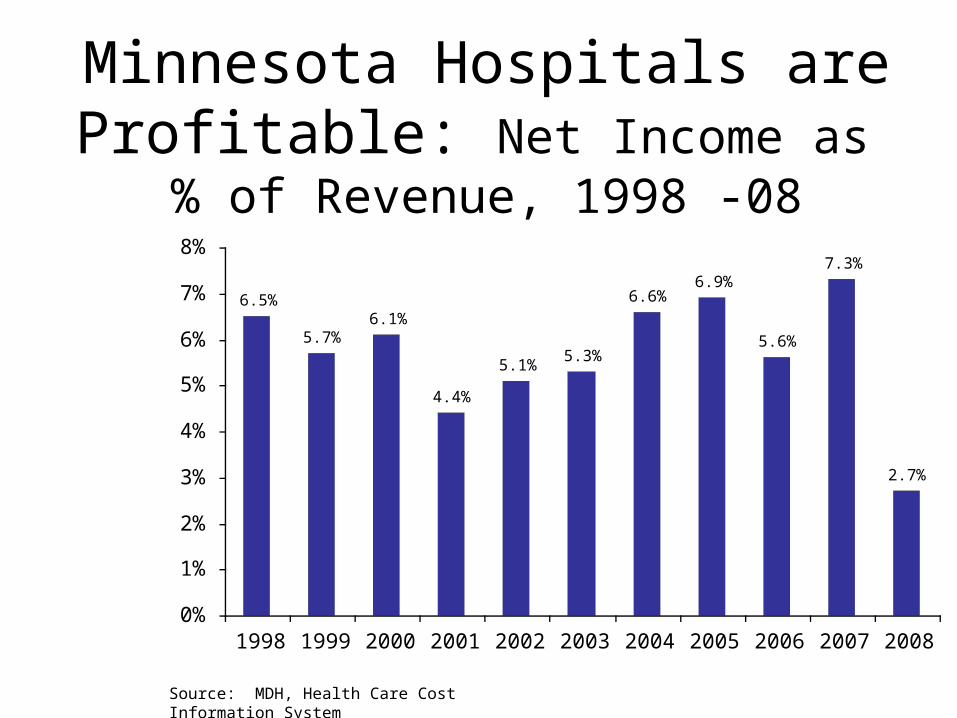
Minnesota Hospitals are Profitable: Net Income as % of Revenue, 1998 -08
6.5%
5.7%6.1%
4.4%
5.1%5.3%
6.6%6.9%
5.6%
7.3%
2.7%
0%
1%
2%
3%
4%
5%
6%
7%
8%
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Source: MDH, Health Care Cost Information System

MN’s Largely “Non-profit” Hospitals accrue even more profit
Non-profit
requirements
Total
in millions
% of operating expenses, 2005
Value of tax exemptions
$ 482.0 5.0%
Uncompensated care
$ 191.2 2.0%
Source:Mn Hospitals: Uncompensated care,community benefits,and the value of tax exemptions,Mn Dept
Health,2007.

Despite Profits,MN Hospitals Cut 100s of Jobs during recession
• Park Nicollet 233• North Memorial 380• Allina 300• Fairview 175• HCMC 100• Regions 30
Source: Recession afflicting metro-area hospitals, Mpls-St Paul StarTribune, Dec 7,2008, other articles.cuts include clinical staff.

Yet Major Capital Expenditure Commitments by MN Hospitals
2007 2008
Percent of Minnesota hospitals reporting major capital expenditure commitment
29.9% 26.1%
Total number of capital expenditure commitments reported
95 95
Value of major capital expenditure commitments reported ($ millions)
$1,118.2 $458.3
Major spending commitments that are reportable under 62J.17 include expenditures in excess of $ 1 million.Source: MDH, Health Care Cost Information System




MN Hospital and Insurance Structure

HEALTHCARE INFRASTRUCTURE:Enough to serve all Minnesotans
• 127,142 healthcare practitioners & technicians
• 140 hospitals with a total of 16,503 staffed beds
• 413 nursing homes• 1,023 home care providers
(facilities and services)

4 HMOs Control MN Health Care
• Blue Cross-Blue Shield 2 million members
• Medica 1 million members
• HealthPartners 660,000 members
• Preferred One 600,000 members
• These 4 insure 9 of every 10 insured Minnesotans • Own or investors in most of MN’s major hospitals & clinics• 646 HMOs and commercial insurers are licensed to sell health and accident
insurance in the state of Minnesota
Source: HMO companies,2002. MN Dept of Health, MN Dept of Commerce

Allina 27%, 29.2%
Fairview University 26%, 20.9%HealthEast12.0%, 12.1%
Hennepin Cty 8%,6.3%
HealthPartners,(was Regions) 7%,7.6%
Methodist 6%
Children’s 5%,5.6% Other non-affiliated 3%,3.9%
Twin Cities Hospital Market Share*,1996 & 2001
Source: MN Dept of Health, Consolidation in MN’s Health Care Market, Issue Brief 98-04, MN Managed Care Review 2002, Part one
*Measured as % of Inpatient Admissions
N.Memorial 7%,7.8%

Implications of Fixed costs
• Once a facility or service is up and running, we pay for it whether it is used or not
• Trying to save money by keeping patients out of the hospital is like trying to save money on schools by keeping kids home for the day
• It is much more cost effective to invest in only what we need.

Hospital Administrative Budget Squeezes Clinical Budget
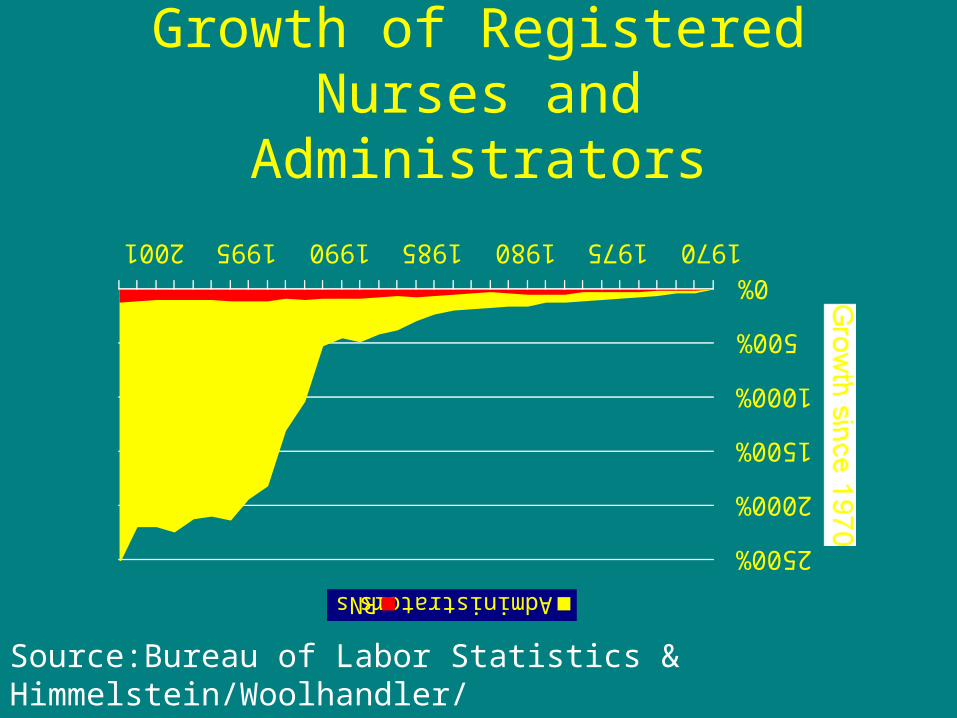
Growth of Registered Nurses and Administrators
0%
500%
1000%
1500%
2000%
2500%
1970197519801985199019952001
Growth since 1970
AdministratorsRNs
Source:Bureau of Labor Statistics & Himmelstein/Woolhandler/Lewontin Analysis of CPS Data


0
500
1000
1500
2000
2500
1970 1975 1980 1985 1990 1995
Administrators
RNs
Physicians
Do you want your
health care
dollars spent
Here or
Here?

Nurses, Labor Unions & Health Care

Health Care Problems for Labor Union Members
*More time is spent negotiating benefits than wage increases
*Wage increases are often eaten up by rising health care costs
*Health care benefits suspended while members are on strike
*Employers are shifting ever more costs of health care to working families
Source: MN COACT

8 Labor Union Strikes Provoked by Health Costs
• 2005 Crosby-Ironton Teachers
• 2004 Bus Drivers ATU 1005
• 2003 AFSCME 3800 U of MN
• 2002 Teachers in Red Wing
• 2002 Teachers in International Falls
• 2001 Nurses Fairview Hosp;
• 2001 MN Assn Prof. Employees
• 2000 HERE , Hotel and Restaurant Union• 2000 Teamsters Mpls Pepsi

Hospital Workers Strike Their Own Hospitals 4 Times April & May 2003
*Service Employees Int’l Union 900 members walked out of United Hospital & Children’s Hospital
*SEIU says Hospital charges workers 2 x as much as CEOs for health insurance
*United Worker’s family $479/mo, CEO $153/mo
*Other hospitals too,strike approval all 90%
Source: Union Advocate, April 24,2003,p1,5;May 15,p4
22 Day Strike by 1,350 MN RNs, 2001*MNA says: “Patient care is being compromised in our hospitals because not enough
nurses are on staff”*Allina spent $8.6 million, Fairview $5 million in RN OT pay,2 000
*RN rural MN worked 42 days w/ only 1 day off*RNs seek say in patient flow, workload, staff levels; pay, benefits
*Hospitals refused to negotiate these issues in a meaningful way*“We cannot and will not accept these conditions for ourselves or for those who follow us
in this profession”
*New contract upped Fairview’s share of premiums from the current 65- 68% of family coverage to 75% in ‘02.Upped pay 19.5%/3 yrs
Source: Fairview nurses OK pact, ending strike. St Paul Pioneer Press,June 26, 2001;Brochure,MNA nurses are standing up and speaking out for safe patient care

Government-funded System will Resolve the HC Crisis