mitral valve repair - pdfs.semanticscholar.org · of mitral regurgitation was seen in our series...
TRANSCRIPT

Circulation Journal Vol.78, March 2014
560 KANEKO T et al.Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
and the robotic assisted surgery was introduced by Chitwood et al12 in 1997.
Philosophy of Mitral Valve RepairMitral valve repair is shown to have better survival, preservation of ventricular function and decreased thromboembolic compli-cations compared to mitral valve replacement for mitral regur-gitation (MR).13–15 At our institution, we have developed a sim-ple algorithm for mitral valve repair in myxomatous disease, which allows reproducible and durable repair. Our general plan is described by the following steps: 1. Assess the valve after opening the left atrium through
Sondergaard’s groove. A saline test is used, as well as a preoperative transesophageal echocardiogram (TEE), to find the exact etiology and pathologic malformation.
2. Perform a standard repair technique to the most obvious lesion causing regurgitation (eg, quadrangular resection to the posterior leaflet.)
3. Use the height of the anterior leaflet to measure and place a prosthetic annuloplasty ring.
4. Test the valve after the ring placement and repair any re-sidual lesions if needed.
We believe that over 90% of the valves will be repaired using this algorithm, even for the bileaflet prolapsed valve. Coordi-nation with cardiac anesthesia colleagues is the key, with TEE images providing more accurate anatomic valve etiology allow-ing surgeons to plan the repair strategies prior to opening the left atrium, and following separation from cardiopulmonary bypass.
Indications for Mitral Valve RepairFrom the Society of Thoracic Surgeons (STS) database, the rate of mitral repair for isolated MR has increased from 51% in 2000 to 69% in 2007 in the USA.16 Current American College of Cardiology/American Heart Association (ACC/AHA) guide-
History of Mitral Valve SurgeryThe first successful mitral valvuloplasty (MVP) was performed at the Peter Bent Brigham Hospital (PBBH) in 1923. Future Chief of Surgery, Dr Elliott Cutler, performed a successful valvulotomy in a 12 year-old girl with rheumatic mitral steno-sis.1 This was done using a neurosurgical tenotomy knife transventricularly, and the patient survived. Unfortunately, subsequent patients died because he used a newly invented valvulotome device that created significant regurgitation and he subsequently abandoned the surgery in 1929. Henry Souttar, in England, performed the first finger-guided transatrial mitral commissurotomy in 1925.2 It was not until 25 years after Cutler’s success, Dr Dwight Harken at Brigham and Women’s Hospital performed a large series of closed MVP beginning in 1948.3 Rheumatic disease was the main focus in this early era, which was most prevalent at the time.
After the invention of cardiopulmonary bypass in 1953 by Gibbon,4 Lillehei reported in 1956 multiple valve repairs through a right thoracotomy using cardiopulmonary bypass.5 Modern MVP for valve prolapse started in the 1950 s but met with fail-ure. McGoon reported his successful case of MVP for ruptured chordate in 1960.6 The concept of valve repair for myxomatous disease by Duran et al7 and Carpentier et al8 opened the new era for MVP, which has now become the standard of treatment for mitral regurgitation.
Minimally Invasive TechniqueFollowing the emergence of laparoscopic surgery, cardiac sur-gery started its era of minimally invasive surgery. Cohn et al9 and Navia and Cosgroove10 performed the first minimally in-vasive mitral valve operations through small incisions. They used a right parasternal and transsternal approach, respective-ly, and had excellent exposure with great procedural success. Carpentier et al performed the first video-assisted MVP in 199611
Received January 19, 2014; accepted January 20, 2014; released online February 4, 2014Division of Cardiac Surgery, Brigham and Women’s Hospital, Boston, MA, USAMailing address: Lawrence Cohn, MD, Division of Cardiac Surgery, Brigham and Women’s Hospital, 75 Francis St, Boston, MA 02115,
USA. E-mail: [email protected] doi: 10.1253/circj.CJ-14-0069All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Mitral Valve Repair– Evolution and Revolution 1923–2013 –
Tsuyoshi Kaneko, MD; Lawrence H Cohn, MD
Mitral valve repair is the gold standard treatment for mitral regurgitation. The history of mitral valve repair and its refinement in terms of the technique used will show the evolution of this surgical technique. The standard technique we use for mitral valve repair is described, and the outcomes we have observed over the past 4 decades are pre-sented. (Circ J 2014; 78: 560 – 566)
Key Words: Mitral valve; Mitral valve repair; Regurgitation
REVIEW
Circulation Journal Vol.78, March 2014
561Mitral Valve Repair – Evolution and Revolution –
Table. Indications for Mitral Valve Surgery17
Class I
1. MV surgery is recommended for the symptomatic patient with acute severe MR.
2. MV surgery is beneficial for patients with chronic severe MR and NYHA functional class II, III, or IV symptoms in the absence of severe LV dysfunction (severe LV dysfunction is defined as the ejection fraction less than 0.30) and/or an end-systolic dimension greater than 55 mm.
3. MV surgery is beneficial for asymptomatic patients with chronic severe MR and mild-to-moderate LV dysfunction, an ejection fraction of 0.30–0.60, and/or an end-systolic dimension greater than or equal to 40 mm.
4. MV repair is recommended over MV replacement in the majority of patients with severe chronic MR who require surgery, and patients should be referred to surgical centers experienced in MV repair.
Class IIa
1. MV repair is reasonable in experienced surgical centers for asymptomatic patients with chronic severe MR with preserved LV function (an ejection fraction greater than 0.60 and an end-systolic dimension less than 40 mm) in whom the likelihood of successful repair without residual MR is greater than 90%.
2. MV surgery is reasonable for asymptomatic patients with chronic severe MR, preserved LV function, and a new onset of atrial fibrillation.
3. MV surgery is reasonable for asymptomatic patients with chronic severe MR, preserved LV function, and pulmonary hypertension (pulmonary artery systolic pressure greater than 50 mmHg at rest or greater than 60 mmHg with exercise).
4. MV surgery is reasonable for patients with chronic severe MR due to a primary abnormality of the mitral apparatus and NYHA functional class III–IV symptoms and severe LV dysfunction (an ejection fraction less than 0.30 and/or an end-systolic dimension greater than 55 mm) in whom MV repair is highly likely.
Class IIb
MV repair might be considered for patients with chronic severe secondary MR due to severe LV dysfunction (an ejection fraction less than 0.30) who have persistent NYHA functional class III–IV symptoms despite optimal therapy for heart failure, including biventricular pacing.
Class III
1. MV surgery is not indicated for asymptomatic patients with MR and preserved LV function (an ejection fraction greater than 0.60 and an end-systolic dimension less than 40 mm) in whom there is significant doubt about the feasibility of repair exists.
2. Isolated MV surgery is not indicated for patients with mild or moderate MR.
LV, left ventricular; MR, mitral regurgitation; MV, mitral valve; NYHA, New York Heart Association.
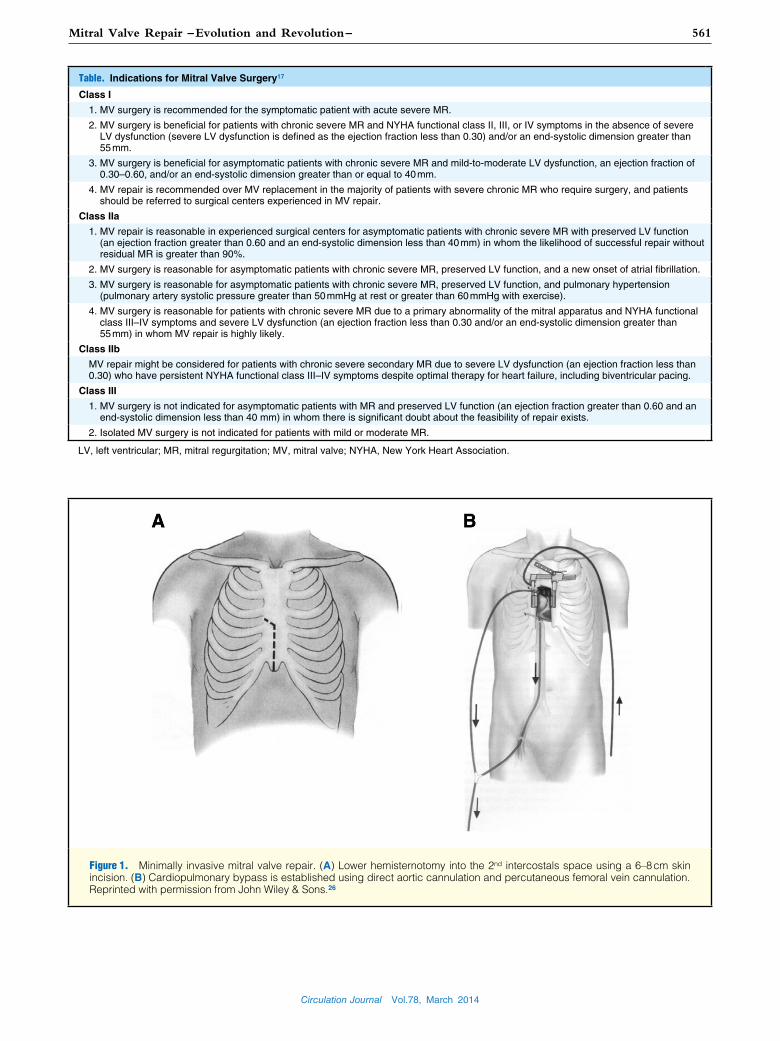
Figure 1. Minimally invasive mitral valve repair. (A) Lower hemisternotomy into the 2nd intercostals space using a 6–8 cm skin incision. (B) Cardiopulmonary bypass is established using direct aortic cannulation and percutaneous femoral vein cannulation. Reprinted with permission from John Wiley & Sons.26

Circulation Journal Vol.78, March 2014
562 KANEKO T et al.
repair. All these techniques are used in conjunction with a pros-thetic ring annuloplasty.
The most common etiology encountered is posterior leaflet prolapse from chordal rupture or elongated chordae. We use a quadrangular resection as a standard repair technique for rup-tured chords. Resection is performed in the limited area of pro-lapse (Figures 2A,B). The surgeon must pay attention not to cut the normal functioning chordae. We use a simplified tech-nique to avoid performing sliding plasty in all cases. Instead, we use what we call the “fold-over leaflet advancement” tech-nique. We use the leaflet edge that is “folded down” and sutured to the annulus (Figure 2C). After both sides of the leaflet are use to close the gap in the annulus (Figure 2D), the 2 leaflet edges are sutured from the edge of the leaflet to the annulus and tied (Figure 2E). This avoids further incision and additional suturing, and simplifies the operation. The key is to lower the height of the posterior leaflet to less than 1.5 cm to avoid sys-tolic anterior motion (SAM).
CommissuroplastyProlapse at the anterolateral or posteromedial commissure is another valve pathology frequently seen in mitral regurgitation. Commissuroplasty provides a simple and easy method to repair this etiology. Several (usually 2–3) polypropylene mattress su-tures are placed from anterior leaflet out to the posterior annu-lus. Tying these sutures will fix the prolapsed segment of leaf-lets. These areas rarely contribute to valve areas; hence, they do not cause mitral stenosis post procedure.
Artificial ChordaeThis technique was originally described in the early 1990 s,18 but has recently reemerged as one of the most frequently used strat-egies to manage both anterior and posterior leaflet prolapse.19 At the Brigham and Women’s Hospital, we use this technique
lines for MVP is listed in Table.17
There is a Class IIa recommendation for asymptomatic pa-tients. “MV repair is reasonable in experienced surgical centers for asymptomatic patients with chronic severe MR17 with pre-served LV function (ejection fraction greater than 0.60 and end-systolic dimension less than 40 mm) in whom the likelihood of successful repair without residual MR is greater than 90%.”
Following this guideline, at Brigham and Women’s Hospital (BWH), any patient with severe degenerative myxomatous MR is offered mitral valve repair regardless of their symptoms and ventricular function.
Technique of Mitral Valve Repair at BWHMinimally Invasive TechniqueMinimally invasive mitral valve repair has been offered at BWH since 1996. We use lower hemisternotomy using a 6–8 cm skin incision (Figure 1). For cardiopulmonary bypass, the aorta is cannulated directly in the field and the femoral vein is cannu-lated percutaneously into the right atrium (into the superior vena cava if needed) under TEE guidance for venous drainage. If the drainage is inadequate, the superior vena cava is cannulated di-rectly. This technique might not be feasible for obese or large anterior posterior diameter chest patients.
Following the establishment of cardiopulmonary bypass and aortic cross-clamp, antegrade and retrograde cardioplegia is given and the heart is arrested. For access to the mitral valve, we use a transatrial approach through Sondergaard’s groove. This dissection is performed both sharply and bluntly. It is un-usual to use any other approach, and this approach brings the mitral valve closer to the surgeon.
Quadrangular ResectionSeveral techniques described here are used in myxomatous valve
Figure 2. “Fold-over leaflet advancement” technique. (A and B) Quadrangular resection of the prolapsed leaflet. (C and D) The edge of the leaflet is “folded-over” to close the gap of the mitral annulus. (E) Two leaflet edges are closed. Reprinted with permis-sion from John Wiley & Sons.26

Circulation Journal Vol.78, March 2014
563Mitral Valve Repair – Evolution and Revolution –
rupture. We also confirm that the double-orifice created is at least 2 cm in diameter. This technique is useful in high SAM potential cases. The edge-to-edge suture will prevent the anterior leaflet from prolapsing into the left ventricular outflow tract. Our ex-perience with this technique has been excellent; no recurrence of mitral regurgitation was seen in our series during mid-term follow up and there was no mitral stenosis.22
FoldoplastyMcGoon first introduced a technique of mitral valve repair with-out valve resection.6 At BWH, we have used a modified tech-nique called “foldoplasty”. This avoids leaflet resection and is performed by placing 2 or 3× 4-0 polypropylene mattress su-tures from the leaflet edge to the annulus on the prolapsed or redundant portion of the posterior leaflet. These sutures are tied, creating a “fold over leaflet” to reduce the height of the posterior leaflet by at least half the length (Figure 4). The height of the leaflet is adjusted to less than 1.5 cm. This technique is typically used in conjunction with other techniques described here and always with a prosthetic annuloplasty ring. We reported over a 90% successful repair rate (less than that of trace regurgitation)
for anterior leaflet prolapse. The Leipzig group has an estab-lished technique to measure the height and use a premade loop as artificial chordae.20 We use the following method. A pled-geted polytetrafluoroethylene (PTFE) suture is placed to the papillary muscle. It is important to place the suture into the ten-don (white portion), otherwise the muscle will tear. This is sutured to the edge of the leaflet and tied down to the adjusted height. The height is determined by the position of the leaflet in the systole. We tent the posterior leaflet and use this as a guide when tying. The most important concept is to keep the coapta-tion plane between the anterior and posterior leaflet as long as possible.
Edge-to-Edge RepairThe edge-to-edge repair was first introduced by Alfieri et al.21 This technique apposes the anterior leaflet to the posterior leaf-let, and prevents the elevation of the anterior leaflet, therefore preventing regurgitation in severe anterior leaflet prolapse or bileaflet prolapse. An apposition suture is placed at the midpor-tion of the leaflet using a figure-of-8 suture (Figure 3). We use a braided polyester suture because the polypropylene sutures can
Figure 3. Edge-to-edge repair. A figure-of-8 suture is placed in the mid or lateral portion of the anterior and posterior leaflet to create a double orifice. Reprinted with permission from Oxford University Press.27
Figure 4. Foldoplasty. A mattress suture is placed from the leaflet edge to the annulus; the leaflet is “folded over” to decrease the height. Reprinted with permission from Elsevier.23
Circulation Journal Vol.78, March 2014
564 KANEKO T et al.
A ring annuloplasty was performed in 87% of the patients, but when analyzed by decade, only 6% of patients treated in the first decade received an annuloplasty ring. Following this, 92.6% received a ring annuloplasty. Concomitant procedures were per-formed in 40.5% of the patients. An excellent outcome was ob-tained and the overall operative mortality was only 1.3%.
Rheumatic DiseasePatients with rheumatic disease compared to patients with myxomatous disease and functional disease were younger (rheumatic vs. myxomatous vs. functional: 54±15 vs. 59±13 vs. 69±10 years, respectively), and had more preserved left ven-tricular ejection fraction (58±10 vs. 61±9 vs. 43±13). Repair was mainly performed using unilateral or bilateral commissur-otomy with occasional extension to the subvalvar apparatus. Only 34.6% were treated with a ring annuloplasty.
Myxomatous DiseaseAs mentioned earlier, patients with myxomatous disease were older and had better preserved LV ejection fraction compared to patients with functional disease. A total of 97 different tech-niques were used for leaflet repair, which shows that there is no single surgical technique for mitral valve repair. Posterior leaf-
during mid-term follow up.23
Annuloplasty RingsAnnuloplasty rings are placed following every valve repair. It is important to emphasize that the ring size rather than ring type is the key for myxomatous mitral regurgitation. We typically mea-sure the ring size using the anterior leaflet height and use a par-tial soft ring. Undersizing will cause SAM and therefore must be avoided in myxomatous disease.
In contrast, for functional disease, downsizing the ring is cru-cial because the etiology of mitral valve regurgitation is from annular dilatation. As both leaflets are tethered, the risk of SAM is extremely low and allows the placement of a smaller size ring.
Experience of 3 Different Diseases at BWHOver 1,500 mitral valve repairs have been performed by a single surgeon (LHC) at PBBH/BWH, beginning in 1972.24 Overall, the mean patient age was 60.3 years, and the etiologies were rheumatic in 12.8%, myxomatous in 69.3%, and isch-emic functional in 15.7%. A minimally invasive technique using lower hemisternotomy was performed in 33% of the patients.
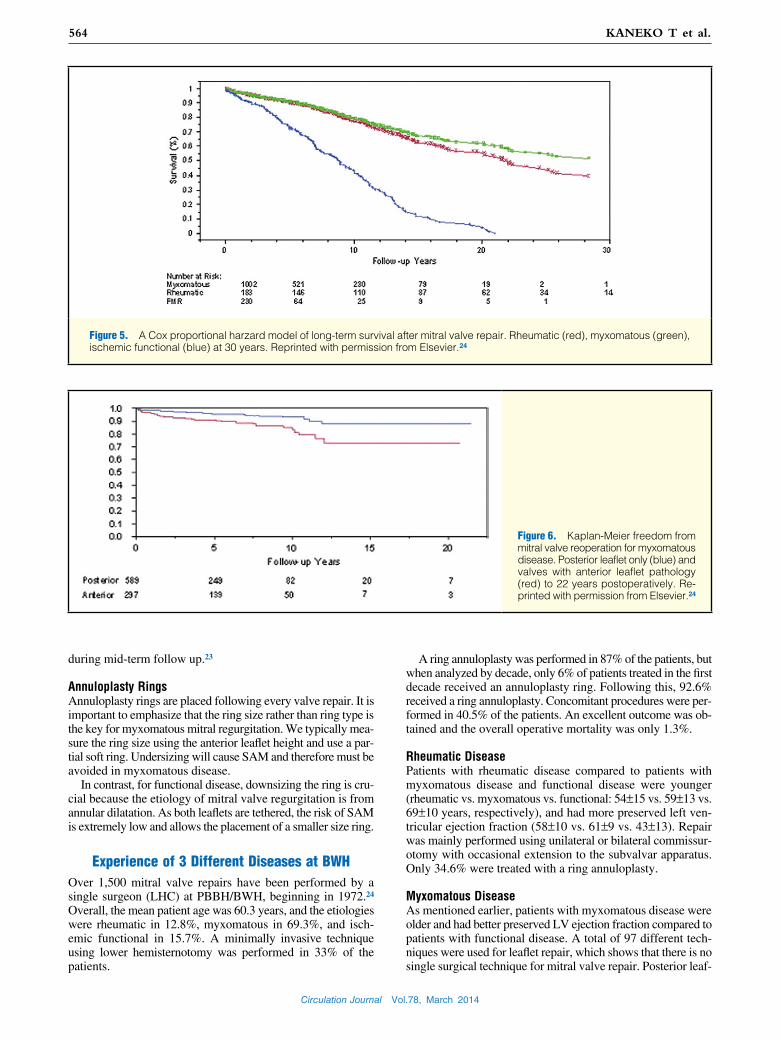
Figure 5. A Cox proportional harzard model of long-term survival after mitral valve repair. Rheumatic (red), myxomatous (green), ischemic functional (blue) at 30 years. Reprinted with permission from Elsevier.24
Figure 6. Kaplan-Meier freedom from mitral valve reoperation for myxomatous disease. Posterior leaflet only (blue) and valves with anterior leaflet pathology (red) to 22 years postoperatively. Re-printed with permission from Elsevier.24

Circulation Journal Vol.78, March 2014
565Mitral Valve Repair – Evolution and Revolution –
decrease the dimension. However, for reasons such as coronary sinus being far away from the mitral annulus, coronary sinus only covers half of the annulus and possible coronary artery compression has limited the use of these devices. A direct cinch-ing method of annuloplasty is currently being studied.
In 2013, United States Food and Drug Administration ap-proved The MitraClip for patients with myxomatous MR that are at high risk for traditional surgery.28 Currently, randomized control studies using The MitraClip for functional MR are being conducted.
ConclusionMitral valve repair has evolved as the gold standard for treatment of mitral regurgitation. The excellent early- and long-term out-comes and freedom from re-operation is obtained using stan-dardized mitral valve repair techniques. Recognition of valve pathology and combining multiple strategies are the key to suc-cessful valve repair. The future application of the percutaneous approach is uncertain at this point. Given the high success rate and low morbidity and mortality, especially for the degenerative disease, surgical mitral repair will remain the gold standard for treatment of MR for some time.
DisclosuresWe, as the authors of the manuscript, do not have a direct financial relation that might lead to a conflict of interest.
References 1. Cutler EC, Levine SA. Cardiotomy and valvulotomy for mitral steno-
sis. Boston Med Surg J 1923; 188: 1023 – 1027. 2. Souttar HS. Surgical treatment of mitral stenosis. BMJ 1925; 2: 603 –
606. 3. Harken DE, Ellis LB, Ware PF, Norman LR. The surgical treatment
of mitral stenosis. N Engl J Med 1948; 239: 801 – 809. 4. Gibbon JH Jr. Application of a mechanical heart and lung apparatus
to cardiac surgery. Minn Med 1954; 37: 171 – 185. 5. Lillehei CW, Gott VL, Dewall RA, Varco RL. The surgical treatment
of stenotic and regurgitant lesions of the mitral and aortic valves by direct utilization of a pump oxygenator. J Thorac Surg 1958; 35: 154 – 191.
6. McGoon DC. Repair of mitral insufficiency due to ruptured chordae tendinae. J Thorac Cardiovasc Surg 1960; 39: 357 – 362.
7. Duran CG, Pomar JL, Revuelta JM, Gallo I, Poveda J, Ochoteco A, et al. Conservative operation for mitral insufficiency. Critical analysis supported by postoperative hemodynamic studies of 72 patients. J Thorac Cardiovasc Surg 1980; 79: 326 – 337.
8. Carpentier A. Deloche A. Dauptain J, Soyer R, Blondeau P, Piwnica A, et al. A new reconstructive operation for correction of mitral and tricuspid insufficiency. J Thorac Cardiovasc Surg 1971; 61: 1 – 13.
9. Cohn LH, Adams DH, Couper GS, Bichell DP, Rosborough DM, Sears SP, et al. Minimally invasive cardiac valve surgery improves patient satisfaction while reducing costs of cardiac valve replacement and repair. Ann Surg 1997; 4: 421 – 428.
10. Navia JL, Cosgrove DM. Minimally invasive mitral valve operations. Ann Thorac Surg 1996; 62: 1542 – 1544.
11. Carpentier A, Loulmet D, Carpentier A, Le Bret E, Haugades B, Dassier P, et al. [Open heart operation under video surgery and mini-thoracotomy. First case (mitralvalvuloplasty) operated with success]. C R Acad Sci III 1996; 319: 219 – 223 (n French).
12. Chitwood WR Jr, Elbeery JR, Moran JF. Minimally invasive mitral valve repair: Using a minithoracotomy and transthoracic aortic occlu-sion. Ann Thorac Surg 1997; 63: 1477 – 1479.
13. Lawrie GM. Mitral valve repair vs. replacement: Current recommen-dations and long-term results. Cardiol Clin 1998; 16: 437 – 448.
14. Ling LH, Enriquez-Sarano M, Seward JB, Tajik AJ, Schaff HV, Bailey KR, et al. Clinical outcome of mitral regurgitation due to flail leaflet. N Engl J Med 1996; 335: 1417 – 1423.
15. McClure RS, Cohn LH, Wiegerinck E, Couper GS, Aranki SF, Bolman RM 3rd, et al. Early and late outcomes in minimally invasive mitral valve repair: An eleven-year experience in 707. J Thorac Cardiovasc Surg 2009; 137: 70 – 75.
16. Gammie JS, Sheng S, Griffith BP, Peterson ED, Rankin JS, O’Brien
let resection and commissuroplasty was used most frequently (63% in total), followed by edge-to-edge repair (4%), foldo-plasty (4%). For patients with bileaflet disease, 48% required posterior leaflet repair only and did not require any anterior leaflet repair, and 23% were treated using edge-to-edge repair. Only 25% required a combined anterior and posterior leaflet repair.
Functional DiseaseThe first repair for ischemic functional mitral disease was per-formed in 1981, and since then, 230 patients have undergone mitral repair for functional MR. This patient group was older and had more cardiac dysfunction. Although partial rings were used in the earlier series, recent patients were all repaired using a total circumferential ring annuloplasty, with an undersized rigid ring. Seventy-seven percent of patients had concomitant procedures, mainly coronary artery bypass surgery.
Short-Term and Long-Term Outcome Following Mitral Valve RepairA 30-day mortality was significantly higher in patients with functional disease (patients with rheumatic disease, 0.5%; pa-tients with myxomatous disease, 0.6%; patients with functional disease, 4.7%; P<0.0001 vs. myxomatous disease and P=0.01 vs. rheumatic disease). Long-term survival was significantly worse in patients with ischemic functional disease. The 10-, 20-, and 30-year survivals were 77%, 56%, and 39%, respectively, in patients with rheumatic disease, 79%, 62%, and 52% in patients with myxomatous disease, and 44%,4%, and 0% (P<0.0001) in patients with ischemic functional disease (Figure 5). The re-operation rate was higher in patients with rheumatic disease compared to those with myxomatous disease; freedom from mitral valve re-operation within 10 and 20 years were 66% and 34% in patients with rheumatic disease, respectively, and 90% and 82% in patients with myxomatous disease, respectively (P<0.0001). The 10-year freedom rate from re-operation for patients with functional ischemic disease was 63%.
When the freedom of re-operation rate was compared be-tween posterior leaflet only vs. anterior leaflet involvement, the 10- and 20-year freedom rate was higher for posterior leaflet only (Figure 6: 93% and 88% vs. 84% and 74%, respectively; P=0.0008).
Percutaneous TechniqueFollowing the success of transcatheter aortic valve replacement, percutaneous approaches for mitral valve disease have been explored. All percutaneous technologies have been developed based on surgical repair techniques.
Perhaps the most studied technique is the MitraClip (Abbott Vascular, Santa Clara, California) system. This replicates edge-to-edge repair by delivering a clip via a transseptal approach. The EVEREST II trial was a randomized control study for symp-tomatic severe MR and asymptomatic severe MR with LV dys-function and compared The MitraClip technique vs. surgical repair. This trial showed non-inferiority of The MitraClip, even in the 4-year follow up. However, The MitraClip was associated with a higher re-operation rate (24.8% vs. 5.5%; P<0.001).25 A Mobius device (Edwards Life Sciences, Irving, California) uses sutures to create edge-to-edge repair and MitraFlex (TransCardiac Therapeutics, Atlanta, Georgia) allows placement of a clip via a tranapical approach and also allows placement of artificial chordate.
Multiple devices have been used to recreate the surgical ring annuloplasty by inserting these devices in the coronary sinus to

Circulation Journal Vol.78, March 2014
566 KANEKO T et al.
22. Brinster DR, Unic D, D’Ambra MN, Nathan N, Cohn LH. Midterm results of the edge-to-edge technique for complex mitral repair. Ann Thorac Surg 2006; 81: 1612 – 1617.
23. Tabata M, Ghanta RK, Shekar PS, Cohn LH. Early and midterm outcomes of folding valvuloplasty without leaflet resection for myxo-matous mitral valve disease. Ann Thorac Surg 2008; 86: 1388 – 1390.
24. DiBardino DJ, Elbardissi AW, McClure RS, Razo-Vasquez OA, Kelly NE, Cohn LH. Four decades of experience with mitral valve repair: Analysis of differential indications, technical evolution, and long-term outcome. J Thoracic Cardiovasc Surg 2010; 139: 76 – 83, dis-cussion 83 – 84.
25. Mauri L, Foster E, Glower DD, Apruzzese P, Massaro JM, Herrmann HC, et al. 4-year results of a randomized controlled trial of percuta-neous repair versus surgery for mitral regurgitation. J Am Coll Car-diol 2013; 62: 317 – 328.
26. Cohn LH. Minimally invasive valve surgery. J Card Surg 2001; 16: 260 – 265.
27. Maisano F, Torracca L, Oppizzi M, Stefano PL, D’Addario G, La Canna G, et al. The edge-to-edge technique: A simplified method to correct mitral insufficiency. Eur J Cardiothorac Surg 1998; 13: 240 – 245.
28. http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm375149.htm.
SM, et al. Trends in mitral valve surgery in the United States: Results from the Society of Thoracic Surgeons Adult Cardiac Surgery Data-base. Ann Thorac Surg 2009; 87: 1431 – 1437.
17. Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD, et al. ACC/AHA 2006 Guidelines for the Management of Patients With Valvular Heart Disease. Circulation 2006; 114: e84 – e231, doi:10.1161/CIRCULATIONAHA.106.176857.
18. Zussa C, Polesel E, Da Col U, Galloni M, Valfré C. Seven-year ex-perience with chordal replacement with expanded polytetrafluoroeth-ylene in floppy mitral valve. J Thorac Cardiovasc Surg 1991; 108: 37 – 41.
19. Falk V, Seeburger J, Czesla M, Borger MA, Willige J, Kuntze T, et al. How does the use of polytetrafluoroethylene neochordae for posterior mitral valve prolapse (loop technique) compare with leaflet resection? A prospective randomized trial. J Thorac Cardiovasc Surg 2008; 136: 1205 – 1206.
20. Kuntze T, Borger MA, Falk V, Seeburger J, Girdauskas E, Doll N, et al. Early and mid-term results of mitral valve repair using premea-sured Gore-Tex loops (‘loop technique’). Eur J Cardiothorac Surg 2008; 33: 566 – 572.
21. Alfieri O, Maisano F, De Bonis M, Stefano PL, Torracca L, Oppizzi M, et al. The double-orifice technique in mitral valve repair: A simple solution for complex problems. J Thorac Cardiovasc Surg 2001; 122: 674 – 681.