mitral regurgitation - basic echo regurgitation.pdf · mitral valve prolapse > 2mm systolic...
TRANSCRIPT

MITRAL REGURGITATION
Joanne Cusack

BSE Breakdown
Assessment of severity by:
Chamber sizes and volume overload CW Doppler – shape and density of contour of Doppler signal Vena contracta
PISA and effective regurgitant orifice area
Size of colour jet relative to atrial size by colour flow Doppler Regurgitant fraction, regurgitant volume
Pulmonary vein flow patterns
Indirect effects on LV and LA
Role of echocardiography in determining timing of surgery for primary mitral valve disease: ejection fraction, end-systolic LV diameter, EROA
Role of TOE in assessing mitral valve pathology and in determining likelihood of repair as opposed to replacement

Role of echo
Determine the cause
Assess the severity
Comment on any secondary effects

Causes of MR
Rheumatic
Mitral valve prolapse
Endocarditis
Congenital
Functional

Rheumatic

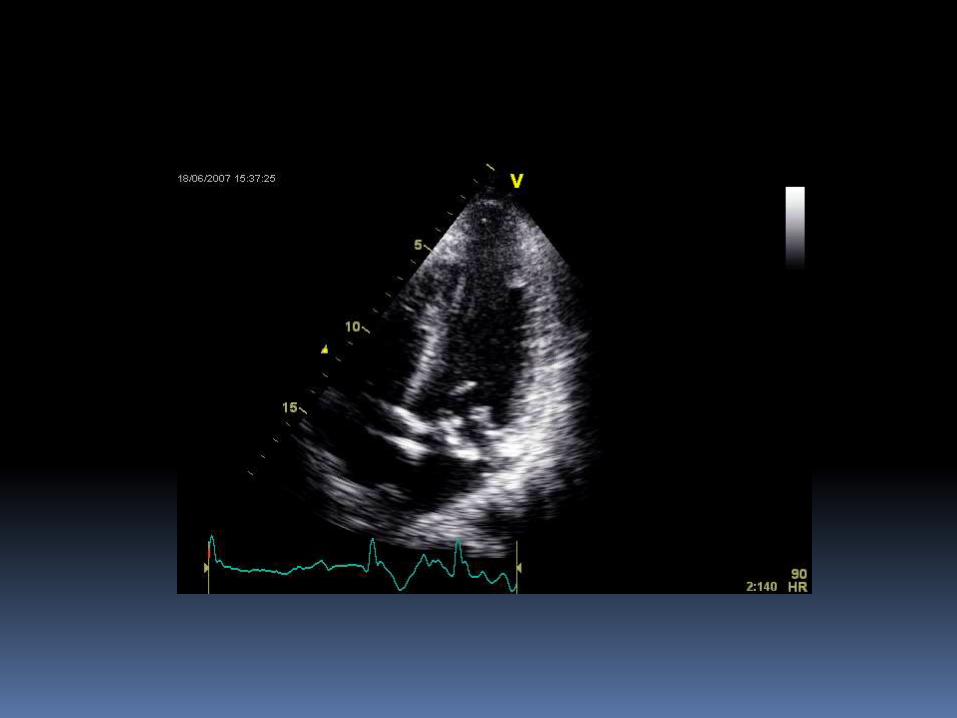
Mitral valve prolapse
> 2mm systolic displacement of one or both mitral valve leaflets into the left atrium, below the plane of the mitral annulus
Diagnosis more certain when the leaflets are thickened (> 5mm) or myxomatous
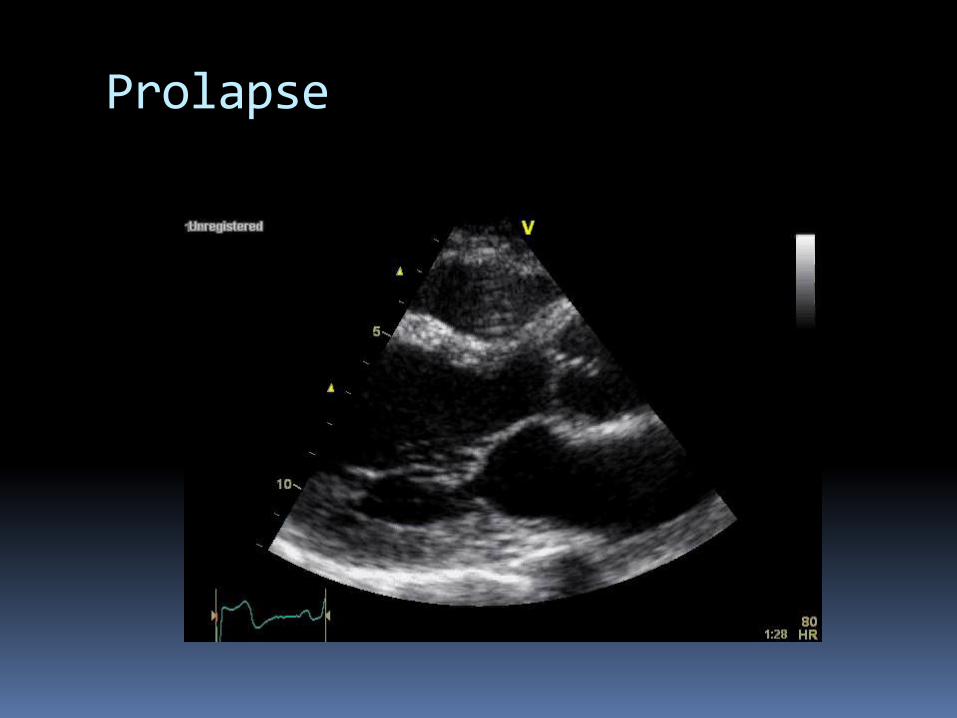
Prolapse





Associations
Increased risk of endocarditis
Severe MR
Mitral valve repair or replacement
Congenital
Isolated mitral valve defects - Mitral valve clefts, fenestrations or perforations, double orifice mitral valve, abnormal chordal tissue or insertion, absent or hypoplastic leaflets, accessory leaflets
Associated with other congenital heart defects - Atrioventricular septal defect, Transposition of the great arteries, anomalous origin of the left coronary artery


Functional MR
Caused by regional or global left ventricular remodelling without structural abnormalities of the valve
Usually central in origin


Measurements
Vena contracta
Mitral regurgitant volume
Regurgitant fraction
Effective regurgitant orifice area (EROA)
Proximal isovelocity surface area (PISA)

Vena contracta
Forms immediately distal to the regurgitant orifice with the smallest cross sectional area of regurgitant jet
Represents the physiologic or effective orifice area

Measuring the vena contracta width Optimise colour flow of the regurgitant jet
Zoom into the region of interest
Acquire a loop
Measure the smallest width immediately distal to the regurgitant orifice, perpendicular to the direction of the jet
Severe ≥ 7mm



Mitral regurgitant volume, regurgitant fraction and EROA

Mitral regurgitant volume
The difference between the flow across the mitral valve and the LVOT
MV RegV = MV flow – LVOT flow
MV flow is the product of the diameter of the mitral annulus
and the TVI through the mitral valve
LVOT flow is the product of the diameter of the aortic
annulus and the TVI through the aortic valve

Regurgitant fraction
The percentage of the LV stroke volume that regurgitates into the left atrium
MR RF = (MV RegV/MV flow) X 100

Effective regurgitant orifice area EROA The area of the regurgitant flow at the level
of the valve
EROA = MV RegV / MR TVI

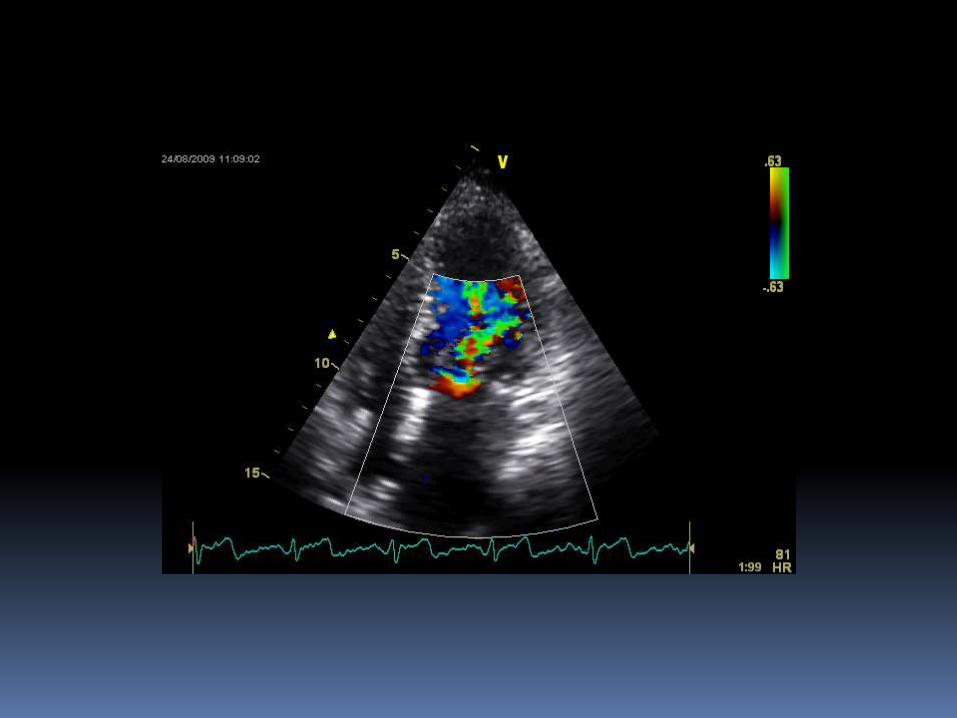
Size of colour jet relative to atrial size by colour flow
When the area of the regurgitant jet is more than 40% of the LA or reaches the posterior wall of the LA, MR is usually severe
CW Doppler shape and density
In severe MR, flow is dense and triangular
Proximal Isovelocity Surface Area (PISA) Based on the haemodynamic principles of flow
through a small circular orifice in a flat plate
There is flow acceleration just proximal to the orifice
The flow converges on the orifice in hemispheric layers of equal velocity
Colour flow Doppler can be used to calculate the area of the hemisphere
This can be used to calculate the EROA


PISA method
Optimise colour flow imaging of mitral regurgitation from apical window
Zoom in on area of interest
Capture a loop and select the most satisfactory hemispheric PISA, which occurs at mid-systole
Measure the radius (r in cm) along the direction of the ultrasound beam


PISA (cont’d)
Measure the MR velocity with CW Doppler to obtain peak MR velocity (cm/s) and TVI (cm)
EROA = 6.28R2 X Alias V / MR V

PISA through machine
Freeze of PISA and measure r
Freeze of MR Doppler trace and measure VTI
Machine calculates EROA and MR volume


Pulmonary vein flow patterns
Systolic flow reversal suggests severe MR

Indirect effects on LV and LA Enlargement of both is common in chronic
significant MR. May be normal in acute setting

Role of TOE
Used to determine cause and severity
Better images required compared to TTE



…CLICKER TIME…