mist ultrasound healing of wounds - flvc27376... · 4 mist ultrasound healing of wounds mist...
TRANSCRIPT

MIST ULTRASOUND HEALING OF WOUNDS
USING MIST ULTASOUND TO ACCELERATE THE HEALING OF WOUNDS AND DEEP
TISSUE INJURIES: A CASE–STUDY
___________________________________________________________________________
A Case-Study
Presented to
The Faculty of the College of Health Professions
Florida Gulf Coast University
In Partial Fulfillment
of the Requirement for the Degree of
Transition Doctorate of Physical Therapy
___________________________________________________________________________
By
Justin Bovee, MSPT
2015

MIST ULTRASOUND HEALING OF WOUNDS
APPROVAL SHEET
This care report is submitted in partial fulfillment of the requirements of the degree of
Transitional Doctor of Physical Therapy (tDPT)
________________________________
Justin Bovee, MSPT
Approved: April, 2015
__________________________________
Rose M. Pignataro, PT, PhD, DPT, CWS
Committee chair/Advisor
The final copy of this case report has been examined by the signatories, and we find that both the content and the form meet acceptable presentation standards of scholarly work in the above mentioned discipline.

MIST ULTRASOUND HEALING OF WOUNDS
ACKNOWLEDGEMENTS
I would like to thank my advisor Dr. Rose Pignataro for providing the assistance,
expertise, and wisdom I needed to complete this scholarly paper. A special thank you goes to all
hospital staff at Lehigh Regional Medical Center for allowing me to utilize my skills in their
facility in order to complete this dissertation.

1
MIST ULTRASOUND HEALING OF WOUNDS
TABLE OF CONTENTS
Abstract 2
Introduction 3
Methods 7
Results 14
Discussion 19
References 22

2
MIST ULTRASOUND HEALING OF WOUNDS
ABSTRACT
OBJECTIVES: This case report examines the effectiveness of Mist Ultrasound Healing
Therapy® by Celleration, Inc. (Eden Prairie, MN) in promoting wound healing and selective
debridement for a deep tissue injury. The patient in this report is an 81 year old male presenting
with a necrotic deep tissue injury.
METHODS: This patient received Mist ultrasound, a non-contact, low frequency ultrasound (25
to 40 kHz) delivered to the wound bed via fine saline spray, while monitoring for signs of
healing. This intervention was given once daily for four consecutive days in the acute setting.
The treatment was discontinued due to the patient’s discharge to a skilled nursing facility for
short-term rehab. The Mist Therapy® was predicted to assist healing by reducing the area of
eschar in the patient’s wound and reducing the entire area of the wound bed. Additionally, greater
amounts of healing tissue or epithelialization would be supplanted. The wound is photographed
and measured daily before each treatment to help confirm that healing of the wound is taking
place.
RESULTS: The patient’s total wound area decreased from 14.06cm2 to 9.52cm2 and the area of
necrosis decreased from 1.0cm2 to 0.54cm2 after receiving Mist ultrasound.
DISCUSSION: Mist ultrasound shows promise toward achieving notable healing of deep tissue
injuries. The findings in this case report warrant further investigation of the effects of Mist
Therapy® on deep tissue injuries and other wound types.
3
MIST ULTRASOUND HEALING OF WOUNDS
INTRODUCTION
Chronic wounds are sometimes called non-healing wounds. The rate of healing of these
wounds is not met within the anticipated time frame based on normal physiological processes.
According to Enoch & Leaper, full-thickness wounds are reduced up to 5-10% of its original size
in six weeks by contraction of a wound under normal physiological conditions1. Contraction and
epithelialization are secondary healing processes. However, some wounds are much slower to
heal. Months or even years may pass while persistent, non-healing wounds significantly impact a
person’s quality of life.2 Prognosis for healing is usually poor due to the long duration of the
wound. A wound that fails to respond to treatment during the first 2-4 weeks is also predicted to
have a poor healing prognosis.3 Chronic wound may be associated with diabetes, vascular
insufficiencies or ischemia, and deep tissue injuries. Chronic wounds are prevalent and difficult
to heal with increases health care costs to the patient. For instance, the most common cause of leg
ulcers in the Unites States is venous insufficiency. With these wounds, the standard of care does
not provide healing rates higher than 70%. Billions of dollars annually spent are spent in health
care cost for venous insufficiency ulcers alone.4 Nearly 15% of diabetic patients with develop a
foot ulcer in their lifetime; some of which do not heal.3 This makes them 30 to 40 times more at
risk of an amputation compared to non-diabetic patients.3,5 According to the manufacturer of the
Mist Therapy System, patients with persistent chronic wounds of various etiologies can benefit
from the accelerated healing this new modality provides.2 In general ultrasound has been widely
used for diagnostic and therapeutic purposes. It is the process of using mechanical energy in the
form of a sound or pressure wave at certain frequencies to provide these effects. Mist ultrasound
is a new and unique modality used for the treatment of wounds. The Mist Therapy® System from
Celleration®, Inc. is a non-contract and non-thermal ultrasound delivered through normal saline
solution as the medium. It is the only low-frequency ultrasonic modality approved by the FDA
for the purpose of treating wounds. It works by debriding the wound bed of devitalized tissue,
stimulating healthy cell growth and promoting angiogenesis, and removing bacteria.2,3
4
MIST ULTRASOUND HEALING OF WOUNDS
Mist ultrasound uses a much lower frequency (25 kHz to 40 kHz) for debridement and
wound healing.6 This frequency is 40-75 times lower. It is still inaudible to the human ear
because it is outside the range of 20 Hz to 20 kHz.6 Intensity levels are also lower during MIST
ultrasound (0.1–0.8 W/cm2).4,7 These studies demonstrate that ultrasound shows promise for
wound healing but further investigation of the effectiveness Mist ultrasound is needed.
According to the manufacturer, the frequency and intensity of the sound waves from Mist
ultrasound are low enough that healthy cells and granulating tissue are undamaged. The sound
waves provide the energy to stimulate healthy growth from these cells while at the same time, kill
bacterial cells by targeting and fracturing the cell membrane. Bacterial cells are more susceptible
to micromechanical stress.2 Mist ultrasound’s impact on wound healing has been investigated via
the mechanism known as acoustical cavitation.3 This refers to the formation and oscillation of
microscopic bubbles that resonate with the frequency of the sound field. Acoustic energy is
concentrated in these bubbles causing cellular changes within the affected tissue.3 Moreover, this
effect is combined with microstreaming, which is the mechanism of sound waves that displace
ions and small molecules. Together, these processes can alter cell membrane activity.3,4
Changes in the synthesis and release of proteins within cells will occur along with increased
blood flow, vascular permeability, angiogenesis, and collagen formation and alignment.8
Although the benefits of ultrasound have been studied for nearly 50 years, Mist
ultrasound is a relatively new modality.5 In 2004, Thawer found a significant increase of blood
vessels and collagen formation in the granulation tissue of mice with experimental diabetes
mellitus after receiving ultrasound through a mist of saline solution.9 Similarly, Demir et al found
that ultrasound and laser treatment were both effective in promoting wound healing in
experimental lab rats. The laser treatment was provided via 904 nm wavelength, at 6 mW average
power, one Jcm2 dosage, 16 Hz frequency for a duration of 10 minutes.10 The ultrasound was
non-continuous and provided within a frequency range of 1 MHz to 3 MHz and at an intensity of
0.5 W/cm3. The ultrasound used in this study was not as effective as the laser treatment. The

5
MIST ULTRASOUND HEALING OF WOUNDS
authors claimed this is due to the lack of thermal effects that provide the healing benefits in the
ultrasound, which were present in laser therapy.10 However, major differences between their use
of ultrasound and Mist ultrasound are noted. Firstly, Sterile Sonogel was used as a medium
instead of saline solution. Also, the frequency used in this study resembled that of traditional
ultrasound used such as in outpatient physical therapy clinics typically used to reduce pain and
inflammation (1 MHz to 3MHz).
Mist ultrasound has intrigued investigators to determine its effectiveness against a variety
of wound-related etiologies. Much of the more recent available literature investigates the effect of
Mist ultrasound on chronic wounds, diabetic foot ulcers, and vascular insufficiency ulcers. Some
researchers have used Mist Therapy as a stand-alone treatment and as a synergistic treatment to
investigate its effectiveness against chronic wounds of various etiologies.3,4 Although one study
was not a randomized control trial, both studies found that Mist ultrasound can be used as a stand-
alone intervention or in combination with other interventions. These studies emulate a similar
spectrum of cases that are seen in most wound care centers and represent a similar scope of
wound care practice that is applicable to a realistic clinical setting.3 However, authors will still
argue that there are a small number of studies that support the use Mist Ultrasound therapy for
treating wounds.
As stated before, chronic wounds have a poor prognosis for healing. Stand-alone
treatment methods may still be utilized, but wound healing may be expedited when used in
conjunction with Mist ultrasound. Most modalities in physical therapy are utilized as part of a
comprehensive program. This is also true in wound care and in the use of Mist Therapy where
there are multiple components of such as debridement types, topical agents, dressings, etc. that
work collectively within a patients wound-healing program. An observational study of a larger
sample size than the study by Ennis and colleagues also found that Mist ultrasound used in
combination with stand alone wound care promotes better wound healing in chronic wounds than

6
MIST ULTRASOUND HEALING OF WOUNDS
standard wound care alone.5 The chronic wounds were also of various etiologies. Aside from
wound healing, Mist ultrasound is claimed to debride chronic wounds. However, there is not
sufficient evidence in the literature that Mist Therapy effectively debrides necrotic tissue from
wounds.6
Another small study examined the effect that non-contact ultrasound had on wound
closure, pain reduction, inflammation, and bacterial count of ten venous ulcers. A significant
reduction in wound area was found. There was an associated reduction of bacteria and cytokine
levels after receiving non-contact ultrasound, which supported the clinical use of Mist
ultrasound.11 Although the authors of this study credit the reduction of the wound area as
statistically significant after receiving Mist ultrasound, they explain that the reduction in bacteria
noted was not statistically significant.11
Other slow healing wounds are diabetes-related ulcers. Patients with diabetic ulcers are
30-40 times more likely to have an amputation than non-diabetic patients presenting with an
ulcer.3,8 A randomized, double-blind study was conducted in the hospital setting to determine the
safety and efficacy of Mist ultrasound for healing of diabetic foot ulcers and evaluate its effect on
wound closure and reduction of bacterial cultures. Ultrasound therapy significantly accelerated
healing times in recalcitrant diabetic foot wounds.8 The positive results found in this study
support Mist ultrasound as a safe and effective modality for accelerating healing in chronic
diabetic wounds.
Evidence is beginning to surface that MIST ultrasound is effective in treating wounds of
a variety of etiologies. Given the relatively small number of studies showing sufficient clinical
evidence and the scarcity of practice-based research in this area, there is a need for further study
regarding the application of the modality in direct patient care. Therefore, this case report will
examine the effectiveness of Mist ultrasound with normal saline solution in selective debridement
and/or acceleration of wound healing and granulation for partial thickness wounds, full thickness

7
MIST ULTRASOUND HEALING OF WOUNDS
wounds, and deep tissue injuries. This study would focus on the development of a relatively new
and uncommon intervention that will deal with a persistent clinical problem among patients.
The patient in this study is an 81-year-old male admitted to the hospital for shortness of
breath. The patient presents with an unstageable and necrotic wound to the left hip over the
greater trochanter. Other findings upon the initial evaluation show that the patient exhibits several
factors increasing risk of delayed wound closure: he is mildly undernourished, confused with
dementia, and presents with general weakness with limited ability to transfer and ambulate.
Subjective findings include that the patient admits to sleeping on his left side a lot. The patient
also presents with a stage one pressure sore on the right medial knee. These findings suggest that
the patient’s wound on the left hip is the result of a deep tissue injury or pressure ulcer. In light of
his clinical presentation and presence of risk factors associated with delayed healing, this patient
is an excellent candidate for use of Mist Therapy®.
METHODS
Mist Therapy®, sometimes referred to Mist Ultrasound or non-contract ultrasound, is a
painless low frequency ultrasound delivered through normal saline solution as a mist to the
wound bed.7 The sound waves produced by this modality stimulate collagen and growth factor
production, leukocyte adhesion, and increase macrophage responsiveness to accelerate healing.7,8
Mist Therapy® is claimed to remove barriers to healing such as removing a wide-range of
bacteria, disrupt biofilm, reduce sustained inflammation, and reduce matrix metallopeptidase
(MMP-9).7 To stimulate cells to promote healing, Mist Therapy® increases blood flow through
vasodilation, increases angiogenesis, releases growth factors, and increases collagen deposition.7
These benefits are summarized in Table 1.
8
MIST ULTRASOUND HEALING OF WOUNDS
Table 1. Summary of physiological effects as claimed by Mist Ultrasound Healing
Therapy® by Celleration, Inc. (Eden Prairie, MN)
Factors Impairing Healing Impact of MIST Therapy®
Impaired angiogenesis Stimulates angiogenesis
Deficient growth factors Causes upregulation of KGF, TGF-b1
Cellular Senescence Activates ERK and c-Jun n – Kinase
Bacterial bioburden Removes biofilm
Bacterial infection Decreases bacteria (VRE, MRSA,
Pseudomonas
Pain Modulates pain
The Mist Therapy® product consists of the ultrasound generator, which creates sound
waves that are sent from the transducer tip to the wound bed. The transducer is also called “the
wand” which is held near the wound bed. The metal tip of the transducer vibrates over 40,000
times per second to produce sound waves at 25,000Hz to 40,000Hz without direct contact.7 The
applicator is a disposable piece of plastic that fits over the transducer. It holds and punctures the
saline bottle, which is congruently fit. The saline becomes the conduit for the sound waves to the
sound bed. The saline and applicator must be discarded after each treatment for infection control.
They are single use only. Table 2 explains in detail how the Mist Therapy® system is applied.
Contraindications to use of the Mist Therapy® system are summarized in Table 3.
9
MIST ULTRASOUND HEALING OF WOUNDS
Figure 1: Mist Ultrasound Healing Therapy® by Celleration, Inc. (Eden Prairie, MN) Photo of
generator and transducer from http://misttherapy.com retrieved April 15, 2015
Figure 2. Mist Ultrasound Healing Therapy® by Celleration, Inc. (Eden Prairie, MN) Photo of
application, saline bottle, and Super Sani-Cloths from http://misttherapy.com retrieved April 15,
2015

10
MIST ULTRASOUND HEALING OF WOUNDS
Table 2. Application MIST Therapy®
1. Clinicians hands and transducer are
cleansed.
Hand hygiene and disinfecting the
transducer, cable, and entire generator
unit is required for infection control.
2. Machine is plugged in and turned on -
3. Infection control personal protective
equipment
Clean gloves, gown, hair net, and face
shield are donned prior to application.
4. Indicate wound size Wound area (cm2) is selected on
generator. The generator calculates the
duration of treatment based on the
selected area.
The disposable absorbent pad provided
in the Mist Therapy® Kit beneath
wound to collect saline and wound
exudate.
5. Applicator cup is attached The applicator is attached to the
transducer until an audible ‘click’ is
heard. The bottle of saline provided in
the kit is inserted into the applicator to
allow a puncture into bottom of the
saline bottle. The bottle and the
applicator are turned 90 degrees
counter-clockwise to align the
applicator opening.
6. Vent opened The cap of the saline bottle is twisted
off.
7. Positioning of the transducer tip The transducer tip is perpendicular to
the wound and 0.5 to 1.5 cm away
while ultrasound is being delivered
through the saline medium. Slow
circular motions over the wound bed
are employed until treatment is over.
The generator will automatically stop
when the given treatment is over.
8. Machine is turned off The applicator is turned 90 degrees
clockwise to stop the saline flow. The
applicator and saline bottle and
discard. The entire Mist ultrasound
unit is cleansed.

11
MIST ULTRASOUND HEALING OF WOUNDS
Table 3. Contraindications to using MIST Therapy®
Usage over electronic implants or prostheses (i.e.: pacemaker). The ultrasound may
disrupt the function of these devices
Usage over the lower back or uterus of a pregnant patient.
Usage over areas of malignancy, which may stimulate cell growth.
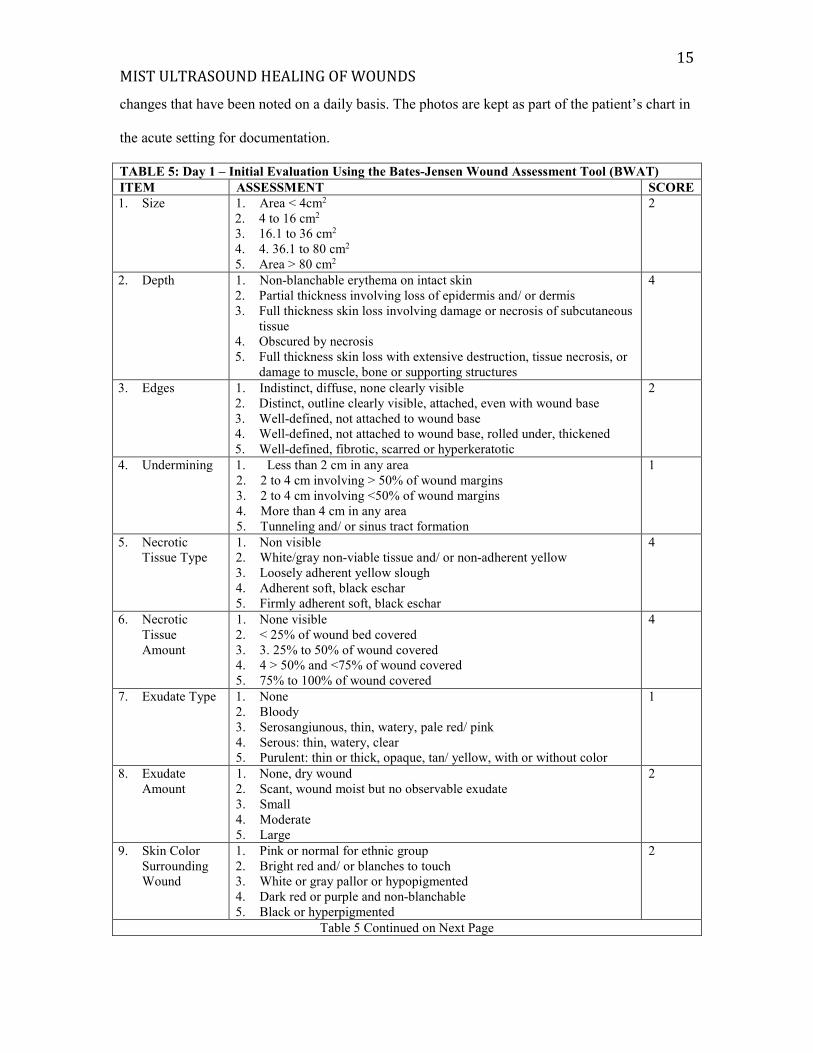
The initial evaluation is completed on day 1 using the Bates-Jensen Wound Assessment
Tool (BWAT), formerly known as the Pressure Sore Status Tool (PSST). This assessment tool
has been shown to demonstrate acceptable reliability and validity. Among clinicians with special
wound management training, this model has yielded an inter-rater reliability coefficient of 0.91
and an intra-rater reliability of 0.975. Clinicians who did not have extraordinary wound
management experience yielded an intra-rater reliability of 0.89 while a reliability estimate of
0.82 was calculated for the inexperienced practitioners versus the expert clinicians. The average
overall content validity index measured 0.91 at the p = .05 level.12
The patient’s wound measuring 3.8cm x 3.7cm is located on the left hip over the greater
trochanter. The wound is unstageable secondary to being 100% covered with hard black eschar.
Detail of the patient’s wound upon evaluation is provided table 4. The evaluation assesses many
characteristics of the wound and scores each category. The total score is set as a baseline.
Upon each treatment including the initial evaluation, Mist Therapy® is applied to the left
hip for four minutes then patted dry with sterile absorbent pads. A 2in x 2in Silverlon® contact
dressing and a hydrocolloid dressing are applied to the left hip. The patient also receives physical
therapy for strengthening and balance training to improve safe transferring and ambulation to
ensure the patient has enough functional independence to frequently offload pressure while
resting in a bed or chair. Moderate assist is required to complete supine to sit. The patient is
ambulatory up to 160 feet total with a front-wheeled walker and contact-guard assist. Nursing

12
MIST ULTRASOUND HEALING OF WOUNDS
staff continually round on the patient and reinforce the importance of offloading the left hip
throughout the entire hospital admission. Since the patient is not resting on an air mattress,
assistance for positioning is provided by the nursing staff by unilaterally offloading one hip with
a pillow and alternating every two hours.
TABLE 4: Day 1 – Initial Evaluation Using the Bates-Jensen Wound Assessment Tool (BWAT)
ITEM ASSESSMENT SCORE
1. Size 1. Area < 4cm2
2. 4 to 16 cm2
3. 16.1 to 36 cm2
4. 4. 36.1 to 80 cm2
5. Area > 80 cm2
2
2. Depth 1. Non-blanchable erythema on intact skin
2. Partial thickness involving loss of epidermis and/ or dermis
3. Full thickness skin loss involving damage or necrosis of subcutaneous
tissue
4. Obscured by necrosis
5. Full thickness skin loss with extensive destruction, tissue necrosis, or
damage to muscle, bone or supporting structures
4
3. Edges 1. Indistinct, diffuse, none clearly visible
2. Distinct, outline clearly visible, attached, even with wound base
3. Well-defined, not attached to wound base
4. Well-defined, not attached to wound base, rolled under, thickened
5. Well-defined, fibrotic, scarred or hyperkeratotic
2
4. Undermining 1. Less than 2 cm in any area
2. 2 to 4 cm involving > 50% of wound margins
3. 2 to 4 cm involving <50% of wound margins
4. More than 4 cm in any area
5. Tunneling and/ or sinus tract formation
1
5. Necrotic
Tissue Type
1. Non visible
2. White/gray non-viable tissue and/ or non-adherent yellow
3. Loosely adherent yellow slough
4. Adherent soft, black eschar
5. Firmly adherent soft, black eschar
5
6. Necrotic
Tissue
Amount
1. None visible
2. < 25% of wound bed covered
3. 3. 25% to 50% of wound covered
4. 4 > 50% and <75% of wound covered
5. 75% to 100% of wound covered
4
7. Exudate Type 1. None
2. Bloody
3. Serosangiunous, thin, watery, pale red/ pink
4. Serous: thin, watery, clear
5. Purulent: thin or thick, opaque, tan/ yellow, with or without color
1

13
MIST ULTRASOUND HEALING OF WOUNDS
Table 4 Continued from previous page
ITEM ASSESSMENT SCORE
8. Exudate Amount 1. None, dry wound
2. Scant, wound moist but no observable exudate
3. Small
4. Moderate
5. Large
2
9. Skin Color Surrounding
Wound
1. Pink or normal for ethnic group
2. Bright red and/ or blanches to touch
3. White or gray pallor or hypopigmented
4. Dark red or purple and non-blanchable
5. Black or hyperpigmented
2
10. Peripheral Tissue Edema 1. minimal swelling around wound
2. non-pitting edema extends < 4 cm around wound
3. non-pitting edema extends ≥ 4 cm around wound
4. Pitting edema extends < 4 cm around wound
Crepitus and/ or pitting edema extends ≥ 4 cm around
wound
1
11. Peripheral Tissue
Induration
1. Minimal firmness around wound
2. Induration less than 2 cm around wound
3. Induration 2 to 4 cm extending < 50% around wound
4. Induration 2 to 4 cm extending ≥ 50% around wound
Induration > 4 cm in any area
5
12. Granulation Tissue 1. Skin intact or partial thickness wound
2. Bright, beefy red: 75% to 100% of wound filled and/ or
tissue overgrowth
3. Bright, beefy re: < 75% and > 25% of wound filled
4. Pink and/ or dull, dusky red and/ or fills < 25% around
wound
No granulation tissue present
5
13. Epithelialization 1. 100% of wound covered, surface intact
2. 75% to < 100% of wound covered and/ or epithelial tissue
extends more than 0.5 cm into wound bed
3. 50% to <75% of wound covered and/ or epithelial tissue
extends to less than 0.5 cm into wound bed
4. 25% to <50% wound covered
<25% wound covered
4
TOTAL SCORE 34
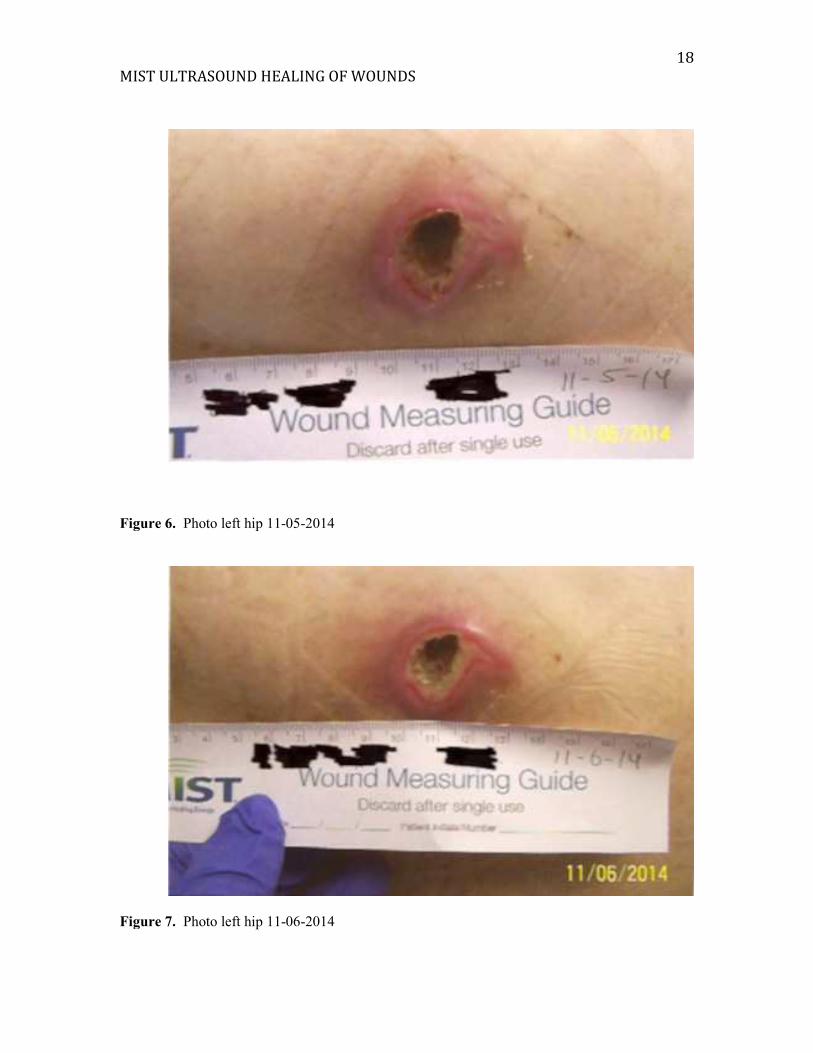
On Day 2, the Mist ultrasound is repeated and the same dressings are applied. The wound
area measured 3.4cm x 3.2cm with a paper ruler and presented and significantly less black
necrotic tissue noted, measuring 1.6cm x 1.2cm in area. Whitish-yellow, loosely-adherent slough
is present covering the area of the wound that previously was covered with eschar, which
collectively still encompass 100% of the wound surface total.
A reassessment is completed on Day 3 and the Mist ultrasound and dressing changes are
repeated. Table 5 summarizes the full reassessment of the wound. On this day the wound

14
MIST ULTRASOUND HEALING OF WOUNDS
measures 3.4cm x 3.2cm with the necrotic eschar measuring 1cm2. The patient also continues
physical therapy once daily beginning immediately after every Mist ultrasound session. The
patient is making slow progress with physical therapy from a functional mobility standpoint.
Minimal assist is required for transfers and bed mobility. The patient’s ambulation distance only
increased by 20 additional feet and still requires a walker for balance. Day 4 is the day of the
patient’s discharge from the hospital to a skilled nursing facility for short-term rehab. A final
treatment of Mist ultrasound with dressing changes is completed. The wound now measures
3.4cm x 2.8cm with the eschar measuring 0.9cm x 0.6cm. In the skilled nursing facility, the
patient will no longer receive Mist Ultrasound Therapy® as it is not provided in the particular
facility. However, the patient will have regular hydrocolloid dressing changes completed by the
wound care nurse as ordered in the hospitalist’s discharge instruction.
RESULTS
Table 5 summarizes the reassessment of the wound, which was completed on Day 3 (the
day prior to the patient’s discharge and final treatment). The total score of 34 upon Day 1 and the
evaluation has reduced to 32 upon the reassessment on Day 3. A lower number in this case
indicates progression in wound healing. The patient’s wound measured 3.8cm x 3.7cm
(14.06cm2) on Day 1 and 3.4cm x 2.8cm (9.52cm2) on Day 4, which is a 32% reduction in size in
just three days. According to Attinger et al, the normal rate of healing shows 10-15% reduction in
wound dimensions one week.13 The patient’s wound in this report shows accelerated healing,
demonstrating potential for Mist ultrasound to promote restoration of normal wound healing
rates. Steady decreases in total wound bed area and eschar are illustrated in figure 3 and figure 4
respectively. The patient’s deep tissue injury showed overall improvement and healing while
receiving Mist Therapy® combined with dressing changes, physical therapy, and monitoring by
the nursing staff and other clinical staff in the acute care setting. Figures 5-8 are photos of the
patient’s left hip. One photo is taken upon each visit (Day 1-4) to illustrate the characteristic
15
MIST ULTRASOUND HEALING OF WOUNDS
changes that have been noted on a daily basis. The photos are kept as part of the patient’s chart in
the acute setting for documentation.
TABLE 5: Day 1 – Initial Evaluation Using the Bates-Jensen Wound Assessment Tool (BWAT)
ITEM ASSESSMENT SCORE
1. Size 1. Area < 4cm2
2. 4 to 16 cm2
3. 16.1 to 36 cm2
4. 4. 36.1 to 80 cm2
5. Area > 80 cm2
2
2. Depth 1. Non-blanchable erythema on intact skin
2. Partial thickness involving loss of epidermis and/ or dermis
3. Full thickness skin loss involving damage or necrosis of subcutaneous
tissue
4. Obscured by necrosis
5. Full thickness skin loss with extensive destruction, tissue necrosis, or
damage to muscle, bone or supporting structures
4
3. Edges 1. Indistinct, diffuse, none clearly visible
2. Distinct, outline clearly visible, attached, even with wound base
3. Well-defined, not attached to wound base
4. Well-defined, not attached to wound base, rolled under, thickened
5. Well-defined, fibrotic, scarred or hyperkeratotic
2
4. Undermining 1. Less than 2 cm in any area
2. 2 to 4 cm involving > 50% of wound margins
3. 2 to 4 cm involving <50% of wound margins
4. More than 4 cm in any area
5. Tunneling and/ or sinus tract formation
1
5. Necrotic
Tissue Type
1. Non visible
2. White/gray non-viable tissue and/ or non-adherent yellow
3. Loosely adherent yellow slough
4. Adherent soft, black eschar
5. Firmly adherent soft, black eschar
4
6. Necrotic
Tissue
Amount
1. None visible
2. < 25% of wound bed covered
3. 3. 25% to 50% of wound covered
4. 4 > 50% and <75% of wound covered
5. 75% to 100% of wound covered
4
7. Exudate Type 1. None
2. Bloody
3. Serosangiunous, thin, watery, pale red/ pink
4. Serous: thin, watery, clear
5. Purulent: thin or thick, opaque, tan/ yellow, with or without color
1
8. Exudate
Amount
1. None, dry wound
2. Scant, wound moist but no observable exudate
3. Small
4. Moderate
5. Large
2
9. Skin Color
Surrounding
Wound
1. Pink or normal for ethnic group
2. Bright red and/ or blanches to touch
3. White or gray pallor or hypopigmented
4. Dark red or purple and non-blanchable
5. Black or hyperpigmented
2
Table 5 Continued on Next Page

16
MIST ULTRASOUND HEALING OF WOUNDS
Table 5 Continued from previous page
ITEM ASSESSMENT SCORE
10. Peripheral
Tissue Edema
1. minimal swelling around wound
2. non-pitting edema extends < 4 cm around wound
3. non-pitting edema extends ≥ 4 cm around wound
4. Pitting edema extends < 4 cm around wound
5. Crepitus and/ or pitting edema extends ≥ 4 cm around wound
1
11. Peripheral
Tissue
Induration
1. Minimal firmness around wound
2. Induration less than 2 cm around wound
3. Induration 2 to 4 cm extending < 50% around wound
4. Induration 2 to 4 cm extending ≥ 50% around wound
5. Induration > 4 cm in any area
1
12. Granulation
Tissue
1. Skin intact or partial thickness wound
2. Bright, beefy red: 75% to 100% of wound filled and/ or tissue
overgrowth
3. Bright, beefy re: < 75% and > 25% of wound filled
4. Pink and/ or dull, dusky red and/ or fills < 25% around wound
5. No granulation tissue present
4
13. Epithelializatio
n
1. 100% of wound covered, surface intact
2. 75% to < 100% of wound covered and/ or epithelial tissue extends
more than 0.5 cm into wound bed
3. 50% to <75% of wound covered and/ or epithelial tissue extends to
less than 0.5 cm into wound bed
4. 25% to <50% wound covered
5. <25% wound covered
4
TOTAL SCORE 32
0
2
4
6
8
10
12
14
16
Day 1 Day 2 Day 3 Day 4
Total Wound Area
Wound Area (cm2)
Figure 3. Total Wound Area

17
MIST ULTRASOUND HEALING OF WOUNDS
0
0.5
1
1.5
2
2.5
Day 2 Day 3 Day 4
Area of Eschar only (cm)
Eschar area (cm2)
Figure 4. Area of Eschar
Figure 5. Photo left hip 11-04-2014
18
MIST ULTRASOUND HEALING OF WOUNDS
Figure 6. Photo left hip 11-05-2014
Figure 7. Photo left hip 11-06-2014

19
MIST ULTRASOUND HEALING OF WOUNDS
DISCUSSION
The effectiveness of Mist ultrasound has been investigated mostly within the past 10
years. Investigators used non-contact ultrasound on mice and rats with experimental diabetic
wounds. More research on Mist ultrasound began surfacing but with small subject size designs.
Very limited randomized control trials were utilized. Also, some research that is available comes
from the machine’s manufacturer, which may facilitate potential research bias. Some research
found Mist ultrasound to be helpful in treating wounds while other sources indicate that there is
no significant evidence to support that Mist ultrasound is effective in debriding wounds.
Therefore the already limited research sometimes presents conflicting results and conclusions.
This may be due to some studies utilizing small sample sizes and suboptimal intervention
designs. The purpose of this case report is to illustrate how Mist ultrasound can be utilized in
wound care to treat deep tissue injuries by performing selective debridement and promoting
wound healing. Mist ultrasound is overall very time-efficient, easy to apply, and has very limited
Figure 8. Photo left hip 11-07-2014

20
MIST ULTRASOUND HEALING OF WOUNDS
contraindications for use. Patient non-compliance issues with Mist Ultrasound may be less likely
since this modality is painless. Clinical use requires an order under a physician and may feasibly
be used in many appropriate acute, sub-acute, and outpatient clinics that are subject to treating a
variety of wounds, whether chronic or acute.
Chronic wounds are difficult to heal. Yet that is why they are chronic in nature.
Oftentimes co morbidities are present such as diabetes mellitus and peripheral vascular disease.
Mist Ultrasound is a new modality that has been acquiring more and more attention in the past ten
years to assist healing in chronic wounds. The purpose of this case report is to examine the effects
Mist Ultrasound has on a slow healing wound. The findings in this case report would contribute
to the limited literature that exists regarding the effects of Mist Ultrasound in non-healing
wounds. Early literature found that ultrasound delivered through normal saline could increase
collagen formation and granulation tissue within wounds among mice and lab rats.9,10 In the
patient population, Mist Ultrasound has been used on chronic wounds, diabetic ulcers, vascular
insufficiency ulcers and has been shown to be effective even as a stand alone treatment for
wounds.3,4 Advocates of MIST ultrasound claim that this modality targets free radicals and
bacteria and eliminates them via the ultrasound. Despite this, some studies have not found a
statistically significant reduction in bacteria of chronic wounds although some bacterial reduction
was noted.4
The patient in this study received Mist Therapy® one time daily for four consecutive
days to treat a necrotic deep tissue injury on the left hip over the greater trochanter. Over the
course of those four days, the patient’s wound showed decreasing total area and black eschar.
The patient was also given pressure relief from the left greater trochanter by the RN staff via
proper positioning and offloading of the left hip. Daily physical therapy assisted in regaining the
patients overall functional mobility and independence. Various absorbent dressings were changed
at least once daily and following each Mist Therapy® treatment to ensure protection of healthy
21
MIST ULTRASOUND HEALING OF WOUNDS
tissue and absorption of drainage from the wound. The patient presented with scant to no drainage
upon each visit by physical therapy staff.
Without the use of sharp debridement, most of the necrosis of the wound progressed from
hard, black eschar to soft, loosely adherent whitish-yellow slough. Sharp debridement is
alternative form of wound care that is painful compared to Mist Therapy®, results in increased
bleeding, and requires a skill level that is more laborious to the clinician. For instance, sharp
debridement requires higher use of fine motor control and careful, precise hand movement.
Pulsed-lavage is also a more painful alternate to wound care than Mist Therapy®.
Overall, the patient displayed remarkable progress in acceleration of debridement of
necrotic tissue and reduction in wound size over the course of only four daily treatments using
Mist therapy as an adjunct to conventional treatment. Mist Therapy® shows promise toward
achieving notable healing of deep tissue injuries and possibly other wound types. This case study
suggests that additional research is warranted while employing and a more controlled
environment to further investigate the effects of Mist Therapy® on deep tissue injuries and other
wound types.

22
MIST ULTRASOUND HEALING OF WOUNDS
REFERENCES
1. Enoch S, Leaper DJ. Basic Science of Wounds Healing. Surgery. 2005: 23(2): 37-42.
2. Celleration Inc. MIST ultrasound healing therapy. Mist Therapy Website.
http://www.misttherapy.com/ Updated 2014. Accessed June 14, 2014.
3. Ennis W, Valdes W, Gainer M, Meneses P. Evaluation of clinical effectiveness of Mist
ultrasound therapy for the healing of chronic wounds. Advances in Skin and Wound Care.
2005; 10(8): 437-446.
4. Escandon J, Vivas AC, Perez R, Kirsner R, Davis S. A prospective pilot study of
ultrasound therapy effectivenss in refractory venous leg ulcers. International Wound
Journal. 2012; 9: 577-578.
5. Kavros S, Liedl D, Boon A, Miller J, Hobbs J, Andrews K. Expedited wound healing
with noncontact low-frequency ultrasound therapy in chronic wounds: A retrospective
analysis. Advances in Skin & Wound Care. 2008; 21(9): 416-423.
6. Ramundo J, Gray M. Is ultrasonic mist therapy effective for debriding chronic wounds? J
Wound Ostomy Continence and Nursing. 2008; 35(6): 579-583.
7. Kent, D. Getting misty over wound care: Learn how therapy with ultrasound waves and
saline mist can help your patient’s wound heal. Nursing. 2007; 37(9): 36-37.
8. Ennis W, Formann P, Mozen N, Massey J, Conner-Kerr T, Meneses P. Ultrasound
therapy for recalcitrant diabetic foot ulcers: results of a randomized, double-blind,
controlled, multicenter study. Ostomy/Wound Management. 2005; 51(8): 24-36.
9. Thawer H. Effects of ultrasound delivered through a mist of saline to wounds in mice
with diabetes mellitus. J Wound Care. 2004; 13(5): 171-176.
10. Demir H, Yaray S, Kirnap M, Yaray K. Comparison of the effects of laser and ultrasound
treatment on experimental wound healing in rats. J Rehab Research and Development.
2004; 41(5): 721-728.
11 Kavros S, Miller J, Hanna S. Treatment of ischemic wounds with noncontact, low-
frequency ultrasound: The Mayo Clinic Experience, 2004-2006. Advances in Skin &
Wound Care. 2007; 20(4): 221-226.
12 Sussman C, Bates-Jensen B. A Collaborative Practice Manual for Health Professions 3rd
edition. Baltimore, MD 21201 & Philadelphia, PA 19106. Lippincott Williams &
Wilkins. 2007
13 Attinger C, Janis J, Steinberg J, Schwartz J, Al-Attar A, & Couch K. Clinical Approach
to Wounds: Debridement and Wound Bed Preparation Including the Use of Dressings
and Wound-Healing Adjuvants. Plastic and Reconstructive Surgery. 2006: 117(Suppl),
72S-109S.