mirnas and biomarkers gabriella sozzi. diagnostic micrornas in lung tumors stratifying lung cancer...
TRANSCRIPT

miRNAs and biomarkers
Gabriella Sozzi

diagnostic microRNAs in lung tumors stratifying lung cancer molecular subtypes ( Landi L. et al)
prognostic microRNAS in tumors miRNA expression profiles to predict clinical outcomes of resectable SCLC patients (Nan Bi et al) MicroRNAs associated with survival in malignant pleural mesothelioma patients (Kirschner et al)
diagnostic microRNAs in biological fluids sputum miRNA expression profiles for the detection of non-small cell lung cancer (Razzak et al) plasma miRNA test for lung cancer screening (Sozzi et al)
Biomarker-Driven Programs for Lung Cancer Screening General considerations (Massion P.)

mRNA
One miRNA
mRNA
mRNA
mRNA
mRNA
…
small noncoding RNAs that regulate gene expression by binding complementary sequences of target mRNAs and inducing their degradation or translational repression
Evolutionary conserved
One miRNA has multiple targets
microRNA: a new class of biomarkers

Diagnostic/prognostic miRNAs in lung cancer
Diagnostic miRNA signatures
let-7a: target KRASTakamizawa et al., 2004
43 miRNAs (let-7a, miR-205, miR-126, miR-21)
Yanaihara et al., 2006
miR-205 SCC; miR-21 ADCLebanony et al., 2009
Prognostic miRNAs
let-7a, miR-221, miR-137, miR-372 & miR-182 ∗ Yu et al., 2008
↓ miR-34a: targets C-MET, BCL2 Gallardo et al., 2009
↓let-7a, -34a, 34c, 25, -91
34 miRNAs ADC vs. SCCLandi et al., 2010
Landi et al., 2010
↓ Let-7a miR-155 in ADCTakamizawa et al., 2004, Yanaihara et al., 2006

Lung cancer meta-signature miRNAs
Urmo Vo˜saInt. J. Cancer 2013Urmo VõsaInt. J. Cancer 2013
20 published miRNA studies 598 tumor and 528 non-cancerous samples 15 miRNA metasignature robust rank aggregation method

microRNA : plasma/serum-based biomarkers for cancer detection?
•Blood-based miRNA studies are in their infancy
•miRNA remain rather intact and stable in plasma/serum
•Simple universally applicable assay for quantification (i.e. qRT-
PCR)
In lung cancer plasma/serum levels of miRNAs might have diagnostic (Silva, ERJ 2010;
Shen, Lab Invest 2010; Foss, J TO 2011; Boeri PNAS 2011; Bianchi EmboMolMed 2011;
Hennessey, PLoS One 2012) and prognostic value (Hu, JCO, 2010).
miRNAs have been found packaged in exosomes derived from multivesicular bodies
(7) or be exported in the presence of RNA-binding proteins (i.e. Ago-2)(8) or might be
exported microvesicles shed during membrane blebbing (9). Once in the
extracellular space, these miRNAs could be taken up by other cells, degraded by RNases,
or excreted(10).

Lorenza Landi1
Pierluigi Gasparini2, Stefania Carasi 2, Carmelo Tibaldi1 , Luciano Cascione2, Greta Alì3, Armida D’Incecco1, Jessica Salvini1, Gabriele Minuti1 , Antonio Chella3 ,
Gabriella Fontanini3, Federico Cappuzzo1 and Carlo M.Croce2
1 Istituto Toscano Tumori, Dipartimento di Oncologia, Livorno Italy2 The Ohio State University, Comprehensive Cancer Center, Department of Molecular Virology,
Immunology and Medical Genetics, Columbus, OH, USA3 Azienda Ospedaliera Universitaria Pisana, Pisa, Italy
MO 16.01: Different Micro-RNA Expression In Lung Adenocarcinoma With Molecular Driver Events

MO 16.01: Different Micro-RNA Expression In Lung Adenocarcinoma With Molecular Driver Events - Landi L
Trial Background:
•Oncogenic driving mutations identify lung adenocarcinoma with different prognosis and
sensitivity to targeted therapy
•Recent studies have suggested that miRNAs could be useful for stratifying lung cancer
subtypes, however miRNAs deregulation in NSCLC with ALK translocation, EGFR or KRAS
mutations is largely unknown
Aim:
•Identify miRNA signature differences according to the presence of specific oncogenic driver
Methods:
•Retrospective analysis of a cohort of 67 NSCLCs matched with 17 normal lung tissues
•RNA was isolated from FFPE using the Recover ALL kit (Ambion) and miRNA levels were
analyzed using the NanoString miRNA V2 panel
•Data were processed according to manufacture guidelines. We used Limma to test for
differential expression analysis data
•The miRNAs expression between tissues for all RT-qPCR was analyzed using the parametric t-
test (unpaired,2-tailed for validation)

* other histology included patients with clear cell carcinoma; § EGFR wild type (wt) included patients EGFR wt and KRAS wt and ALK negative; ^ Codon 12 exclusively; ° defined by break-apart FISH assay.
Patient Characteristics
MO 16.01: Different Micro-RNA Expression In Lung Adenocarcinoma With Molecular Driver Events - Landi L

Results
hsa-miR-515 family expression in normal versus tumor and according to molecular events
*p < 0.001MO 16.01: Different Micro-RNA Expression In Lung Adenocarcinoma With Molecular Driver Events - Landi L
hsa-miR-515 family Normal ALK pos * EGFR WT* EGFR mut* KRAS mut*
miR-520d-5p+hsa-miR-518a-5p+hsa-miR-527 5.3 5.2 2.7 2.0 1.4
miR-520h 4.9 5.3 2.8 3.0 2.0
miR-548d-3p 5.7 5.0 2.6 2.5 1.3
miR-548q 5.5 3.7 2.0 1.8 1.3
miR-549 7.1 5.7 2.5 1.8 1.5
UpregulatedDownregulated
ALK +ve
EGFR mut
Normal
EGFR WT
KRAS mut.

• miRNAs profile significantly differs in lung cancer
patients with ALK translocation, EGFR mutations and
KRAS mutations
• Prognostic and predictive role of several miRNAs are
currently under investigation
• miRNAs expression could represent an useful tool to
refine diagnosis of oncogene addicted NSCLC
• Targeting miRNAs could represent a potential strategy
to modulate sensitivity to biological agents
Conclusions
MO 16.01: Different Micro-RNA Expression In Lung Adenocarcinoma With Molecular Driver Events - Landi L
MicroRNA Signature Predicts Survival in Resectable Small Cell Lung Cancer
Nan Bi, Jianzhong Cao, Yongmei Song, Jie Shen, Wenyang Liu, Jing Fan, Guogui Sun, Tong Tong, Jie He, Yuankai Shi, Xun Zhang, Ning Lu, Qimin Zhan, and Luhua
Wang
Cancer Hospital and Cancer Institute, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100021, China
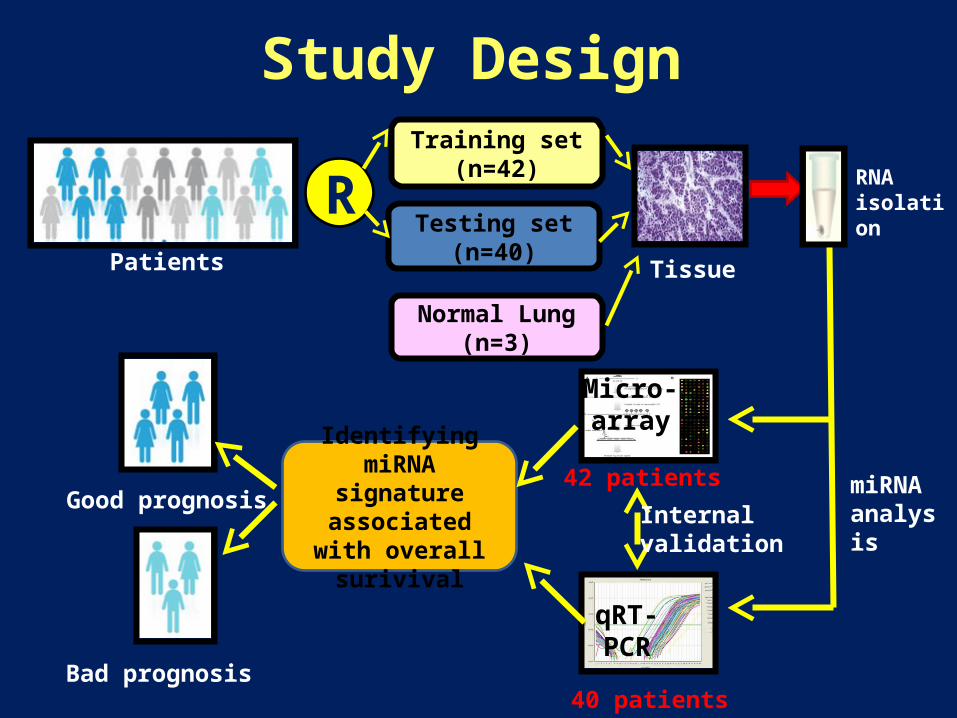
Study Design
RTraining set
(n=42)
Testing set(n=40)
Micro-array
qRT-PCR
Internal validation
Identifying miRNA signature
associated with overall surivival
Good prognosis
Bad prognosis
RNA isolation
TissuePatients
miRNA analysis
42 patients
40 patients
Normal Lung (n=3)

Results (3)-Training Set (N=42)
miR-886-3p
0
1000
2000
3000
4000
miR-150
0
1000
2000
3000
4000
5000
NL NLSCLC SCLC
P=0.05 P=0.09
N=3 N=3N=42 N=42
The expression levels of miR-886-3p and miR-150 are lower in SCLC tumors than those in normal lung tissues.

Results (3)-Training Set (N=42)
miRNA signature: 0.545microRNA150 + 0.617microRNA886-3p
0 12 24 36 48 60 72 84 960
20
40
60
80
100
Months
OS
(%) Low risk (N=21) MST
not reached
High risk (N=21) MST = 12.6 months
D
P=0.02

Results (5)-Test Set (N=40)
0 12 24 36 48 60 72 84 96 108 1200
20
40
60
80
100
Months
OS
(%)
Low risk (N=20) MST not reached
High risk (N=20) MST = 18.9 months
P=0.005

Results (6)- MiRNA Signature Predicts PFS in both Training and Test Groups
0 12 24 36 48 60 72 84 960
20
40
60
80
100
P=0.045
Months
PF
S(%
)
Low risk
High risk
A
0 12 24 36 48 60 72 84 96 108 1200
20
40
60
80
100
P=0.017
MonthsP
FS
(%)
Low risk
High risk
B
Test group (N=40)Training group (N=42)

Results (7)- Multivariate Regression Analysis of MiRNA Signature and Survivals in Test Set (N=40)
Variable Hazard Ratio 95%CI P value
Overall survival
miRNA signature (low risk vs high risk) 0.26 0.10-0.69 0.007
Age (≥60 vs <60) 1.96 0.77-5.02 0.16
Gender (female vs male) 1.12 0.11-11.71 0.92
Smoking status (no smoking vs smoking) 0.57 0.07-4.49 0.60
Progression-free survival
miRNA signature (low risk vs high risk)0.36 0.15-0.86 0.02
Age (≥60 vs <60) 1.45 0.60-3.52 0.41
Gender (female vs male) 1.15 0.11-11.73 0.91
Smoking status (no smoking vs smoking)0.45 0.06-3.46 0.44

Conclusion A miR-150/miR-886-3p signature was correlated with the
survivals in 42 resectable SCLCs and validated independently with another 40 SCLC cases.
The expression levels of both miR-150 and miR-886-3p were lower in tumors than in normal lung tissues, indicating both of them could serve as tumor suppressor genes in SCLC.
MicroRNAs may serve as promising prognostic markers as well as noval therapeutic targets for SCLC.
Larger sample size and function studies are warranted to validate our findings.

MicroRNAs miR-17-5p, miR-21 and miR-210 are associated with survival in
malignant pleural mesothelioma patients undergoing extrapleural pneumonectomy
Michaela B Kirschner1,
Yuen Yee Cheng1, Steven C Kao1,2, Brian C McCaughan3,4, Nico van Zandwijk1, Glen Reid1
1Asbestos Diseases Research Institute, University of Sydney2Department of Medical Oncology, Sydney Cancer Centre
3Cardiothoracic Surgical Unit, Royal Prince Alfred Hospital Sydney 4The Baird Institute and Sydney Medical School, University of Sydney

Patient characteristics• Patients undergoing EPP in Sydney between 1994 and 2009:
– Series previously used to assess NLR and Calretinin (Kao et al, JTO, 2011)
– Complete Cohort = 85– Patients with RNA = 64
Variables Long survivors(N=8)
Short survivors(N=8)
Median Age (range)
51.5 (37 – 64) 62 (47 – 70)
GenderMaleFemale
62
62
Histological SubtypeEpithelioidBiphasic
80
80
StageIIIIIIIV
0170
0080
Induction ChemotherapyYesNo
08
08
Median survival (mo)
57.2 ( 45.83 – 90.48) 6.4 (1.94 – 8.28)
Variables All patients (N=48)
Median Age (range)
58 (22 - 74)
GenderMaleFemale
3711
Histological SubtypeEpithelioidBiphasic
3117
StageIIIIIIIV
28
326
Induction ChemotherapyYesNo
1335
Median survival (mo)
15.28 (0.07 – 81.18)
Training Set (microarray+RT-qPCR) Test Set (RT-qPCR)

Kaplan-Meier and Multivariate Analysis
Hazard Ratio
95 % CI p-value
miR-17-5pLowHigh 2.26 1.04 – 4.93
1 (ref)0.041
Factor Hazard Ratio
95 % CI p-value
miR-21LowHigh 4.12 1.86 – 9.14
1 (ref)<0.001
Factor Hazard Ratio
95 % CI p-value
miR-210LowHigh 1.46 0.73 – 2.89
1 (ref)0.283
28.2 mo
13.3 mo (p=0.005)
24.2 mo
9.4 mo(p=0.001)
19.7 mo
13.3 mo(p=0.031)
• Classic prognostic factors (N=48):– Female gender (49.8 mo vs 14.6 mo in males, p=0.019)– Epithelioid histology (18.17 mo vs 12.16 mo in biphasic, p=0.048)
• Cox-Regression for each microRNA combined with classic prognostic factors (Histology, age, gender, stage)

Conclusions and Future Directions
Those microRNAs have the potential to assist in better selection of patients considered for EPP
• Validation in independent samples sets is required
• Combination of several microRNAs as potential prognostic signature
• Lower expression levels of three microRNAs in tumour tissue are associated with longer survival of patients undergoing EPP
• miR-17-5p and miR-21 remain significant in a multivariate model including classic prognostic factors
• P2.20-011 | A prospective clinical study evaluating stage dependent sputum micro-RNA expression profiles for the detection of non-small cell lung cancer
• Authors: Rene Razzak1, Eric L.R. Bédard1, Julian O. Kim2, Sayf Gazala1, Linghong Guo2, Sunita Ghosh2, Anil A. Joy2, Tirath Nijjar2, Eric Wong1, Wilson H. Roa2 1University of Alberta, Edmonton, AB/CANADA, 2Cross Cancer Institute, Edmonton, AB/CANADA
miRNAs in biological fluids

Our objective was to utilize an efficient, cost-effective panel consisting of 3 miRNAs (miR-21, miR-210 and miR-372) for prospective validation as a potential means of accurately detecting NSCLC. This panel was selected based on retrospective analysis of 11 miRNAs our group had previously undertaken using separate NSCLC and control cohorts.

• 21 early NSCLC (≤ Stage II) patients, 22 advanced NSCLC (≥ Stage III) patients and 10 control subjects were prospectively accrued. A single sputum sample was obtained through spontaneous expectoration from each study participant.
• miR-21, miR-210 and miR-372 expression was conducted on each sputum sample and normalized to an endongenous control (U6) relative to a MRC-5 reference sample, using RNA reverse transcription and Quantitative real-time Polymerase Chain Reaction (RT-qPCR).
• Statistical evaluation consisted of unsupervised hierarchical cluster analysis of the experimental-normalized miRNA expression profiles using within-group linkage.

Comparing early NSCLC to controls, the use of miR-21, miR-210 and miR372 expression yielded a diagnostic sensitivity of 66.7% and a specificity of 90.0%. Advanced NSCLC patients had an improved sensitivity of 81.8% with the same specificity of 90.0%.
The utilization of miR-21, miR-210 and miR372 sputum expression might provide a sensitive and specific means of detecting NSCLC. The potential linkage between their expression and NSCLC stage may account for the higher sensitivity observed in the advanced NSCLC group. Future use of this promising panel on a larger population will be required to establish its potential application as a screening tool.

Plasma miRNA test for lung cancer screening
Gabriella Sozzi

+ LDCT
4,000 Smokers ≥ 50 years
Smoking cessationLung function assessment blood sampling
R
2005 - 2011
LDCT every year
LDCT every 2 years
Pastorino U. et al., Eur J Cancer Prev. 2012
R
> 100,000 biological samples

Study Design &
Aims
Diagnostic performance of miRNA test (3 levels, H-I-L risk MSC classifier) for lung cancer detection across LDCT and observational arms
Combination of LDCT and plasma miRNA test
Prognostic value of the miRNA assay Sozzi G. et al., in press

TotalMSC (risk of lung cancer)
High (H)Intermediate
(I) Low (L)
All subjects 939 63 (6.7) 159 (16.9) 717 (76.4)
No lung cancer 870 32 (3.7) 130 (14.9) 708 (81.4)
Lung cancer 69 31 (44.9) 29 (42.0) 9 (13.0)
performance* SE=87%, SP=81%, PPV=27%, NPV=99%
Lung cancer deaths+ 19 12 (63.2) 6 (31.6) 1 (5.3)º
Lung cancer, stage Iǂ 37 14 (37.8) 19 (51.4) 4 (10.8)Lung cancer, stage II-IIIǂ 12 5 (41.7) 4 (33.3) 3 (25.0)
Lung cancer, stage IVǂ 19 11 (57.9) 6 (31.6) 2 (10.5)
*SE, SP, PPV and NPV were calculated combining pre-specified MSC High and Intermediate versus Low risk. +P=0.0366, based on the Cochran-Armitage test for trend in the proportion of deaths across strata of MSC risk groups among subjects with lung cancer. º plasma sample obtained 30 months before disease detection. ǂ tumor stage information was not available in one patient.p=0.49 for association of MSC with tumor stage
Diagnostic and prognostic performance of MSC
Sozzi G. et al., in press

Months from blood sampling to lung cancer detection
SE SP PPV NPV
6 83% 80% 18% 99%
12 86% 81% 22% 99%
18 86% 81% 23% 99%
24 87% 81% 25% 99%
Time dependency analysis of diagnostic performance of MSC, at 6, 12, 18 and 24 months intervals between blood sampling and lung cancer diagnosis ( according to Heagerty PJ )
Sozzi G. et al., in press

Pre At Post
H
I
L
-30 -20 -10 0 10 20 30 40 50
H
I
L
Months from first surgery
Pre-
At surgery
Post
At II
Post II
miRNAs returning at the normal
levels after surgery
miRNAs remaining deregulated after
surgery660 451
106a 19717 142-3p
92a 320
486-5p28-3p
Patient developing a second primary lung cancer
Modulation of the miRNA signatures in plasma samples collected pre-disease, at time of disease and after surgery (disease-free) from 20 pts
Median time 18 months (4-46)
Median time 20 months (5-28)
0 2 4 6 8
H
I
L
Months from CT detection
Patient developing surrenal metastases
At surgery
Post
LDCT +
Biomarker-Driven Programs for Lung Cancer Screening
Pierre P. Massion, MD
Thoracic ProgramVanderbilt University
Nashville, TN
WCLC Oct 30th, 2013

DiagnosticBMBM of risk
Disease
non-measurable Lung
nodules
BM of Response
Biomarkers in the natural history of lung cancer
RecurrenceBehavior
Dia
gn
osis
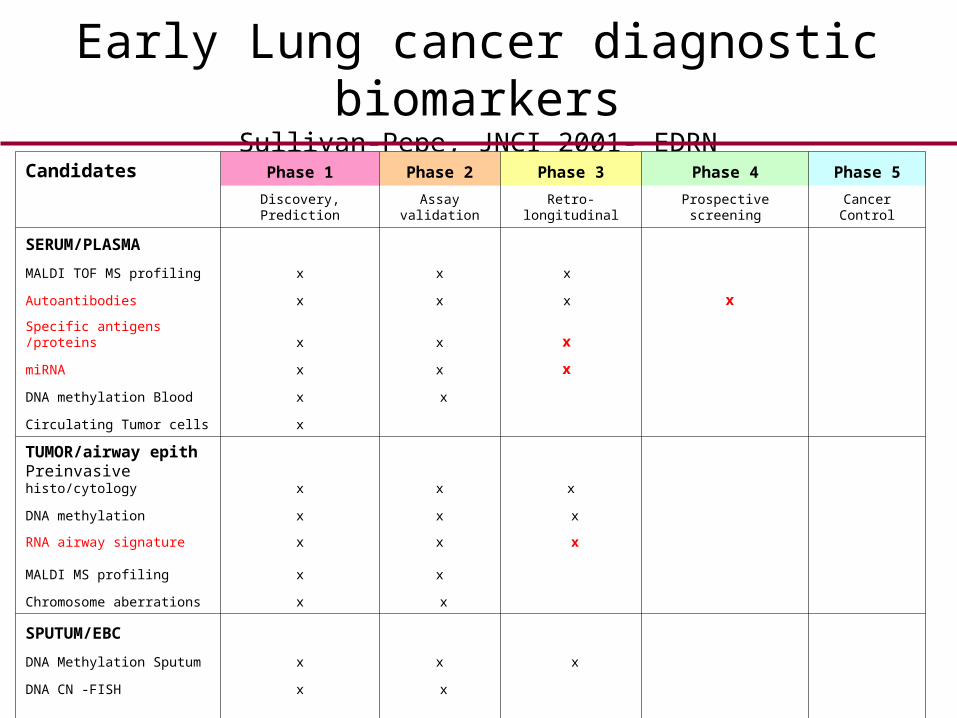
Early Lung cancer diagnostic biomarkers
Sullivan-Pepe, JNCI 2001- EDRNCandidates Phase 1 Phase 2 Phase 3 Phase 4 Phase 5
Discovery, Prediction
Assay validation Retro-longitudinal Prospective screening
Cancer Control
SERUM/PLASMA
MALDI TOF MS profiling x x x
Autoantibodies x x x x
Specific antigens /proteins x x x
miRNA x x x
DNA methylation Blood x x
Circulating Tumor cells x
TUMOR/airway epithPreinvasive histo/cytology x x x
DNA methylation x x x
RNA airway signature x x x
MALDI MS profiling x x
Chromosome aberrations x x
SPUTUM/EBC
DNA Methylation Sputum x x x
DNA CN -FISH x x
VOCs x x

37
Indeterminate Pulmonary Nodules (6-15 mm)
High ProbLow probability
Low Prob
IPNPET or Biopsy
High ProbLow probability
Risk model
IPNPET or Biopsy
Decrease rate of invasive bx, futile thoracotomyDecrease in cost, radiation and anxiety
High Prob
Risk model + Biomarkers Risk reduction Risk increase
Low ProbLow probability
Low Prob

How good should the biomarker be?
• Better than standard of care. • What are the metrics?
- Performance of the test: PPV & NPV- ROC curves (TPR vs FPR). C index comparison- Net reclassification Improvement (NRI) index- Change in decision making.
• De-emphasize Sensitivity and Specificity– Irrelevant (except in early phase of marker evaluation)– Not stable across populations– Require dichotomization of marker values (loss of
information)– No information on added value– Not actionable metric; PPV or NPV are. – Independent of the prevalence of the cancer.
Pecot, CEBP 2012

C4d in plasma samples from early lung cancer
Ajona et al, JNCI 2013
Plasma C4d levels (a stable complement split product) in early stage lung cancer
Phase 2
N=50N=50

C4d levels in screening detected lung cancer
N=32N=158
Ajona et al, JNCI 2013

A Blood-Based Proteomic Classifier for the Molecular Characterization of Pulmonary Nodules
Phase 3
• Shotgun Proteomic analysis of tumors. • Selected candidate proteins for testing in the blood• Developed 13 multiple reaction monitoring MRM
assays. LRP1, BGH3, COIA1, TETN, TSP1, ALDOA,GRP78, ISLR, FRIL, LG3BP, PRDX1, FIBA, GSLG1
• Training and testing algorithm.
Li et al. Sci Transl Med. 2013 Oct
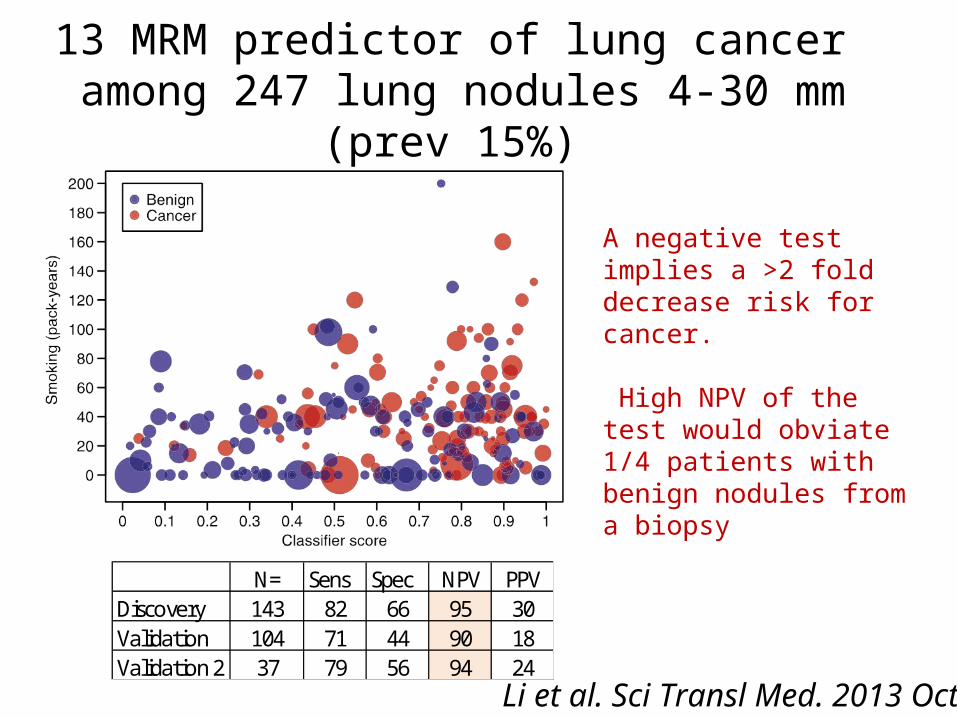
13 MRM predictor of lung cancer among 247 lung nodules 4-30 mm (prev 15%)
Li et al. Sci Transl Med. 2013 Oct
A negative test implies a >2 fold decrease risk for cancer.
High NPV of the test would obviate 1/4 patients with benign nodules from a biopsy
N= Sens Spec NPV PPVDiscovery 143 82 66 95 30Validation 104 71 44 90 18Validation 2 37 79 56 94 24

Boyle, Annals of Oncology 2010Lam, Cancer Prev Res 2011Chapman Tum. Biol. 2012Jett, Lung Cancer 2013 in press
7 Autoantibody signature Phase 4
CAGE, GBU 4–5, HER2, p53, c-myc, NY-ES0-1 and MUC1

7 Autoantibody signatureEarlyCDT- Lung Oncimmune
44
In nodules 8-20 mm, the RR is 4.6
Cases Controls Sensitivity 44.2Profile + 19 17 36 Specificity 88.4Profile - 24 129 153 PPV 52.8
43 146 NPV 84.3Prevalence 0.23RR 3.36
189 nodules tested with the 7 AAB test
P2.20-006 | Autoantibodies to a panel of lung cancer-associated antigens can provide significant discrimination between malignant and non-malignant lung nodules
P. Massion
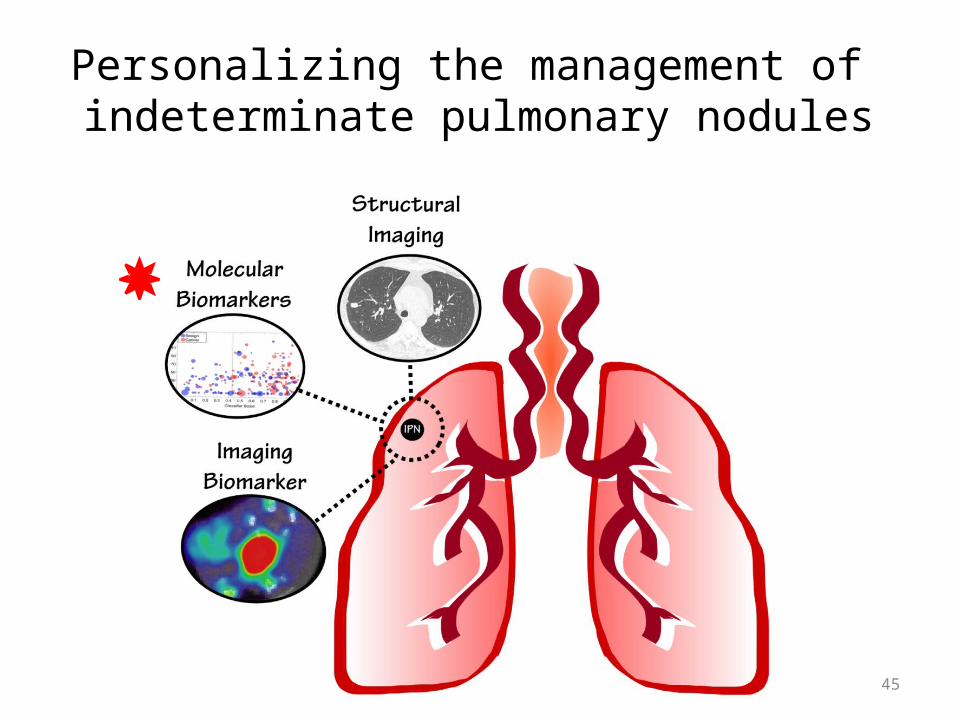
Personalizing the management of indeterminate pulmonary nodules
45

Clinical utility of a diagnostic biomarker:
study design
Positive
RandomizeIPNs
Biopsy
Negative 3 mo CT F/U
SOC (Guidelines)
Randomization of nodules based on the use of a biomarker test. Proves that biomarker “+” affects patients outcomeProves that biomarker test affects patients outcome when compared with unselected use of same Standard Of Care.
test
No testBiopsy
3 mo CT F/U
Outcomes:Early stageFutile Thorac.SurvivalDecrease cost

Conclusions
• Many early detection candidate biomarkers exist
• Few are validated or tested in preclinical setting. Priority to validate existing candidates.
• We need to de-emphasize Sensitivity and Specificity and emphasize NPV or PPV with change in decision making.
• BM should provide knowledge about added value and therefore should be integrated to clinical, laboratory and imaging routine data.
• To demonstrate clinical utility requires significant investment in effort and resources towards biomarkers driven clinical trial.