minority mothers' perceptions of children's body size
TRANSCRIPT
ORIGINAL ARTICLE
Minority mothers’ perceptions of children’s body size
LORRAINE KILLION1, SHERYL O. HUGHES2, JANICE C. WENDT3, DALE PEASE3
& THERESA A. NICKLAS2
1Houston Baptist University, Department of Education and Kinesiology, Houston, Texas, USA, 2Baylor College of Medicine,
Children’s Nutrition Research Center, Department of Pediatrics, Houston, Texas, USA, 3University of Houston, Department
of Health & Human Performance, Houston, Texas, USA
AbstractObjective. To investigate African-American and Hispanic mothers’ perceptions of their children’s body size using a scale withchild figure silhouettes and compare those perceptions with their children’s actual body mass index. Methods. A set of childfigure silhouettes was developed depicting 4 and 5 year-old African-American and Hispanic children. Body mass index wassystematically estimated for each child figure on the set of silhouettes. Minority mothers with children enrolled in ten HeadStart centers (n�/192) were interviewed using the silhouettes, and height and weight measurements were taken on theirchildren. Head Start, a comprehensive child development program that serves children aged 3 to 5 years old, was chosenbecause of the large percentage of minorities, the low-income status of the families, and the age of the children. Results .Significant differences were found between mothers’ perceptions of their children’s body size and the actual body size of thechildren. On average, mothers perceived their children to be thinner than their actual size. Furthermore, of those motherswith children at risk for overweight or overweight, two-thirds were either satisfied with their children’s existing body size orwanted their children to be heavier. However, half of the mothers of children above the 95th percentile for BMI wanted theirchildren to be thinner. Conclusions. These data suggest that minority mothers’ perceptions of their children’s body size maynot be consistently biased in one direction. Despite the possible social norm for a larger body size among low-incomeminorities, some mothers of overweight minority children do perceive their children to be too heavy when they reach acertain size.
Key words: Preschoolers, overweight, measurement, silhouettes, ethnic minorities, BMI, perceptions of body size, Head Start,
body satisfaction, parental socialization
Introduction
The prevalence of adult and pediatric obesity has
increased dramatically in the past two decades (1).
Women tend to be more at risk for being obese, with
low-income minority women facing the greatest risk
(2). Furthermore, overweight among preschoolers
has increased, and is more prominent in minority
children (3,4). Numerous studies have implicated
genetic and social factors as predictors of children’s
weight with positive associations existing between
parental weight and that of their offspring (5,6). The
specific contributions of parental socialization fac-
tors on children’s weight are still unclear.
Parental perceptions of their own weight and
their children’s weight have been investigated as
potential socialization factors on children’s weight.
It is possible that parents’ attitudes and beliefs
concerning eating, weight, and body size directly
influence (either through modeling or direct trans-
mission) their children’s eating behaviors, body
size and weight (7). Parental perceptions among
European-American parents have shown that par-
ents and their 5 year-old children share similar
weight concerns, for example, they both desire
thinner body sizes (8). However, cultural differ-
ences may exist between perceptions of the major-
ity of the European-American population and
those of minorities (e.g., African-American and
Hispanic) regarding ideal weights for their chil-
dren.
Correspondence: Sheryl O. Hughes, PhD, Baylor College of Medicine, Children’s Nutrition Research Center, Department of Pediatrics, 1100 Bates Avenue,
Houston, Texas 77030-2600, USA. Fax: 1 713 798 7130. E-mail: [email protected]
International Journal of Pediatric Obesity. 2006; 1(2): 96�102
(Received 5 December 2005; accepted 12 March 2006)
ISSN Print 1747-7166 ISSN Online 1747-7174 # 2006 Taylor & Francis
DOI: 10.1080/17477160600684286

Recent studies have found that many minority
parents underestimate the weight of their children
(13,14). However, the measurement of these weight
perceptions has been somewhat simplistic, resulting
in a possible misunderstanding of the construct and/
or measurement error. A more comprehensive way
to measure cultural perceptions of weight among
minority parents may be through the use of scales
with child figure silhouettes. These scales provide
contour figures ranging in size from very under-
weight to very overweight and have typically been
used by individuals to assess their own body size
(15).
The purpose of our study was to investigate
minority mothers’ misperceptions of their children’s
body size. Scales with child figure silhouettes depict-
ing 4 and 5 year-old African-American and Hispanic
children were developed specifically for this study
and estimated body mass index (BMI) was calcu-
lated for each of the child figures. These scales were
used to investigate minority mothers’ perceptions of
their children’s body size, determine mothers’ satis-
faction with the size of their children, and investigate
how these factors were related to the children’s
actual BMI.
We hypothesized that mothers in this study would
perceive their children to be thinner than their actual
body size. Furthermore, based on the possible
existence of a cultural norm for a larger body size
among minorities, we wanted to explore differences
in mothers’ satisfaction with their children’s body
size as a function of their children’s weight status. We
also wanted to examine perceptions of mothers who
had normal weight children and those with children
whose weight was above normal.
Methods
Participants
Participants were part of a larger study to investigate
parental feeding practices of African-American and
Hispanic preschool children in Head Start (16). A
total of 231 parents were recruited from ten Head
Start centers located in a suburban area in Southeast
Texas. Head Start is a comprehensive child devel-
opment program that serves children aged 3 to
5 years old and their families. The program is
child-focused with the overall goal of increasing the
school readiness of young children from low-income
families. The population of Head Start is large with
more than 900 000 children. More than 40% of the
children living in poverty in the United States during
the first 5 years of life will participate in Head Start.
In the present study, fathers, grandparents, and
pregnant mothers were excluded from the study
resulting in 192 non-pregnant mothers of Head Start
children. Only mothers were included in this study
because of evidence showing that mothers are
influential in shaping children’s early eating habits,
which may affect weight status (17). Of the mothers
in this study, 42% were African-American (n�/81)
and 58% were Hispanic (n�/111). Mean age of the
mothers was 29.9 years old (SD�/6.6). Of the
children, 43% were African-American and 57%
were Hispanic with a gender breakdown of 45%
boys and 55% girls. The children ranged from 3 to
5 years-of-age with 18% 3 year-olds, 51% 4 year-
olds, and 31% 5 year-olds. Mean age of the children
was 4.2 (SD�/0.07). Specific details regarding the
socio-demographic characteristics of the sample are
provided elsewhere (16).
Procedures
Participants were recruited at the Head Start centers
prior to picking up their children and with phone
calls to the home. The general consent form
procedure was for the participants to take the
consent form home. Participants were then sched-
uled to complete questionnaires. When participants
came to the Head Start centers to complete the
questionnaires, project staff went over the consent
form in detail and answered questions. At that time,
a staff member explained the purpose of the study,
confidentiality was assured, and consent forms were
signed.
Data collection took place after hours at the Head
Start centers from 2:30 p.m. to 5:30 p.m. Partici-
pants were selected one at a time to be interviewed in
a separate area to ensure privacy. Interviews were
conducted in Spanish or English based on the
mothers’ preference. Height and weight measure-
ments were obtained on the mothers and children.
The study was reviewed and approved by the
Internal Review Board at Baylor College of Medicine
prior to data collection and conforms to the provi-
sions of the Declaration of Helsinki in 1995.
Measurements
Body mass index
Body mass index (BMI; weight (kg)/height2 (m))
was assessed following procedures described by
Lohman, Roche, & Martorell (18). Participants
were asked to remove their shoes and any heavy
clothing before being weighed and measured.
Height and weight measurements were obtained by
trained staff, measured in duplicate, and recorded in
centimeters (height) and kilograms (weight) to the
nearest tenth of a point. Age- and gender-specific
Mothers’ perceptions of children’s body size 97

BMI scores were calculated for children using the
CDC standard criteria (19). Children were classified
as normal weight (BMIB/85th percentile), at risk for
overweight (BMI]/85th percentile), and overweight
(BMI]/95th percentile). Mothers were classified
using gender-specific CDC criteria as normal weight
(BMI5/24.9), overweight (BMI]/25) or obese
(BMI]/30).
Mothers’ perceptions of their children’s body size
Mothers’ perception of their children’s body size was
assessed by figure silhouettes of 4 and 5 year-old
children. These rating scales consisted of line draw-
ings of children’s bodies designed to be age and
ethnic appropriate. Mothers were shown cards con-
taining seven figures which corresponded to the
gender and ethnicity of their children. They were
asked to view the card and indicate which of the
seven figures most closely resembled the current size
of their children and the ideal size or which child
figure they would like their children to look like. The
mothers’ responses were recorded on a separate
scoring sheet by the staff member. The child figures
were developed based on input from Head Start
parents through cognitive interviews. Multiple itera-
tions of the child figures were culled resulting in
ethnically age-appropriate silhouettes for use with
African-American and Hispanic mothers.
Development of the silhouettes
During the development phase, cognitive interviews
with three sets of African-American & Hispanic
parents with children from another Head Start
center were conducted to ensure that: 1) the pictures
depicted 4 to 5 year-old children, 2) the facial
features and hair were ethnically appropriate, and,
3) the scaling represented thinnest to heaviest. First,
the age appropriateness of the child figures was
addressed. Twenty parents were asked to estimate
the age of the children through the following
question: ‘‘Approximately what age does the child
on the card represent?’’ Based on parental feedback,
the faces and physiques of the child figures were
adjusted to better reflect 4 and 5 year-old children.
Second, cultural sensitivity of the child figures was
addressed. Twenty different parents were asked two
questions: ‘‘Are the facial features (hair, nose, eyes,
etc.) appropriate to the culture of the child shown on
the card?’’ and ‘‘Is there anything offensive to the
culture that needs to be changed?’’ Based on parents’
suggestions, facial features and hairstyles were ad-
justed. Third, 25 parents were asked questions
regarding the sequencing of the child figures. Each
parent was given a set of seven cards (gender and
ethnic specific) arranged randomly in the packet
with each card containing one child figure. Parents
were asked to remove the cards and arrange them on
the sheet provided. Parents were given the following
instructions: ‘‘Please remove the cards from the
packet and arrange them on the sheet in a progres-
sion with the first card representing the thinnest
child and the last card representing the heaviest
child’’. With a 92% agreement, parents concurred
with the arrangement of child figures from thinnest
to heaviest. The families used in the development of
the child silhouettes were different from those who
took part in the study.
Estimation of BMI for each child figure
One limitation to the use of scales with child
silhouettes is that figures usually do not estimate
the weight of the figure they represent (15). As part
of the validation process in developing these figures,
two methods were used to estimate BMI for each
child figure in the set of seven figures. Two separate
experts in the field of body composition and young
children’s growth and development were used to
estimate the BMI for each child figure. The first
expert, a pediatric nutritional scientist, subjectively
assigned BMI values for each child figure using
the Center for Disease Control’s (CDC) BMI age-
and gender-specific data for 4 and 5 year-old
children (personal communication with N. Butte).
The second expert, a body composition scientist,
used a different approach by utilizing a volume of
cylinders method (personal communication with
K. Ellis). This procedure consisted of measuring
the arms, legs, and trunk of each child figure, and
forming one cylinder by adding each part together
to form the total volume. This procedure is similar to
the BOMAD model used in Health Physics to
calculate radiation doses (20). BMI for each child
figure was then determined by applying the volume
to the CDC age-and gender-specific growth charts
for 4 and 5 year-old children. To make certain that
the calculations by the two experts were similar, a
Pearson’s correlation was conducted showing the
two ratings to be highly correlated (r�/0.96; pB/
0.001). The authors decided to use the mathema-
tical calculations for the estimates of BMI for each
child figure because of their relative objectivity.
Final four sets of gender and ethnic specific silhouettes
The final sets of silhouettes consisted of four lami-
nated cards (based on gender and ethnicity) depicting
seven figures of 4 and 5 year-old children. The four
sets were as follows: 1) seven male African-American
children, 2) seven female African-American children,
98 L. Killion et al.
3) seven male Hispanic children, and 4) seven female
Hispanic children. The four sets were developed on a
single template of seven child figures with only the
skin color, facial features, and hair changing (to
reflect gender and ethnicity) across the four sets.
The difference in size between each of the seven
figures was synchronized to an incremental 7/16 inch
(0.0625) scaling metric added to the waistline of each
child figure, with the middle child figure as the anchor
figure . Therefore, only the torso changed across the
seven figures, with the height and clothing held
constant.
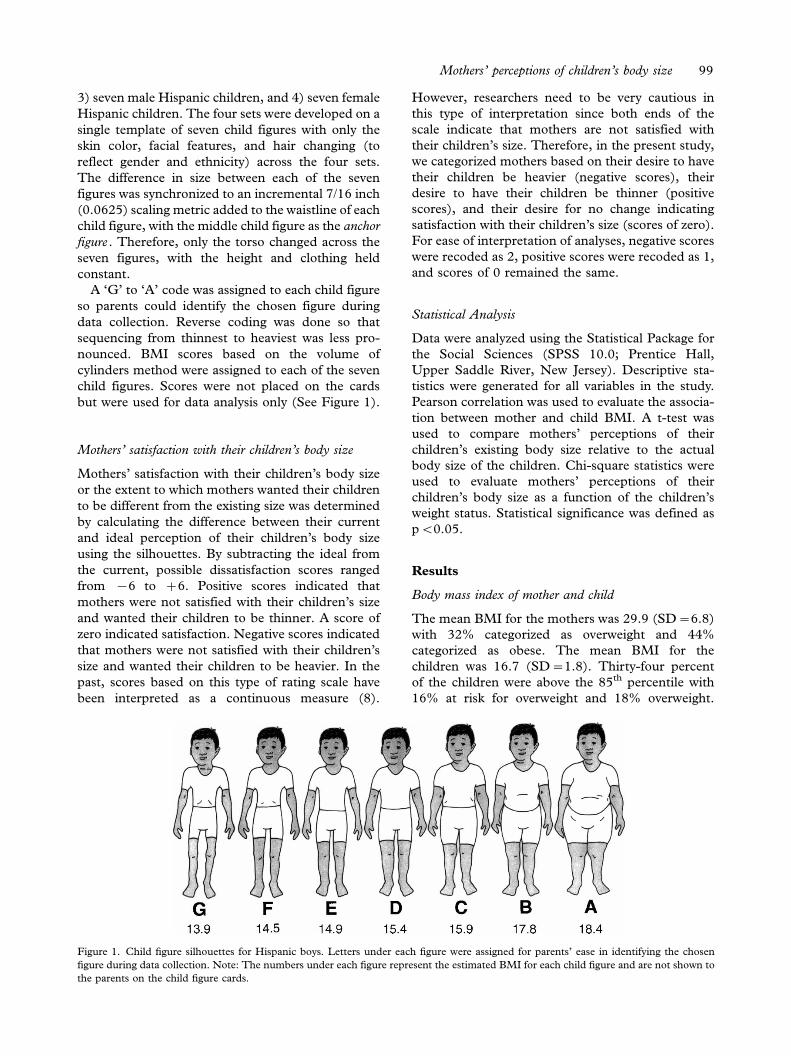
A ‘G’ to ‘A’ code was assigned to each child figure
so parents could identify the chosen figure during
data collection. Reverse coding was done so that
sequencing from thinnest to heaviest was less pro-
nounced. BMI scores based on the volume of
cylinders method were assigned to each of the seven
child figures. Scores were not placed on the cards
but were used for data analysis only (See Figure 1).
Mothers’ satisfaction with their children’s body size
Mothers’ satisfaction with their children’s body size
or the extent to which mothers wanted their children
to be different from the existing size was determined
by calculating the difference between their current
and ideal perception of their children’s body size
using the silhouettes. By subtracting the ideal from
the current, possible dissatisfaction scores ranged
from �/6 to �/6. Positive scores indicated that
mothers were not satisfied with their children’s size
and wanted their children to be thinner. A score of
zero indicated satisfaction. Negative scores indicated
that mothers were not satisfied with their children’s
size and wanted their children to be heavier. In the
past, scores based on this type of rating scale have
been interpreted as a continuous measure (8).
However, researchers need to be very cautious in
this type of interpretation since both ends of the
scale indicate that mothers are not satisfied with
their children’s size. Therefore, in the present study,
we categorized mothers based on their desire to have
their children be heavier (negative scores), their
desire to have their children be thinner (positive
scores), and their desire for no change indicating
satisfaction with their children’s size (scores of zero).
For ease of interpretation of analyses, negative scores
were recoded as 2, positive scores were recoded as 1,
and scores of 0 remained the same.
Statistical Analysis
Data were analyzed using the Statistical Package for
the Social Sciences (SPSS 10.0; Prentice Hall,
Upper Saddle River, New Jersey). Descriptive sta-
tistics were generated for all variables in the study.
Pearson correlation was used to evaluate the associa-
tion between mother and child BMI. A t-test was
used to compare mothers’ perceptions of their
children’s existing body size relative to the actual
body size of the children. Chi-square statistics were
used to evaluate mothers’ perceptions of their
children’s body size as a function of the children’s
weight status. Statistical significance was defined as
pB/0.05.
Results
Body mass index of mother and child
The mean BMI for the mothers was 29.9 (SD�/6.8)
with 32% categorized as overweight and 44%
categorized as obese. The mean BMI for the
children was 16.7 (SD�/1.8). Thirty-four percent
of the children were above the 85th percentile with
16% at risk for overweight and 18% overweight.
Figure 1. Child figure silhouettes for Hispanic boys. Letters under each figure were assigned for parents’ ease in identifying the chosen
figure during data collection. Note: The numbers under each figure represent the estimated BMI for each child figure and are not shown to
the parents on the child figure cards.
Mothers’ perceptions of children’s body size 99
Overall, mothers’ BMI was significantly correlated
with child BMI (r�/0.20; pB/0.01).
Mothers’ perceptions of their children’s body size and
actual body size of their children
Significant differences were found between mothers’
perception of their children’s existing body size and
the actual body size of their children. Mothers
perceived BMI (mean�/15.0; SD�/0.66) of their
children were less than the actual BMI (mean�/
16.7; SD�/1.84) of their children (t�/15.77; pB/
0.0001). Therefore, on average, mothers perceived
their children to be thinner than their actual size.
Differences in mothers’ perceptions as a function of
children’s weight status
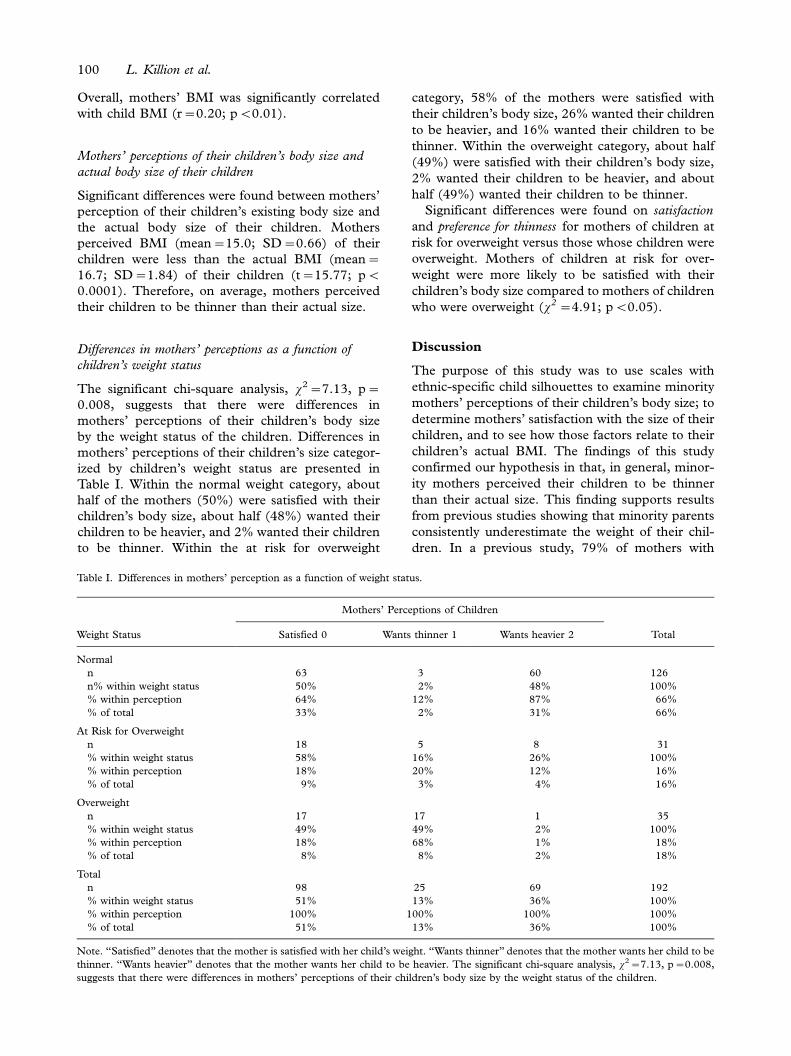
The significant chi-square analysis, x2�/7.13, p�/
0.008, suggests that there were differences in
mothers’ perceptions of their children’s body size
by the weight status of the children. Differences in
mothers’ perceptions of their children’s size categor-
ized by children’s weight status are presented in
Table I. Within the normal weight category, about
half of the mothers (50%) were satisfied with their
children’s body size, about half (48%) wanted their
children to be heavier, and 2% wanted their children
to be thinner. Within the at risk for overweight
category, 58% of the mothers were satisfied with
their children’s body size, 26% wanted their children
to be heavier, and 16% wanted their children to be
thinner. Within the overweight category, about half
(49%) were satisfied with their children’s body size,
2% wanted their children to be heavier, and about
half (49%) wanted their children to be thinner.
Significant differences were found on satisfaction
and preference for thinness for mothers of children at
risk for overweight versus those whose children were
overweight. Mothers of children at risk for over-
weight were more likely to be satisfied with their
children’s body size compared to mothers of children
who were overweight (x2 �/4.91; pB/0.05).
Discussion
The purpose of this study was to use scales with
ethnic-specific child silhouettes to examine minority
mothers’ perceptions of their children’s body size; to
determine mothers’ satisfaction with the size of their
children, and to see how those factors relate to their
children’s actual BMI. The findings of this study
confirmed our hypothesis in that, in general, minor-
ity mothers perceived their children to be thinner
than their actual size. This finding supports results
from previous studies showing that minority parents
consistently underestimate the weight of their chil-
dren. In a previous study, 79% of mothers with
Table I. Differences in mothers’ perception as a function of weight status.
Mothers’ Perceptions of Children
Weight Status Satisfied 0 Wants thinner 1 Wants heavier 2 Total
Normal
n 63 3 60 126
n% within weight status 50% 2% 48% 100%
% within perception 64% 12% 87% 66%
% of total 33% 2% 31% 66%
At Risk for Overweight
n 18 5 8 31
% within weight status 58% 16% 26% 100%
% within perception 18% 20% 12% 16%
% of total 9% 3% 4% 16%
Overweight
n 17 17 1 35
% within weight status 49% 49% 2% 100%
% within perception 18% 68% 1% 18%
% of total 8% 8% 2% 18%
Total
n 98 25 69 192
% within weight status 51% 13% 36% 100%
% within perception 100% 100% 100% 100%
% of total 51% 13% 36% 100%
Note. ‘‘Satisfied’’ denotes that the mother is satisfied with her child’s weight. ‘‘Wants thinner’’ denotes that the mother wants her child to be
thinner. ‘‘Wants heavier’’ denotes that the mother wants her child to be heavier. The significant chi-square analysis, x2�/7.13, p�/0.008,
suggests that there were differences in mothers’ perceptions of their children’s body size by the weight status of the children.
100 L. Killion et al.

overweight preschool children failed to perceive
those children as overweight, with misclassification
greater among less educated mothers (13). In
another study of low-income parents of obese
children (mostly Hispanic), 35% did not believe
their obese child was overweight and 53% did not try
to control what their children ate (14).
The second objective of this study was to deter-
mine whether mothers with children at risk for
overweight or overweight were satisfied with the
weight of their overweight children. Of those
mothers with children at or above the 85th percen-
tile, 66% were satisfied with their children’s size or
wanted their children to be heavier. The fact that
essentially two-thirds of mothers with children who
were at risk for overweight or overweight were
satisfied or wanted their overweight children to be
heavier may be indicative of a social norm for a larger
body size among low-income African-Americans and
Hispanics.
The idea that some of these mothers may have a
distorted view of their children is not a novel idea.
Social psychologists have explored the construct of
‘positive illusions’ in many studies. Taylor (21)
argues that the normal person construes information
in a manner that promotes illusions or mispercep-
tions about the self and others. Normal human
perception is marked not by accuracy but by positive
self-enhancing illusions. Taylor believes that these
illusions are adaptive and promote well-being (21).
Furthermore, other researchers have argued that
because of the great importance of the concept of
the ‘good family’ or the idea of what constitutes a
‘good parent’ to both individuals and society, parents
may be unwilling or unable to provide truthful
accounts of their perceptions (22). This may be
especially true with low-income minorities because
of cultural and/or socio-economic differences.
Although misperceptions or illusions regarding the
weight status of their children may benefit mothers’
well-being in the short-term, these misperceptions
could have long-term consequences for children’s
health in these populations.
The concept that mothers believe that a larger
body size means a healthier child has been explored
in some studies with minorities. Sherry et al. (23)
found that low-income African-Americans generally
believed that their children would outgrow their
overweight as they got older and having a high
weight in childhood was healthy. Because of these
beliefs, parents may be satisfied with heavier children
and/or want their children to be larger.
An unexpected finding in this study was that half
of mothers with children at or above the 95th
percentile for BMI actually wanted their children
to be thinner. This may be indicative of a shift in
perception among some mothers of very overweight
children. These data suggest that despite the possible
social norm for a larger body size among low-income
minorities, some mothers of very overweight minor-
ity children do perceive their children to be too heavy
and want them to be thinner when they reach a
certain size.
The significant correlation between the BMI of
mothers and their children in this study supports
previous studies showing the heritability of weight
status. Strauss and Knight (24) found that maternal
obesity was the most significant predictor of child-
hood obesity compared with a range of factors
relating to the home environment. Furthermore,
there is other evidence showing that children with
overweight or obese parents have a higher chance of
becoming overweight or obese themselves (25�27).
Limitations to the study and suggestions for future
research
The current study was limited to low income
African-American and Hispanic mothers and their
children and, therefore, can only be generalized to
those populations. Misperception of children’s
weight has been found in other studies with nearly
one third of mothers across all ethnic groups
reporting their overweight children as ‘about the
right weight’ (28). Future studies should take a more
comprehensive approach to better understand the
social norms for a thinner or heavier body size
among specific socio-economic and ethnic groups.
Implications
Many studies have suggested obesity is a socio-
cultural problem. Given that this is true, mothers’
perceptions of their children’s size could have an
impact on their feeding behavior with young chil-
dren, their motivation to obtain information on
healthy eating and nutrition for the family, and their
encouragement for their children to be more physi-
cally active. Since some mothers of overweight
minority children do perceive their children to be
too heavy when they get to a certain size, it is
important to understand why some parents perceive
their children as overweight whereas others do not.
By better understanding the etiology of cultural
perceptions regarding body size, we will be able to
enhance parental understanding of what overweight
means and what is a desired body size for healthy
children. However, to raise parents’ awareness of
overweight at this time may be somewhat premature
because we currently do not have effective over-
weight intervention programs in the community.
Mothers’ perceptions of children’s body size 101
Acknowledgements
This research was supported by funds from the
United States Department of Agriculture, Environ-
mental Influences on Children’s Food Consumption
Grant No. 2001-35200-10659. Partial support was
received from Dairy Management Inc. This work is a
publication of the United States Department of
Agriculture (USDA/ARS) Children’s Nutrition Re-
search Center, Department of Pediatrics, Baylor
College of Medicine, Houston, Texas, and has
been funded in part with federal funds from the
USDA/ARS under Cooperative Agreement No. 58-
6250-6001. The contents of this publication do not
necessarily reflect the views or policies of the USDA,
nor does mention of trade names, commercial
products, or organizations imply endorsement from
the U.S. government.
The authors wish to thank Sandra Lopez and
Janet Bonner, who were instrumental in the devel-
opment of the questionnaire, and for their help in
data collection. We also thank Pamelia Harris for
help in preparing the manuscript. We extend a
special thanks to Nancy Butte and Ken Ellis for
their help in estimating the BMI of each of the child
silhouette figures.
References
1. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR,
Flegal KM. Prevalence of overweight and obesity among US
children, adolescents, and adults, 1999�2002. JAMA. 2004;/
291(23):/2847�50.
2. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence
and trends in obesity among US adults, 1999�2000. JAMA.
2002;/288(14):/1771�3.
3. Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence
and trends in overweight among US children and adolescents,
1999-2000. JAMA. 2002;/288(14):/1728�32.
4. Flegal KM, Ogden CL, Carroll MD. Prevalence and trends in
overweight among Mexican-American adults and children.
Nutrition Reviews. 2004;/62(7):/S144�8.
5. Koeppen-Schomerus G, Wardle J, Plomin R. A genetic
analysis of weight and overweight in 4-year-old twin pairs.
Int J Obes Relat Metab Disord. 2001;/25(6):/838�44.
6. Maes HH, Neale MC, Eaves LJ. Genetic and environmental
factors in relative body weight and human adiposity. Behav
Genet. 1997;/27(4):/325�51.
7. Fisher JO, Birch LL. Early Experience with Food and Eating:
Implications for the Development of Eating Disorders. In:
Thompson JK, Smolak L, eds. Body Image, Eating Disorders,
and Obesity in Youth. Washington DC: American Psycholo-
gical Association, 2001:23�39.
8. Davison KK, Markey CN, Birch LL. Etiology of body
dissatisfaction and weight concerns among 5-year-old girls.
Appetite. 2000;/35(2):/143�51.
9. Becker DM, Yanek LR, Koffman DM, Bronner YC. Body
image preferences among urban African Americans and
whites from low income communities. Ethn Dis. 1999;/9(3):/
377�86.
10. Contento IR, Basch C, Zybert P. Body image, weight, and
food choices of Latina women and their young children. J
Nutr Educ Behav. 2003;/35(5):/236�48.
11. Kumanyika S, Wilson JF, Guilford-Davenport M. Weight-
related attitudes and behaviors of black women. J Am Diet
Assoc. 1993;/93(4):/416�22.
12. Massara EB. Obesity and cultural weight valuation: a Puerto
Rican case. Appetite. 1980;/1(4):/291�8.
13. Baughcum AE, Chamberlin LA, Deeks CM, Powers SW,
Whitaker RC. Maternal perceptions of overweight preschool
children. Pediatrics. 2000;/106(6):/1380�6.
14. Myers S, Vargas Z. Parental perceptions of the preschool
obese child. Pediatr Nurs. 2000;/26(1):/23�30.
15. Stunkard A, Sorenson T, Schlusinger F. Use of the Danish
Adoption Register for the study of obesity and thinness. In:
Kety S, Rowland LP, Sidman RL, eds. The genetics of
neurological and psychiatric disorders. New York: Raven,
1983:115�20.
16. Anderson CB, Hughes SO, Fisher JO, Nicklas TA. Cross-
cultural equivalence of feeding beliefs and practices: the
psychometric properties of the child feeding questionnaire
among Blacks and Hispanics. Preventive Medicine. 2005;/41:/
521�31.
17. Birch LL, Fisher JO. Development of eating behaviors among
children and adolescents. Pediatrics. 1998;/101:/539�49.
18. Lohman TG, Roche AF, Martorell R. Anthropometric
Standardization Reference Manual. Champaign, IL: Human
Kinetics Books, 1988.
19. Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM,
Flegal KM, Mei Z, et al. 2000 CDC Growth Charts for the
United States: methods and development. Vital Health
Statistics 11. 2002;/246:/1�190.
20. Kramer GH, Burns L, Noel L. The BRMD BOMAB
phantom family. Health Phys. 1999;/61(6):/895�902.
21. Taylor SE. Positive illusions: creative self-deception and the
healthy mind. New York: Basic Books, 1989.
22. Straus M. Measuring families. In: Christensen H, ed. Hand-
book of marriage and the family. Chicago: Rand McNally,
1964.
23. Sherry B, McDivitt J, Birch LL, Cook FH, Sanders S, Prish
JL, et al. Attitudes, practices, and concerns about child
feeding and child weight status among socioeconomically
diverse white, Hispanic, and African-American mothers. J Am
Diet Assoc. 2004;/104(2):/215�21.
24. Strauss RS, Knight J. Influence of the home environment on
the development of obesity in children. Pediatrics. 1999;/
103(6):/e85.
25. Serdula MK, Ivery D, Coates RJ, Freedman DS, Williamson
DF, Byers T. Do obese children become obese adults? A
review of the literature. Prev Med. 1993;/22(2):/167�77.
26. Power C, Lake JK, Cole TJ. Measurement and long-term
health risks of child and adolescent fatness. Int J Obes.
1997;21:507�26, 810�9.
27. Guo SS, Roche AF, Chumlea WC, Gardner JD, Siervogel
RM. The predictive value of childhood body mass index
values for overweight at age 35 y. Am J Clin Nutr. 1994;/59(4):/
810�9.
28. Maynard LM, Galuska DA, Blanck HM, Serdula MK.
Maternal perceptions of weight status of children. Pediatrics
2003;/111(5 Part 2):/1226�31.
102 L. Killion et al.