minnesota society of clinical pathologists … · minnesota society of clinical pathologists annual...
TRANSCRIPT

..
MINNESOTA SOCIETY OF CLINICAL PATHOLOGISTS
ANNUAL TUMOR SEMINAR
November 6, 1976 Minnesota Club, St. Paul
Dr. Wil l iam A. Meissner, Moderator
2S6

CASE 1. 24- yea r - o l d black female wi th a mass in the right thyroid lobe for 2 years . The patien t intermi t tent ly took thyroid medication during this time, On scan, the nodule was cold . T3 and T4 were normal . A total thyroidectomy was performed after a frozen section . The mass in the right lobe measured 4x3x2 em and was poorly circumscribed . (Contributed by Dr. Karl Chen , Minneapolis , Minnesota),
CASE 2. 60-yea-c.- old man wi th soli tary thyroid nodule . A hemithyt'oidectomy was performed . (Con t r i bu ted by Dr. D. J . Nolle t, Hibb i ng , Minnesota) .
CASE 3. 65- year- old Swiss ma n with goi ter for many year s. Recent rapid enlargement of right l obe . A poorly circumscribed hemorrhagic tumor was excised. (Contributed by Dr. w. A. Me issne r , Boston , Massachuse t ts) .
CASE 4. The pati~nt i s a 70- year- o l d d i abetic female who had a lapar otomy sponge left in her abdominal cavi t y at the time of a cholecystectomy in 1955, Twenty years later she under wen t an explora tory laparotomy be cause of an abdominal mass . At surgery a grapefruit si ze mass consisting of remnants of t he s ponge and necrotic debris was r emoved . The surg i cal incision did not heal and the pa t ient continued bleeding from the abdominal wound. She was re-explored t wice and received 25 units of b l ood, cryoprecipitate a nd Vitamin K with no impr ovement in hemostas i s .
On admiss ion to University Hospitals the patient was bleeding profusely. Her BP was 126/70 and p~lse was 120/min. Other pertinent physical findings included bronchial breath sounds at bo t h bases and peda l edema.
Admi ssion lab studies revea led: hemoglobin 8.7 , wh i te blood count 11;500 with 90% neu t r ophil s , platele ts adequa t e , BUN 7, Creatinine 0.7 , Prot i me 12 . 0, partial thromboplas tin t i me 32.1, and thrombin t i me 19. 2 with control of 14, 7.
The pa t ient was re- exp l ored twice in an attempt to obta i n hemostasis . Dur i ng the second proceaure a t umor mass was removed from the upper anterior abdominal wall . She continued to deteriora te , developed r espiratory distress and hypotension and expired 5 weeks ~fter admi ss i on. (Contribute d by Dr. Leanne Peterson, Minneapolis, Mi nnesota) .
CASE'S , A man, _age 51 , had had an inconspicuous pigmented skin lesion on his left lower eyelid for s e veral years . Recen tly the lesion had enlarged, unde r gone superficial ulceration and exhib i ted a firm nodu le in its center. (Contributed by Dr . Ellias Manoles , Me t hl list Hos pital, St . Lo uis Park, Mi nnesota) .
CASE 6. 50- year- old whi te fema le with history of trauma to her left face 9 mon ths PTA. Four months PTA developed a "toothache " in her left upper alveolar ridge. The patient had sinus sur gery 17 year s ago . Physical examination revealed a smooth mass visible under the left infe r i or turbinate and in the upper alveolar ridge extending to the piriform apperture. The remainder of the examination was unremarkable and the laboratory results were within nor ma l limits. X- ray films showed a premaxillary cystic lesion with a tooth at its edge. I t was easily shelled out at surgery. Grossly , the specimen consisted of an ovoid 3 em cyst ic f ragment of sof t tissue covered on one aspect by mucous membrane and con taining a tooth, (Contributed by Dr . Robert A. Vickers, Minneapolis , Minnesota) .
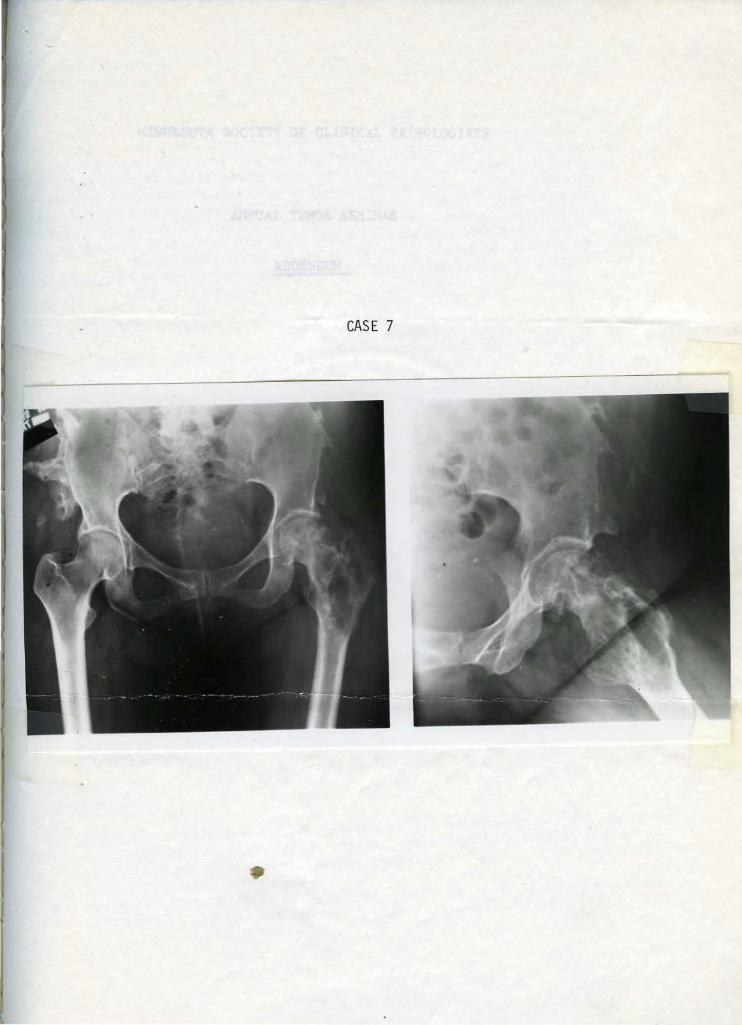
CASE 7. This 50- year- old woman had curettage and graft of an upper femora l lesion on 7- 22-and again, for r ecurrence , in April, 1972 . She presented at Mayo Clinic and hao 14 . 5cm of upper par t of femur r esected on 3- 16- 71 . (Contributed by Dr. D. C. Drthlin, Mayo Cli nic, Rochester, Minne sota) .

CASE 8 . A woman, age 64, had leukopenia (2100 WBC - 65% lymphocytes). No anemia or thrombocytopenia . The patient had hepatosplenomegaly and a skin rash. Skele ta l x-ray revealed mye losclerosis . A laparotomy was done for a non- functioning gallbladder . A lymph node was biopsied . (Contributed by Or. Louis H. Weiland, Mayo Cl in ic , Roches ter , Minnesota ) .
CASE 9. A 72- year- old woman compla ined of psoriasiform, on her abdomen. She was treated with topical s tero i ds. "flared" and she developed generalized lymphadenopathy. Meissn~r, Boston , Massachusetts) .
erythematous , non- tender plaq ues Some months later the lesions (Contributed by Dr . W. A.
CASE 10. A 10-year- old girl with chronic anemia since age five years. She had an extensi work-u~ for hypochromic ~icrocytic anemia which is refractory to iron , folic acid and prednisone . She has been small fo r her age all her l ife and is the smal l est gir l in ~er school class . Weight 45 pounds, height 46~ inches.
On physi cal examination she had normal proportions of a "primordial dwarf . '' There was no adenopathy or hepatosplenomega ly. RBC - 3. 93, Hg; - 7.8, slight elevation of serum gamma globulin .
At exploratory laparotomy, surgeon noted - - "To our delight we palpated a 3x4x5cm mass in the gastrolienal ligament" which was carefully removed from its close adherence to the pancreas . (Contributed by Dr. E. G. Harrison , Mayo Clinic , Rochester, Minnesota) ( deceased).
CASE 11. A woman~ age 25 , was found to have a palpable breast mass. Mammogram revealed an area of calcification. (Contributed by Dr. Thomas A. Gaffey, Mayo Clinic, Rochester, Minnesota).
CASE 12. ·sa-year- old male wi t h lumbar pain, weakness and weight loss . Laparotomy reveale< a lar ge tumor mass replacing the left adrenal g land. An adrenelectomy and nephrec tomy were performed. Grossly, the tumor measured 7 em and was found spl it ting t he shea ths of the adrenal. It was solid, yellowish, with areas of hemorrhage . The kidney was not involved ~y tumor . (Contributed by Dr. Ronald Villella, Minneapolis , Minnesota ) .
CASE •13. A 35- year- old man with right lower quadrant pain for one year was found on I V pyelogram to nave a large retroperitoneal tumor on the left s ide. There was also an osteolytic lesion in the 12th vertebra. A lOcm encapsulated tumor was removed from the lef t 1drenal . Four months later patient had recurrent abdominal pain. A calcification was found by x- ray in the region of the right adrenal . 17- hydroxy corticoid and 17-~etos teroid values were slightly elevated. A 4cm cyst with some calcifi cation was removed f rom the right adrenal, and a vertebra l biopsy was performed. Postoperatively the adrenal function tests continued to be slightly elevated. (Contributed by Dr. W. A. Meissner, Boston , Massachuse tts).
CASE 14. 33- year- old female with pelvic mass . At operation , one ovary was enlarged (5 . 5 in greatest diameter) and partially repla ced by a single , solid yellowi sh- white spherical mass of firm cons istency measur i ng 2. 5 em in greatest diameter . (Contributed by Dr. AbeL. Fox, Jr . , Minneapolis, Minnesota).
CASE 15 . 19-year- old male with a large anterosuperior mediastinal mass . There i s no evidence of tumor elsewhere or of metastas es . The t umor weighed 400 gm and meas ured 12x8x6 em. It was encaps ulated. The cut surface had a grayish-white mot t led appea rance , with areas of necrosis and hemo rrhage . A few cys tic caviti es were pres en t , th~ lnrg~ s t me asur ing 2cm. The con~istency o f lh C' tumo r wl'l s so fl. ( Contributed hy Dr. l{ol>C' rl W. Weber , Minne apolis, Minnesot a) .

t ... .. •
USE 16 . A woman, age 45, comes with an enlarging, asymptomatic nodular density in her left lower lobe: Three months ago the lesion was first noted on a routine chest x-ray. ~he lesion has enlarged during the past 3 months . (In retrospect , the lesion was present ll months prior to admission). Two closely related nodules 2.5 and 2 em in diame ter were excised . (Contributed by Dr. E. H. Soule, Mayo Clinic , Rochester, Minnesota).
USE 17 . 45- year- old white male with past history of renal lithiasis and perforated duodenal ulcer . He now presents with sudden onset of severe abdominal pain. X-rays showed marked thickening of gastric rugal folds and deformation of the duodenal bulb with a lcm ulcer crater. Laboratory data: serum calcium, 10.9 to 11.9 mg/dl; serum phosphorus, 2. 2 to 2.6 mg/dl; serum parathyroid hormone, 2.0 ng/ml (normal: 0 to 1.5 ng/ml with normal serum calcium levels); serum gastrin , 2,554 pg/ml (normal: up to 300 pg/ml) . Gastroscopy revealed markedly enlarged rugae with active ulceration in a pattern suggestive of Henetrier's disease. A total gastrectomy was carried out. The stomach wall was markedly thickened (0 . 6 to 4.5 em) • . The mucosal surface bore numerous superficial ulcers . On cross section, ill- defined whi tish nodules were present in the gastric wall. (Contributed ~yDr. John Kyllo, Minneapolis , Minnesota) .
CASE 18. 40-year•old male with clinical pic ture of acute appendicitis. An appendectomy was performed. Grossly, the appendix was enlarged and indurated, with a reddened serosa . (Contributed· by Dr . Juan Rosai, Minneapolis, Minnesota).
~E 19 . A woman, age 39 , experienced the onset of hematuria following an episode of straining to force open a stuck elevator door. Bleeding continued, sometimes with clots, but there was ~o dysuria. Past history was negative. BP 136/78. Urograms revealed a fundal filling defect. A segmental resection was done . (Contributed by Dr . G. J. Obert , Fargo, North Dakota).
CASE 20. A 59- year-ol d woman was admitted for abdominal pain (5 mos.) and a rapidly enlarging liver (2 mos . ) . Liver studies had been performed 25 years previously for "an enlarged liver" bu t no details were available. An exploratory laparotomy was carried out with biopsy of a large liver mass. Patient deteriorated rapidly with ascites and liver failure and died a few weeks postoperatively . (Contributed by Dr. W. A. Meissner, Boston, Massachusetts) • .
CASE 7

MINNESOTA SOCIETY OF CLINIC~L PATHOLOGISTS
ANNUAL TUMOR SEl'!:~AR
ADDENDUM
November 6, 197c Minnesota Club, St. ?aul
Dr. William A. Meissner, ~oderator

CME l
The patient was a 24-year-old woman with a thyroid mass for 'two years. A total thyroidectomy was performed. The mass in the right lobe measured 4 x 3 x 2 em. and was poorly circumscribed.
Microscopically the mass has a rather uniform pattern throughout with the formation of small follicles filled with colloid. The epithelial cells lining the ~ollicles are, for the most part, also uniform. At times they are flattened and other times they are cuboidal or columnar. A frequent feature of the epithelial cells is the_presence of pale, "see-through" nuclei which sometime~ appear to be arranged in layers . There are no mitoses. A few of the epithelial cells form abortive papillary processes. In the cen'tlral portion of the mass there is some old scarring. Some of the mass is well circumscribed; in other areas it is poorly demarcated and seems to infiltrate directly into the adjacent thyroid without any encapsulation . I found no vascular invasion.
Diagnosis: Papillary carcinoma.
DISCUSSION: This is a rather typical microscopic appearance of one of the variants of papillary carcinoma in which the papilliferous processes are not well developed and in which there is a considerable amount of follicle formation. It is ~w appreciated that mixed papillary and follicular carcinomas, ~ch as th'!s, have a prognosis and clinical behavior, for the most part, like pure papillary carcinomas. There is a suggestion, however, that such mixed .umors with a predominance of follicular elements have a slightly better prognosis. The presence ~f see-through nuclei in papillary tumors is common and has even been used ·as a diagnostic characteristic of papillary carcinomas . The tumor in the Seminar section shows definite, but limited invasion of the adjacent thyroid.
There are many facets of papillary carcinoma that are interesting for discussion, but here I would like to mention briefly some prognostic studies we have recently completed on differentiated thyroid cancers. Although it is well appreciated that both papillary and follicular carcinomas ("differentiated' tumors ) have as a group a good prognosis, some patients do die of the disease; it is important, therefore, to recognize any h-istologic or other features of such tumors which imply a poorer prognosis so that more aggressive treatment may be carried out. In addition to the histologic type, the following features are associated with a poorer prognosis: older age ; male sex ; extension of tumor beyond thyroid capsule; large tumor; blood vessel invasi on; multiple intraglandular foci of tumor; and distant metastases. The presence of lymph node metastases does not worsen the prognosis in differentiated tumors of the thyroid.
REFERENCES :
1. Cady, B., Sedgwick, c. E., Meissner, w. A., Bookwalter, J. R., Romagosa, V. and Werber, J. : Changing clinical, pathologic, treatment and survival patterns in differentiated thyroid carcinoma. (To be published, Annals of Surg. , Nov . , 1976. )
2. Woolner, L. B., Beahrs, 0. H., Black, B. M. et al.: Classification a.nd prognosis of thyroid carcinoma . Am. J . Surg. 102:354-387, 1961.

The patient was a 60-year-old man with a solitary thyroid nodule. A '-i thyroidectomy was performed.
Microscopically the tissue shows a nodule with a very small portion of its capsule which appears to be intact. The nodule is composed of a ass of small follicles , some of which are so small as to have· no colloid. !here are no normal or oversized follicles. The microfollicular portion in 101118 foci shows almost a complete absence of follicle formation with the cells growing in solid clusters or masses. The cells have small, dark nuclei which are rounded' and which show only an occasional mitosis . There are no papillary foci. I found no vascular invasion or capsule invasion, but the small amount ~capsule that · s present is inadequate for true evaluation.
Diagnosis: Follicular carcinoma of thyroid with poorly di.fferentiated foci.
DISCUSSION: There really is an insufficient amount of capsule around this thyroid nodule to evaluate adequately the presence or absence of inva-sion. In a microfollicular tumor of this type, it is imperative to examine a.t least a half dozen blocks, preferably of capsular area where both vascular and capsular invasion are best identified before one can be reasonably sure that invasion has been excluded. My diagnosis is , therefore, not based on my findjng invasion, but on my strong suspicion that additional sections \IIIOuld show it in th.is particular type of lesion. The microfollicular portion of this tumor may represent a transition from a better differentiated carcinoma. Many have suggested that with passage of time the well differentiated carcinomas of the thyroid may become increasingly undifferentiated and more malignant. An interesting feature of this case is the resemblance of some of the more solid follicular foci to lymphoma, and it is possible that some of the cases of thyroid lymphoma that have been reported would be found to represent poorly differentiated carcinoma if more sections had been studied. The incidence of small cell carcinoma of the thyroid, which actually represents an undifferentiated follicular carcinoma, is not common in the United States, but is quite common in some parts of Europe. One report of over 1200 cancers of the thyroid found that small cell carcinomas made up over 20 per cent of all thyroid cancers. Th~ value of a uniform classification of thyroid cancer, such as provided by the WOrld Health Organization, will help considerably in evaluating geographical differences in the respectiv e types o f thyroid cancer.
REFERENCES :
1. Meissner, w. A.: Undifferentiated carcinomas of the thyroid. International Onion Against Cancer, Monograph Series 12, Berlin, Springer. 1969, pp. 36-43.
2.. World Health Organization. Histological Typing of Thyroid Tumours, iHl , Geneva.

CASE 3
The ·patient was an elderly Swiss man with goiter for many years. There was recent enlargment of the thyroid, and a poorly circumscribed hemorrhagic, cystic tumor was excised.
Microscopically the lesion is characterized by sinus-like clefts of varying size which are lined by tumor cells simulating endothelium. In some parts ~f the tumor, the sinus-like clefts certainly resemble vascular spaces, and t.~e tumor cells greatly resemble endothelium. In other parts of the tumor, · the lesion is less cellular and contains considerable collagen. The reticulum stains show a considerable amount of irregular network , usually surrounding clusters of cells, rather than individual cells. In a few foci the cells suggest anaplastic carcinoma.
Diagn! sis : Malignant hemangioendothelioma.
DISCUSSION: I included this case in the seminar specifically because it is such an interesting lesion--seldom seen in this country, but frequently seen in Switzerland. Drs. Hedinger and Egloff, who have written about this particular leS!ion, have furnished the material for the seminar. The lesion, ,..,.hile rare in this country, makes up 10 to 15 per cent of all thyroid cancers in Switzerland . This tumor, which has been called hemangioendothelioma by the S\ltiss pathologists, occurs almost exclusively in older individuals of either sex . The patient characteristically has a goiter for a long period o f time witm sudden, rapid growth. The tumor is characteristically hemorrhagic as are the metastases that are common in the lungs: metastases also may be found in lymph nodes and elsewhere. The clinical course is rapid, the prognosis is very poor.
The nature of the lesion allows considerable speculation. In 1909, Iiedinger, Sr. , first described the lesion and believed it to be a malignant tumor of endot.~elium . Since then, others have suggested that it might arise from the fibrocytes of the adventitia or that it might represent an angieplastic reticulum cell sarcoma. Still o thers feel it most likely represents· an anaplastic carcinoma, and this is my personal feeling. Why the lesion is not seen more frequently in this country is also unknown. I have seen only one case in Boston material. I do think it is important to emphasize, as the Swiss pathologists have done, that the . t umor is one with a distinctive and constant histologic pattern, and I agree with them that it is not difficult to recognize. It is for this reason that the term has been included in the w1i0 classification, although everyone, including the Swiss, realizes that t.'1e term may prove to be the incorrect one for what is, nevertheless, a recognizable histologic entity.
REFERENCES :
l. Egloff, B. : The. Hemangioendothelioma. Thyroid Cancer. International Union Against Cancer, Monograph Series, Vol. 12, p. 52, Springer-Verlag , Berlin-Heidelberg-New Y.ork, 1968 .

CASE 4
The. patient was a 70-year-old diabetic woman with a long, unfortunate history of numerous laparotomies, including removal of a retained foreign body from one of the operations. Ultimately the patient had a tumor mass removed from the upper anterior abdominal wall.
Microscopically the tumor mass is a highly vascular one which extends into · the fibrous tissue, muscle and fat of the abdominal wall. The vascular channels of the tumor are anastomosing, but irregular in size and shape and are lined in part by relatively no:rma.l appearing endothelial cells, but, for the most part, of endothelial cells which are · swollen, irregular and often have ·an epithelial appearance. The nuclei of such cells are often bizarre, and some show mitoses. The endothelial cells at times form masses that grow into the_tumen of the vascular spaces. The vascular spaces are outlined particul:rrly well by the silver stain. Some of the endothelial cells contain pigment, and this pigment, presumably hemosiderin, is scattered throughout the entire tumor.
Diagnosis: Malignant hemangioendothelioma (angiosarcoma).
DISCUSSION: The differential diagnosis in this instance must include, in addition to hemangiosarcoma, an organizing, proliferating granulation ti~S\le which I believe can be excluded by the severe atypia of the vascular spaces and of the endothelial lining cells. Another consideration would be a mesotilelioma which sometimes can be quite vascular and form spaces,_ but the localized nature of the lesion in itself probably is sufficient to exclude mesothelioma; if the mesothelioma were of this size and degree of malignancy , it should have spread further throughout the abdominal cavity . The abnormal endothelial cells certainly resemble epithelium in some foci, but i n other places there . are clear transitions to endothelium; and an epi t.~elial neoplasm, such as a renal cell carcinoma, does not, therefore, need to be seriously considered. The terminology of these tumors has been gradually standardized, and the WHO term is malignant hemangioendothelioma, rather than angiosarcoma .
The relationship of this tumor to the patient's numerous operations, the foreign body and ~~e very severe anemia are a little difficult to fit together . . ' into one clear picture. One can see why her anemia should have been so ex-treme. with extensive bleeding. I think it is quite possible that the vascular tumor may have spread rather extensively and that there i s more than just that present as an anterior abdominal wall mass.
REFERENCES:
l. Kau£fman, S. L. and Stout, A. P. : Malignant hemangioendothelioma in infants and children. cancer !!:1186-1196, 1961.

CASE 5
A 61-year-old man had an inconspicuous pigmented lesion on his eyelid for several years. Recently the lesion enlarged and ulcerated, showing a firm nodule in its center.
Microscopically the epidezmis is indeed ulcerated over the central portion of the subcutaneous and deJ:ma.l mass. At one focus in the epidermis there is a small accumulation of highly pigmented cells and some j unctional neval changes. Whi~e one or two of these neval cells show hyperchromatism, I found -no mitoses and really very little atypia of these cells. The pigment in this area, presumably melanin pigment, extends for a very short distance down into the dermis. There are no other evidences of neval change in the remaining epidermis, and I found no melanin pigment at any point in the deeper structures other than as just mentioned. The bulk of the mass involving both dermis and fubcutaneous tissues is composed of cells with irregular outlines that vary considerably in size and shape . Some are almost without outlines and are more like syncytial cells . The nuclei of these cells a~so vary considerably in size and shape. Some are quite abnormal, and mitoses are relatively frequent, including atypical mitoses. These cells have an intimate relationship with spindle cells and collagen which is present in varying degrees throughout the 'entire lesion. Some of the cells have a foamy cytoplasm. There are a few infl~tory cells around the periphery of the tumor . The tumor surro~s nerves and skin appendages and is poorly demarcated. I found no multinucleated giant cells, and I found no storeiform pattern arrangement of the cell~ of the mass.
Diagnosis : Mal..ignant fibrous histiocytoma with pigmented nevus •
DISCUSSION: The differential diagnosis in this- instance is between a malignant fibrous histiocytoma and a desmoplastic ~ignant melanoma. I think this tumor is definitely malignant because of the presence of the numerous mitoses, often atypical, and the pleomorphism of the cells-~ The intimate relationship of the cells, which I am assunri-~g to be histiocytes, and the stroma is a strong point in favor of its being a malignant fibrous histiocytoma, although I could find no storeiform pattern and no multinucleated giant cells . I found no pigment other than a sma~~ amount adj acent to the nevus in any· part of the lesion. It is always difficult to make the diagnosis of malignant melanoma without f-inding some me·lanin pigment. This tumor is a superfi cial one and is arisL"lg in the dermis and subcutaneous tissues. Such superficial malignant fibrous histiocytomas have a much lower malignant potentia~ than a c omparable tumor arising in the deeper tissues.
REFERENCES :
l. Soule and Enriquez: Benign and malignant histiocytoma. Cancer l£: 1 28, 197 2 •

'
CASE 6
The patient was a SO-year-old woman with a history of trauma to her left face. x-rays showed a pre-maxillary lesion with a tooth at its edge. The lesion shelled out easily at surgery and consisted of an ovoid, 3 em. cystic fragment of soft tissue containing a tooth.
Microscopically there is a mass of ep~thelial tissue on the inner cyst wal.l ·wi ~ the epithelial cells growing in several patterns • In some foci the pattern is cribriform; in others it is rather solid with spindle-shaped cells · between which there is hyal·in deposited in the stroma. In still other areas, the epithelial cells are cuboidal or columnar and often form ductlike 'structures <?Ontaining eosinophilic material. Between some layers of epithelial cells, there is l?AS positive material. In the fibrous tissue of the cyst ~1, there are some strands of odontogenic epithelium. No mitoses are evidel!t :in any of the epithelial cells.
Diagnosis! Adenomatoid odontogenic tumor (adenoameloblastoma) .
DISCUSSION: The older name for this rare tumor was adenoameloblastoma, but since the lesion is not an amelobl astoma, the terminology is :inappropriate. Abrams et al. have suggested the term "adenomatoid odontogenic tumor," a term that has been accepted in the WHO Classification. The lesion really does not muC'h .resemble an ameloblastoma. and certainly does not have the latter's potential for local invasion and recurrence. In a review (67 cases in the English literature) by Abrams, he was unable to find a single instance of recurrence of this lesion, even with conservative or incomplete excision. It has been suggested that rather than being a neoplasm, the lesion is more likely a hamartoma. Whatever the nature of the lesion, it :is most commonly seen in the cuspid area of tr~ maxilla where it presents as a cystic, encapsulated mass, usually associated with an unerupted tooth.
Microsco~ically the tumor consists of odontogenic epithelium with ductlike structures and various other patterns. Calcification is often present'· although not seen :in the Seminar slide. The only unusual feature in the Seminar case is the fact that the patient was SO years of age when the lesion was diagnosed; most adenomatoid odontogenic tumors occur in the second decade. The oldest patien~ in Abrams' review wa.s 48 years.
REFERENCES :
1. Abrams, A.M., Melrose, R. J. and Howell, F. V. : Adenoameloblastoma. Cancer 31:l75-18S, 1968.

CASE 7
The patient was a SO-year-old woman with a lesion of the upper femur which was curetted and gra£ted in 1970 and again for recurrence in 1972. One year later she apparently had another recurrence, and the upper part of the femur was resected.
A photograph of two x-rays of the lesion, presumably the last recurrence, shows a fusiform swelling of the entire upper femur, including the head, with a mottled, vacuolated appearance. The periphery of the expansile portion ·is surpr isingly sharp. There is no evidence of Paget's disease, but ther·e are mul. tiple, ·irregular extrusions from the pel vic bones •
'
The microscopic examination shows, as the predomj nant finding, a proliferation f fairly well differentiated cartilaginous tissue which, in many places, has foci o£ enchondral ossification. The cartilagino~ cells are arranged in solid masses with irregular outlines. The individual cells are often almost normal appearing, but some show plump, irregular nuclei, sometimes two nuclei, but no mitoses. In some foci of the lesion, there are scattered mul. tinucleated giant cells, but these are not numerous. There is new bone formation in some areas in addition to the enchondral ossification, but the new bone fo:r:mation shows no:r:mal appearing osteoblasts and suggests repair, rather than neoplasm. In still other foci, there are vascular spaces of various size within the cartilaginous overgrowth. I had two sec'Q.ons to study, one from the femoral. head and one from a trochanter; both sl'iow the cartilaginous proliferation. The periphery of the lesion, as in the x- ray, is sharp with a thinned, but not invaded she:ll of cortical bone.
Diagnosis: Low-grade chondrosarcoma.
DISCUSSION: This is a large cartilaginous lesion in, an adult and , therefore, must be suspected of being malignant. The fact that it has recurred three times and necessitated a wide resection is further evida~ce of its lowgrade malignant potential. The individual cartilaginous cells are fairly well differentiated and do not suggest rapid growth rate ; mitoses are absent although some cells and nuclei are atypical . The considerable amount o f ne~
bone formation independent of the cartilage cells I interpret as reactive new bone secondary. to the two previous curettages and grafts which make the lesion 'difficult to interpret, both from the radiologic and the pathologic point of view. Since the patient has other bone lesions by x-ray, I think tbis is an instance of chondrosarcoma arisin~ in multiple osteochondromatosis. About 10 per cent of chondrosarcomas are said t o arise from osteochondrosarcomas.
REFERENCES :
l. Henderson, E. P. and Dahlin, D. C. : Chondrosarcoma of bone . J. Bone Joint Surg. _!2 :1450-1458, 1963.

CASE 8
This was a woman, 64-years old, with leukopenia, hepatosplenomegaly and a skin rash. She also had myelosclerosis. A lymph node was biopsied, apparently as an incidental finding during a laparotomy for a cholecystectomy;
Microscopically the tissue is a lymph node which is well circumscribed and stil~ shows some residual peripheral sinuses. The node is rather diffusely infiltrated by a mixed cellular population. Most of the nodal architecture is not destroyed, and germinal follicles are still identifiable. The cellular infi~trate at times is associated with a considerable amount of fibrosis either in sheets or in nodules. The in£iltrate itself a~so presents in sheets or in nodules. The individual cells of the infiltrate consist of eosinophils, plasma cells and histiocytes, but predominantly of a cell larger than a lymp.Pocyte and with a pale, non-granular cytoplasm. There are no mitoses in 'bese latter cells. With giemsa stain, such cells show varying numbers of cytoplasmic, dark granules and many are quite typical of mast cells.
Diagnosis : Mastocytosis •
DISCUSS~ON: The lymph node 's architecture is not destroyed, but rather diffu.sely infiltrated by sheets and cords of cells. Without the giemsa stain it is not possible to identify well the type of cell , but with the giemsa stain or toluidine blue, the cells are clearly recognizable as mast cells. Mastocytosi~ is a systemic variant of urticaria pigmentosa in which the liver and sp+een are usual~y enlarged along with lymph nodes. Systemic mastocytosis is a rare disease. It may have a benign or malignant course. The patient in the Seminar case had skin rash, but systemic mastocytosis may occasio~ly occur without skin involvement. The tissues usually involved when the disease is systemic are: bone (a few instances of sclerosis of bone have been reported, as in the Seminar case); hematopoietic system; lymph nodes; liver; and spleen. Patients may die from the disease. Most deaths occur within two years of onset of the disease.
REFERENCES :
1. Sagher, F. and Evan-Paz, Zvi: Mastocytosis and the mast cell . Year Book Publishers, Chicago, 1967.

CASE 9
This was an elderly woman who complained of a skin rash which was treated with topical steroids. Some months later the lesions flared and, at the same_ time, she developed lymphadenopathy.
Microscopically the slides ~how a moderately enlarged lymph node diffusely involved with a pleomorphic cellular infiltrate. In many places the capsule of the node is respected, but in some foci the infiltrate extends beyond the node into the adjacent fat. Some of the nodal ar:chi tecture appears to be effaced while other portions of it remain, but nevertheless are infiltrated with the pleomorphic cells. Eosinophilia in the infiltrate is prominent; but, in addition, there are histiocytes , lymphocytes and numerous bizarre cells, some with irregular nucl,ei, which are difficult to classify. There are no Sternberg cells. ThE:'!e is only a minimal amount of pigment found.
Diagnosis: Mycosis fungoides involving lymph node.
DIAGNOSIS: The diagnosis of mycosis fungoides in a lymph node is an extremely diffi:,cult one. Some have suggested that it usually can only be made morphologically on a presumptive basis. The differential diagnosis of the lymph node in this instance includes dermatopathic hyperplasia which would seem to be excluded by the lack of pigment and by the extreme pleomorphic' infiltrate. A second possibility is Hodgkin's disease because of the n9-ture of the infiltrate and the eosinophilia, but there are no typical Reed-Sternberg cells. A third alternative in a patient with a skin rash is mycosis fungoides. The pleomorphic infiltrate is good for this diagnosis, and there are some peculiar cells with hyperchromatic, irregular nuclei which have been called by some mycosis cells. Some have stated that such cells must be in clusters before the diagnosis of mycosis fungoides can be made. In any event, it remains a difficult diagnostic problem without additional information which we, fortunately, have. in this case. A short time before the lymph node was biopsied, the patient had a biopsy of the skin rash which showed the dermal mycosis fungoides infiltrate including the Pautrier's intraepidermal abscesses.
Mycosis fungoides may involve viscera, particularly lymph nodes, spleen and liver, but the diagnosis by light microscopy is often a difficult one, even in a known case such as this. The resemblance of the atypical mono-_, nuclear cells of mycosis fungoides to Sezary cells has been emphasized with the suggestion that both have the characteristics of T cells and that the S~zary syndrome is a peripheral blood manifestation of mycosis fungoides.
REFERENCES:
l. Rabinowitz, B. N., Noguchi, S. and Roenigk, H. H., Jr.: Tumor cell characterization in mycosis fungoides. Cancer l!:1747-1753, 1976 .
2. Long, J. C. and Mihm, M. C. : Mycosis fungo ides with extracu taneous dissemination: A distinct clinicopathologic entity. cancer 34:1745-1755, 1974.
3. Variakojis, D., Rosas-Uribe, A. and Rappaport, H.: Mycosis fungoides : pathologic findings in staging laparotomies . Cancer ~:1589-1600, 1974.
CASE 10
The patient was a 10-year-old girl who presented with chronic anemia and dwarfism. At exploratory laparotomy the surgeon was delighted to find and remove a 3 x 5 em. mass from the gastrolili'eal ligament.
Microscopically the tissue is a lymph node which is well circumscribed. The architecture is not effaced. The node is characterized by prominent ge.rmi..nal centers which, while not unduly large, nevertheless have a peculiar appearance suggesting a splenic follicle or even Hassall's corpuscles. Some of the follicles have a vessel extending into them surrounded by a small aJIX)unt of hyaline material. The interfollicular substance of the node also shows increased vascularity and is characterized particularly by various sized sheets composed almost purely of plasma cells • .
Diagno~: Angiofollicular lymph node hyperplasia (plasma cell variant) •
DISCUSSION: This case was reported in the Mayo Clinic Proceedings in 1975. In 1956, Dr. Castleman reported 13 cases of an unusual hyperplasia of mediastinal lymph nodes resembling thymoma. In fact, two of the cases had previously been reported as thymoma. Microscopically the nodes were characterized by hyperplasia of· the lymphoid follicles, plus a capillary proliferation and endothelial hyperplasia with the capillary proliferation sometimes extending into the follicles. Since that time additional cases were reported, and there wa$ an excellent review paper by Dr. Harrison in 1963. In 1972, Keller et al •. reviewed 81 additional cases plus those reported in the literature and defined two types of giant lymph node hyperplasia. The first, making up ov~ 90 per cent of all the cases, was the hyaline vascular type with prominent follicles and interfollicular capillary proliferation. This type was rarely accompanied by any systemic symptoms. The second type, while similar, was composed of larger follicles and, in addition, showed interfollicular sheets of plasma cells • In this plasma cell variant, there were numerous systemic manifestations, including fever, anemia and various types of hyperglobulinemias. The lesions were not limited to the mediastinum, but were seen elsewhere as well. Removal of the node resulted in complete cure of the symptoms. In the Seminar case it is stated in the publication that the anemia r~tted, and the patient grew 6 em. in 8 months.
The nature of the peculiar lymph node derangement is still unknown and controversial. Although most of the nodes have been large--up to 16 em. in diameter--some of them have been relatively small so t."le term giant lymph node hyperplasia is not always appropriate . A.ngioinvasive hype.rplasia seems to be a good descriptive term for the disease. Some have suggested that the process represents a tumor, others a hamartoma, but the concensus at the moment is that it represents an inflammatory and reactive change due to unknown causesj ~have pointed out the resemblance to rheumatoid lymph nodes. Why the plasma cell variant should be associated with anemia and dysglobulinemia is still to be evaluated.
REFERENCES :
1. Burgert, E. o., Jr., et al.: Intra-abdominal, angiofollicular lymph node hyperplasia (plasma-cell variant) with an antierythropoietic factor. Mayo Clin. Proc. 50:542-546, 1975.
2. Harrison, E. G., Jr. and Bernatz, P. E.: A.ngiofollicular mediastinal lymph-node hyperplasia resembling thymoma. Arch. Path. 12..: 284-292, 1963.
3. Keller, A. R., Hochholzer, t. and Castleman, B.: Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer ~:670-683, 1972.

CASE ll
The, patient was a 25-year-old woman with a palpable breast mass. Mammogram r~vealed an area of calcification.
" Microscopically there is a rounded mass about 1 em. in diameter
that is not encapsulated, but is nevertheless well delineated from the adjacent 'breast tissue. While there are a few stromal elements, most of the mass is composed of epithelial cells which, for the most part, are arranged in small follicles. The cells have an acidophilic cytoplasm which is often vacuolated. The nuclei are reqular and there is only a rare m.i tosis. The lumens fo.rmed by the epithelial cell contain PAS positive material which does not disappear after diastase. The adja~t breast tissue shows no changes except for slight vacuolization of some of the epithelial cells. In one small focus of the nodule, there is dark staining material, possibly calcium.
Diagnosis~ Pure (lactating) adenoma.
DISCUSSION: There are several categories of breast adenomas such as the fibroadenoma and the nipple papilloma. Both of these, however, con-tain a considerable amount of stroma, and there is another type of adenoma, oftan called "pure" or true adenoma which is a circumscribed lesion with very little stroma. The pure adenomas , again are broken down into several sub-groups--the most common of which are tubular and lactating. All pure adenomas occur, for the most part, in young •..romen; and the !acta ting adenomas perhaps merely represent a variant of the tubular adenoma in a pregnant woman. The secretory activity of the cells in the nodule as well as the adjacent breast tissue both suqqest pregnancy in the Seminar case.
Pure adenomas are thought by some to be merely hyperplasia, but in any event they should not be confused with carcinoma. It is true, however, that an occasional carcinoma has been thought to arise from a pure adenoma. Contrary to an opinion at one time, there does not seem to be a proven relationship of the pure adenomas with oru contraceptives.
REFERENCES :
L Rertel et al. : Breast adenomas. Cancer 37: 2891, 1976.

CASE 12 .·;
The patient was a 58-year-old man admitted with lumbar pain, weakness and weight -loss . A large tumor was removed from the region of the left adrenal gland. The kidney was not involved.
Microscopically the slide shows some normal adrenal gland adjacent to a large · mass of tumor tissue. The tumor lies adjacent to the adrenal cortex and does not show an intimate association with it, but rather seems to be compressing it. In addition, there is some normal adrenal medulla which ·shows a much more intimate relationship with the underlying tumor mass and actually seems to send a few cords of medullary tissue into the tumor ma'ss. The cells of the tumor are quite varied in size, shape and gen~ appearance. Some of them are quite large and resemble ganglion cells, both in their size an<i their configuration. Some of these cells seem to have processes extending from them. Nissl stains failed to identify any Nissl substance. Other of these cells are more syncytial; still others have a basophilic or an acidophilic cytoplasm and many contain rather large droplets of pink-staining material. While the nuclei are often large and contain a prominent nucleolus, I failed to identify any mitoses. Some of the cells are arranged around blood vessels and have an intimate process relationship with such vessels. The overall appearance is that of extreme va=iability, both of cell and nuclear size and arrangement.
Diagnosis: Pheochromocytoma.
DISCUSSION : The differential diagnosis on a lesion of this type includes renal cell carcinoma and adrenal cortical carcinoma as well as pheochromocytoma. We are told that grossly the kidney was not involved with tumor so I believe it is reasonable to exclude this from the differential diagnosis. The differentiation of pheochromocytoma from adrenal cortical neoplasm is often a very difficult one. Factors that seem to be of assistance in making such a distinction are the variable size, with polyhedral shapes, of the cells in the pheochromocytoma along with complete absence of mitoses. Sherwin .in his extensive study of pheochromocytomas emphasizes the tumormedulla continuity, as is seen in the Seminar case, as being one of the more important factors in establishing the diagnosis. He also emphasizes tumor and medullary cell similarity , which I think we see in this case. Other points that he mentions which are also seen here include tumor cell mosaic pattern, cytoplasmic pools or lakes, droplet formation, and the absence of mitotic figures . Feta.l fat had been mentioned as being rather common in cases of pheochromocytoma. I did not identify any in my single section of the tumor.
The diagnosis of pheochromocytoma, while difficult from histologic examination alone, should be an easy one with appropriately fixed tissue and subsequent stains. Demonstration of chroma.ffin material is quite easily done on the fresh specimen and can also be carried out with numerous stains on a specimen fixed in chromic acid solutions, such as Zenker's.
The distinction between malignant and benign pheochromocytoma is an extremely difficult one, and for practical purposes can be made only by the finding of metastases.
REFERENCES :
L Sherwin, Russell P.: Histopathology of pheochromocytoma. Cancer 12 : 861-877, 1959,

CASE 13 ·". '
This 35- year-old man complained of abdominal pain and was found to have a 10 ~. encapsulated tumor which was removed from the region of the left adrenal. An osteolytic lesion was noted in the 12th vertebra. Four months later, the patient had recurrent pain, and calcification was noted in the right adrenal and a 4 ~. cyst was removed . The bone lesion was biopsied, and the tests for adrenal function, including 17-hydroxy corticosteroids and 17- keto steroids, remained slightly elevated. The left adrenal tumor weighed 670 gms. It had a brown- yellow surface and num.u-ou.s small cysts and foci of necrosis~
A large palpable adrenal mass has a good chance of being carcinoma. Othe~than size there is no help in diagnosis from the gross appearance.
Microscopically the tumor shows two patterns of gr owth and cells. In one, the cells and arrangement are similar to that of the fascicular zone of the adrenal cortex. In another region of the tumor, the cells are much _more anaplastic, show less resemblance to adrenal cortical cells and have numero~s mitoses. A biopsy of the lesion of the 12th thoracic vertebra shows tumor tissue similar to that in the adrenal and represents a metastasis. The tumor of the adrenal, therefore, is an adrenal cortical carcinoma with metastasis to vertebra.
Diagnosis: Adrenal cortical carcinoma with metastasis to vertebra.
DISCUSSION: Adrenal cortical carcinomas are infrequent. Huvos et al. reported 34 cases ·seen at Memorial Hospital in New York over a 30-year period. They occur at all ages and are more common in females. The tumors in younger patients usually function to varying degrees, often producing CUshing's syndrome. In older patients the tumors are less likely to function. Recurrences and metastases (usually blood borne) are common, and most patients die from the disease within a few years.
Four months after the removal of the rem,oved from the right adrenal. The cyst contain any identifiable adrenal tissue. the adrenal carcinoma is unknown; adrenal
left adrenal, a 4 em. cyst was was partly calcified and did not The relationship of the cyst to cysts in- themselves are rare.
Followup: It is now about five years since the adrenal cancer was removed. The patient "has been treated with several courses of chemotherapy and radiation therapy for metastases to bone, including ribs, and abdominal recurrences . At the moment he is without symptoms, but has moderately el evated ketosteroids.
REFERENCES :
1 . Foster, D. C.: Adrenal cysts . Arch. Surg. 92:131, 1966. 2. Huvos, A. G. et al. : Adrenal cortical carcinoma : clinicopathologic
study of 34 cases. Cancer ~:354-361, 1970.

ClSE 14
Th.e patient was a 32-year old woman with a pelvic mass. At operation one ovary y as enlarged to 5.5 em. and was partially replaced by a single yellow- white 2.5 em . mass. There is no mention of involvement of the opposite ovary nor is ther e mention of abnormal endocrine symptoms nor of tumor elsewhere.
Microscopically the mass is uniform and consists of 2 components . one is a rather dense fibrous tissue which extends to the periphery of the aodule which is presumably. the per itoneal surface. The fibrous tissue is fairly well d~fferentiated and in some places forms a considerable amount of collagen. Embedded and dispersed throughout the fibrous tissue are small ne.s. s of 20 to 40 cells which usually grow in rather solid clusters . These cells look epithelial and show no transition to the adjacent fibrous stroma. The cells are usually in solid masses which are rounded or ovoid, but at times the cells form lumens which contain a small droplet of mucus . The individual cells of these clusters are fairly uniform in size, rounded except for tlle relatively few that are cuboidal or aJ.most columnar. The nuclei show no mitc;>ses. Fontana stains show a few granules, dark staining, particularly near the base of the cells.
Diagnosis: Carcinoid tumor of ovary.
DISCUSSION: The differential diagnosis here is between all tumors that induce or produce excessive ovarian stroma and that also have nests of epithelium embedded in the stroma. In addition to carcinoid tumors which often stimulate a great fibrous response when they arise or are metastatic to the ovary, one must consider the various gonadal stromal tumors as well. The cells of the nests do not form Call- Exner bodies so granulosa cell tumors can be excluded. The one gonadal stromal tumor that needs to be considered particularly here is the androblastoma ·or the Sertoli cell tumor. I think, however, that with formation of mucus and the presence of a few argentaffin granules in the epithelial cells in this lesion that the diagnosis is better for the carcinoid tumor. Carcinoid tumors may be either metastatic or primary in the ovary. The metastatic tumors are usually associated with multiple foci of carcinoid elsewhere and in the opposite ovary. Presumably that was not the case in this instance so the diagnosis of primary carcinoid tumor of the ovary seems more realistic . Primary carcinoids of the ovary usually arise in association with other teratoid elements, such as a cystadenoma or a dennoid cyst. Sometimes these are evident only in the opposite ova_ry, rather than in the ovary containing the carcinoid tumor . In one review by Robboy et al. , carcinoid tumors primary in the ovary showed carcinoid syndrome in about a third of the cases, especially when the tumors were large. The overall prognosis of carcinoid tumors arising in the ovary is relatively good .
REFERENCES :
l. Ro.bboy et al. : Insular carcinoid primary in the ovary . Cancer ~: 404, 1975.

CASE 15
The patient was a 19-year-old male who presented with a large anterior mediastinal ~ss without evidence of tumor elsewhere or of metastases . The mass was encapsulated and weighed 400 gms . It had a few cystic cavities with some necrosis and hemorrhage .
The mass is either arising in or near the thymus because of the presence of considerable· thymic tissue immediately adjacent. The mass is composed of epithelial-like cells that grow in the papillary, reticular, acinar and solid pattern. There are also some sinusoidal areas. The individual cells are ~idal or flat and show an intimate relationship with many blood vessels. Mitoses are ~ommon in these cells • At times the cells invaginate into a vascular space, forming a glomerular structure. The stroma is prominent in some areas arl shows a fibromyxoid appearance. The stroma, too, is intimately related to the blood vessels and to the epithelial-like cells. Near some of the cells are some hyalin-like, rounded bodies and prominent basement membrane 111aterial that stains positively with PAS. In one focus there are some large
· anaplastic cells, almost of a syncytial nature. The tumor is fairly well circumscribed for the most part, but adjacent to it there are several small daughter nests o~ similar tumor, suggesting either invasion or metastasis.
Diagnosis : Endodermal sinus tumor (yolk sac tumor) .
DISCUSSION: In the past few years, various types of tumors, not typical thymomas, have been reported arising in the thymus or near the thymus gland. Some of these tumors have been ca.lled germinomas and have an appearance similar to the seminoma or the embryonal carcinoma of the testis . Choriocarcinomas have also been reported, and endodermal sinus tumors as well. Some of these arise as elements of a teratoma. Most do not represent metastasis from a tumor of the testis. This has been conclusively proved by the fact that at autopsy no testicular tUJnOr has been found in most instances of lesions of this type and, furth~re, . while this group of tumors is more common in males, they have also been reported in females as well.
The endodermal sinus tumor is a confusing one partly because of the various terms used to describe it and partly because its exact tissue derivation is still poorly understood. In 1959, Teilum described the tumor very well and separated it from other embryonal type tumors of the testis. Since it resembled t..'le primitive endodermal sinus of the rat , he designated it as an endoder.mal sinus tumor. Other observers, such as Huntington and Bullock, compared the tumor to the yolk s~c, hence the diagnosis yolk sac tumor . It has been called by other names, including juvenile embryonal carcinoma (testis). No matter what it is called or what its exact tissue of origin, it is a rather distinctive tumor with a wide variety of histologic patterns. The tumor arises in ovary, testis and extragonadal sites. Huntington and Bullock reported 5 extragonadal tumors of this type, one of which was a malignant component of a mediastinal te.ratoma. Another interesting paper is from Indiana University; 14 of these tumors were reviewed from their files. They found that 6 arose in the testis, 4 in the ovary and 4 were extragonadal. One of the extragonadal tumors arose in the mediastinum , just as in this case. While the prognosis in those tumors arising in the testis of male infants is somewhat better, the overall prognosis ·of most of these endodermal sinus tumors is rather poor.
REFERENCES :
l. Pierce, G. B. I Bullock, w. K. and Huntington, R. w • 1 Jr.: Yolk sac twnors of the testis. Cancer 25:644-658, 1970.
2. Huntington, R. w • 1 Jr. and Bullock I w. K.: Yolk sac tumors of the ovary. Cancer 25:1357-1367, 1970.
3 • . Huntington, R. w • I Jr. and Bullock, w. !(. : Yolk sac tumors of extragonadal origin. cancer li:l368-l376, 1970.

CASE 15 (continued)
4. Roth, L. M. and Panganiban, w. G.: Gonadal and extragonadal yolk sac carcinomas. Cancer IL:812- 820, 1976.
5 . "'Martini, N. , Golbey, R. B. , Hajdu, S. I., Whitmore, W. F. and Beattie, E. J., Jr.: Primary mediastinal germ cell tumors. Cancer l!:763-769, 1974.
..
2

CASE 16
The patient was a 45-year-old woman who presented with an enlarged asymptomatic nodular density in her left lower lobe. The lesion was noted on routine x - ray 3 months earlier and probably was present 11 months before in retrospect. There were two closely related nodules excised. It was not stated in the history whether the large nodule . was also excised.
Microscopically the tissue consists of lung, almost all of which is diffus~ly infiltrated by a mixed cell population. The infiltrate extends to...,.c but does not involve the pleura. Most of the cells· are adult lymphoy'les, and there are numerous small, but definite germinal centers. The cellular infiltrate also contains plasma cells, eosinophils and a few polymrphonuclears as well as histiocytes . There are no mitoses in the cells of the infiltrate. While most of the infiltrate is interstitial , some of it extends into smal.l bronchi. There is no vasculitis.
Diagnosis: Benign inflammatory lymphoid infiltrate.
DISCUSSION: The differential diagnosis o£ a lesion such as this in the lung is between a nonspecific benign lymphoid infiltrate and a lymphoma. True lymphomas do arise in the lung on occasion and are usually lymphocytic or histiocytic, but other lymphomas, such as Hodgkin's disease , have also been reported as primary pulmonary neoplasms . The distinction between true lymphoma and benign inflammatory lymphoid infiltrate may be a difficult one. Characteristically, however, the benign inflammatory in£iltrates show (l)
mature lymphocytes mixed with other inflammatory cells, (2) formation of true gez7;1lina1 centers and (3) lack of pleural involvement. All of these characteristics are present in the Seminar case. The one feature t.~at would be of assistance would be an examination of a hilar lymph node since such nodes are frequently involved if the lesion is a true lymphoma.
REFERENCES :
l. Saltzstein, s. L. : Pulmonary malignant lymphomas and pseudolymphomas: classification, therapy and prognosis. Cancer ~:928-955, 1963.

CASE 17 •
The patient was a 45-year-old man ~ith a history of renal lithiasis and perforated duodenal ulcer presenting with sudden onset of aevere abdominal pain. x-ray showed large rugal folds and an ulcer crater in the duodenal bulb. Serum calcium was scme•..,hat elevated, and the serum gastrin considerably elevated . A total gastrectomy was performed. There were superficial mucosal. ulcers of the gastric mucosa and ill-defined, whitish nodules in the gastric wall.
Micr~scopic section shows the entire gastric wall with a normal appearing serosa and muscular coat. The mucosa is thrown into giant rugal folds. There are a· few tiny superficial mucosal. ulcerations. The mu9 sa. is infiltrated, rather diffusely, but without its destruction by cells extencling from a mass in the submucoaa, which does not extend into the muscularis at any point. The cells of the infiltrating mass show a varied architectural arrangement, the most frequent of which is a trabecular or ribbon arrangement, but in other foci the cells are growing in a rather solid fashion and in still other foci they are forming small glandular struct'.Jres. The. individual. cells of the mass are relatively uniform in size and shape. Most of them are polygonal or rounded and have nuclei that are relatively uniform and show only rare mitoses. The cells that show the glandular arrangements often have a plug of mucus in the center of the glandular space. The stroma between the cells is inconspicuous.. The mucosa that is infiltrated shows a prominence. of the parietal cells, often with vacuolization of them. A striking feature is the la~ of destruction of the mucosa by the infiltrati.ng cells which seem to be very L-itilnately associated ' with mucosal glands at many points. In addition to the formation of mucus by some of the cells, stains were carried out both for argentaffin and argyrophil granules. The argentaffin stain (Fontana) showed no granules in any of the cells of the mass, but the Pascual. stain for argyrophilic cells is positive in many of them with a majo::::ity of the cells of the mass showing granulation.
Diagnosis: Atypical carcinoid (lesion of gastric endocrine cells).
DISCUSSION: The lesion in this case shows, for the most part, a trabecular or riblxin-like appearance which is suggestive either of a carcinoid tumor or an islet cell tumor. The trabecular arrangement is quite characteristic of the carcinoid tumors of the upper gut, and the absence of argentaffin, but the presence of argyrophilic granules is al!:!O. quite characteristic. Small gland spaces into which t..lote cells are secreting un:..cus is also another feature that may be found in carcinoid tumors. It appears, therefore, that we are dealing with an atypical tumor or proli=eration that has many of the features of carcinoid tumor.
A second problem relates to the high gastrin levels the patient showed and the Zollinger-Ellison syndrome whic~ the patient obviously has. The staining reactions of the cells of t.~e ;astric a: 1ss are also those of the gastrin-producing cells of the stomach :xucosa. I think it is quite reasonable, therefore, ~o assume that the high gastrin level;. in this instance are produced by the gastric lesion itself, ::::ather than needing to postulate that there is an islet cell tumor in the pancreas or elsewhere as the ga~ trin producer . A few similar cases have bee:l reported either of hyperplasia or neoplasia of the G cells of the ga_stric mucosa.
Still another problem dea~s with the exact nature of the proliferative process in this insta~ce. The process, if it is a tumor, is not invading the muscularis and shows no lymphatic invas~on or other vascular invasion.
l
asE _l7 (continued) 2
Its infiltration and relationship with the mucosa is a very intimate one and is carried out without destruction of t."'le normal gastric epithelial cells, quite unusual. for a tumor. I think, therefore, that rather than this being a ~cinoid neoplasm that, in spite of its size, it may well represent just a ~lasia of the endocrine cells of the gastric mucosa .
The endocrine cells of the GI system and their capabilities are still
I poorly understood. They include cells that are argentaffin and ones that show ofnlY a.rgyropldlia. There are many dif£erent secretions that can be attributed to the so-cal.led enterochromaffin endocrine system of the gastro-intestinal tract. These include, for example, serotonin, glucagon, catecholamine, gastrin, secretin and, as in this case,. mucus as well. Whether these can a.ll be secreted by the same cel.1 or whether a different 'cell is necessary for each of these respective secretions is unknown . ~
It will be interesting in this case to find if the high gastrin levels were relieved merely by the total gastrectomy since there has been at least one instance where the gastrin levels remained high, presumably because of similar small collections of gastrin producing cells in the duodenum or even jejunum.
1. Goodrich, w. and Dockerty, M. B.: Zoll.inger-Ellison syndrome, associated gastric tumor showing is·let cell features . Minn. Med. 46:634-639, 1963.
2. Black, W. c-. and Hoffner, H. E. : Diffuse hyperplasia of gastric argyrophil cells and multiple carcinoid tumors. cancer ~:1081, 1968.
3. Bhagavan et al.. : Zollinger-Ellison syndrome in a child with endocrL"le tumorlets- of gastric antrum. Arch. Path. 2!!_:217, 1974.
4. Bordi, et al. . : Gastric endocrine cell proliferation. Arch. Path. 68: 274, 1974.

CASE 18
The patient was a 40-year-old man with acute appendicitis. The appendix was enlarged and indurated. Apparently no tumor was detected grossly.
Microscopically there is an acute inflammatory exudate on the serosa of the appendix, but the lumen, mucosa and muscularis are not inflammed. There are, however, numerous discrete clusters of large, round cells scattered throughout the muscularis and the submucosa. These cells. are often signet-ring type or at least have a vacuolated cytoplasm with the vacuoles staining with both PAS and mucicarmine. The cells occasionally fo;m an abortive. lumen, but usually the nests are rather solid. All the cells in the clusters are similar. There are no mitoses. A few lymphatics contain clusters of tumor cells. Argentaffin stains {Fontana) and argyrophil stains (Pascual) are negative.
Diagnosis: Goblet cell (mucinous) carcinoid of the appendix.
DISCUSSION: The first consideration is whether the lesion, growing so di£fuse1y in the appendiceal wall, is a primary tumor of the appendix or whether it is a metastasis or extension from elsewhere. It seems unlikely that there could be this much involvement of the appendiceal wall with tumor without there being carcinomatosis of the peritoneum or an obvious tumor from which it could have spread. I think,. therefore, that it is reasonable to conclude that the lesion is a primary appendiceal cancer.
The next consideration is the terminology for the tumor. The tumor cells for:m mucus and have the appearance of a well differentiated adenocarcinoma. There are, however, several features that make one question this diagnosis. In. the first place, there is no mucosal origin of the tumor. There are tumor cells in the lamina propria, but the mucosal glands. are normal. Furthe.nnore, the extenSive infiltration of the lamina propria and of the muscularis is much more characteristic of a cazcinoid tumor than the typical appendiceal adenocazcihoma. It is disappointing that the argentaffin and argyrophil stains were negativ e, but I, nevertheless, feel that the tumor falls into the category that has been described as a goblet cell or mucous carc~oid. of the appendix. It is important to recognize this variant of appendiceal tumor since the biologic behavior resembles that of carcinoid tumors rather than intestinal. carcinoma, and simple excision of the lesion by appendectomy is adequate therapy. The diagnosis of all carcinoid t umors is, of course, complicated by the fact that many ·of them form mucus, that some of them, typical in all other respects, do not .show argentaffin or argyrophil granules, and ~;at argentaffin granules have been demonstrated in some ·otherwise typical gastric and colonic adeno~ carcinomas. In the absence of positive argentaffin or argentophil granuJ.es by light microscopy, the diagnosis of appendiceal carcinoid may still be made by electronmicroscopy; Rosai has reported such an instance.
Since tumors of this type tend to occur in the centz:al third of the appendix and produce constriction of the lumen, the pathogenesis of the acut'e inflammation is readily explained.
REFERENCES:
1. Subbuswamy, S.c., Gibbs, N. M., Ross, C. F. and Morson, B. C.: Goblet cell carcinoid of the appendix. Ca."'lcer 34:338-344, 1974.
2. Klein, H. Z.: Mucinous carcinoi d tumor Of the vermiform appendix. Cancer 1!:770-777, 1974 .
3. Rosai, J . and Rodriguez, H. A.: Ap?lication of electron microscopy to the differential diagnosis of tumors : Am. J. Clin. Path. 50: 555-562, 1968 .

CASE 19
The patient was a 39-year-old woman who experienced the onset of hematuria , following an episode of straining. The bleeding continued, but there was· no dysuria, and the urograms revealed a fundal filling defect ·for which a segmental resection was carried out .
Microscopically the mass appears to be arising from the bladder wall and extending through the mucosa into the lumen. Only a small amount of bladder epithelium is seen on one edge, and l.t appears relatively normal. The mass is composed of a rather uniform pattern with cells growing in well circumscribed small. nests or balls. These nests are separated by thin connective tissue and vascular partitions . The individual cells of the nests are polyhedral·, have an acidophilic cytoplasm. The cytoplasm is sometimes vacuolated, suggesting the presence of fat. Some bizarre nuclei are seen, but there are no or only rare mitoses. Many of the 'cells contain a distinct nucleolus. The arrangement of the cells into balls is· emphasized with the silver stain. The tumor, for the most part, is well demarcated from the adjacent bladder muscularis, but in a few places the tumor seems to infiltrate in an invasi:ve fashion. Around the periphery of the tumor there are occasional small clusters of small cells with small nuclei as compared with the rest of the tumor; these cells suggest neuroblasts.
Diagnosis: Paraganglioma (pheochromocytoma).
DISCUSSION: The nature of the cells and particularly the accumulation of the cells into "zellballen" is characteristic of a paraganglioma ~r pheochromocytoma. In 1971, Leestma and Price reported 24 cases of paraganglioma from the files of the AFIP, reviewed the literatura and found 34 others. These tumors are, thus, an infrequent lesion arising in the urinary bladder. They are thought to arise probably from rests of neural cells which perhaps accompany the· sympathetic ganglia. At any rate, these paraganglia are comparable to the paraganglia of , for example, the organ of Zuckerkandl and other paraganglia in the general area, a.."ld tumors arising from the respective sites are similar. Also similar is the pheochromocytoma of the adrenal medulla. Some of these bladder tumors are associated with hypertension just as the comparable tumors arising in the adrenal, and the hypertension is particularly brought about with micturition. Hematuria is another common finding ·in these tumors; The hematuria tends to be intermittent. The tumors arise in both sexes, and the age range in the Leestma and Price series was from ll years to 78 years. The most common site of the tumor is in the trigone of the bladder.
REFERENCES:
l. L~estma, J. E. and Price, E. B. , Jr. : Paraganglioma of the urinary bladder. cancer ~:1063-1073, 1971.

.CASE 20
~s is ·a case of a 59- year-old wo~ who had li~er studies of unknown type 25 years before she was admitted for abdominal pain and rapidly enlarging liver.
The Seminar specimen represents a portion of the liver removed at autopsy. The liver weighed 840 gms. It showed broad bands of fibrosis . as well as fibrosis of the capsule , par+-..i.cularly encircling the major intrahepatic bile ducts. In addition, there were multiple small and several large . nodul~s in the liver parenchyma.
Microscopically the liver shows foci of fairly well differentiated, mucus-producing carcinoma which often are associated with dense fibrosis. In addition to the tumor in the liver, there were metastases in regional lymph nodes, lung and periteneum. Throughout both the carcinoma and the uninvolved liver tissue, there are focal deposits of brown-black granular material. Radioautography of these deposits shows numerous alpha tracks, characteristic of thorotrast. Thoro~ast deposits were . also present in many lymph nodes, spleen, thyroid and bone marrow.
Diagnosis: Cholangiocarcinoma, secondary to thorotrast.
DISCUSSION: The cause of this woman • s enlarged liver in 1947 is unknown, but the liver function tests performed certainly must have included injection of thorotrast, and the cholangiocarcinoma is undoubtedly secondary to that material. Thorotrast is a colloidal suspension of thorium dioxide which was used extensively from about 1930 to 1950 in diagnostic radiology for visualization of the liver, spleen and cerebral arteries. The material is· no longer used for this purpose as it is now well appreciated that various types of ·tumors, not only in the liver, but elsewhere, may result from the thorotrast.. The unstable thorium nucleus emanates particl.es and rays, including .alpha particles. It bas a biologic half life of about 400 years. The tumors perhaps arise as a direct result of the radiation, although a chemical stimulation cannot be excluded . Most thorotrast introduced into the body is deposited in the reticuloendothelial system, especially the liver, and most of the tumors have arisen in t.i.e liver. The tumors include cholangiocarcinoma, as in this instance, as well as hepatocellular carcinomas and hemangiosarcomas. Leukemias and carcinomas and sarcomas of other organs and tissues also have been reported .
REFERENCES :
1. Saragoca, A., Tavares, M. H., Barros, F. B. and Horta, J . D.: Some clinical and laboratory findings in pati:nts injected with thorium dioxide. Am. J. Gastroenterology 57 : 301-310 , 1972.
2. Smoron, G. and Battifora:-a.: Thorotrast-induced hepatoma. Cancer 30 : 1252-1259, 1972.