microsporidial stromal keratitis and endophthalmitis in an
TRANSCRIPT

Microsporidial stromal keratitis andendophthalmitis in an immunocompetent patientArjun B. Sood, Emory UniversityMatthew R. Debiec, Madigan Army Medical CenterSteven Yeh, Emory UniversityHans Grossniklaus, Emory UniversityJames Randleman, Emory University
Journal Title: Journal of Ophthalmic Inflammation and InfectionVolume: Volume 6, Number 1Publisher: BioMed Central | 2016-12-01, Pages 30-30Type of Work: Article | Final Publisher PDFPublisher DOI: 10.1186/s12348-016-0099-7Permanent URL: https://pid.emory.edu/ark:/25593/rrtt2
Final published version: http://dx.doi.org/10.1186/s12348-016-0099-7
Copyright information:© 2016, The Author(s).This is an Open Access work distributed under the terms of the CreativeCommons Attribution 4.0 International License(https://creativecommons.org/licenses/by/4.0/).
Accessed April 4, 2022 6:24 AM EDT

BRIEF REPORT Open Access
Microsporidial stromal keratitis andendophthalmitis in an immunocompetentpatientArjun B. Sood1,2*, Matthew R. Debiec3, Steven Yeh1,2, Hans E. Grossniklaus1,2 and J. Bradley Randleman4,5
Abstract
Purpose: The purpose of this study is to report a case of microsporidial endophthalmitis after penetratingkeratoplasty in a healthy patient and discuss the management.
Methods: This is a case report.
Results: A 69-year-old healthy male underwent penetrating keratoplasty for corneal scar secondary to herpesstromal keratitis. He presented with features of acute graft rejection 3 years later. After failure of medicalmanagement, a repeat full thickness keratoplasty was performed. Pathologic examination of the corneal specimenshowed microsporidia. The patient then developed a chronic endophthalmitis, and a vitreous tap and injectionfollowed by pars plana vitrectomy were performed. Pathologic examination of tissue showed microsporidia.
Conclusions: Microsporidia are being increasingly identified as the cause of stromal keratitis. This is the first reportof microsporidial endophthalmitis in a patient without underlying systemic illness.
FindingsMicrosporidia are a group of obligate intracellular spore-forming parasites that behave as opportunistic pathogensand cause ocular disease [1, 2]. Ocular manifestations in-clude keratoconjunctivitis, stromal keratitis, scleritis, andrarely endophthalmitis [3, 4]. Here, we present a uniquecase of microsporidial stromal keratitis confirmed histo-pathologically masquerading as graft rejection. The patientsubsequently developed endophthalmitis, which has notpreviously been reported in an immunocompetent patient.
Case reportA 69-year-old male was referred to Emory Eye Center inJune 2010 for herpetic stromal keratitis in the left eye.His past ocular history was notable for central retinalvein occlusion (CRVO) in the left eye 3 years earlier. Heunderwent multiple intravitreal injections of bevacizu-mab and triamcinolone for the treatment of CRVO-associated macular edema. He subsequently developed asuspected herpetic keratouveitis resulting in a dense
central stromal scar and visual acuity of count fingersdespite aggressive topical and oral antiviral therapy.The patient underwent penetrating keratoplasty (PK)
with extra-capsular cataract extraction and intraocularlens placement in July 2010. Pathologic examination ofthe corneal transplant showed microsporidial organisms.Visual acuity improved to 20/80 with use of rigid gas per-meable contact lens, and the graft remained clear untilMarch of 2013 when the patient presented with signs andsymptoms of early graft rejection. Topical corticosteroidswere utilized with no improvement, so repeat PK was per-formed in October 2014. Pathologic examination of therepeat PK specimen again showed microsporidia despitethe absence of intraocular inflammation, hypopyon, orany other signs of clinical infection.Five weeks post-operatively, the patient presented with
new onset floaters that had been present for 2 weeks. Vis-ual acuity was light perception, and intraocular pressurewas 17 mmHg. Anterior segment examination showedtrace haze at the cornea graft-host interface, 1+ anteriorchamber cells, a normal iris with a round and reactivepupil, and a well-positioned posterior chamber intraocularlens. There was no view of the posterior pole. B-scanultrasound showed a presumed vitreous hemorrhage. The
* Correspondence: [email protected] of Ophthalmology, Emory University, Atlanta, GA, USA2Emory Eye Center, Atlanta, GA, USAFull list of author information is available at the end of the article
Journal of OphthalmicInflammation and Infection
© 2016 The Author(s). Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made.
Sood et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:30 DOI 10.1186/s12348-016-0099-7

patient was lost to follow-up and presented again on post-operative week 9. Examination showed keratic precipi-tates, trace anterior chamber cell, and neovascularizationof the iris. There was no view of the posterior segmentdue to a dense yellow opacity over the pupil (Fig. 1). B-scan ultrasound showed vitreous opacities, and the patientwas diagnosed with presumed endophthalmitis. A vitreoustap and injection with vancomycin 1.0 mg/0.1 mL and cef-tazidime 2.25 mg/0.1 mL were performed. A diagnosticand therapeutic pars plana vitrectomy was performed asthe patient failed to improve. Examination of vitreous spe-cimen and iris tissue biopsied at the time of vitrectomyshowed microsporidia, consistent with a diagnosis ofmicrosporidial endophthalmitis. Bacteria and fungi didnot grow in culture. The patient was lost to follow-up andtherefore did not undergo testing for the human immuno-deficiency virus (HIV). To our knowledge, he was other-wise healthy and without underlying systemic disease.
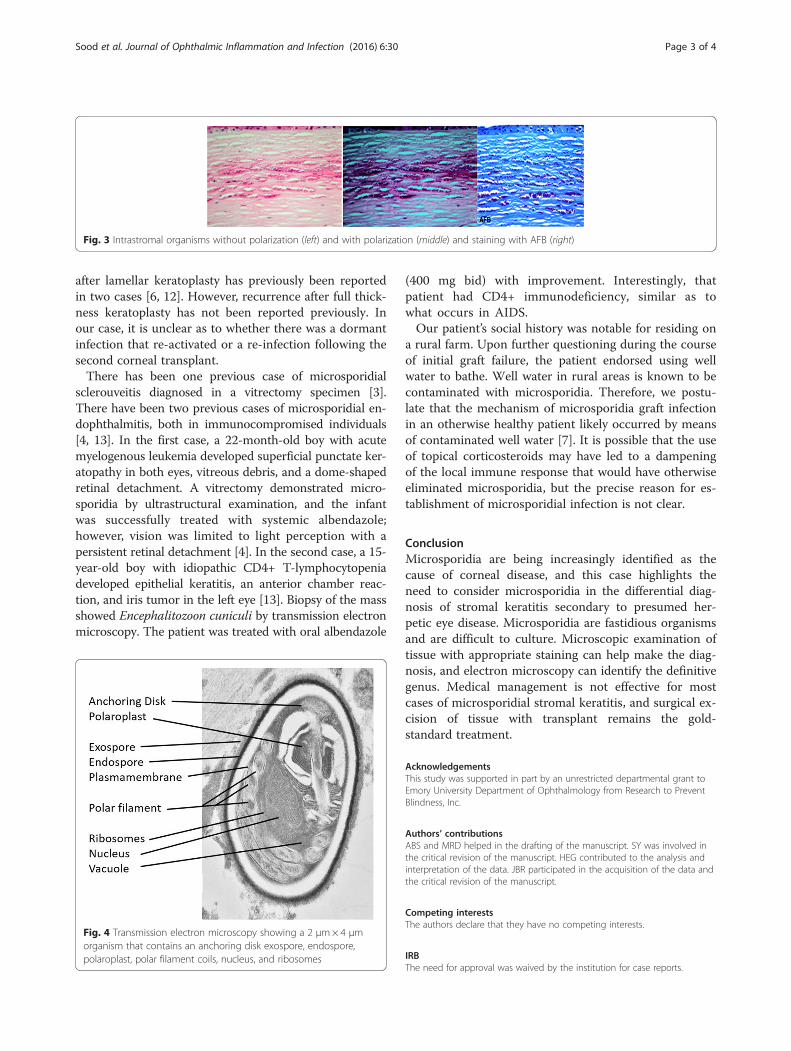
Pathologic findingsExamination of the first penetrating keratoplasty specimenfrom 2010 showed a focally disrupted epithelium andBowman’s layer. The superficial stroma contained aband of 2 μm× 4 μm organisms (Fig. 2). Examination ofthe second penetrating keratoplasty specimen showedintrastromal infiltrates or organisms as described for thefirst specimen. These organisms were polarized and stainedwith gram and AFB stains (Fig. 3). Examination by trans-mission electron microscopy showed 2 μm×4 μm organ-isms that contained an exospore, endospore, plasmamembrane, polaroplast, polar filaments, nucleus, and ribo-somes (Fig. 4). Molecular PCR testing of the corneal samplewas positive for Anncaliia algerae, part of the Nosemagenera of microsporidia. Examination of the vitrectomy spe-cimen with special stains demonstrates 2 μm×4 μm AFB-positive organisms in the iris tissue. The final diagnosis forthe corneal and vitrectomy specimen was microsporidiosis.
DiscussionThe case presented herein represents the first report ofmicrosporidial endophthalmitis in a patient without
underlying systemic illness at presentation. Microspori-dia are opportunistic pathogens causing gastrointestinal,sinus, pulmonary, muscular, renal, and ocular diseases[1]. Classically, ocular manifestations include keratocon-junctivitis, corneal stromal keratitis, sclerouveitis, andrarely endophthalmitis [3, 4]. Keratoconjunctivitis, themost common primary ocular infection was describedby Frieberg et al. in individuals with acquired immuno-deficiency syndrome (AIDS) [5]. Clinical symptoms in-clude sudden onset of unilateral pain, watering, and lightsensitivity [6]. There may be an associated papillary orfollicular conjunctivitis and the cornea will exhibit mul-tiple, coarse, punctate epithelial lesions, which may evolveinto a nummular keratitis. The disease resembles acuteadenoviral keratoconjunctivitis or herpes simplex (HSV)keratoconjunctivitis [6]. Predisposing conditions includeimmunodeficiency, use of contact lenses, topical or sys-temic corticosteroids, trauma, and exposure to contami-nated water. In India, most cases occur during the rainyseason [7].Microsporidia keratoconjunctivitis is generally a self-
limited condition, especially in immune competent per-sons. A variety of drugs have been used as treatments,including fumagillin, propamidine, isethionate, and poly-hexamethylene biguanide (PHMB), or with antifungalagents such as natamycin with or without systemic ther-apy with albendazole or itracanozole [8, 9].Microsporidia stromal keratitis has rarely been reported
[10]. The clinical diagnosis of stromal microsporidiosis ischallenging and it may occur in immunocompetent con-tact lens wearers [11]. The initial clinical presentationmimics HSV stromal keratitis, and clinical signs varydepending on the stage of disease [6]. Predisposingfactors include contaminated water, trauma, or contactwith domesticated animals. The diagnosis is confirmed oncorneal scrapings or tissue sections. The organisms meas-ure approximately 2 μm× 4 μm, polarize, and stain withacid fast stains.There is no definitive medical treatment for micro-
sproidal stromal keratitis. Current literature suggeststhat the definitive treatment is excision of infected tissueand replacement with corneal tissue [6]. Recurrence
Fig. 1 External photograph of left eye. The corneal sutures areintact. There is a yellow opacity overlying the pupil
Fig. 2 The superficial stroma showing organismsmeasuring 2 μm× 4 μm
Sood et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:30 Page 2 of 4
after lamellar keratoplasty has previously been reportedin two cases [6, 12]. However, recurrence after full thick-ness keratoplasty has not been reported previously. Inour case, it is unclear as to whether there was a dormantinfection that re-activated or a re-infection following thesecond corneal transplant.There has been one previous case of microsporidial
sclerouveitis diagnosed in a vitrectomy specimen [3].There have been two previous cases of microsporidial en-dophthalmitis, both in immunocompromised individuals[4, 13]. In the first case, a 22-month-old boy with acutemyelogenous leukemia developed superficial punctate ker-atopathy in both eyes, vitreous debris, and a dome-shapedretinal detachment. A vitrectomy demonstrated micro-sporidia by ultrastructural examination, and the infantwas successfully treated with systemic albendazole;however, vision was limited to light perception with apersistent retinal detachment [4]. In the second case, a 15-year-old boy with idiopathic CD4+ T-lymphocytopeniadeveloped epithelial keratitis, an anterior chamber reac-tion, and iris tumor in the left eye [13]. Biopsy of the massshowed Encephalitozoon cuniculi by transmission electronmicroscopy. The patient was treated with oral albendazole
(400 mg bid) with improvement. Interestingly, thatpatient had CD4+ immunodeficiency, similar as towhat occurs in AIDS.Our patient’s social history was notable for residing on
a rural farm. Upon further questioning during the courseof initial graft failure, the patient endorsed using wellwater to bathe. Well water in rural areas is known to becontaminated with microsporidia. Therefore, we postu-late that the mechanism of microsporidia graft infectionin an otherwise healthy patient likely occurred by meansof contaminated well water [7]. It is possible that the useof topical corticosteroids may have led to a dampeningof the local immune response that would have otherwiseeliminated microsporidia, but the precise reason for es-tablishment of microsporidial infection is not clear.
ConclusionMicrosporidia are being increasingly identified as thecause of corneal disease, and this case highlights theneed to consider microsporidia in the differential diag-nosis of stromal keratitis secondary to presumed her-petic eye disease. Microsporidia are fastidious organismsand are difficult to culture. Microscopic examination oftissue with appropriate staining can help make the diag-nosis, and electron microscopy can identify the definitivegenus. Medical management is not effective for mostcases of microsporidial stromal keratitis, and surgical ex-cision of tissue with transplant remains the gold-standard treatment.
AcknowledgementsThis study was supported in part by an unrestricted departmental grant toEmory University Department of Ophthalmology from Research to PreventBlindness, Inc.
Authors’ contributionsABS and MRD helped in the drafting of the manuscript. SY was involved inthe critical revision of the manuscript. HEG contributed to the analysis andinterpretation of the data. JBR participated in the acquisition of the data andthe critical revision of the manuscript.
Competing interestsThe authors declare that they have no competing interests.
IRBThe need for approval was waived by the institution for case reports.
Fig. 3 Intrastromal organisms without polarization (left) and with polarization (middle) and staining with AFB (right)
Fig. 4 Transmission electron microscopy showing a 2 μm× 4 μmorganism that contains an anchoring disk exospore, endospore,polaroplast, polar filament coils, nucleus, and ribosomes
Sood et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:30 Page 3 of 4

Author details1Department of Ophthalmology, Emory University, Atlanta, GA, USA. 2EmoryEye Center, Atlanta, GA, USA. 3Madigan Army Medical Center, Tacoma, WA,USA. 4Department of Ophthalmology, Keck School of Medicine of USC, LosAngeles, CA, USA. 5USC Roski Eye Institute, Los Angeles, CA, USA.
Received: 13 June 2016 Accepted: 2 August 2016
References1. Weber R, Bryan RT, Schwartz DA et al (1994) Human microsporidial
infections. Clin Microbiol Rev 7(4):426–612. Shadduck JA, Greeley E (1989) Microsporidia and human infections. Clin
Microbiol Rev 2(2):158–653. Mietz H, Franzen C, Hoppe T et al (2002) Microsporidia-induced sclerouveitis
with retinal detachment. Arch Ophthalmol 120(6):864–54. Yoken J, Forbes B, Maguire AM et al (2002) Microsporidial endophthalmitis
in a patient with acute myelogenous leukemia. Retina 22(1):123–55. Friedberg DN, Stenson SM, Orenstein JM et al (1990) Microsporidial
keratoconjunctivitis in acquired immunodeficiency syndrome. ArchOphthalmol 108(4):504–8
6. Garg P (2013) Microsporidia infection of the cornea—a unique andchallenging disease. Cornea 32(Suppl 1):S33–8
7. Reddy AK, Balne PK, Garg P et al (2011) Is microsporidial keratitis a seasonalinfection in India? Clin Microbiol Infect 17(7):1114–6
8. Diesenhouse MC, Wilson LA, Corrent GF et al (1993) Treatment of microsporidialkeratoconjunctivitis with topical fumagillin. Am J Ophthalmol 115(3):293–8
9. Khandelwal SS, Woodward MA, Hall T et al (2011) Treatment of microsporidiakeratitis with topical voriconazole monotherapy. Arch Ophthalmol 129(4):509–10
10. Pradhan S, Mascarenhas J, Srinivasan M (2015) Microsporidial stromalkeratitis masquerading as acute graft rejection. Cornea 34(3):353–4
11. Fogla R, Padmanabhan P, Therese KL et al (2005) Chronic microsporidialstromal keratitis in an immunocompetent, non-contact lens wearer. IndianJ Ophthalmol 53(2):123–5
12. Font RL, Samaha AN, Keener MJ (2000) Corneal microsporidiosis. Report of case,including electron microscopic observations. Ophthalmology 107(9):1769–75
13. Kodjikian L, Garweg JG, Nguyen M et al (2005) Intraocular microsporidiosisdue to Encephalitozoon cuniculi in a patient with idiopathic CD4+ T-lymphocytopenia. Int J Med Microbiol 294(8):529–33
Submit your manuscript to a journal and benefi t from:
7 Convenient online submission
7 Rigorous peer review
7 Immediate publication on acceptance
7 Open access: articles freely available online
7 High visibility within the fi eld
7 Retaining the copyright to your article
Submit your next manuscript at 7 springeropen.com
Sood et al. Journal of Ophthalmic Inflammation and Infection (2016) 6:30 Page 4 of 4