methods for manual and self-stretching of the posterior ... · methods for manual and...
TRANSCRIPT

10/20/2015
1
Methods for Manual and Self-Stretching of the Posterior Shoulder
Region
Cory Manton, PT, DPT, OCS, CSCS
Sunday, October 25, 2015
11:00am-11:55am
AAOMPT Conference 2015 1
OBJECTIVES
1. Discuss glenohumeral internal rotation deficit and its association with shoulder conditions.
2. Current evidence for stretching of the posterior shoulder region and the dosing of therapeutic exercise will be reviewed.
3. Describe the various manual and self-stretching stretching techniques for the posterior shoulder region.
4. Demonstrate and practice the stretching techniques for the posterior shoulder region with emphasis on manual stretching of the posterior shoulder.
5. Mobility exercises for the posterior shoulder region will also be discussed.
AAOMPT Conference 2015 2
Posterior Shoulder Anatomy
AAOMPT Conference 2015 3

10/20/2015
2
Shoulder Symptoms
• The top 4 reasons given by patients for visiting orthopedic surgeons were:
– Knee symptoms
– Shoulder symptoms
– Postoperative visit
– Back symptoms
– (CDC, 2010)
AAOMPT Conference 2015 4
Glenohumeral Internal Rotation Deficit • Loss of internal rotation
– “The loss in degrees of glenohumeral internal rotation of the throwing shoulder compared with the nonthrowing shoulder” (Burkhart et al., 2003).
– Most often discussed in the context of the overhead thrower
• Potential causes 1. Bony changes in the glenohumeral joint
2. Posterior shoulder muscle tightness secondary to increased
deceleration forces of the arm during follow through
3. Posterior capsule tightness from repetitive microtrauma during the late cocking and follow through phases of throwing • (Salamh et al, 2015).
AAOMPT Conference 2015 5
• Burkhart et al introduced the concept of GIRD in their article on the Disabled Throwing Shoulder. (Burkhart et al., 2003)
AAOMPT Conference 2015 6

10/20/2015
3
Disabled Throwing Shoulder “Dead arm”
• Unable to throw with preinjury velocity and control
• Pain and subjective unease in the shoulder
• Usually relates to late cocking and early acceleration phase of throwing sequence
• Associated with SLAP lesions
• (Burkhart et al., 2003)
Contributing factors to “Dead arm”
• Tight posterior inferior capsule – GIRD – Posterosuperior shift of the
GH rotation point – Increased sheer stress applied
to the posterosuperior glenoid labrum
• Peel-back forces in late cocking that cause SLAP lesion
• Hyperexternal rotation • Scapular protraction • (Burkhart et al., 2003)
AAOMPT Conference 2015 7
GIRD & Shoulder Conditions
GIRD may be a contributing factor to the following shoulder conditions:
– Impingement (external/Internal)
–SLAP lesion
–Anterior instability
AAOMPT Conference 2015 8
Bony Adaptations Humeral retroversion & Glenoid retroversion
• Associated with GIRD.
• Occurs in young pitchers – Forces across the physis lead to a twisting of the bone
and an
– Increase in retroversion
• Allows an increase in the effective external rotation of the shoulder before the humerus reaches its physiologic limit
• Protective mechanism • (Tokish, 2014)
AAOMPT Conference 2015 9
10/20/2015
4
Posterior shoulder muscle tightness
• Deceleration strains observed in the follow-through phase of pitching can lead to muscle stiffness
– (Tokish, 2014)
• Acute change
AAOMPT Conference 2015 10
Posterior capsular tightness
Pathomechanics of the deceleration of the overhead throw • Requires forceful eccentric contraction of posterior rotator
cuff muscles
• If posterior rotator cuff cannot decelerate the arm, then the posterior capsule may be required to absorb the remainder of the energy.
• Cyclical loading combined with poor dynamic stability causes a continuous cycle of repetitive microtrauma and tissue healing, leading to hypertrophied posterior capsule
• (Thomas et al, 2011)
AAOMPT Conference 2015 11
Obligate Translation
• Tightening of the posterior portion of the glenohumeral capsule causes anterior and superior translation of the humeral head with passive shoulder flexion.
• Decreased subacromial space
• Compression of tissues
• Limited and symptomatic shoulder flexion, IR, horizontal adduction
AAOMPT Conference 2015 12
10/20/2015
5
GIRD in overhead athlete
• “Rather uniform increase in external humeral rotation usually with a concomitant decrease in internal rotation in the pitching arm”
• (King et al,1969 ;Tokish, 2014)
AAOMPT Conference 2015 13
Loss of internal rotation in general population
• Proximal migration of the humerus on the glenoid while the arm is at rest is regarded as a sign advanced RC disease.
• Excessive superior-anterior translations of the humeral head with active arm elevation.
• Shortening of posterior-inferior GH capsule
• Decreased RC muscle performance
• (Seitz et al, 2011)
AAOMPT Conference 2015 14
MOVEMENT
2 Types of Glenohumeral Internal Rotation Deficit
Type of GIRD IR ER TROM
1. Anatomical GIRD Loss of IR <18⁰-20⁰ Adequate ER gain TROM within 5⁰ of the uninvolved side (symmetrical TROM)
2. Pathologic GIRD Loss of IR >18⁰-20⁰ ER deficit Loss of TROM >5⁰
IR=Internal Rotation; ER=External rotation; TROM=Total rotational motion (Manske et al, 2013)
AAOMPT Conference 2015 15

10/20/2015
6
GIRD Summary • Not all GIRD is pathologic.
• GIRD is not related to any single
type of injury.
• GIRD is a common finding in overhead athletes.
• External rotation deficiency (ERD) may be a predictor of future shoulder injury
• Problems can occur when the amount of the GIRD exceeds the ERG (GIRD:ERG ratio>1.0)
• (Manske et al, 2013)
• Loss of TROM is predictive of future injury to the shoulder in professional athletes.
• Increasing TROM exhibited a higher correlation to shoulder injuries than GIRD.
• If the TROM is equal bilaterally, treatments designed to increase IR motion are not recommended.
AAOMPT Conference 2015 16
Impairments Associated with Posterior Shoulder Tightness
• Decreased “shoulder” internal rotation ROM
• Decreased “GH” IR ROM
• Decreased “shoulder” horizontal adduction ROM
• Decreased “GH” horizontal adduction ROM
• Hypomobile posterior glide
• “We could not say with any certainty whether the side with lesser motion was lacking flexibility or if the side with greater motion was showing excessive flexibility”.
AAOMPT Conference 2015 17
Assessment Shoulder Motion vs. Glenohumeral Motion
AAOMPT Conference 2015 18

10/20/2015
7
AAOMPT Conference 2015 19
Internal Rotation in Frontal Plane Internal Rotation in Scapular Plane
Internal rotation in the open pack position
AAOMPT Conference 2015 20
Measurement of GH ER motion (Manske et al., 2013)
1. Patient in supine
2. Shoulder at 90 degrees of abduction
3. Humerus in the plane of the scapula (10-15⁰ anterior to the coronal plane). Rest the humerus on a towel roll.
4. Elbow flexed to 90 ⁰
5. Start with forearm vertical.
6. The examiner passively ER the GH joint while maintaining stabilization of the scapula via gentle palpation of the coracoid process, to feel for motion, and minimize scapulothoracic contribution or compensatory movement.
7. When the scapula begins to move into retraction and or posterior tilt, the measurement should be taken.
AAOMPT Conference 2015 21

10/20/2015
8
Measurement of GH IR Motion (Manske et al., 2013)
1. Patient supine
2. Shoulder at 90 degrees of abduction
3. Humerus in the plane of the scapula (10-15⁰ anterior to the coronal plane). Rest the humerus on a towel roll.
4. Elbow flexed to 90 ⁰
5. Start with forearm vertical.
6. The examiner passively IR the GH joint while maintaining stabilization of the scapula via gentle palpation of the coracoid process, to feel for motion, and minimize scapulothoracic contribution or compensatory movement.
7. When the scapula begins to move into protraction and or anterior tilt, the measurement should be taken.
AAOMPT Conference 2015 22
Sports Health. 2012.
1(2):131-136.
AAOMPT Conference 2015 23
Humeral head stabilization Scapular stabilization No stabilization
2 groups of asymptomatic overhead athletes Group 2: 39 male professional baseball players (mean age, 27±4.2 years; mean height 190.5±cm; mean weight, 93.4±10.4 kg; 32 pitchers) (Wilk et al., 2012)
No stabilization Scapular Stabilization Humeral headstabilization
52.3±8.4⁰
43.9±8.1⁰ 35.8±8.7⁰
65.2±8.4⁰
53.5±9.1⁰ 45.3±8.4⁰
Internal Rotation Range of Motion (mean)
Dominant Shoulder Nondominant shoulder
AAOMPT Conference 2015 24

10/20/2015
9
Reliability of 3 methods of measuring internal rotation. Group 1: 20 males (mean age, 27±6 years; mean height 170±7cm; mean weight 72±15 kg)
(Wilk et al., 2012)
Internal Rotation (mean)
Intrarater ICC Interrater ICC
No stabilization 58⁰ 0.48 0.47
Scapular stabilization
46⁰ 0.62 0.43
Humeral head stabilization
40⁰ 0.51 0.45
AAOMPT Conference 2015 25
A statistically significant difference was observed between each method of stabilization (p<.001).
Correlation between stabilization techniques Dominant shoulder of group 2. (p<.001)
(Wilk et al., 2012)
No stabilization Scapular stabilization
Humeral head stabilization
No stabilization .792 .729
Scapular stabilization
.792 .940
Humeral head stabilization
.729 .940
AAOMPT Conference 2015 26
Correlation between stabilization techniques Nondominant shoulder of group 2. (p<.001)
(Wilk et al., 2012)
No stabilization Scapular stabilization
Humeral head stabilization
No stabilization .835 .840
Scapular stabilization
.835 .899
Humeral head stabilization
.840 .899
AAOMPT Conference 2015 27

10/20/2015
10
•Resulted in the greatest amount of IR •Minimal stabilization of scapula from treatment table
•Scapula anterior tilt and protraction will result in greater “shoulder” IR ROM.
•Not pure GH motion, but scapulothoracic motion + glenohumeral motion
No stabilization
Visual inspection
•Resulted in the least amount of IR •May restrict normal arthrokinematics of the GH joint
•May restrict the normal anterior translation of the humeral head
•May generate tension on the glenohumeral joint capsule via direct contact with the articulating surfaces
•Greater posterior directed pressure on the humeral head results in less IR
•May change the starting position of scapula from anterior tilt/protraction to posterior tilt/retraction resulting in relative IR of GH joint
Humeral head stabilization
•The examiner attempts to palpate and stabilize any scapular motion, while allowing for normal glenohumeral motion
•The goal of this technique is to passively move the humerus until scapular motion occurs, then measure the degree of IR before the compensatory scapulothoracic joint motion contributes to the overall motion.
•Wilk et al. (2012) recommend this technique for measurement of GH IR motion.
Stabilization of scapula
“C” technique
AAOMPT Conference 2015 28
(Wilk et al., 2012)
Measurement of GH Horizontal Adduction
AAOMPT Conference 2015 29
GH H-ADD without scapular stabilization GH H-ADD with scapular stabilization
Measurement of GH Horizontal Adduction
AAOMPT Conference 2015 30
Side lying method with scapular stabilization
10/20/2015
11
Assessment: Glenohumeral Motion
• Vigor of measurement technique (SINSS)
• Comparison: Apples to apples
• Discipline in the cognitive and psychomotor skills of assessment of joint motion
• Practice
• “A joint’s movements can never be classed as normal unless firm over-pressure can be applied painlessly”
• “During examination and assessment pain should never be considered without relation to range nor range without relation to pain”
• Maitland 1991
AAOMPT Conference 2015 31
Intervention for Posterior Shoulder Tightness
• “The scientific and clinical rationale behind managing the hypomobile shoulder is predicated on treating soft tissue in order to create a plastic deformation response” (Manske et al., 2013).
• Physical Stress Theory (Mueller & Maluf, 2002)
AAOMPT Conference 2015 32
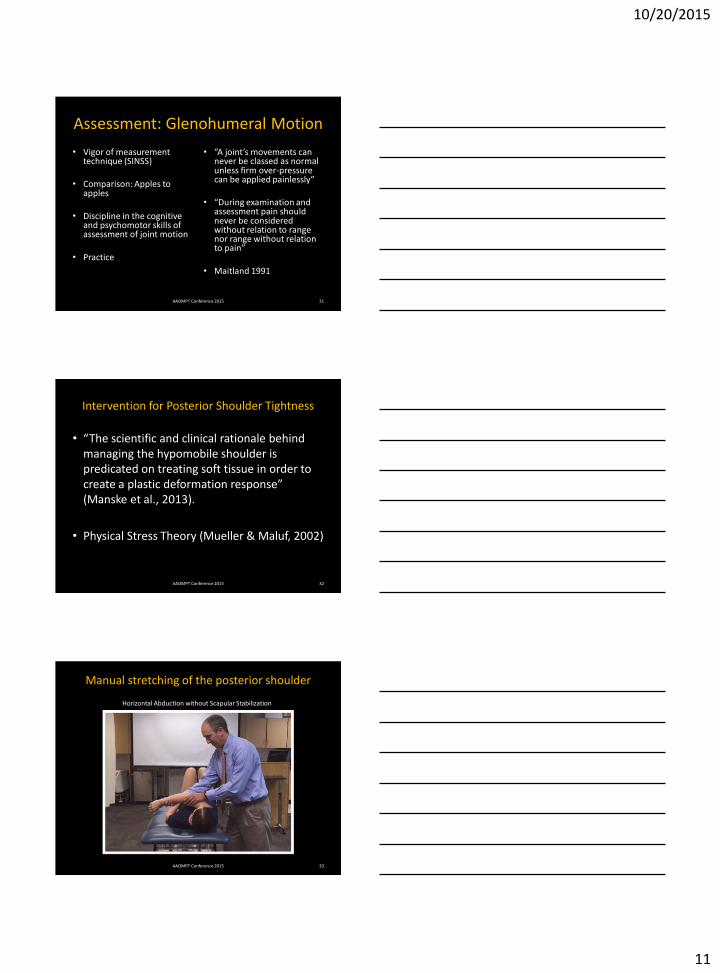
Manual stretching of the posterior shoulder
AAOMPT Conference 2015 33
Horizontal Abduction without Scapular Stabilization
10/20/2015
12
AAOMPT Conference 2015 34
Identify lateral scapular border
Add horizontal abduction (Critical)
Stabilize scapula
Avoid excessive skin tension
Maintain scapular stabilization
Add horizontal adduction
May use body to maintain humerus position during stretch
AAOMPT Conference 2015 35
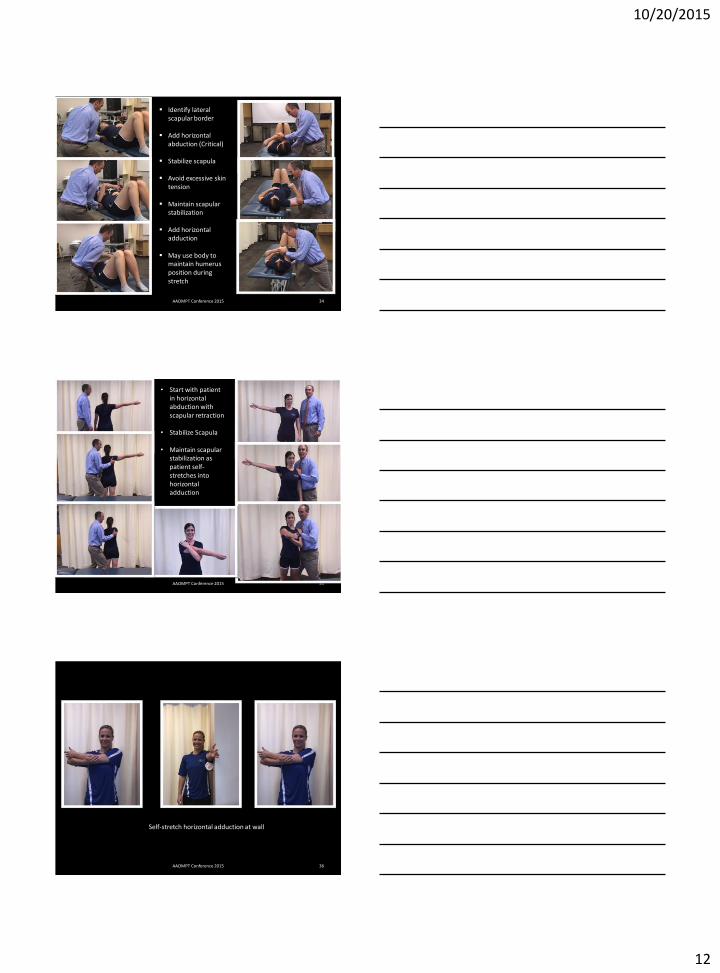
• Start with patient in horizontal abduction with scapular retraction
• Stabilize Scapula
• Maintain scapular stabilization as patient self-stretches into horizontal adduction
AAOMPT Conference 2015 36
Self-stretch horizontal adduction at wall

10/20/2015
13
AAOMPT Conference 2015 37
Slee
per
Str
etch
Sleep stretch v. Cross body stretch (Wilk et al., 2013)
Internal Rotation Motion • Cross body > Sleep stretch
(McClure et al., 2007) • Cross body stretch + joint
mobilization (Manske et al., 2010)
• Manual H-ADD with scapular stabilization > Manual H-ADD (Salamh et al., 2015)
• Sleeper stretch (Laudner et al., 2008)
• Sleeper stretch (Maenhout et al., 2012)
Horizontal Adduction Motion
• Manual H-ADD with scapular stabilization > Manual H-ADD (Salamh et al., 2015)
• Sleeper stretch (Laudner et al., 2008)
• Sleeper stretch (Maenhout et al., 2012)
AAOMPT Conference 2015 38
AAOMPT Conference 2015 39
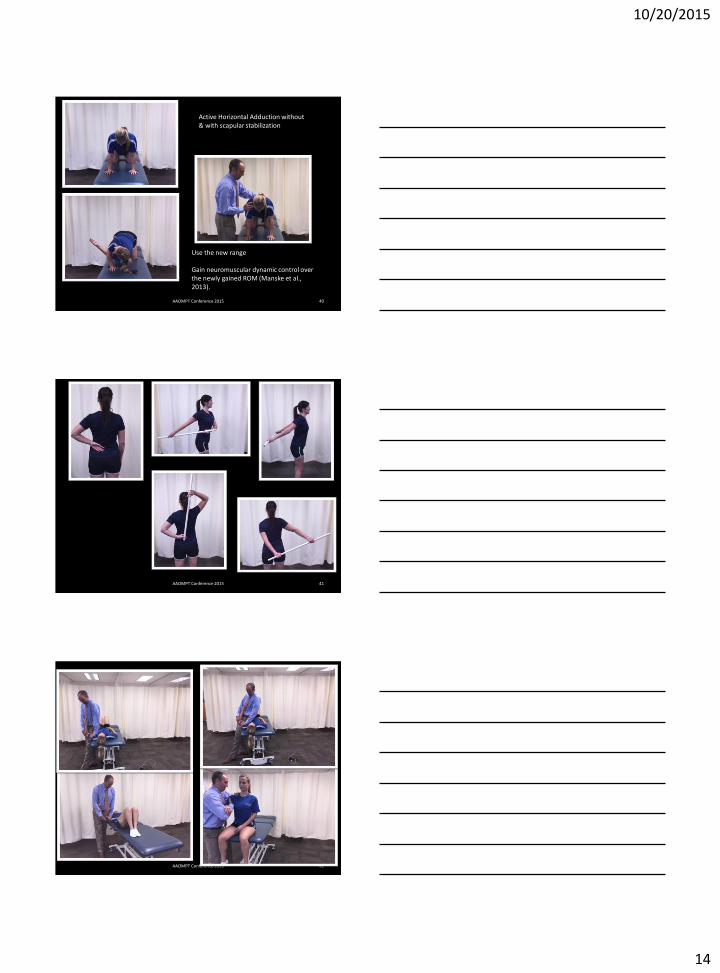
Side lying Horizontal Adduction Self-Stretch
10/20/2015
14
AAOMPT Conference 2015 40
Active Horizontal Adduction without & with scapular stabilization
Use the new range Gain neuromuscular dynamic control over the newly gained ROM (Manske et al., 2013).
AAOMPT Conference 2015 41
AAOMPT Conference 2015 42

10/20/2015
15
Don’t forget regional interdependence
• Glenohumeral joint
• Scapulothoracic motion
• AC joint
• SC joint
• Spine
• Hips
• Supination
AAOMPT Conference 2015 43
A technique is the brainchild of ingenuity. (Maitland, 1991, p8)
• “Although it is necessary to have a basis of technique from which to teach, the clinician must be totally open minded and capable of adapting and modifying techniques to achieve the purposes for which they were chosen in relation to movement and pain” (Maitland, 1991, p8).
AAOMPT Conference 2015 44
References • Burkhart, S.S., Morgan, C.D., & Kibler, W.B. (2003). The disabled throwing shoulder: Spectrum of pathology part I: Pathoanatomy and
biomechanics. Arthroscopy. 19(4): 404-420.
• Burkhart, S.S., Morgan, C.D., & Kibler, W.B. (2003). The disabled throwing shoulder: Spectrum of pathology part II: Evaluation and treatment of SLAP lesion in throwers. Arthroscopy. 19(5): 531-539.
• Burkhart, S.S., Morgan, C.D., & Kibler, W.B. (2003). The disabled throwing shoulder: Spectrum of pathology part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy. 19(6): 641-661.
• Centers for Disease Control. (2010) National Ambulatory Medical Care Survey. Factsheet: Orthopedic Surgery. Retrieved from http://www.cdc.gov/nchs/data/ahcd/NAMCS_2010_factsheet_orthopedic_surgery.pdf
• Harryman, D.T., Sidles, J.A., Clark, J.M., McQuade, K.J., Gibb, T.D., Matsen, F.A. (1990). Translation of the humeral head on the glenoid with passive glenohumeral motion. JBJS. 72-A(9):1334-1343.
• Kibler, W.B., Sciascia, A., Thomas, S.J. (2012). Glenohumeral internal rotation deficit: Pathogenesis and response to acute throwing. Sports Med Arthrosc Rev. 20(1): 34-38.
• Kolber, M.J. & Hanney, W.J. (2010). The reliability, minimal detectable change and construct validity of a clinical measurement for identifying posterior shoulder tightness. N Am J Sport Phys Ther. 5(4): 208-219.
• King, J.W., Brelsford, H.J., & Tullos, H.S. (1969). Analysis of the pitching arm of the professional baseball pitcher. Clinical Orthopaedics and Related Research. 67:116-23.
• Laudner, K.G., Stanek, J.M., & Meister, K. (2006). Assessing posterior shoulder contracture: The reliability and validity of measuring glenohumeral joint horizontal adduction. J Athletic Training. 41(4): 375-380.
• Laudner, K.G., Sipes, R.C., & Wilson, J.T. (2008). The acute effects of sleeper stretches on shoulder range of motion. J Athletic Training. 43(4): 359-363.
• Maitland, G.D. (1991) Peripheral Manipulation. 3rd ed. Oxford: Butterworth-Heinemann.
• Manske, R., Wilk, K.E., Davies, G., Ellenbecker, T., & Reinhold, M. (2013). Glenohumeral motion deficits: Friend or foe? Int J Sport Phys Ther. 8(5):537-553. Sports Health. 2:94-100.
AAOMPT Conference 2015 45
10/20/2015
16
References • Manske, R., Meschke, M., Poerter, A., Smith, B., & Reiman, M. (2010). A randomized controlled single-blinded comparison of stretching
versus stretching and joint mobilization for posterior shoulder tightness measured by internal rotation motion loss.
• McClure, P., Balaicuis, J., Heiland, D., Broersma, M.E., Thorndike, C.K., & Wood, A. (2007). A randomized controlled comparison of stretching procedures for posterior shoulder tightness. J Orthop Sports Phys Ther. 37(3):108-114. doi:10.2519/jospt.2007.2337
• Mueller, M.J., & Maluf, K.S. (2002). Tissue adaptation to physical stress: A proposed “Physical Stress Theory” to guide physical therapist practice, education, and research. Phys Ther. 82:383-403.
• Salamh, P.A. & Kolber, M.J. The reliability, minimal detectable change and construct validity of a clinical measurement for quantifying posterior shoulder tightness in the post-operative population. Int J Sport Phys Ther. 7(6): 565-575.
• Salamh, P.A., Kolber, M.J., & Hanney, W.J. (2015). Effect of scapular stabilization during horizontal adduction stretching on passive internal rotation and posterior shoulder tightness in young women volleyball athletes: a randomized controlled trial. Arch Phys Med Rehab. 96: 349-356.
• Seitz, A.L., McClure, P.W., Finucane, S., Boardman, N.D., Michener, L.A. (2011). Mechanisms of rotator cuff tendinopathy: Intrinsic, extrensic, or both. Clinical Biomechanics. 26:1-12.
• Thomas, S.J., Swanik, C.B., Higginson, J.S., Kaminski, T.W., Swanik, K.A., Bartolozzi, A.R., Abboud, J.A., & Nazarian, L.N. (2011). A bilateral comparison of posterior capsule thickness and its correlation with glenohumeral range of motion and scapular upward rotation in collegiate baseball players. J Shoulder Elbow Surg. 20: 708-716.
• Tokish, J.M. (2014). Acquired and adaptive changes in the throwing athlete: Implications on the disabled throwing shoulder. Sports Med Arthrosc Rev. 22:88-93.
• Wilk, K.E., Reinold, M.M., Macrina, L.C., Porterfield, R., Devine, K., Suarez, K., & Andrews, J.R. (2009). Glenohumeral internal rotation measurements differ depending on stabilization techniques. Sport Health. 1(2): 131-136.
• Wilk, K.E., Hooks, T.R., & Macrina, L.C. (2013). The modified sleeper stretch and modified cross-body stretch to increase shoulder internal rotation range of motion in the overhead throwing athlete. J Orthop Sport Phys Ther. 43(12): 891-894.
• Wilk, K.E., Meister, K. & Andrews, J.R. (2002). Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sport Med. 30(1): 136-151.
AAOMPT Conference 2015 46