methodological issues in social support and social network research
TRANSCRIPT

Sot. Sci. Med. Vol. 26, No. 8. pp. 863-873, 1988 0277-9536188 53.00 + 0.00 Printed in Great Britain. All rights reserved Copyright 0 1988 Pcrgamon Rem pk
METHODOLOGICAL ISSUES IN SOCIAL SUPPORT AND SOCIAL NETWORK RESEARCH
PATRICK o%ILLY Cardiovascular Institute, Boston University School of Medicine, 80 E. Concord St., Boston,
MA 02118, U.S.A.
Abstract-With the plethora of articles describing a relationship between social support and/or social network and health status, it was considered useful to take stock of the current status of research in this area, focusing on two critical methodological issues: clarity of definition, and validity and reliability of the measurement instruments. Of the 33 instruments reviewed only modest agreement was found in conceptual definition, and frequently the concepts were not defined or ill-defined. Of particular concern is the definitional confusion between social support and social network. Variables used to operationalire these concepts confirm this lack of specificity and ambiguity in definition. As for validity and reliability, many of the investigators reported no data on these issues; others provided information that only modestly supported the validity or reliability of their instrument. The conclusion of this assessment suggests the need to clarify the essential elements of social support and social networks in order to better distinguish between the behavioral (support) and structural (network) variables that may be affecting health status. A question is also raised as to the likelihood of a single questionnaire being designed that would accurately measure the perceptions of support or supportive behaviors in the variety of supportive research that will continue to be studied. Finally, more rigorous standards need to be used by investigators in establishing the validity and reliability of the instruments in order to improve their predictive utility.
Key wordr-social support, social network, conceptual definition, operationalization, validity, reliability
INTRODUCTION
In the relatively few years following Cassel’s [l] seminal paper on host susceptibility to illness and the social environment, theoretical statements [2-6], major reviews [7-l I], and numerous research studies have been published on the often ill-defined concepts of social support and social networks. Using a variety of direct and indirect measures, investigators have noted an association between social support and social networks and overall mortality [ 12, 131, chronic diseases [14-l 91, depression and psychological dis- tress [20-271, psychiatric disorders [28-321, bereave- ment [33,34], and other health and medical problems [3543]. While most of these studies have provided evidence of either the direct and/or indirect (‘buffering’) effects of social support and social net- works on health status, the data have often been uncritically accepted. Under close scrutiny, a number of methodological weaknesses in this research be- comes apparent.
Some of these methodological issues were ad- dressed in a recent article by Orth-Gomer and Unden [44], which provides a detailed examination of 16 instruments used to measure social support and social networks. The following review extends this type of analysis by examining first the use of conceptual and operational definitions in the development of 33 instruments and then, the validity and reliability of these instruments.
Letters were sent to over 60 individuals who had reported either the development or use of instruments to measure these concepts or reported results of investigations of social support or social networks which implied the use of such instruments. The authors were asked to provide copies of the instru-
ments used and to indicate how they had addressed the issue of validity and reliability. The following analysis, based on their responses as well as published reports, focuses primarily on 24 measures, sum- marized in Table 1, that purported to measure social support. In addition, we will briefly comment on the nine measures, summarized in Table 2, that pur- ported to measure social networks.
SOCIAL SUPPORT
Conceptual definitions of social support
Conceptual definitions were provided for 14 of the 24 instruments listed in Table 1. Six of the definitions were derived from the writings of Caplan [3], Cobb [4], Kahn [5] and Weiss [6]. In looking for a concep tual link in the writings of these authors (as well as others), one can identify three common elements. Support is seen as (a) an interactive process in which (b) particular actions or behaviors (c) can have a positive effect on an individual’s social, psycho- logical, or physical well-being. The differences in definition develop over what actions, interactions, and effects should be considered as related to social support. Caplan [3], Kahn (51 and Weiss [6] include cognitive, affective, and instrumental behaviors. Cobb’s [4] definition is more circumscribed. He ex- cludes instrumental assistance, and also sees support as functioning predominantly in crisis situations.
Other definitions of social support used in the studies listed on Table I include such network dimen- sions as size, source and frequency of contact, and accessibility to members [45-49]. Finally, 10 of the 24 researchers (41%) had either no or very unclear definitions of social support.
863

Co
nce
olu
al
def
init
ion
Tab
le
I M
eth
od
olo
gic
al
com
po
nen
ts
of
stu
die
s o
f so
cial
su
pp
ort
Op
erat
ion
al
def
init
ion
V
alid
ity
Rel
iabi
lity
An
dre
ws
ef
al.
(197
7)
WI
_
Bar
rerr
a el
al
.
(198
1)
1641
B
arre
rra
(198
1)
[35]
Div
ersi
ty
of
nat
ura
l h
elp
ing
b
ehav
iors
th
at
ind
ivid
ual
s ac
tual
ly
rece
ive
wh
en
pro
vid
ed
with
as
sist
ance
Bla
zer
(198
2)
[73]
-
Bra
nch
an
d
Jett
e (1
983)
13
61
Cal
dwel
l an
d
Blo
om
(198
2)
[45]
Car
veth
an
d
Go
ttlie
b
(197
9)
[46]
Go
ttlie
b
(197
8)
(651
Hen
der
son
el
o
l
(198
0)
[59]
Du
nca
n-J
on
es
(198
1)
[W
Hir
sch
(1
980)
17
21
Six
teen
it
ems
are
use
d
to
mea
sure
th
e p
rese
nce
o
f
thre
e ty
pes
o
f su
pp
ort
u
nd
er
stre
ss:
cris
is
sup
po
rl;
sup
po
rt
fro
m
nei
gh
bo
rho
od
; so
cial
p
arti
cip
atio
n
Fo
rty
item
s g
ener
ated
fr
om
th
e lit
erat
ure
ar
e u
sed
to
spec
ify
amo
un
t o
f h
elp
ing
b
ehav
iors
re
ceiv
ed
in
the
pre
ced
ing
m
on
th
Info
rmal
lo
ng
-ter
m
care
as
sist
ance
: al
l ty
pes
of
hel
p,
pai
d
or
un
pai
d,
pro
vid
ed
by
fam
ily,
frie
nd
s,
or
nei
gh
bo
rs
Ind
icat
ed
that
si
x as
pec
ts
sho
uld
b
e
con
sid
ered
: so
urc
e;
net
wo
rk
size
;
acce
ssib
ility
; fr
equ
ency
o
f co
nta
ct;
typ
e o
f
sup
po
rt;
adeq
uac
y
Th
ree
def
init
ion
s ar
e su
gg
este
d:
amo
un
t o
f
net
wo
rk
con
tact
; p
rob
lem
-cen
tere
d
feed
bac
k;
imp
ort
ance
o
f co
nta
ct
with
net
wo
rk
mem
ber
s
So
cial
re
lati
on
s ar
e p
rovi
ded
b
y:
atta
chm
ent;
so
cial
in
teg
rati
on
; n
urt
ura
nce
;
reas
sura
nce
o
f p
erso
nal
w
ort
h;
sen
se o
f
relia
bilit
y;
hel
p
and
g
uid
ance
Fiv
e fo
rms
of
inte
ract
ion
th
at
po
siti
vely
o
r
neg
ativ
ely
affe
ct
succ
ess
of
cop
ing
ef
fort
s:
gu
idan
ce;
soci
al
rein
forc
emen
t;
aid
;
soci
aliz
ing
; em
oti
on
al
sup
po
rt
Ele
ven
it
ems
sele
cted
th
at
rela
te
to:
role
s an
d
atta
chm
ents
; fr
equ
ency
o
f so
cial
in
tera
ctio
n;
per
ceiv
ed
sup
po
rt
Res
po
nd
ents
sp
ecif
y if
assi
stan
ce
is p
rovi
ded
in
I I
bas
ic
and
in
stru
men
tal
acti
viti
es
of
daily
liv
ing
Fo
rty
item
s ar
e u
sed
to
re
flec
t d
egre
e o
f su
pp
ort
rece
ived
in
th
e si
x co
nce
ptu
al
area
s
Fo
r fi
ve
core
n
etw
ork
m
emb
ers:
n
um
ber
o
f d
ays
in
con
tact
si
nce
ev
ent
(e.g
. a
child
’s
bir
th);
n
um
ber
o
f
dis
cuss
ion
s si
nce
ev
ent;
im
po
rtan
ce
of
the
con
tact
Tw
enty
si
x em
pir
ical
ly-g
ener
ated
ca
teg
ori
es
of
hel
pin
g
beh
avio
rs
are
org
aniz
ed
into
fo
ur
clas
ses:
emo
tio
nal
ly-s
ust
ain
ing
; p
rob
lem
-so
lvin
g;
per
son
al
infl
uen
ce:
envi
ron
men
tal
acti
on
Fift
y tw
o q
ues
tio
ns
are
use
d
to
spec
ify
deg
ree
of
avai
lab
ility
an
d
per
ceiv
ed
adeq
uac
y o
f su
pp
ort
fo
r
each
o
f si
x so
cial
re
lati
on
ship
s
Res
po
nd
ents
sp
ecif
y am
ou
nt
of
daily
in
tera
ctio
n
with
n
etw
ork
m
emb
ers
and
in
fi
ve
area
s o
f
sup
po
rtiv
e ac
tivi
ty,
thei
r d
egre
e o
f sa
tisf
acti
on
w
ith
inte
ract
ion
s th
at
occ
urr
ed
Fac
e P
ilot
stu
dy,
no
re
sult
s g
iven
(I)
Fac
e (I)
T
est&
rete
st,
r =
0.88
(2
) P
osi
tive
co
rrel
atio
ns
with
M
oo
s’
Fam
ily
(2)
Co
rrel
atio
n
coef
fici
ents
, C
oh
esio
n
sub
scal
e o
f F
amily
E
nvi
ron
men
t 0.
4‘&
0.91
Sca
le
(FE
S),
an
d
net
wo
rk
size
(3
) A
lph
as,
0.93
-0.9
4
Item
s se
lect
ed
fro
m
pre
vio
usl
y-va
lidat
ed
-
inst
rum
ent
Wit
hin
cl
ust
ers:
(I)
Co
rrel
atio
n
coef
fici
ents
.
0.25
-0.4
3
(2)
Alp
has
, 0.
59-0
.73
(I)
Fac
e
(2)
Ag
reem
ent
by
thre
e o
f fo
ur
rate
rs
on
cate
go
ry
and
d
efin
itio
n
of
beh
avio
rs
Inte
r-ra
ter
con
sist
ency
fo
r:
sco
rin
g
un
its,
0.
76;
cod
e
assi
gn
men
ts,
0.86
(I)
Fac
e
(2)
New
re
sid
ents
h
ad
sig
nifi
can
tly
few
er
and
le
ss a
deq
uat
e re
lati
on
ship
s
(3)
Lo
w
corr
elat
ion
s w
ith
Eys
enck
Per
son
alit
y S
cale
(I)
Tes
t-re
test
, r
= 0.
5lL
O.7
9
(2)
Inte
rnal
co
nsi
sten
cy,
0.37
0.
81
(4)
Sig
nif
ican
t co
rrel
atio
ns
with
re
spo
nse
s o
f
net
wo
rk
info
rman
ts
(I)
Fac
e
(2)
Co
rrel
atio
n
bet
wee
n
sub
ject
an
d
inte
rvie
wer
ra
tin
gs
of
sati
sfac
tio
n
with
sup
po
rt.
r =
0.53
Inte
rco
rrel
at~o
ns.
0.22
4.
51

Hol
ahan
an
d M
oos
(198
1) [
ZS]
Hou
se a
nd W
ells
(1
978)
[47
] R
elat
ions
hip
with
one
or
mor
e pe
rson
s th
at
In w
ork/
nonw
ork
rela
tions
hips
, I2
que
stio
ns
spec
ify
is c
hara
cter
ized
by
rel
ativ
ely
freq
uent
de
gree
of:
rel
iabi
lity;
w
illin
gnes
s to
lis
ten;
in
tera
ctio
ns,
stro
ng,
posi
tive
feel
ings
. he
lpfu
lnes
s;
and
from
sup
eyvi
sors
, co
ncer
n an
d pe
rcei
ved
abili
ty
IO le
nd a
id
com
pete
ncy
Jenk
ins
CI a
l. (1
981)
In
form
atio
n le
adin
g in
divi
dual
IO
bel
ieve
I’
4 s/
he i
s ca
red
for,
love
d, a
nd a
par
t of
a
netw
ork
of m
utua
l ob
ligat
ion
A s
erie
s of
ope
n-en
ded
ques
tions
ar
e us
ed t
o pr
obe
stru
ctur
al
posi
tion,
sa
tisfa
ctio
n,
prob
lem
s an
d su
ppor
t in
fiv
e lif
e do
mai
ns:
wor
k;
fina
nce;
hou
sing
; so
cial
lif
e; m
arri
age
Lin
er
ol.
(198
1) [
57]
Supp
ort
avai
labl
e IO
an
indi
vidu
al
thro
ugh
Dea
n C
I al.
(198
1)
soci
al t
ies
to o
ther
in
divi
dual
s,
grou
ps
and
1221
th
e co
mm
unity
Mar
mot
(1
982)
[SS
]
McF
arla
ne
et o
f. (1
981)
(62
,63]
Mill
er t
-f a
l. (1
976)
(26
1
- -
Nor
beck
et
cd.
(198
1) 1
661
Inte
rper
sona
l tr
ansa
ctio
ns
that
in
clud
e:
expr
essi
on
of a
ffec
tion;
af
firm
atio
n of
an
othe
r’s
beha
vior
s;
and/
or
givi
ng a
id
Co
ntin
ued
over
leaf
Thr
ee i
ndic
es a
re u
sed:
(I)
Fam
ily
Env
iron
men
t Sc
ale
(FE
S)
cons
istin
g of
thr
ee s
ubsc
ales
. ea
ch w
ith
nine
tru
e-fa
lse
ques
tions
on
qua
lity
of s
ocia
l re
latio
ns
in f
amily
; (2
) W
ork
Env
iron
men
t In
dex
(WE
I) c
onsi
stin
g of
thr
ee s
ubsc
ales
of
nine
tr
utfa
lse
ques
tions
on
soc
ial
clim
ate
at w
ork;
(3)
A
Tra
ditio
nal
Soci
al S
uppo
rt
Inde
x as
king
re
spon
dent
s ab
out
netw
ork
ties
and
relig
ious
/soc
ial
part
icip
atio
n
Four
in
dice
s us
ed I
O sp
ecif
y th
e de
gree
of:
(I
) Fa
mily
pr
oble
ms
(4 i
tem
s);
(2)
Satis
fact
ion
with
ne
ighb
orho
od
(2 i
tem
s);
(3)
Inst
rum
enta
l/exp
ress
ive
supp
ort
(26
item
s);
(4)
iden
tific
atio
n/
char
acte
riza
tion
of r
elat
ions
hip
with
con
fida
nt(s
) (I
I ite
ms)
Seri
es o
f qu
estio
ns
cove
ring
IO
are
as
incl
udin
g co
nfid
ants
; so
cial
con
tact
s;
soci
al/r
elig
ious
pa
rtic
ipat
ion;
an
d ne
twor
k lo
ss d
urin
g pr
evio
us
Yea
r
In s
ix c
ateg
orie
s of
pot
entia
l lif
e st
ress
: w
ork;
m
oney
/lina
na;
hom
e/fa
mily
; pe
rson
al/s
ocia
l; pe
rson
al
heal
th;
soci
ety,
re
spon
dent
s sp
ecif
y w
ith
who
m d
iscu
ssio
ns
held
, he
lpfu
lnes
s,
and
if
rela
tions
hip
reci
proc
al
Que
stio
nnai
re
incl
udes
tw
o se
ries
of
ques
tions
th
at
spec
ify:
For
con
fida
nts;
nu
mbe
r;
freq
uenc
y of
co
ntac
t; an
d qu
ality
, av
aila
bilit
y an
d re
cipr
ocity
of
re
latio
nshi
p;
For
nonc
onfi
dant
s:
num
ber;
fr
eque
ncy
of c
onta
ct;
dom
ain
of r
elat
ions
hip
and
soci
al
part
icip
atio
n
Aft
er
resp
onde
nt
iden
tifie
s up
to
20 n
etw
ork
mem
bers
an
d do
mai
n of
rel
atio
nshi
p,
nine
qu
estio
ns
are
used
to
rate
mem
bers
on
thr
ee
func
tiona
l ar
eas
of s
uppo
rt
and
on t
hra
netw
ork
com
pone
nts
(I)
FES
and
WE
I pa
rt
of p
revi
ousl
y-
valid
ated
in
stru
men
ts
(2)
Pred
ictiv
e va
lidity
of
FE
S an
d W
EI
infe
rred
fr
om
unpu
blis
hed
pape
rs
Que
stio
ns
adap
ted
from
oth
er
sour
ces
FaC
e
(I)
Indi
ces
l-2
take
n fr
om o
ther
so
urce
s (2
) Fa
mily
pr
oble
m
inde
x, m
oney
pr
oble
ms,
fa
mily
inc
ome,
lif
e de
man
ds,
neig
hbor
hood
sa
tisfa
ctio
n an
d re
cipr
ocal
, du
rabl
e,
conf
iden
tial
rela
tions
hips
si
gnif
ican
tly
rela
ted
to d
epre
ssio
n sc
ale
(CE
S-D
)
-
(I)
Inst
rum
ent
eval
uate
d by
fou
r ju
dges
an
d fo
und
acce
ptab
le
(2)
Hel
pful
ness
of
spo
use
in a
ll ca
tego
ries
si
gnif
ican
tly
diff
eren
t be
twee
n pa
rent
-the
rapi
st
coup
les
and
coup
les
in
ther
apy
-
(I)
Sign
ific
ant
corr
elat
ions
w
ith C
ohen
an
d L
azar
us
scak
fo
r af
firm
atio
n an
d a&
t bu
t no
t fo
r ai
d (2
) N
o si
gnif
ican
t co
rrel
atio
ns
with
m
easu
res
of m
ood
stat
es n
or l
ife
expe
rien
ces
Alp
has:
(I
) FE
S, 0
.89;
(2
) W
EI,
0.8
8
Alp
has,
0.
7H.9
2
Cor
rela
tions
: (I
) In
terr
ater
, 0.
754K
~O; (
2) S
ubje
ct-
info
rman
t: In
itial
, 0.
62-0
.72;
Fo
llow
-up,
0.
52-0
.73
Inle
r-ile
m
corr
elat
ion
for
four
E
in
dice
s:
8 (I
) 0.
5%0.
76
g (2
) 0.
28-0
.82
(3)
Zer
o or
der,
0.67
; g
(4)
Five
fac
tors
lo
aded
hi
gh
-
8 vr
Tes
-ret
est:
(I)
Indi
vidu
als
nam
ed
in e
ach
cate
gory
, I
= 0.
62-0
.99
1
(2)
Hel
pful
ness
in
dica
ted
in
;! ET
ea
ch c
ateg
ory,
0.
5409
4
-
(I)
Tes
-ret
est
for
supp
ort
and
netw
ork
item
s, r
= 0
.8M
.92
(2)
Inte
rnal
co
nsis
tenc
y fo
r ite
ms,
0.6
9-0.
98
Tab
le
I-co
ntin
ued
Oxl
ey
t-1
al.
(198
1) [
71]
Pear
lin
el o
l. (1
981)
15
2)
sara
son 9,
al.
(198
3)
[67]
Sch
aefe
r er
01.
(1
981)
[4
8]
Tur
ner
( I98
I)
[49]
T
urne
r (1
981)
’
Vac
hon
er a
l. (1
982)
13
41
Will
iam
s er
al
(198
1)
[68]
D
onal
d et
al.
(197
8)
[69]
w
are
PI a
l. ( 1
980)
[70
]
Acc
ess
to a
nd
use
of
indi
vidu
als,
gr
oups
or
or
gani
zatio
ns
in d
ealin
g w
ith
life
Exi
sten
ce
or
avai
labi
lity
of
peop
le
upon
w
hom
w
e ca
n re
ly,
who
le
t us
kno
w
they
ca
re
abou
t, va
lue
and
love
us
App
rais
al
of w
heth
er
and
to
wha
t ex
tent
an
in
tera
ctio
n,
patt
ern
of
inte
ract
ion
or
rela
tions
hip
is h
elpf
ul.
Thr
ee
type
s of
su
ppor
t ar
e id
entif
ied:
ta
ngib
le;
emot
iona
l; in
form
atio
nal
Tw
o de
fini
tions
: (I
) In
form
atio
n le
adin
g to
be
lief
one
is
love
d,
este
emed
. an
d a
mem
ber
of a
ne
twor
k (2
) W
eiss
’ pr
ovis
ions
of
soc
ial
rela
tions
-
Eig
ht-i
tem
sc
ale
is u
sed
to
mea
sure
: as
sist
ance
; co
ncer
n;
trus
t; va
lue/
inte
rest
si
mila
rity
am
ong
up
to
IO i
mpo
rtan
l no
nfam
ily
mem
bers
Res
pond
ents
w
ere
aske
d if
ther
e w
as
anyo
ne
to
who
m
they
co
uld
tell
anyt
hing
; m
arri
ed
resp
onde
nts
wer
e al
so
aske
d if
they
co
uld
talk
to
sp
ouse
ab
out
impo
rtan
t m
atte
rs
In
27 c
omm
on
situ
atio
ns,
resp
onde
nts
list
up
lo
nine
pe
ople
w
ho
can
be c
ount
ed
on
(num
ber
scal
e)
and
spec
ify
degr
ee
of s
atis
fact
ion
with
su
ppor
t (s
atis
fact
ion
scal
e)
Tw
o-pa
rt
ques
tionn
aire
is
use
d lo
m
easu
re:
(I)
Tan
gibl
e su
ppor
t: re
spon
dent
s id
entif
y up
to
fiv
e pe
ople
w
ho
wou
ld
prov
ide
help
in
nin
e si
tuat
ions
(2
) E
mot
iona
l an
d in
form
atio
nal
supp
ort:
afte
r lis
ting
netw
ork
mem
bers
, re
spon
dent
s ra
te
each
as
to
in
form
atio
n pr
ovid
ed;
relia
bilit
y;
boos
ts
spir
its;
is
cari
ng;
can
be c
onfi
ded
in
Thr
ee
indi
ces
are
used
: (I
) R
espo
nses
to
ni
ne
vign
ette
s ab
out
love
, es
teem
an
d ne
twor
k:
(2)
Eig
ht-i
tem
sc
ale
of r
efle
cted
lo
ve
and
self
-est
eem
; (3
) E
ight
een-
item
sc
ale
of
prov
isio
ns
of
soci
al
rela
tions
Lis
t of
que
stio
ns
on
netw
ork
ties;
co
nfid
ants
: ca
re;
soci
al
part
icip
atio
n;
and
aid
Nin
e ite
ms
mea
sure
so
cial
co
ntac
ts
and
reso
urce
s no
w
and
duri
ng
prev
ious
m
onth
to
ye
ar
Que
stio
ns
adap
ted
from
ot
her
sour
ces
-
Bot
h sc
ales
as
soci
ated
ne
gativ
ely
with
te
sts
of
pers
onal
ity
and
posi
tivel
y w
ith
life
attit
udes
an
d se
lf e
stee
m.
Num
ber
scal
e as
soci
ated
ne
gativ
ely
with
ex
tern
al
cont
rol
and
cogn
itive
in
terf
eren
ce
and
posi
tivel
y w
ith
posi
tive
life
even
ts.
Satis
fact
ion
scal
e po
sitiv
ely
asso
ciat
ed
with
ne
gativ
e lif
e ev
ents
. N
o re
latio
nshi
p be
twee
n sc
ales
an
d so
cial
de
sire
abili
ty.
Indi
ces
adap
ted
from
ot
her
sour
ces
(I)
For
vign
etle
s,
corr
elat
ions
w
ith
trad
ition
al
supp
ort
vari
able
s,
r =
0.2
4-0.
44
(2)
For
all
scal
es,
sign
ific
ant
corr
elat
ions
w
ith
five
mea
sure
s of
dis
tres
s
(I)
Fac
e (2
) F
acto
r an
alys
is
iden
tifie
d so
cial
he
alth
(i
.e.
soci
al
supp
ort)
as
sep
arat
e fa
ctor
(3
) Si
gnif
ican
t co
rrel
atio
ns
with
ph
ysic
al.
men
tal,
gene
ral
heal
th
indi
ces
Alp
ha.
0.56
(I)
Tes
t re
test
: N
umbe
r sc
ale,
I
= 0
.90;
Sa
tisfa
ctio
n sc
ale,
I
= 0
.83
(2)
Alp
has:
N
umbe
r sc
ale,
0.
97;
Satis
fact
ion
scal
e,
0.94
(I)
Tes
t-re
test
, r
= 0
.56-
0.66
?
(2)
Alp
has,
0.
314.
95
;6
B
Alp
has
for
thre
e in
dice
s (I
) V
igne
ttes,
0.
87;
(2)
Lov
e/es
teem
, 0.
724.
75;
(3)
Soci
al
rela
tions
, 0.
73
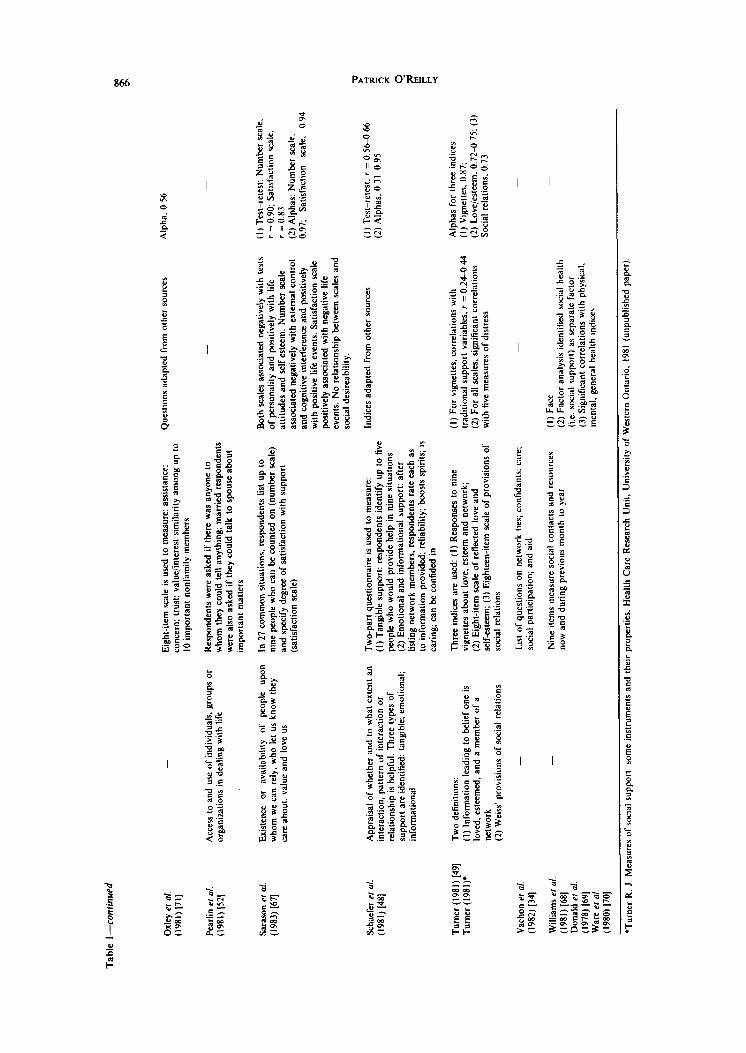
*Tur
ner
R.
J. M
easu
res
of s
ocia
l su
ppor
t: so
me
inst
rum
ents
an
d th
eir
prop
erti
es.
Hea
lth
Car
e R
esea
rch
Uni
t, U
nive
rsity
of
W
este
rn
Ont
ario
, 19
81 (
unpu
blis
hed
pape
r).

Studv
Table 2. Methodological components of studies of social networks
Conceptual definition Operational definition Validitv Rcliabilitv
Barnra Individuals who provide the (1980) [81] functions that define support
(I) In six areas of social support. respondents identify individuals who typically supply such support and who actually supplied it in the previous month (2) Respondents identify those persons to be encountered in a social conflict and with whom they actually conflicted during the previous month
Respondents identify up to seven persons to whom they talk about health-related matters and for each, give: age; proximity; frequency of visits. Respondents also are asked: whether they know one another; show concern; are consulted on health matters
Respondents identify children, other relatives and friends who are seen or talked to often and characterize: proximity; frequency of contact; closeness; health (of children); duration of friendships
Extensive series of questions characterize networks in terms of: overall structure (size, proximity, density domain of relation); patterns of interaction (durability, frequency of contact); supportive functions (help provided, strength of ties); stability of network (changes, losses, deaths)
Respondents identify up to four persons with whom they talk on matters of concern or importance and for each, specify: frequency of contact; if they know one another; proximity; content; intensity; homogeneity; duration and directedness of relationship
(I) Respondent lists up to 20 significant others with whom s/he is likely to interact during specified time period and uses matrix to indicate where one is a friend of another (2) Interviewer rates social network variables: feedback; sex differences in relationships; frequency of contact; preferences of interactions; multidimensionality
- (I) Test-retest for: Support categories r = 0. I g-0.87; Perceived network size, r = 0.88; Actual network size, r = 0.88; Individuals named both times, r = 0.48-0.73 (2) Alphas: Perceived, 0.78; Actual, 0.74
Questions drawn from other sources
- Berkanovic er ol. (1981) 1821
-
Branch and Jette (1983) [36]
Those significant others with whom elders have close contact
- -
Froland et al. (1979) [23]
Social ties that have a potential for providing social support defined as accessible and important
- -
- Gallo (1982) (831
Set of interpersonal links from which dependable others gratify a person’s psychosocial needs
Questions adapted from other sources
- Fats Hirsch (1980) [72]
Natural support system: significant others who are members of one’s social network or unaffiliated nonmental-health professionals
From list of up to six individuals who are most important to respondent, or to whom s/he feels closest, respondents identify extent to which each is relied on for material assistance, emotional support, companionship and information
From person who committed patient to hospital, interviewer identified and then interviewed patient’s network members on network relationships to determine: network size; density; openness; pattern of ties; and role structure
Structured interviews and participant observations are used to identify providers of support and reciprocal nature of helping behaviors
Mitchell (1982) [3l]
Correlation between respondent and family members on number of close friends, I = 0.62
- -
Peru& and Targ (1982) [32]
A set of direct and indirect ties among a defined group of individuals or organizations
- -
Wentowski (1981) (801
867

868 PATRICK O'REILLY
The first obvious but not very original conclusion is the need for increased agreement on a conceptual definition of social support. Particularly critical in this effort to clarify the definition of support is ending the confusion resulting from including components of social networks in the conception of social support. Social network is an analytic concept, used to de- scribe the structure of linkages between individuals or groups of individuals [50,51]. Such networks have a variety of functions of which the provision of social support is but one. Social support is provided through the behaviors or actions of members of a network and communicated through the network’s structure. Clearly, network analysis can provide an effective approach toward understanding and ex- plaining how support is offered and received. How- ever, the network is not, and should not be, confused with the support its members transmit to one an- other.
While we continue to seek to achieve a broader agreement on a conceptual definition of support, investigators must also realize the inappropriateness of operationalizing this concept without benefit of a clear definition. The continuing lack of a linkage between conceptual definition and operationalization results in very likely the often ambiguous and incon- clusive findings obtained in social support research.
Operational definitions of social support
Following from conceptual definitions are those issues related to operationalization of social support. Operationalized definitions were either stated by the investigators or reflected in the elements included in the research instruments that they used.
Returning to Table 1, the measures of social sup- port that are the least appropriate appear to be those measures that were based on a few items, such as the presence of a confidant [52] or social participation [53], which investigators selected from a more exten- sive questionnaire. The use of such indices as mea- sures of social support often appears to have been carried out retrospectively, using concepts originally designated as social health or social relationships. The use of questionnaire items in these ways could indicate the interchangeability of multiple concepts, conceptual confusion, or the inappropriate extension of one concept (i.e. social relationship) to cover a second (i.e. social support). Also in these studies the connection between the investigators’ conceptual definitions of social support and their operationalized measures of this concept is often weak or nonexistent. As a result, a variety of indirect indices of ‘social support’ were found to Ix associated with different aspects of health status, but it is not at all clear what the investigators meant by social support.
Of the remaining support studies, researchers ap- pear to have made operational decisions in three areas: (a) specificity of questions; (b) type of format; and (c) specificity of dimensions of support.
Speczjiciry of questions. The first distinction among the social support instruments was whether the ques- tions measuring support were constructed for use in a general [35,48,54-711 or specific population. By including population-specific questions, investigators were able to address issues related to type and
provision of support that were germane to that population, such as assistance provided after divorce [45,72], death [53], to new mothers [46], to the elderly [36,73], or in a work setting [25,47].
Type of format. Following from Broadhead et al.‘s [7] work, it appears that investigators used two broad formats to elicit information on support. They were:
Network format: Who provides support? In- vestigators using this format posed questions in one of two ways. In one group of studies [48, 59, 60, 62, 63, 671. investigators described one or more real or hypothetical situations and asked respondents if support or help would be provided in this situation, and if so by whom. A second group of studies [25,45,47.66,72] used either previously- elicited names of network members or simply a type of relationship (i.e. wife, friend, coworker) and asked if support had been or would be provided by such individuals in a particular situation. Clearly it was important to these investigators to know not only if support were provided, but who provided the support.
Behavioral format: Is support being provided? Investigators using this approach listed specific help- ing or supportive actions or behaviors and obtained information on whether or not respondents received or would expect to receive any of these behaviors, often limiting a positive response to behaviors that occurred within a specific period of time [56.57, 64,65,68,69]. The providers of the support- ive behaviors were not identified; what these in- vestigators considered critical was the provision of a particular behavior or the perception of support, regardless of the provider.
It should be noted that the above format dis- tinctions should not be interpreted as being mutually exclusive in terms of the overall design of an instru- ment. In fact, some investigators utilized more than one format in different sections of the same instru- ment [25,26,48, 56, 571.
Specificity of dimensions of support. Finally, in- vestigators chose whether or not to measure support as one broad, single variable [36, 52, 53, 5867,681 or to measure its conceptualized components separately, such as tangible aid, emotional support, or the ability to confide in someone [48,49,56,57,59,66].
Based upon the above, the decision tree for select- ing an approach to the measurement of social sup- port appears (at the top of facing page).
When the multiple options for instrument design are combined with the wide range of interests among researchers, it is difficult to imagine any single instru- ment being developed that would accurately measure the perceptions of support or supportive behaviors in the variety of research that continues to be conducted.
Finally, when operationalizing support, research- ers should consider the probability that there are two basic types of support [38,74, 751; everyday support leading to a general sense of well-being, similar to what Weiss [6] has proposed, and support at critical times, as Cobb [4] has proposed. There are difficulties in measuring both types of support. Everyday sup- port is difficult to measure as it is so much a part of our ‘taken for granted world’ that often we are not conscious of its importance until it is no longer

Social support and social network research 869
Conceptual Definition
What questions?
What component?
I
Multi- component
available. This support may not lend itself readily to standardized measures and survey methodology, and may be more accurately described with observational or longitudinal studies using semi-structured inter- view formats [76]. As for support at critical times, it is not readily measured prior to the crisis, and when measured retrospectively it is subject to all of the biases of this type of research. So again, use of longitudinal data would be more appropriate than the use of cross-sectional data [75].
Specific indicators of social support
After deciding which approach will be used for the instrument, the investigator must still decide on the specific indicators to be selected to measure support. As Table 1 illustrates, not only were the indicators used quite broad, but a number of researchers in- cluded questions related to participation in clubs or religious services, satisfaction with neighborhood, recent losses from the network, feelings about oneself or society, and network dimensions, such as size, frequency of contact, and reciprocal nature of re- lationships [54,56,58,61,62,71]. The use of such diverse indicators may be a reflection of the lack of clarity in how some investigators conceptualized social support, or it may simply reflect the in- vestigators’ use of available data. However, while some of these items might be considered indirect indicators of support, particularly of its availability, others, while cited as measures of social support, are
What dimension? 2 Specific
dimension
actually measures of social participation, social iso- lation, state of personal well-being, and most often, components of social networks. As Pearlin et al. [52] remind us, with social support “. . . we confront a notion that is sufficiently unspecified that it poten- tially embraces virtually all social relationships, even the most intermittent and contractual.” And, it may be added, something that measures everything ends up measuring nothing.
An additional issue related to the choice of indi- cators for measuring social support is the question of the appropriateness of relying primarily on subjective perceptions of support, or alternatively, of using only actual helping behaviors as the indicators of support. A perception of social support could be classified as a coping or adaptive mechanism based on some sense of past experiences. Subjective perceptions of support can also be influenced by the personality, mood, and illness state of an individual [771. In addition, such indicators do not provide much in sight into the specific behavioral interactions that resulted in these perceptions of support. That is, they usually do not inform us as to who did/would do what for whom in what circumstance that was/would be deemed helpful or supportive. Alternatively, when the measurement of support is based primarily on having individuals indicate if others have provided them with specific behaviors or actions, then there is no information on whether or to what extent such actions were consid- ered supportive. The probability exists that behaviors

870 PATRICK O'REILLY
intended to be supportive are interpreted differently, even negatively, by different people.
In summary, if research findings are intended to help us better understand the social processes related to social support and ultimately to develop inter- ventions aimed at improving health outcomes, then the indices used to measure support need to be consistent with conceptual definitions, differentiate the multidimensionality of support, specify the per- ceived adequacy of support, and where appropriate, identify not only general supportive behavior but the specific supportive behaviors and interactions that are presumed to affect the health outcomes being measured. Under these conditions, the development of one instrument that can accurately and precisely measure social support in all potential situations is highly unlikely.
It is probable that a widely-accepted, valid, and reliable instrument can be developed for studies in which the population and health outcomes are fairly general, such as in studies of the relationship of social support to rates of mortality or depression in a random population. But, the more specific the aims of a study, the less likely that a single valid and reliable instrument, sensitive to the provision of support relevant to the study’s outcome can be developed. In these circumstances, it is likely that over time a series of instruments tailored to particular populations and/or health outcomes could be devel- oped. As part of this process, and in lieu of always developing a totally new instrument, investigators should attempt to identify instruments that: (1) use a format that has been shown to be convenient and reliable; (2) reflect the multifaceted nature of social support; and (3) can be adapted to obtain responses that are specific to the provision of social support relevant to the aims of their particular study.
Validity and reliability
Although specifically requested, few of the re- sponses to our inquiry provided any additional infor- mation about validity and reliability of instruments beyond what was stated in published reports. Seven reports did not even mention reliability, four reported on validity, two reported only on reliability, and 11 reported on both validity and reliability. While the latter proportion may appear to be better than ex- pected, the methods used and, in many instances, the results obtained, do not provide overwhelming confidence in the data collection instruments.
Various approaches were used to establish validity. Face validity, the weakest of the available ap- proaches, was frequently used to provide evidence of the accuracy of the operational indices. Moreover, the results of studies in which more exacting methods of validation were utilized, such as discriminate, predictive, or convergent validity, generally were only modestly supportive, and often poorly to non- supportive, of the validity of the instrument [49, 56, 59,61,64,66]. In addition, four investigators [25,47, 71, 731 used questions selected from other questionnaires and inappropriately noted the tests of validity for the original questionnaire as an indicator of the validity of the selected items.
As for reliability, nine of the 24 investigators reported that they had carried out a test of reliability.
Six of these investigators and seven others who included no evidence of a test of reliability did report the correlation coefficients for their instruments, which ranged from 0.22 to 0.98, and/or alphas, which ranged from 0.31 to 0.97. Of the nine checks on reliability, six investigators [48,59, 62,64, 66,671 re- ported generally favorable results using a test-retest approach, and two [61,65] reported favorable inter- rater correlations. One study [61] contacted infor- mants from the social network in an attempt to establish the reliability of the subjects’ self- assessments of support, and reported positive results. The difficulty with interpreting this latter result is that a second study [59] also used a network informant for verification of subject responses, but claimed the positive findings to be a measure of the validity of their instrument. The use of an informant from a subject’s social network is a particularly powerful measure, but it can establish either validity or re- liability, not both. The degree of correspondence between the responses of a subject and an informant informs the researcher of the accuracy of the subject’s responses; that is, of their validity. However, it should also be remembered that the accuracy of the respondents’ answers should not be interpreted as meaning that the questions included in the instrument are valid indicators of the concept being measured. In the absence of an objective standard or criterion, complete validity of a measure cannot be established. Reliability, on the other hand, is more easily deter- mined, but was tested in only a minority of the studies reviewed here.
It appears that most investigators either moved rapidly from instrument design into data collection, without paying sufficient attention to establishing the validity and reliability of their instruments, or they inappropriately extracted ‘support’ items from a longer validated measure without validating the se- lected questions. These major methodological short- comings in the development of measures of support need to be addressed before research findings can be confidently accepted and interventions planned.
SOCIAL NETWORKS
Conceptual and operational definitions
The remaining nine reports reviewed were designed to measure social networks. They are found on Table 2.
The initial research on social networks was carried out by social anthropologists (78,791 who attempted to clarify the relationship between total or extended social networks and social behavior. More recently, the use of this analytic concept, particularly in the health field, has generally been limited to obtaining information from a focal individual about his/her personal social network; that is, those individuals to whom one has direct links (501. In the network studies reviewed here some investigators were concerned with these personal social networks [23, 32, 36,801 but the majority focused on the even more restrictive social support network (31, 72,8 l-831, what research- ers defined as the significant or important ties that provide support to a focal individual. Unlike the contrasting definitions used for social support, there appears to be strong agreement on the definitions of
Social support and social network research 871
the term ‘network’ in both the broad and narrow scope in which it has been applied. However, as with social support research, a review of the oper- ationalization of social network or social support network reveals limited correspondence among the different approaches used. Three levels of decision- making again appear to be involved in this oper- ationalization process: (a) specificity of questions; (b) specificity of network; and (c) specificity of components to be measured.
Specificity of questions. Three of the investigators [32,36,80] worded their instruments such that they were applicable only for a specific population, such as the elderly or the hospitalized. The other instruments were designed to be applicable to a general population.
Specificity ofnetwork. A seemingly critical decision was made by investigators as to whether or not to limit the number of network members identified by the respondents. Four investigators [23,32,80,8 l] asked for a list of significant others. The others collected information on a predetermined number of network members, ranging from 4 to 20. It is not clear how the specific number for network members was selected or if all investigators addressed the issue of what, if any, effect such a limitation would have on the conclusions drawn from the data. It would appear that the reasons for this decision may have had more to do with the logistics of data collection than with the logic of scientific investigation.
Specificity of components. The network com- ponents identified in the reports can be divided into those that are structural and those that are inter- actional. Among the structural dimensions, the most frequently measured were: relationship, size, density, and proximity. Among the interactive dimensions, durability, frequency of contact, and intensity of relationship were used most often by the in- vestigators. After size of the network, frequency of contact was used more often than any other com- ponent, and it was used in only five of the nine network studies reviewed.
Some of the studies [23,31,82] also included sup- portive functions such as help provided, instrumental role, type of activity, and concern shown. The inclu- sion of indicators of support in the network instru- ments again points out the confusion and/or lack of specificity among investigators about these two concepts.
Related to the issue of social network versus support network as the unit of study is the question of whether studying only supportive ties may create a distorted picture of a social network‘ in which some members can be both supportive and nonsupportive [84,85]. Focusing only on the supportive aspects of these ties will not accurately account for the stresses and tensions that lead to nonsupportive or possibly destructive actions within the network. Such actions could result from situations in which the focal indi- vidual is reluctant to request assistance from mem- bers of his network, or a network member is reluctant or unable to provide support or acts contrary to the interests of the focal individual. It is also important for researchers using social network analysis to ap- preciate the fact that individuals, particularly in urban settings, have affiliations with individuals in
different groups. As such, some members of that network may be called upon to be supportive in some situations and not in others. The identification of a support system without reference to specific situ- ations could, as a result, exclude key individuals from the analysis [40, 861.
Validity and reliability
As for validity and reliability of the instruments, it can be seen on Table 2 that most of the blocks of information are missing. Particularly distressing is the almost total lack of information on the reliability of these methods (Orth-Gomer and Unden [44] noted a similar situation in the instruments they reviewed). The criticisms discussed above need not be repeated, and should be considered as equally applicable to this group of studies. Additional concern has also been voiced about the reported low to moderate validity of subjects’ responses to questions about their social networks [87,88]. In view of these questions it would be reasonable for any investigator studying personal social networks to consider the value of using net- work informants (i.e. key members of the network) as a check on the accuracy of the responses obtained from subjects.
CONCLUSION
In summary, the criticism of the lack of critical assessments of social support and social network research as it relates to health status appears quite justified. Before the utility of these concepts is ac- cepted, it is necessary that increased attention be paid to clarify what the essential elements of social support and social networks are. It must be understood that social support and the effects of its provision are a function of an individual’s social network, and while the network has structural and interactive dimensions which can affect the provision of support, they are not themselves supportive nor necessarily indicators of supportive behaviors. Aspects of either social support or social networks can be investigated inde- pendent of each other. However, because of their interrelationship, it is potentially more productive to describe both the functional (and dysfunctional) and structural properties of the social support system. Maintaining the distinction between these concepts will be important in terms of identifying in what circumstances or situations behavioral (functional) or social (structural) interventions would be more effective in altering health status. These more clearly specified conceptual definitions should also increase agreement as to the operational components used in instrument design. Investigators should also address the issue of whether or not one questionnaire can be designed that is equally applicable in all situations, for all populations and health outcomes being ob- served. More likely we should be looking to identify the instrument(s) or formats that are most effective in measuring support or networks in specific popu- lations and for particular health outcomes. Finally, investigators need to be more rigorous in the stan- dards they use to establish the validity and reliability of their instruments.
However, the most critical issue remains the lack of agreement on what are the conceptual and

872 PATRICK O’REILLY
operational definitions of social support and social network. As long as conceptual and operational confusion remains, the predictive utility of the con- 19. cepts will not progress to the stage where logical and meaningful interventions can be developed.
Acknowledgemenrs-The author is indebted to John B. 20.
McKinlay for his suggesting the subject of this paper, and his early guidance in its formative stages, and to Kirsten Levy for her assistance in the preparation of the manuscript. 2I This research was supported in part by a grant from the National Heart. Luna and Blood Institute, NIH (HL 18318). 22.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
REFERENCES
Cassel J. The contribution of the social environment to host resistance. Am. J. Epidem. 104, 107, 1976. Antonovsky A. Health, Stress and Coping. Jossey-Bass, San Francisco, Calif., 1981. Caplan G. Support Systems and Community Mental Health. Behavioral Publications, New York, 1974. Cobb S. Social support as a moderator of life stress. Psychosom. Med. 38, 300, 1976. Kahn R. Aging and social support. In Aging from Birth IO Death, A.A.A.S. (Edited by Riley M. W.), Selected Symposia Series 30. American Association for the Ad- vancement of Science, Washington, D.C., 1979. Weiss R. W. The provisions of social relationships. In Doing Unto Others (Edited by Rubin Z.). Prentice-Hall, Englewood Cliffs, N.J., 1974. Broadhead W. E., Kaplan B. H., James S. A. er al. The epidemiologic evidence for a relationship between social support and health. Am. J. Epidem. 117, 521, 1983. Hamburg B. H. and Killia M. Relationship of social support, stress, illness and use of health services in healthy people. In Healthy People, The Surgeon Gen- eral’s Report on Health Promorion and Disease Pre- vention, Backaround Pawrs. DHEW Pub. No. 79-55071 A. G&t Printing- Of&., Washington, D.C., 1979. Kaplan B. H., Cassel J. C. and Gore S. Social support and health. Med. Care 15, 47, 1977. McKinlay J. B. Social network influences on morbid . . _.
23.
24.
25.
26.
21.
28.
29.
30.
31.
32. eptsodes and the career ot help seeking. In The Rele- vance of Social Science for Medicine (Edited by Eisen- berg L. and Kleinman A.). Reidel, Dondrecht, 1980. 33.
11. Cohen S. and Svme S. L. (Eds) Social Suooorl and
12.
13.
14.
15.
16.
17.
18.
Health. Academic Press, New York, 1985. ‘* Berkman L. F. and Syme S. L. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. Am. J. Epidem. 109, 186, 1979. House J. S., Robbins C. and Metzner H. L. The association of social relationships and activities with mortality: prospective evidence from the Tecumseh community health study. Am. J. Epidem. 116, 123, 1982. De Araujo G., Van Arsdel P. P. Jr, Holmes T. H. and Dudley D. L. Life change, coping ability, and chronic intrinsic asthma. J. psychosom. Res. 17, 359, 1973. Dimond M. Social support and adaptation to chronic illness: the case of maintenance hemodialysis. Res. Nurs. Hhh 2, 101, 1979. Earp J. L., Ory M. G. and Strogatz D. S. The effects of family involvement and practitioner home visits on the control of hypertension. Am. J. publ. Hhh 72, 1146, 1982. Matsumoto Y. S. Social stress and coronary heart disease in Japan: a hypothesis. Milbank Meml. Fund Q. 48, 9, 1970. Medalie J. H. and Goldbourt U. Angina pectoris among 10,000 men. II. Psychosocial and other risk factors as
34.
35.
36.
37.
38.
39.
40.
41.
evidenced by a multivariate analysis of a five-year incidence study. Am. J. Med. 60, 910, 1976. Morisky D. E., Levine D. M.. Green L. W. er al. Five-year blood pressure control and mortality follow- ing health education for hypertensive patients. Am. J. p&l. Hlth 73, 153, 1983. Andrews G.. Tennant C.. Hewson D. M. and Vaillant G. L. Life events, stress, social support, coping style and risk of psychological impairment. J. nerv. ment. Dis. 166, 307, 1978. Brown G. W. and Harris T. Social Origins of Depres- sion: A Study of Psychiarric Disorder in Women. The Free Press, New York, 1978. Dean A., Lin N. and Ensell W. M. The epidemiological significance of social support systems in depression. In Research in Community Mental Health (Edited by Simmons R. G.), Vol. II. JAI Press, New York, 1981. Froland C., Brodsky G., Olsen M. and Stewart L. Social support and social adjustment: implications for mental health professionals. Commun. menu. Hhh J. 15, 82, 1979. Henderson S. The social network, support, and neuro- sis: the function of attachment in adult life. Br. J. Psychiaf. 131, 185, 1977. Holahan C. J. and Moos R. H. Social support and psychological distress: a longitudinal analysis. J. ab- norm. Psycho/. 90, 365. 1981: Miller P. McC. and Ingham J. G. Friends, confidants, and symptoms. Sot. Psychiat. 11, 51, 1976. Pavkel E. G.. Emms E. M.. Fletcher J. and Rassabv E. ‘s. Life events and social support in puerperal depres- sion. Br. J. Psychiaf. 136, 339, 1980. Cohan C. I. and Sokolovsky J. Schizophrenia and social networks: ex-patients in the inner-city. Schizophr. Bull. 4, 546, 1978. Frydman M. I. Social support, life events and psychiatric symptoms: a study of direct, conditional and interaction effects. Sot. Psychiar. 16, 69, 1981. Hammer M., Makiesky-Barrows S. and Gutwirth L. Social networks and schizophrenia. Schizophr. Bull. 4, 522, 1978. Mitchell R. Social networks of psychiatric clients: the personal and environmental context. Am. J. commun. Psychol. 10, 387, 1982. Perrucci R. and Targ D. Network structure and reac- tions to primary deviance of mental patients. J. Hlfh sac. Behav. 23, 2, 1982. Parkes C. M., Benjamin B. and Fitzgerald R. G. Broken heart: a statistical study of increased mortality among widowers. Br. med. J. 1, 740, 1969. Vachon M. L. S., Rogers J., Lyall W. A. et al. Predictors and correlates of high distress in adaption to conjugal bereavement. Am. J. Psychiat. 139, 998, 1982. Barrera M. Social support in the adjustment of preg- nant adolescents: assessment issues. In Social Networks and Social Support (Edited by Gottlieb B. H.). Sage, Beverly Hills, Calif., 198 I. Branch L. G. and Jette A. M. Elders’ use of informal long-term care assistance. Geronfologisl 23, 51, 1983. Caulan R. D.. Cobb S. and French J. R. P. Jr. Re- lati’onships of cessation of smoking with job stress, personality, and social support. J. appl. Psycho/. 60, 211, 1975. House J. Work Stress and Social Support (Edited by Reading M. H.). Addison-Wesley, Reading, Mass., 198 1. Gore S. The effect of social support in moderating the health consequences of unemployment. J. Hhh sot. Behav. 19, 157, 1978. McKinlay J. B. Social networks, lay consultation and help-seeking behavior. Sot. Forces 51, 275, 1973. Nuckolls K. B., Cassel J. and Kaplan B. H. Psycho- social assets, life crisis, and the prognosis of pregnancy. Am. J. Epidem. 95, 431, 1972.
Social support and social network research 873
42. Tolsdorf C. C. Social networks, support, and coping: an exploratory study. Fem. Process. 15, 407, 1976.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60
61
62.
63.
64.
Wilcox B.- L. Social support in adjusting to marital disruption: a network analysis. In Social Nerworks and So&l Support (Edited by Gottlieb II. H.). Sage, Beverly Hills, Calif., 1981. Orth-Gomer K. and Uden A. L. The measurement of social support in population surveys. Sot. Sci. Med. 24, 83, 1987. Caldwell R. A. and Bloom B. L. Social support: its structure and impact on marital disruption. Am. J. commun. Psychol. 10, 647, 1982. Carveth W. B. and Gottlieb B. H. Social support and stress. Can. J. Behav. Sri. 11, 179. 1979. House J. S. and Wells J. A. Occupational stress, social support and health. In Reducing Occupational Stress (Edited by McLean A., Black G. and_Colligan M.), Conference Proceedines. DHEW Pub. No. 78-140. Govt Printing Office, Washington, D.C., 1978. Schaefer C., Coyne J. C. and Lazarus R. S. The health-related functions of social support. J. behov. Med. 4, 381, 1981. Turner R. J. Social support as a contingency in psycho- logical well-being. J. Hlrh sot. Behuv. 22, 357. 1981. Mitchell J. C. The concept and use of social networks. In Social Nerworks in Urban Siruotions (Edited by Mitchell J. C.). University of Manchester Press, 1969. Craven P. and Wellman B. The network city. Social. Inquiry 43, 57, 1973. Pearlin L. I., Lieberman M. A., Menaghan E. G. and Mullan J. T. The stress process. J. Hlth sot. Behav. 22, 337, 1981. Vachon M. L. S., Sheldon A. R., Lancer W. J. er al. Correlates of enduring distress patterns following be- reavement: social network, life situations, and person- ality. Am. J. Psychior. 139, 998, 1982. Andrews G., Schonel M. and Tennent C. The re- lationship between physical, psychological, and social morbidity in a suburban community. Am. J. Epidem. 105, 324, 1977. Andrews G., Tennant C., Hewson D. and Schonell M. The relationship of social factors to physical and psychiatric illness. Am. J. Epidem. 108, 27, 1978. Lia N., Simeoper R., Ensel W. M. and Kuo W. Social support, stressful life events and illness: a model and an emperical test. J. Hlth sot. Behau. 20, 108, 1979. Lin N., Dean A. and Ensel W. M. Social support scales: a methodological note. Schizophr. Bull. 7, 73. 1981. Marmot M. G. Socio-economic and cultural factors in ischaemic heart disease. Ado. Curdiol. 29, 68, 1982. Henderson S., Duncan-Jones P., Byrne D. G. and Scott R. Measuring social relationships: the interview schedule for social interaction. Psychoion. Med. 10, 723, _ - 1980. Duncan-Jones P. The structure of social relationships: analysis of a survey instrument, parts l-2. Sec. Psychiaf. 16, 143, 551, 1981. Jenkins R., Mann H. H. and Belsey E. The background, design, and use of a short interview to assess and support in research and clinical settings. Sot. Sci. Med. 15E, 195, 1981. McFarlane A. H., Norman G., Streiner D. L. e( al. A longitudinal study of the influence of the psychosocial environment on health status: a preliminary report. J. Hlth sot. Behov. 21, 124, 1981. McFarlane H. H., Neale K. A., Norman G. A. er 01. Methodological issues in developing a scale to measure social support. Schizophr. Bull. 7, 90, 1981. Barrera M. Jr, Sandler I. N. and Ransay T. B. Pre- liminary development of a scale of social support: studies on college students. Am. J. commun. Psychol. 9, 435, 1981.
65.
66.
67.
68.
69.
70.
71.
72
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
Gottlieb B. The development and application of a classification scheme of informal helping behaviors. Can. J. behuu. Sci. 10, 105, 1978. Norbeck J. S., Lindsey A. and Carrieri V. L. The development of an instrument to measure social sup port. Nurs. Res. 30, 264, 1981. Sarason I. G., Levine H. M., Bashom R. B. and Samson B. R. Assessing social support: the social support questionnaire. JT Person. so>: Psychol. 44, 127, 1983. Williams A. W.. Ware J. E. and Donald C. A. A model of mental health, life events, and social supports appli- cable to general populations. J. Hlth sot. Behav. 22,324, 1981. Donald C. H., Ware J. E., Brook R. H. and Davies- Avery A. Conceptualization and Measurement of Health in the Health Insurance Study, Vol IV, Social Health, R-1987/4-HEW. Rand Corp, Santa Monica, Calif., 1978. Ware J. E., Davies-Avery A. and Brook R. H. Concep- tualization and Measuremenl of Health for Adults in the Health Insurance Study, Vol. VI, Analysis of Re- lationships Among Health Srarus Measures, R-198716 HEW. Rand Corp, Santa Monica, Calif., 1980. Oxley D., Barrera M. Jr and Sadella E. K. Re- lationships among community size, mediators, and so- cial support variables: a path analysis. Am. J. commun. Psychol. 9, 637, 1981. Hirsch B. J. Natural support systems and coping with major life changes. Am. J. commun. Psychol. 8, 159, 1980. Blazer D. G. Social support and mortality in an elderly community population. Am. J. Epidem. 115, 684, 1982. Veiel H. 0. Dimensions of social support: a conceptual frame work for research. Sot. Psych&. 28, 156, 1985. Brown G. W.. Andrews B.. Harris T.. Adler Z. and Bridge L. Social support. self-esteem and depression. Psycholog. Med. 16; 813, 1986. Sokolovskv J. and Cohen C. I. Toward a resolution of methodological dilemmas in network mapping. Schizo- phr. Bull. 7, 109, 1981. Alloway R. and Bebbington P. The buffer theory of social support-a review of the literature. Psycholog. Med. 17, 91, 1987. Barnes J. A. Class and communities in a Norwegian island parish. Hum. Relations 7, 39, 1954. Bott E. Family and Social Network: Norms and External Relationships in Ordinary Urban Families’ (Revised Edi- tion). Tavistock, London, 1971. Wentowski G. J. Reciprocity and the coping strategies of older people: cultural dimensions of network build- ing. Geronrologisr 21, 600, 1981. Barrera M. A method for the assessment of social support networks in community survey research. Con- nections 3, 8. 1980. Berkanovic E., Telesky C. and Reader S. Structural and social psychological factors in the decision to seek medical care for symptoms. Med. Core 19, 693, 1981. Gallo F. The effects of social support networks on the health of the elderly. Sot. Work Hlfh Care 8, 65, 1982. Wellman B. Applying network analysis to the study of support. In Social Networks and Social Support (Edited by Gottlieb B. H.). Sage, Beverly Hills, Calif., 1981. Fischer C. S., Jackson S. R. M., Stueve C. H. et al. Networks and Places: Social Relations in the Urban Serring. Free Press, New York, 1977. McCallister L. and Fischer C. S. A procedure for surveying personal networks. Sociolog. Merh. Res. 7, 131, 1978. Killworth P. and Bernard H. Informant accuracy in social network data. Hum. Org. 35, 269, 1976. Hammer M. Some comments on the validity of network data. Connections 3, 13, 1980.