methodological discussions of therapeutic environments
TRANSCRIPT

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 1 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
The Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Abstract
Psychologists’ offices have been largely absent from contemporary theoretical andmethodological discussions of therapeutic environments. Research on environmentalstressors, healing environments, psychiatric facilities, and the transactions between apsychologist and client during a therapy session suggest that psychologists’ offices aresignificant for the psychologists who work there daily and the clients who visit them.
To address the gap in the literature, we examined the relationship between psychologistsand their office environments in an exploratory, qualitative study using interviews andprojective measures. Projective measures included cognitive mapping exercises andphotographs taken of the psychologist’s and client's views of each office. We interviewed10 licensed psychologists about how they perceived—and how they believed their clientsperceived—their office environments.
Content analyses of the interviews revealed that the environmental responsespsychologists used in their office designs met the needs imposed by therapeutictransactions. In addition, environmental responses helped psychologists adapt difficultspaces to the ongoing needs of therapy. Implications include design recommendations forpsychologists and designers. The training of psychologists also should give greaterconsideration to office design. Sensitivity to office design could differentiate psychologistsfrom their competitors. This is especially important in contemporary healthcare, wherehealing designs offer a competitive advantage.
Researchers have investigated the therapeutic value of institutional healthcare environments such as hospitalsand Alzheimer’s facilities in fostering positive medical outcomes and recovery from stress (McCormick andShepley 2003). Several researchers have discussed the lack of research about psychologists’ offices (Anthony1998; Anthony and Watkins 2002a; Anthony and Watkins 2002b). Experimental research lacks externalvalidity because actual psychologists, psychologists’ offices, and clientele have not been used (Miwa andHanyu 2006). As such, psychologists’ offices have been largely absent from contemporary theoretical andmethodological discussions of therapeutic environments.
Psychologists recognize that their clients suffer from stressors related to mental illness and daily routines.Clients also suffer stress from making a life transition involving discomfort and disclosure of privateinformation within an unfamiliar setting (Demick and Andreoletti 1995; McLoughlin 1995; Spivack 1984).Consequently, how, if at all, do psychologists believe that their office designs contribute to the therapeuticprocess? How do psychologists compensate for the inadequacies of their therapeutic environments? Answersto these questions could guide future research on and design of psychologists’ offices.
Environments for the treatment of mental illnessWhen an imbalance exists between the demand posed by a stressor and a person’s perceived resources toadaptively respond to the stressor, stress occurs (Stokols 1979; Stokols et al. 2000). A stressor mightoverwhelm a person’s physical and psychological resources and, as a result, cause a person to feel incompetent(Stokols et al. 2000). Evans and McCoy (1998) identify negative, stressful experiences resulting from therelationship between physical environments and a person’s psychology. These concepts include

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 2 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
overstimulation resulting from crowding and ambiguous spatial configurations.
Researchers and designers have long expressed interest in creating healthcare environments that mitigatestress. Healing gardens, views of nature, and legible building plans and signage have been well documented asdesign features that contribute to positive psychological and physiological health (Evans and McCoy 1998;Ulrich 1999; Ulrich et al. 2003).
Researchers have extensively investigated institutions such as psychiatric facilities and their possible negativeeffects on mental health. Their research reveals that the design of a psychiatric facility can reinforce rigidsocial programs and patterns of behavior among patients and staff (Bechtel 1997; Goffman 1961; Schefflen1965; Stevenson 2000). Consequently, the design of an institution reflects its philosophy of care (Bechtel1997; Stevenson 2000; Williams 1994). For instance, in the 19th century, Thomas Kirkbride designed mentalhospitals for the humane treatment of patients. His designs required one room for each patient, double-loadedmain corridors, wards terminating with sunlit bays, and access to natural settings (Good et al. 1965; Sachs1999).
Critics warn that the physical designs of many mental institutions exacerbate patients’ conditions. Fortress-likefacades reinforce the larger community’s stigma of the mentally ill (Ittelson et al. 1970; Stevenson 2000).Commons areas equipped with fixed seating inhibit social interaction (Osmond 1957; Sommer 1969). Spacesefficient for staff, such as radial plans and long corridors lined with easy-to-clean surfaces, convey a sense ofsterility and distort patients’ already disturbed perceptions with illusions and glare (Ittelson et al. 1970;Spivack 1984). Ironically, the design of mental institutions can undermine the competence of the patient,thereby worsening the patient’s illness (Moos 1973; Timko et al. 2000).
Similarly, a psychologist’s office both communicates and facilitates communication. People imbue theenvironment with psychosymbolic meaning formed through interactions with the environment (Lawrence andLow 1990). Likewise, office features and psychologist-client transactions have psychosymbolic importance.Obvious symbolic cues include artwork, desks, and diplomas (Pressly and Heesacker 2001). Less obviousforms of communication include those physical features that reflect the psychologist-client transaction andthose integral to treatment and diagnosis. In general, the therapeutic setting should be a holding environment;psychologists and their offices should provide comfortable and secure environments within which clients feelfree to communicate sensitive information (Saari 2002; Winnicott 1986).
Clients and psychologists communicate through transference relationships (Wachtel and Messer 1997; Saari2002). Horvath and Lubrosky (1993) state that a transference “implies that emotions and thoughts associatedwith the unresolved relationships with significant others are bound to be displaced (transferred) onto therelationship with the therapist” (p. 562). Transferences are imbued with feelings that the client andpsychologist hold for each other and for inanimate objects (Winnicott 1953). From positive transferences, thepsychologist and client develop a “working alliance” to relieve the client of distress (Pipes and Davenport1999; Horvath and Lubrosky 1993).
Saari’s (2002) concept of interpsychic space is the nonverbal, spatial expression of positive and negativetransferences through proxemics and personal space. For Stern (1997), an interpersonal field opens a contextfor disclosure between a psychologist and a client. Similarly, Satir (1964), Shefflen (1973), and Sommer(1969) have all demonstrated that in mental health settings, clients communicate psychological statesnonverbally with seating arrangements and the manipulation of nonfixed physical features. Psychologists caninfluence transferences through their intentional manipulations of space. For instance, Henry Stack Sullivan sat

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 3 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
across a desk from his schizophrenic clients because such an arrangement focused their attention on therapy(Goodman 1962).
Psychologists record transferences with the physical manipulation of their therapeutic environments. In theprocess, psychologists use space to treat and diagnose clients. Klein (1949) used play therapy with children sothat transferences between psychologist and client were expressed through toys. Lowenfield adapted Klein’splay therapy to trays of sand. Play with sand trays enabled a healing connection with natural elements, whilehelping the psychologist reach a diagnosis (Mitchell and Friedman 1994). Peled and Ayalon (1988) analyzedattachments to home as part of family therapy.
As is the case with other therapeutic environments, psychologists’ offices must also alleviate and adapt tostressors. Psychologists’ offices should convey holding environments within which psychologist-clienttransactions are accommodated. Also, they should empower psychologists to perform transactions necessaryfor maintaining a holding environment. Therefore, they should provide psychologists with the resourcesnecessary to adapt to the ongoing needs of therapy.
Environment-function fitA traditional measure of compatibility between an environment and the activities performed within isenvironment-function fit (Alexander 1970; Sherrod and Cohen 1982). A derivation of environment-functionfit, person-environment congruency measures the relationships between a person’s perceptions and thedemands exerted by a sociophysical environment (Lawton 1989). Researchers have applied person-environment congruency to measure fit between the elderly and nursing home facilities and the mentally illand psychiatric facilities (Kristoff 1996; Lawton 1989; Moos 1973; Timko et al. 2000). Lawton theorized thatcongruency occurred when a demand fell into a person’s perceived competency to meet that demand. If so,either a person’s perceived control or actual control over the demand increased.
The built environment is a resource that people use to exert control over demands and increase competency(Alexander 1970). Flexible environments made of nonfixed features can create greater opportunities for fit(Lang 1987). At the other extreme, negative fit decreases competency (Alexander 1970). Lower competencyalso results in decreased performance, increased stress, negative affect, and a lack of control (Lawton 1989).
Just as stress exacerbated by the environment of mental institutions and other therapeutic environments reducesthe competency of users, we suggest that the design of a psychologist’s office provides a resource for masteryover the demands of psychotherapy. Therefore, environment-function fit could be a paradigm forunderstanding psychologists as users of design, and consequently, the function of design in psychologists’offices.
Methodology
Participant sampleTen psychologists agreed to participate in a study of their office environments under the condition thatclientele were not to be included or discussed. Participants were all: (1) licensed counseling or clinicalpsychologists; (2) employed in private practice or by a healthcare facility; (3) practicing within the city wherethe researchers were located. Subjects varied in psychotherapeutic philosophy from psychoanalytic tocognitive-behavioral. Six had a private practice, and four worked for a healthcare facility.
The sample’s composition conformed to principles of strategic nonrepresentative sampling formulated by Trost
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 4 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
(1986) and used in prior research of built environments (Gustafson 2001). Nonrepresentative sampling allowsresearchers to determine a sample reflective of the breadth of the topic under study without overrepresentationby any one characteristic of the sample. Each psychologist represented one private practice or healthcarefacility. Conveniently, this prevented overrepresentation from any facility.
Procedures and measuresThe exploratory nature of the study and the sample size warranted an antipositivitic research approachemphasizing on-site research, richness of data, smaller sample size, less emphasis on generalizability, andidentification of contextual factors and information specific to each subject’s unique experience(Mazumdar and Geis 2001; Mazumdar 2002).
Interviews were conducted within the therapeutic setting so that the researchers could see firsthand and discussthe unique design features of each office and so that psychologists could describe their offices in detail.
Researchers used techniques of questioning described by Carspecken (1996) and Kvale (1996): specifically,descriptive questions, nonleading leads, and low-inference paraphrasing. After each interview, the researcherand psychologist reviewed the topics discussed on the interview guide to assess verification between theresearcher’s and psychologist’s interpretations of questions (Carspecken 1996). Such “member checking”ensured the “trustworthiness” and validity of the data (Lincoln and Guba 1985). All interviews weretranscribed verbatim.
AnalysesGrounded theory was used to identify categories within each interview and across interviews (Mazumdar andGeis 2001; Strauss and Corbin 1998). The diversity of the sample controlled for theoretical sampling, duringwhich collection and analyses of data coincide to fill gaps in the data revealed during analyses (Noonan et. al.2004; Patton 1990). Extensive auditing ensured the dependability and confirmability of the results(Lincoln and Guba 1985). Concepts representing discrete parts of the interviews emerged through a process ofopen coding. Then, concepts were synthesized into larger categories. Axial coding further synthesizedcategories and revealed dimensions (“not valued” to “highly valued”). Also, axial coding identifiedconnections between categories, revealing novel interpretations of the data. Selective coding isolated two corecategories as nuclei of the subjects’ experiences. Theoretical redundancy and saturation were achieved whenthe subjects’ transcribed interviews failed to generate categories beyond those already existing from theanalyses. To assess the reliability and validity of the categories, the researchers asked an impartial, independentresearcher—blind to the analyses and the coding of the categories—to code random samples from thetranscripts.
ResultsThe content analysis produced two core categories important to the design of psychologists’ offices. Consistentwith theories of person-environment congruence, categories of needs and responses emerged (Kristoff 1996).As shown in Table 1, the first category included therapeutic needs identified by the psychologists, i.e., criteriathat they believed were necessary for successful psychotherapy. The second category consisted ofenvironmental responses that psychologists implemented in response to therapeutic needs. Both the therapeuticneeds and environmental responses express psychologists’ desire to accommodate their clientele and relievestressors imposed by therapy. All 10 psychologists stressed the importance of therapeutic needs but differedwith respect to what environmental responses were highly valued in meeting those needs.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 5 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
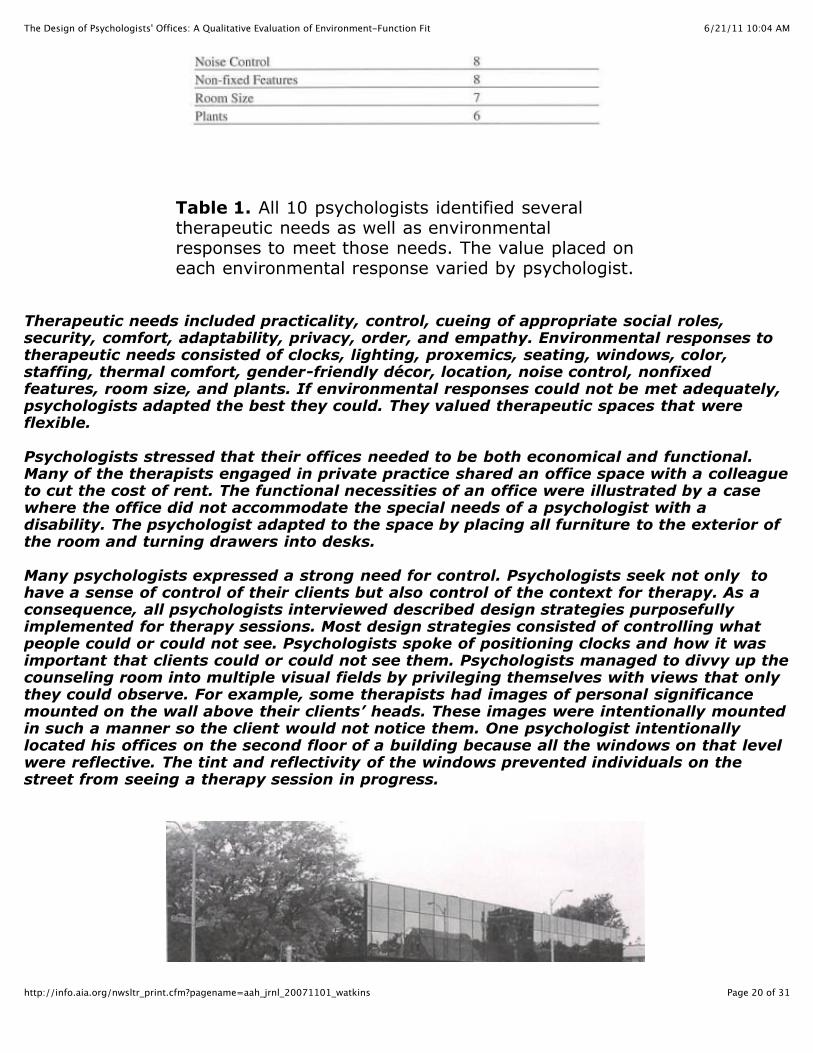
Table 1. All 10 psychologists identified several therapeutic needsas well as environmental responses to meet those needs. The valueplaced on each environmental response varied by psychologist.
Therapeutic needs included practicality, control, cueing of appropriate social roles, security, comfort,adaptability, privacy, order, and empathy. Environmental responses to therapeutic needs consisted of clocks,lighting, proxemics, seating, windows, color, staffing, thermal comfort, gender-friendly décor, location, noisecontrol, nonfixed features, room size, and plants. If environmental responses could not be met adequately,psychologists adapted the best they could. They valued therapeutic spaces that were flexible.
Psychologists stressed that their offices needed to be both economical and functional. Many of the therapistsengaged in private practice shared an office space with a colleague to cut the cost of rent. The functionalnecessities of an office were illustrated by a case where the office did not accommodate the special needs of apsychologist with a disability. The psychologist adapted to the space by placing all furniture to the exterior ofthe room and turning drawers into desks.
Many psychologists expressed a strong need for control. Psychologists seek not only to have a sense ofcontrol of their clients but also control of the context for therapy. As a consequence, all psychologistsinterviewed described design strategies purposefully implemented for therapy sessions. Most design strategiesconsisted of controlling what people could or could not see. Psychologists spoke of positioning clocks andhow it was important that clients could or could not see them. Psychologists managed to divvy up thecounseling room into multiple visual fields by privileging themselves with views that only they could observe.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 6 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
For example, some therapists had images of personal significance mounted on the wall above their clients’heads. These images were intentionally mounted in such a manner so the client would not notice them. Onepsychologist intentionally located his offices on the second floor of a building because all the windows on thatlevel were reflective. The tint and reflectivity of the windows prevented individuals on the street from seeing atherapy session in progress.
In this psychologist's office, clients can see out, but outsiders cannotsee in due to the reflective windows. This helps protect clients'privacy.
Diffuse spot lighting was a common technique used to focus a session and encourage clients to disclosesensitive information. Floor lamps lit up corners and framed seating areas during later hours.
A clear need for all psychologists was that an office communicates the appropriate social scripts necessary fora successful therapeutic session. In this regard, the design of psychologists’ offices varied according to theguiding philosophy and associated social role of each psychologist. Psychologists who were inclined to take apsychoanalytic and humanistic philosophy offered seating that was warm and comforting. In addition,psychologists made an effort to imply that the psychologist-client relationship was that of a team. Thepsychologist did not sit any higher than the client, and both often sat in similar seats with the psychologist’schair facing the client. Yet on occasion, stepping outside the designated social roles implied by the design ofthe therapeutic setting did have its consequences:
“A client picked the hard, straight-back chair. So I fell into the beanbag chair, and it really, really upset her.”(Psychologist No. 5)

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 7 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Client's view of the psychologist's office. Note the full-length viewof a private garden, making this by far one of the most user-friendlyoffice environments for both therapist and clients
Psychologists had to rely on security methods when presented with a potentially harmful client. A commonmeasure used to mitigate a confrontation between a psychologist and a client was to provide an easy means ofegress for clients in case they became upset. Also, psychologists placed their chairs away from the path leadingto the doorway, believing that anxious clients felt comforted by having a clearly defined exit.
Psychologists emphasized a desire to keep a client’s attention on the session at hand. Windows were beneficialin anchoring a client to the therapeutic setting by offering natural views onto greenery. Even thoughpsychologists favored having the natural light from a window looking onto a street or sidewalk, they listeddrawbacks such as sporadic cars and passersby diverting a client’s focus. In addition, windows looking outonto public areas threatened the privacy of clientele. As a result, many psychologists kept blinds drawn overtheir windows, causing offices to be dimly lit. One psychologist avoided such problems with the use ofclerestory windows.
Plants and small items were also used to keep the client focused on the therapy session at hand. Two femalepsychologists catering to a female clientele displayed collections of figurines and stuffed animals. Malepsychologists often presented gender-neutral objects and those reflecting sporting interests such asphotographs of motorcycles and bicycles and prints of natural scenery. Many psychologists emphasized theneed for an office with a warm, home-like appearance—comfortable chairs, framed pictures, wood shelving,plants, soft colors, and lamps.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 8 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
A psychologist's visual image of her office. It featured the comfortassociated with a homelike interior.
Thermal conditions of a therapeutic space were often troublesome. Many psychologists struggled with thermalcontrol when neighboring businesses shared the same thermostat. Certain seasons and times of day whenwindow exposures were hit hard by the sun caused overheating and discomfort. One psychologist used a spaceheater to compensate for the drafty winter air leaking through his windows.
Psychologists favored spaces with neutral colors, believing that these had a calming effect. Creams and whiteswere common. Carpets often were soft green or maroon. Shelves and furniture were often made of stainedwood and upholstered with patterned fabrics.
One of the most critical needs for psychologists’ offices was the ability to adapt to ongoing change. Whethermoving into a new office or taking on additional clientele (in, say, shifting focus to family therapy),psychologists required spaces that would easily respond to their needs. In new offices, places to sit had to benegotiated to accommodate previously practiced social roles. If necessary, a few psychologists were evenwilling to rearrange furniture for specific clients. Flexible, sizable rooms were favored in this regard.
Privacy was another need that psychologists felt their office environments should reflect. Many offices hadtheir own adjoining waiting rooms. Some psychologists staggered appointments with those of their colleaguesso that clients would not run into each other. Psychologists who shared offices with other units in mental healthcenters or other businesses in an office building often could rely on anonymity to protect any given client’sprivacy:
"Having our own waiting room is certainly a privacy issue. But the location of the office is not as much of anissue [because] it’s a building that has a variety of businesses in it. Anyone coming into the building isn’tnecessarily seeing a therapist." (Psychologist No. 2)

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 9 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
This busy intersection was adjacent to a mental health facility.Clients had to park on one side of the intersection and then wait tocross. Psychologists felt it overexposed clientele and threatenedconfidentiality.
Psychologists often cited noise as a threat to privacy. They complained of thin walls and hollow-core doorsthat bled conversations through to the adjoining waiting room. They used radios and indoor water features toprovide white noise. Insulated interior walls and those constructed with concrete or brick were effective.
Psychologists believed that their clientele already dealt with too much chaos outside of the therapeutic setting.Accordingly, most believed it necessary to keep their offices in good order for therapy sessions. However,psychologists in both administrative and counseling positions who accumulated large volumes of paperworkoften found it difficult to portray a sense of order.Some of their desks conveyed a sense of disorder and disarray.
In this office, the client's view consists of the psychologist's computerand a messy desk. This office also lacked windows.
Often, psychologists made their empathetic intentions clearer by displaying positive images on walls for aclient’s easy view, maintaining a comfortable proximity in relation to the client, maintaining healthy plants,and showcasing items such as signs with healing phrases and small angel statuettes. The cumulative effect ofsatisfying all the needs listed above was that of an empathetic and caring holding environment—one reflecting

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 10 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
a psychologist's desire to foster positive therapeutic transactions with clientele.
Conclusion and discussionThis study explored psychologists as users of design with an environment-fit paradigm. Its goal was to identifyways in which psychologists use their offices to reinforce their competency and control over therapeutictransactions with clients. In-depth interviews and content analyses revealed that physical features ofpsychologists’ offices provide resources for what psychologists perceived were their own needs as well asthose of their clients. Several environmental responses facilitated the meeting of needs and, in turn, a fit orcongruency between an office and a psychologist.
Given the importance of physical features in the designs of psychologists’ offices to meet therapeutic needs,designers and researchers should expand upon the repertoire of healthcare environments to includepsychologists’ offices. Such an enhanced definition would accommodate issues unique to psychologists’offices and allow comparisons between psychologists’ offices and other therapeutic environments.
Psychologists whose offices did not meet their needs perceived these spaces as satisfactory for their clientelebut not ideal. Most of the psychologists were housed in office space that they defined as less than ideal fortherapeutic transactions. Consequently, relationships between therapeutic needs and environmental responsesfluctuated. For example, some offices were too small and required rearrangement of furniture to suit thedemands of an upcoming therapy session.
Psychologists considered certain design features prerequisites for a healthy, therapeutic environment and forpositive outcomes among clients. The important physical features of psychologists’ offices were analogous tothose identified by Evans (2003) for most therapeutic settings and those suggested by Pressly and Heesacker(2001) and Goldstein (1998) specific to psychologists’ offices. For example, psychologists believed that a quietenvironment, control over the design of the office, views of nature including water and trees, indoor plants,and landscape paintings were restorative, reduced stress, and facilitated therapeutic transactions. Fluorescentlighting should be avoided as it leads to clients' discomfort and anxiety. Abstract works of art whose content isdeliberately ambiguous and can be subject to potentially negative interpretations should not be displayed(Ulrich 1999). Comfortable seating arrangements must meet proxemic requirements but not be so comfortableas to induce sleepiness. Several psychologists preferred neutral colors so as not to provoke anxiety associatedwith vibrant colors such as red and orange.
In most cases, psychologists’ offices engaged clients’ sense of vision. Consequently, the designs of manyoffices were underused as tactile, auditory, and olfactory components within treatment and diagnosis. Incontrast to Klein (1949), the physical design of psychologists’ offices was also underused as an indicator oftransferences. Consistent with prior literature, many psychologists would use the nonverbal behaviors ofclients’ seating habits as indicators of a therapeutic session’s progress (Saari 2002; Satir 1964; Shefflen 1973).One cognitive-behavioral psychologist used a dinner table around which he and his clients sat to fill out testsand negotiate homework tasks. Another used clients’ attachments to stuffed animals as indicators ofunconscious, underlying feelings. However, treatment and diagnosis were usually relegated to talking andsitting, not playing or acting.
Psychologists must recognize the discrepancies between their own viewpoints of their offices and those oftheir clients. Their photographs and drawings revealed that they and their clients have dramatically differentperspectives of the same office. Many psychologists had views of bookshelves and framed images, whileclients faced a blinking computer screen and a desk cluttered with paper. Many of the psychologists were not

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 11 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
aware of this discrepancy between viewpoints until they were asked to take the client’s perspective.
The dynamics between therapeutic needs and environmental responses varied depending upon whether thepsychologist was engaged in private practice or was a team member of a consortium or a mental health center(Luhrman 2000). For example, many large healthcare facilities frequently relocate their counseling departmentsto accommodate the changing needs of other departments. As a result, counseling offices are often housed inwindowless basements and cramped quarters.
This plan for a hypothetical Psychological Services Center at auniversity shows clear separation between the research staff, support,and therapeutic areas. It allows clients to exit inconspicuously aftertherapy without parading through the waiting room and allowstherapists and research staff to circulate without clients seeing them.Privacy concerns like these are paramount and must be integratedsensitively into the design of therapeutic environments.Source: Cannon Design Healthcare Design Studio participants Coral Brandt, Jill Kirchherr, and SelwaNadhimi
Psychologists’ offices serve as workspaces laden with the territoriality and symbolism associated with otheroffice environments (Joiner 1971; Sundstrom 1986). Ironically, some mental health facilities forcepsychologists to work in deplorable offices that inhibit personalization and territoriality. Several psychologistsspoke of dissatisfying internships in inadequate offices. Many recalled windowless rooms with little privacy.One psychologist recalled an internship spent in a former gynecologist’s office. The psychologist was forced tomeet clientele with a decrepit gynecologist's chair positioned in the center of the room. Whether they areclinicians at mental health centers, private clinicians, or interns, psychologists should receive some opportunityand adequate resources to select and design spaces for therapy.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 12 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Psychologists seem to take a trial-and-error approach when designing their offices. None of the psychologistsinterviewed had been taught how to design their offices. None used professional interior designers. Graduateschools of clinical and counseling psychology ought to train future clinicians on the importance of the officeenvironment in the therapeutic process. Students could be informed about where to place lamps and clocks andhow to personalize a space without intruding on a client's field of vision. Graduate training could address howand where to set up office environments with adequate views, lighting, and seating. Indeed, the discrepanciesbetween clients’ versus psychologists’ viewpoints of psychologists’ offices underscore that good designpractices are not intuitive.
Conducting a qualitative study was advantageous given the exploratory nature of the research. Psychologistswelcomed one-on-one interviews to discuss their offices, procedures that were compatible with those useddaily when treating clients. In the future, the needs and responses revealed by the researchers in this studycould be used in the development of a questionnaire.
Future research could isolate one specific need (e.g., privacy) or response and examine it in detail. Researcherscould study the relationship between a specific therapeutic approach and the design of psychologists’ offices.Further studies could focus specifically on either psychologists in private practice or those working for mentalhealth centers. More important, future research can underscore that psychologists’ offices are not onlyworkspaces but also therapeutic environments affecting how well therapy might or might not be performed. Inan era of competitive healthcare, clients who have a choice might gravitate to psychologists’ offices that appearrestorative and uplifting.
REFERENCES
Alexander, C. (1970). The goodness of fit and its source. In H.M. Proshansky, W.H. Ittelson, & L.G. Rivlin(Eds.), Environmental psychology: Man and His Physical Setting. New York: Holt, Rinehart, and Winston.
Anthony, K. H. (1998). Designing for psychotherapists’ offices: Reflections of an environment-behaviorresearcher. Presentation as part of a symposium on environments for psychotherapy—problems in officedesign at the national convention of the American Psychological Association, San Francisco, August.
Anthony, K.H., and N.J. Watkins (2002a). Exploring pathology: Relationships between clinical andenvironmental psychology. In R. Bechtel and A. Churchman (Eds.), Handbook of Environmental Psychology.New York: John Wiley & Sons.
______ (2002b). Safe havens or perilous ports? The design of psychotherapists’ offices. In P. Hecht (Ed.),Community: Evolution or revolution? Proceedings of the 33rd annual conference of the Environmental DesignResearch Association (EDRA), Edmond, Okla.: EDRA.
Bechtel, R.B. (1997). Environment and Behavior: An Introduction. Thousand Oaks, Calif.: Sage Publications.
Carspecken, P.F. (1996). Critical Ethnography in Educational Research: A Theoretical and Practical Guide.New York: Routledge.
Demick, J., and C. Andreoletti (1995). Some relations between clinical and environmental psychology.Environment and Behavior, 27, 56–72.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 13 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Evans, G.W., and J.M.M. McCoy (1998). When buildings don’t work: The role of architecture in humanhealth. Journal of Environmental Psychology, 18, 85–94.
Evans, G.W. (2003). The built environment and mental health. Journal of Urban Health, 80, 536–554.
Goffman, I. (1961). Asylums. Garden City, N.Y.: Doubleday.
Goldstein, W.N. (1998). A Primer for Beginning Psychotherapy. Washington, D.C.: Brunner/Mazel.
Good, L.R, S.M. Siegel, and A.P. Bay (1965). Therapy by Design: Implications of Architecture for HumanBehavior. Springfield, Ill.: CC Thomas.
Goodman, P. (1962). Utopian Essays and Practical Proposals. New York: Random House.
Gustafson, P. (2001). Roots and routes: Exploring the relationship between place attachment and mobility.Journal of Environmental Psychology, 33, 667–686.
Horvath, A.O., and L. Luborsky (1993). The role of the therapeutic alliance in psychotherapy. Journal ofConsulting and Clinical Psychology, 61, 561–573.
Ittelson, W.H, H.M. Proshansky, and L.G. Rivlin (1970). The environmental psychology of the psychiatricward. In H.M. Proshansky, W.H. Ittelson, W.H., Rivlin L.G. (Eds.), Environmental Psychology: Man and HisPhysical Setting. New York: Holt, Rinehart, and Winston.
Joiner, D. (1971). Office territory. New Society, 7, 660–663.
Klein, M. (1949). The Psychoanalysis of Children. London: Hogarth.
Kristoff, A.L. (1996). Person-organization fit: An integrative review of its conceptualizations, measurement,and implications. Personnel Psychology, 49, 1–51.
Kvale, S. (1996). Interviews: An Introduction to Qualitative Research Interviewing. Thousand Oaks, Calif.:Sage.
Lang, J. (1987). Creating Architectural Theory: The Role of the Behavioral Sciences in Environmental Design.New York: Van Nostrand Reinhold.
Lawrence, D.L., and S. Low (1990). The built environment and spatial form. Annual Review of Anthropology,19, 453–505.
Lawton, M.P. (1989). Behavior-relevant ecological factors. In K.W. Schaie, & C. Schooler (Eds.), SocialStructure and Aging: Psychological Processes. Hillsdale, N.J.: Lawrence Erlbaum Associates.
Lincoln, Y.S., and E.G. Guba (1985). Naturalistic Inquiry. Beverly Hills, Calif.: Sage.
Luhrman, T.M. (2000). Of Two Minds: An Anthropologist Looks at American Psychiatry. New York: Vintage.
Mazumdar, S., and G. Geis (2001). Case study method for research on disability. In B.N. Altman, & S.Barnartt (Eds.), Research in Social Science and Disability. New York: Elsevier.
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 14 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Mazumdar, S. (2002). “Qualitative” research methods: An introduction and inquire into Its scientific qualities.Journal of Asian Urban Studies, 3, 21–28.
McCormick, M., and M.M. Shepley (2003). How can consumers benefit from therapeutic environments?Journal of Environmental Psychology, 20, 4–15.
McLoughlin, B. (1995). Developing Psychodynamic Counselling. London: Sage.
Mitchell, R.R., and H.S. Friedman (1994). Sandplay: Past, Present, and Future. London: Routledge.
Miwa, Y., and K. Hanyu (2006). The Effects of Interior Design on Communication and Impressions of aCounselor in a Counseling Room. Environment and Behavior, 38, 484–502.
Moos, R.H. (1973). Conceptualization of human environments. American Psychologist, 28, 652–665.
Osmond, H. (1957). Function as the basis of psychiatric ward design. Mental Hospital, 8, 23–30.
Peled, A., and O. Ayalon (1988). The role of the spatial organization of the home in family therapy: A casestudy. Journal of Environmental Psychology, 8, 87–106.
Pipes, R.B., and D.S. Davenport (1999). Introduction to Psychotherapy: Common Clinical Wisdom. 2nd ed.Boston: Allyn and Bacon.
Pressly, P.K., and M. Heesacker (2001). The physical environment and counseling: A review of theory andresearch. Journal of Counseling and Development, 79, 148–160.
Saari, C. (2002). The Environment: Its Role in Psychosocial Functioning and Psychotherapy. New York:Columbia University Press.
Sachs, N.A. (1999). Psychiatric hospitals. In C.C. Marcus, & M. Barnes (Eds.), Healing Gardens: TherapeuticBenefits and Design Recommendations. New York: John Wiley & Sons.
Satir, V. (1964). Conjoint Family Therapy: A Guide to Theory and Technique. Palo Alto, Calif.: Science andBehavior Books.
Scheflen, A.E. (1965). The institutionalized, the institution-prone and the institution. Psychiatric Quarterly, 39,203–219.
_____ (1973). Communicational Structure: Analysis of a Psychotherapy Transaction. Bloomington: IndianaUniversity Press.
Sherrod, D.R., and S. Cohen (1982). Density, personal control, and design. In S. Kaplan, & R. Kaplan (Eds.),Humanscape: Environments for People. Ann Arbor, Mich.: Ulrich’s Books.
Sommer, R. (1969). Personal Space: The Behavioral Basis of Design. Englewood Cliffs, N.J.:Prentice Hall.
Spivack, M. (1984). Institutional Settings: An Environmental Design Approach. New York: Human SciencesPress.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 15 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Stern, D. B. (1997). Unformulated Experience: From Dissociation to Imagination in Psychoanalysis. Hillsdale,N.J.: The Analytic Press.
Stevenson, C. (2000). Medicine and Magnificence: British Hospital and Asylum Architecture, 1660–1815. NewHaven: Yale University Press.
Stokols, D. (1979). A congruence analysis of stress. In I. Saranson, & C. Spielberger (Eds.), Stress andAnxiety, Vol. 6. New York: Hemisphere.
Stokols, D., H.C. Clitheroe Jr., and M. Zmuidzinas (2000). Modeling and managing change in people-environment transactions. In W.B. Walsh, K.H. Craik, and H.R. Price (Eds.), Person-Environment Psychology:New Directions and Perspectives. 2nd ed. Mahwah, N.J.: Erlbaum.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for developinggrounded theory. London: Sage.
Sundstrom, E. (1986). Work places: The psychology of the physical environment in offices and factories. NewYork: Cambridge University Press.
Timko, C., Moos, R.H., & Finney, J.W. (2000). Models of matching patients and treatment programs. In B.W.Walsh, & K.H. Craik (Eds.), Person-environment psychology: New directions and perspectives. 2nd ed.Mahwah, NJ: Erlbaum.
Trost, J. (1986). Statistically nonrepresentative stratified sampling: A sampling technique for qualitativestudies. Qualitative Sociology, 9, 54-57.
Ulrich, R.S. (1999). Effects of gardens on health outcomes: Theory and research. In C.C. Marcus, & M. Barnes(Eds.), Healing gardens: Therapeutic benefits and design recommendations. New York: John Wiley & Sons.
Ulrich, R.S., Simons, R.F., & Miles, M.A. (2003). Effects of environmental simulations and television onblood donor stress. Journal of Architectural and Planning Research, 20, 38-47.
Wachtel, P.L., & Messer, S.B. (1997). Theories of psychotherapy: Origins and evolution. AmericanPsychological Association, Washington, DC.
Williams, S.M. (1994). Environment and mental health. John Wiley & Sons.
Winnicott, D.W. (1953). Transitional objects and transitional phenomena. International Journal of Psycho-analysis, 34, 89-97.
_____. (1986). Holding and interpretation: Fragment of an analysis. New York: Grove Press.
Nicholas J. Watkins, PhD, is the director of research for Cannon Design in St. Louis. He earned his doctoratein social and cultural factors in design from the University of Illinois at Urbana-Champaign.
Kathryn H. Anthony, PhD, is a professor in the School of Architecture, Department of Landscape Architecture,and Gender and Women’s Studies Program at the University of Illinois at Urbana-Champaign. She earned herdoctorate in architecture from the University of California at Berkeley.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 16 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Article
Researchers have investigated the therapeutic value of institutional healthcareenvironments such as hospitals and Alzheimer’s facilities in fostering positive medicaloutcomes and recovery from stress (McCormick and Shepley 2003). Several researchershave discussed the lack of research about psychologists’ offices (Anthony 1998;Anthony and Watkins 2002a; Anthony and Watkins 2002b). Experimental research lacksexternal validity because actual psychologists, psychologists’ offices, and clientele havenot been used (Miwa and Hanyu 2006). As such, psychologists’ offices have been largelyabsent from contemporary theoretical and methodological discussions of therapeuticenvironments.
Psychologists recognize that their clients suffer from stressors related to mental illnessand daily routines. Clients also suffer stress from making a life transition involvingdiscomfort and disclosure of private information within an unfamiliar setting (Demick andAndreoletti 1995; McLoughlin 1995; Spivack 1984). Consequently, how, if at all, dopsychologists believe that their office designs contribute to the therapeutic process? Howdo psychologists compensate for the inadequacies of their therapeutic environments?Answers to these questions could guide future research on and design of psychologists’offices.
Environments for the treatment of mental illnessWhen an imbalance exists between the demand posed by a stressor and a person’sperceived resources to adaptively respond to the stressor, stress occurs (Stokols 1979;Stokols et al. 2000). A stressor might overwhelm a person’s physical and psychologicalresources and, as a result, cause a person to feel incompetent (Stokols et al. 2000).Evans and McCoy (1998) identify negative, stressful experiences resulting from therelationship between physical environments and a person’s psychology. These conceptsinclude overstimulation resulting from crowding and ambiguous spatial configurations.
Researchers and designers have long expressed interest in creating healthcareenvironments that mitigate stress. Healing gardens, views of nature, and legible buildingplans and signage have been well documented as design features that contribute topositive psychological and physiological health (Evans and McCoy 1998; Ulrich 1999;Ulrich et al. 2003).
Researchers have extensively investigated institutions such as psychiatric facilities andtheir possible negative effects on mental health. Their research reveals that the design ofa psychiatric facility can reinforce rigid social programs and patterns of behavior amongpatients and staff (Bechtel 1997; Goffman 1961; Schefflen 1965; Stevenson 2000).Consequently, the design of an institution reflects its philosophy of care (Bechtel 1997;Stevenson 2000; Williams 1994). For instance, in the 19th century, Thomas Kirkbridedesigned mental hospitals for the humane treatment of patients. His designs required oneroom for each patient, double-loaded main corridors, wards terminating with sunlit bays,and access to natural settings (Good et al. 1965; Sachs 1999).
Critics warn that the physical designs of many mental institutions exacerbate patients’conditions. Fortress-like facades reinforce the larger community’s stigma of the mentallyill (Ittelson et al. 1970; Stevenson 2000). Commons areas equipped with fixed seatinginhibit social interaction (Osmond 1957; Sommer 1969). Spaces efficient for staff, such asradial plans and long corridors lined with easy-to-clean surfaces, convey a sense ofsterility and distort patients’ already disturbed perceptions with illusions and glare(Ittelson et al. 1970; Spivack 1984). Ironically, the design of mental institutions can

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 17 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
(Ittelson et al. 1970; Spivack 1984). Ironically, the design of mental institutions canundermine the competence of the patient, thereby worsening the patient’s illness (Moos1973; Timko et al. 2000).
Similarly, a psychologist’s office both communicates and facilitates communication.People imbue the environment with psychosymbolic meaning formed through interactionswith the environment (Lawrence and Low 1990). Likewise, office features andpsychologist-client transactions have psychosymbolic importance. Obvious symbolic cuesinclude artwork, desks, and diplomas (Pressly and Heesacker 2001). Less obvious formsof communication include those physical features that reflect the psychologist-clienttransaction and those integral to treatment and diagnosis. In general, the therapeuticsetting should be a holding environment; psychologists and their offices should providecomfortable and secure environments within which clients feel free to communicatesensitive information (Saari 2002; Winnicott 1986).
Clients and psychologists communicate through transference relationships (Wachtel andMesser 1997; Saari 2002). Horvath and Lubrosky (1993) state that a transference“implies that emotions and thoughts associated with the unresolved relationships withsignificant others are bound to be displaced (transferred) onto the relationship with thetherapist” (p. 562). Transferences are imbued with feelings that the client andpsychologist hold for each other and for inanimate objects (Winnicott 1953). Frompositive transferences, the psychologist and client develop a “working alliance” to relievethe client of distress (Pipes and Davenport 1999; Horvath and Lubrosky 1993).
Saari’s (2002) concept of interpsychic space is the nonverbal, spatial expression ofpositive and negative transferences through proxemics and personal space. For Stern(1997), an interpersonal field opens a context for disclosure between a psychologist anda client. Similarly, Satir (1964), Shefflen (1973), and Sommer (1969) have alldemonstrated that in mental health settings, clients communicate psychological statesnonverbally with seating arrangements and the manipulation of nonfixed physicalfeatures. Psychologists can influence transferences through their intentionalmanipulations of space. For instance, Henry Stack Sullivan sat across a desk from hisschizophrenic clients because such an arrangement focused their attention on therapy(Goodman 1962).
Psychologists record transferences with the physical manipulation of their therapeuticenvironments. In the process, psychologists use space to treat and diagnose clients. Klein(1949) used play therapy with children so that transferences between psychologist andclient were expressed through toys. Lowenfield adapted Klein’s play therapy to trays ofsand. Play with sand trays enabled a healing connection with natural elements, whilehelping the psychologist reach a diagnosis (Mitchell and Friedman 1994). Peled andAyalon (1988) analyzed attachments to home as part of family therapy.
As is the case with other therapeutic environments, psychologists’ offices must alsoalleviate and adapt to stressors. Psychologists’ offices should convey holdingenvironments within which psychologist-client transactions are accommodated. Also, theyshould empower psychologists to perform transactions necessary for maintaining aholding environment. Therefore, they should provide psychologists with the resourcesnecessary to adapt to the ongoing needs of therapy.
Environment-function fitA traditional measure of compatibility between an environment and the activitiesperformed within is environment-function fit (Alexander 1970; Sherrod and Cohen 1982).A derivation of environment-function fit, person-environment congruency measures the
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 18 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
A derivation of environment-function fit, person-environment congruency measures therelationships between a person’s perceptions and the demands exerted by a sociophysicalenvironment (Lawton 1989). Researchers have applied person-environment congruencyto measure fit between the elderly and nursing home facilities and the mentally ill andpsychiatric facilities (Kristoff 1996; Lawton 1989; Moos 1973; Timko et al. 2000). Lawtontheorized that congruency occurred when a demand fell into a person’s perceivedcompetency to meet that demand. If so, either a person’s perceived control or actualcontrol over the demand increased.
The built environment is a resource that people use to exert control over demands andincrease competency (Alexander 1970). Flexible environments made of nonfixed featurescan create greater opportunities for fit (Lang 1987). At the other extreme, negative fitdecreases competency (Alexander 1970). Lower competency also results in decreasedperformance, increased stress, negative affect, and a lack of control (Lawton 1989).
Just as stress exacerbated by the environment of mental institutions and othertherapeutic environments reduces the competency of users, we suggest that the design ofa psychologist’s office provides a resource for mastery over the demands ofpsychotherapy. Therefore, environment-function fit could be a paradigm forunderstanding psychologists as users of design, and consequently, the function of designin psychologists’ offices.
Methodology
Participant sampleTen psychologists agreed to participate in a study of their office environments under thecondition that clientele were not to be included or discussed. Participants were all: (1)licensed counseling or clinical psychologists; (2) employed in private practice or by ahealthcare facility; (3) practicing within the city where the researchers were located.Subjects varied in psychotherapeutic philosophy from psychoanalytic to cognitive-behavioral. Six had a private practice, and four worked for a healthcare facility.
The sample’s composition conformed to principles of strategic nonrepresentative samplingformulated by Trost (1986) and used in prior research of built environments (Gustafson2001). Nonrepresentative sampling allows researchers to determine a sample reflective ofthe breadth of the topic under study without overrepresentation by any one characteristicof the sample. Each psychologist represented one private practice or healthcare facility.Conveniently, this prevented overrepresentation from any facility.
Procedures and measuresThe exploratory nature of the study and the sample size warranted an antipositiviticresearch approach emphasizing on-site research, richness of data, smaller sample size,less emphasis on generalizability, and identification of contextual factors and informationspecific to each subject’s unique experience (Mazumdar and Geis 2001; Mazumdar 2002).
Interviews were conducted within the therapeutic setting so that the researchers couldsee firsthand and discuss the unique design features of each office and so thatpsychologists could describe their offices in detail.
Researchers used techniques of questioning described by Carspecken (1996) and Kvale(1996): specifically, descriptive questions, nonleading leads, and low-inferenceparaphrasing. After each interview, the researcher and psychologist reviewed the topicsdiscussed on the interview guide to assess verification between the researcher’s andpsychologist’s interpretations of questions (Carspecken 1996). Such “member checking”

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 19 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
psychologist’s interpretations of questions (Carspecken 1996). Such “member checking”ensured the “trustworthiness” and validity of the data (Lincoln and Guba 1985). Allinterviews were transcribed verbatim.
AnalysesGrounded theory was used to identify categories within each interview and acrossinterviews (Mazumdar and Geis 2001; Strauss and Corbin 1998). The diversity of thesample controlled for theoretical sampling, during which collection and analyses of datacoincide to fill gaps in the data revealed during analyses (Noonan et. al. 2004; Patton1990). Extensive auditing ensured the dependability and confirmability of the results(Lincoln and Guba 1985). Concepts representing discrete parts of the interviews emergedthrough a process of open coding. Then, concepts were synthesized into larger categories.Axial coding further synthesized categories and revealed dimensions (“not valued” to“highly valued”). Also, axial coding identified connections between categories, revealingnovel interpretations of the data. Selective coding isolated two core categories as nucleiof the subjects’ experiences. Theoretical redundancy and saturation were achieved whenthe subjects’ transcribed interviews failed to generate categories beyond those alreadyexisting from the analyses. To assess the reliability and validity of the categories, theresearchers asked an impartial, independent researcher—blind to the analyses and thecoding of the categories—to code random samples from the transcripts.
ResultsThe content analysis produced two core categories important to the design ofpsychologists’ offices. Consistent with theories of person-environment congruence,categories of needs and responses emerged (Kristoff 1996). As shown in Table 1, the firstcategory included therapeutic needs identified by the psychologists, i.e., criteria that theybelieved were necessary for successful psychotherapy. The second category consisted ofenvironmental responses that psychologists implemented in response to therapeuticneeds. Both the therapeutic needs and environmental responses express psychologists’desire to accommodate their clientele and relieve stressors imposed by therapy. All 10psychologists stressed the importance of therapeutic needs but differed with respect towhat environmental responses were highly valued in meeting those needs.
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 20 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Table 1. All 10 psychologists identified severaltherapeutic needs as well as environmentalresponses to meet those needs. The value placed oneach environmental response varied by psychologist.
Therapeutic needs included practicality, control, cueing of appropriate social roles,security, comfort, adaptability, privacy, order, and empathy. Environmental responses totherapeutic needs consisted of clocks, lighting, proxemics, seating, windows, color,staffing, thermal comfort, gender-friendly décor, location, noise control, nonfixedfeatures, room size, and plants. If environmental responses could not be met adequately,psychologists adapted the best they could. They valued therapeutic spaces that wereflexible.
Psychologists stressed that their offices needed to be both economical and functional.Many of the therapists engaged in private practice shared an office space with a colleagueto cut the cost of rent. The functional necessities of an office were illustrated by a casewhere the office did not accommodate the special needs of a psychologist with adisability. The psychologist adapted to the space by placing all furniture to the exterior ofthe room and turning drawers into desks.
Many psychologists expressed a strong need for control. Psychologists seek not only tohave a sense of control of their clients but also control of the context for therapy. As aconsequence, all psychologists interviewed described design strategies purposefullyimplemented for therapy sessions. Most design strategies consisted of controlling whatpeople could or could not see. Psychologists spoke of positioning clocks and how it wasimportant that clients could or could not see them. Psychologists managed to divvy up thecounseling room into multiple visual fields by privileging themselves with views that onlythey could observe. For example, some therapists had images of personal significancemounted on the wall above their clients’ heads. These images were intentionally mountedin such a manner so the client would not notice them. One psychologist intentionallylocated his offices on the second floor of a building because all the windows on that levelwere reflective. The tint and reflectivity of the windows prevented individuals on thestreet from seeing a therapy session in progress.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 21 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
In this psychologist's office, clients can see out, butoutsiders cannot see in due to the reflective windows.This helps protect clients' privacy.
Diffuse spot lighting was a common technique used to focus a session and encourageclients to disclose sensitive information. Floor lamps lit up corners and framed seatingareas during later hours.
A clear need for all psychologists was that an office communicates the appropriate socialscripts necessary for a successful therapeutic session. In this regard, the design ofpsychologists’ offices varied according to the guiding philosophy and associated socialrole of each psychologist. Psychologists who were inclined to take a psychoanalytic andhumanistic philosophy offered seating that was warm and comforting. In addition,psychologists made an effort to imply that the psychologist-client relationship was that ofa team. The psychologist did not sit any higher than the client, and both often sat insimilar seats with the psychologist’s chair facing the client. Yet on occasion, steppingoutside the designated social roles implied by the design of the therapeutic setting didhave its consequences:
“A client picked the hard, straight-back chair. So I fell into the beanbag chair, and itreally, really upset her.” (Psychologist No. 5)
Client's view of the psychologist's office. Note the full-length view of a private garden, making this by farone of the most user-friendly office environments for

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 22 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
both therapist and clients
Psychologists had to rely on security methods when presented with a potentially harmfulclient. A common measure used to mitigate a confrontation between a psychologist and aclient was to provide an easy means of egress for clients in case they became upset. Also,psychologists placed their chairs away from the path leading to the doorway, believingthat anxious clients felt comforted by having a clearly defined exit.
Psychologists emphasized a desire to keep a client’s attention on the session at hand.Windows were beneficial in anchoring a client to the therapeutic setting by offeringnatural views onto greenery. Even though psychologists favored having the natural lightfrom a window looking onto a street or sidewalk, they listed drawbacks such as sporadiccars and passersby diverting a client’s focus. In addition, windows looking out onto publicareas threatened the privacy of clientele. As a result, many psychologists kept blindsdrawn over their windows, causing offices to be dimly lit. One psychologist avoided suchproblems with the use of clerestory windows.
Plants and small items were also used to keep the client focused on the therapy sessionat hand. Two female psychologists catering to a female clientele displayed collections offigurines and stuffed animals. Male psychologists often presented gender-neutral objectsand those reflecting sporting interests such as photographs of motorcycles and bicyclesand prints of natural scenery. Many psychologists emphasized the need for an office witha warm, home-like appearance—comfortable chairs, framed pictures, wood shelving,plants, soft colors, and lamps.
A psychologist's visual image of her office. Itfeatured the comfort associated with a homelikeinterior.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 23 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Thermal conditions of a therapeutic space were often troublesome. Many psychologistsstruggled with thermal control when neighboring businesses shared the same thermostat.Certain seasons and times of day when window exposures were hit hard by the suncaused overheating and discomfort. One psychologist used a space heater to compensatefor the drafty winter air leaking through his windows.
Psychologists favored spaces with neutral colors, believing that these had a calmingeffect. Creams and whites were common. Carpets often were soft green or maroon.Shelves and furniture were often made of stained wood and upholstered with patternedfabrics.
One of the most critical needs for psychologists’ offices was the ability to adapt toongoing change. Whether moving into a new office or taking on additional clientele (in,say, shifting focus to family therapy), psychologists required spaces that would easilyrespond to their needs. In new offices, places to sit had to be negotiated to accommodatepreviously practiced social roles. If necessary, a few psychologists were even willing torearrange furniture for specific clients. Flexible, sizable rooms were favored in thisregard.
Privacy was another need that psychologists felt their office environments should reflect.Many offices had their own adjoining waiting rooms. Some psychologists staggeredappointments with those of their colleagues so that clients would not run into each other.Psychologists who shared offices with other units in mental health centers or otherbusinesses in an office building often could rely on anonymity to protect any given client’sprivacy:
"Having our own waiting room is certainly a privacy issue. But the location of the office isnot as much of an issue [because] it’s a building that has a variety of businesses in it.Anyone coming into the building isn’t necessarily seeing a therapist." (Psychologist No. 2)
This busy intersection was adjacent to a mental healthfacility. Clients had to park on one side of theintersection and then wait to cross. Psychologists felt itoverexposed clientele and threatened confidentiality.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 24 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Psychologists often cited noise as a threat to privacy. They complained of thin walls andhollow-core doors that bled conversations through to the adjoining waiting room. Theyused radios and indoor water features to provide white noise. Insulated interior walls andthose constructed with concrete or brick were effective.
Psychologists believed that their clientele already dealt with too much chaos outside ofthe therapeutic setting. Accordingly, most believed it necessary to keep their offices ingood order for therapy sessions. However, psychologists in both administrative andcounseling positions who accumulated large volumes of paperwork often found it difficultto portray a sense of order.Some of their desks conveyed a sense of disorder and disarray.
In this office, the client's view consists of thepsychologist's computer and a messy desk. This officealso lacked windows.
Often, psychologists made their empathetic intentions clearer by displaying positiveimages on walls for a client’s easy view, maintaining a comfortable proximity in relationto the client, maintaining healthy plants, and showcasing items such as signs with healingphrases and small angel statuettes. The cumulative effect of satisfying all the needs listedabove was that of an empathetic and caring holding environment—one reflecting apsychologist's desire to foster positive therapeutic transactions with clientele.
Conclusion and discussionThis study explored psychologists as users of design with an environment-fit paradigm.Its goal was to identify ways in which psychologists use their offices to reinforce theircompetency and control over therapeutic transactions with clients. In-depth interviews

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 25 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
competency and control over therapeutic transactions with clients. In-depth interviewsand content analyses revealed that physical features of psychologists’ offices provideresources for what psychologists perceived were their own needs as well as those of theirclients. Several environmental responses facilitated the meeting of needs and, in turn, afit or congruency between an office and a psychologist.
Given the importance of physical features in the designs of psychologists’ offices to meettherapeutic needs, designers and researchers should expand upon the repertoire ofhealthcare environments to include psychologists’ offices. Such an enhanced definitionwould accommodate issues unique to psychologists’ offices and allow comparisonsbetween psychologists’ offices and other therapeutic environments.
Psychologists whose offices did not meet their needs perceived these spaces assatisfactory for their clientele but not ideal. Most of the psychologists were housed inoffice space that they defined as less than ideal for therapeutic transactions.Consequently, relationships between therapeutic needs and environmental responsesfluctuated. For example, some offices were too small and required rearrangement offurniture to suit the demands of an upcoming therapy session.
Psychologists considered certain design features prerequisites for a healthy, therapeuticenvironment and for positive outcomes among clients. The important physical features ofpsychologists’ offices were analogous to those identified by Evans (2003) for mosttherapeutic settings and those suggested by Pressly and Heesacker (2001) and Goldstein(1998) specific to psychologists’ offices. For example, psychologists believed that a quietenvironment, control over the design of the office, views of nature including water andtrees, indoor plants, and landscape paintings were restorative, reduced stress, andfacilitated therapeutic transactions. Fluorescent lighting should be avoided as it leads toclients' discomfort and anxiety. Abstract works of art whose content is deliberatelyambiguous and can be subject to potentially negative interpretations should not bedisplayed (Ulrich 1999). Comfortable seating arrangements must meet proxemicrequirements but not be so comfortable as to induce sleepiness. Several psychologistspreferred neutral colors so as not to provoke anxiety associated with vibrant colors suchas red and orange.
In most cases, psychologists’ offices engaged clients’ sense of vision. Consequently, thedesigns of many offices were underused as tactile, auditory, and olfactory componentswithin treatment and diagnosis. In contrast to Klein (1949), the physical design ofpsychologists’ offices was also underused as an indicator of transferences. Consistentwith prior literature, many psychologists would use the nonverbal behaviors of clients’seating habits as indicators of a therapeutic session’s progress (Saari 2002; Satir 1964;Shefflen 1973). One cognitive-behavioral psychologist used a dinner table around whichhe and his clients sat to fill out tests and negotiate homework tasks. Another usedclients’ attachments to stuffed animals as indicators of unconscious, underlying feelings.However, treatment and diagnosis were usually relegated to talking and sitting, notplaying or acting.
Psychologists must recognize the discrepancies between their own viewpoints of theiroffices and those of their clients. Their photographs and drawings revealed that they andtheir clients have dramatically different perspectives of the same office. Manypsychologists had views of bookshelves and framed images, while clients faced a blinkingcomputer screen and a desk cluttered with paper. Many of the psychologists were notaware of this discrepancy between viewpoints until they were asked to take the client’sperspective.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 26 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
The dynamics between therapeutic needs and environmental responses varied dependingupon whether the psychologist was engaged in private practice or was a team member ofa consortium or a mental health center (Luhrman 2000). For example, many largehealthcare facilities frequently relocate their counseling departments to accommodate thechanging needs of other departments. As a result, counseling offices are often housed inwindowless basements and cramped quarters.
This plan for a hypothetical Psychological ServicesCenter at a university shows clear separation betweenthe research staff, support, and therapeutic areas. Itallows clients to exit inconspicuously after therapywithout parading through the waiting room and allowstherapists and research staff to circulate without clientsseeing them. Privacy concerns like these are paramountand must be integrated sensitively into the design oftherapeutic environments.Source: Cannon Design Healthcare Design Studio participants Coral Brandt, Jill Kirchherr, and SelwaNadhimi
Psychologists’ offices serve as workspaces laden with the territoriality and symbolismassociated with other office environments (Joiner 1971; Sundstrom 1986). Ironically,some mental health facilities force psychologists to work in deplorable offices that inhibitpersonalization and territoriality. Several psychologists spoke of dissatisfying internshipsin inadequate offices. Many recalled windowless rooms with little privacy. Onepsychologist recalled an internship spent in a former gynecologist’s office. Thepsychologist was forced to meet clientele with a decrepit gynecologist's chair positioned
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 27 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
psychologist was forced to meet clientele with a decrepit gynecologist's chair positionedin the center of the room. Whether they are clinicians at mental health centers, privateclinicians, or interns, psychologists should receive some opportunity and adequateresources to select and design spaces for therapy.
Psychologists seem to take a trial-and-error approach when designing their offices. Noneof the psychologists interviewed had been taught how to design their offices. None usedprofessional interior designers. Graduate schools of clinical and counseling psychologyought to train future clinicians on the importance of the office environment in thetherapeutic process. Students could be informed about where to place lamps and clocksand how to personalize a space without intruding on a client's field of vision. Graduatetraining could address how and where to set up office environments with adequate views,lighting, and seating. Indeed, the discrepancies between clients’ versus psychologists’viewpoints of psychologists’ offices underscore that good design practices are notintuitive.
Conducting a qualitative study was advantageous given the exploratory nature of theresearch. Psychologists welcomed one-on-one interviews to discuss their offices,procedures that were compatible with those used daily when treating clients. In thefuture, the needs and responses revealed by the researchers in this study could be usedin the development of a questionnaire.
Future research could isolate one specific need (e.g., privacy) or response and examine itin detail. Researchers could study the relationship between a specific therapeuticapproach and the design of psychologists’ offices. Further studies could focus specificallyon either psychologists in private practice or those working for mental health centers.More important, future research can underscore that psychologists’ offices are not onlyworkspaces but also therapeutic environments affecting how well therapy might or mightnot be performed. In an era of competitive healthcare, clients who have a choice mightgravitate to psychologists’ offices that appear restorative and uplifting.
REFERENCES
Alexander, C. (1970). The goodness of fit and its source. In H.M. Proshansky, W.H.Ittelson, & L.G. Rivlin (Eds.), Environmental psychology: Man and His Physical Setting.New York: Holt, Rinehart, and Winston.
Anthony, K. H. (1998). Designing for psychotherapists’ offices: Reflections of anenvironment-behavior researcher. Presentation as part of a symposium on environmentsfor psychotherapy—problems in office design at the national convention of the AmericanPsychological Association, San Francisco, August.
Anthony, K.H., and N.J. Watkins (2002a). Exploring pathology: Relationships betweenclinical and environmental psychology. In R. Bechtel and A. Churchman (Eds.), Handbookof Environmental Psychology. New York: John Wiley & Sons.
______ (2002b). Safe havens or perilous ports? The design of psychotherapists’ offices.In P. Hecht (Ed.), Community: Evolution or revolution? Proceedings of the 33rd annualconference of the Environmental Design Research Association (EDRA), Edmond, Okla.:EDRA.
Bechtel, R.B. (1997). Environment and Behavior: An Introduction. Thousand Oaks, Calif.:Sage Publications.
Carspecken, P.F. (1996). Critical Ethnography in Educational Research: A Theoretical and
6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 28 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Carspecken, P.F. (1996). Critical Ethnography in Educational Research: A Theoretical andPractical Guide. New York: Routledge.
Demick, J., and C. Andreoletti (1995). Some relations between clinical and environmentalpsychology. Environment and Behavior, 27, 56–72.
Evans, G.W., and J.M.M. McCoy (1998). When buildings don’t work: The role ofarchitecture in human health. Journal of Environmental Psychology, 18, 85–94.
Evans, G.W. (2003). The built environment and mental health. Journal of Urban Health,80, 536–554.
Goffman, I. (1961). Asylums. Garden City, N.Y.: Doubleday.
Goldstein, W.N. (1998). A Primer for Beginning Psychotherapy. Washington, D.C.:Brunner/Mazel.
Good, L.R, S.M. Siegel, and A.P. Bay (1965). Therapy by Design: Implications ofArchitecture for Human Behavior. Springfield, Ill.: CC Thomas.
Goodman, P. (1962). Utopian Essays and Practical Proposals. New York: Random House.
Gustafson, P. (2001). Roots and routes: Exploring the relationship between placeattachment and mobility. Journal of Environmental Psychology, 33, 667–686.
Horvath, A.O., and L. Luborsky (1993). The role of the therapeutic alliance inpsychotherapy. Journal of Consulting and Clinical Psychology, 61, 561–573.
Ittelson, W.H, H.M. Proshansky, and L.G. Rivlin (1970). The environmental psychology ofthe psychiatric ward. In H.M. Proshansky, W.H. Ittelson, W.H., Rivlin L.G. (Eds.),Environmental Psychology: Man and His Physical Setting. New York: Holt, Rinehart, andWinston.
Joiner, D. (1971). Office territory. New Society, 7, 660–663.
Klein, M. (1949). The Psychoanalysis of Children. London: Hogarth.
Kristoff, A.L. (1996). Person-organization fit: An integrative review of itsconceptualizations, measurement, and implications. Personnel Psychology, 49, 1–51.
Kvale, S. (1996). Interviews: An Introduction to Qualitative Research Interviewing.Thousand Oaks, Calif.: Sage.
Lang, J. (1987). Creating Architectural Theory: The Role of the Behavioral Sciences inEnvironmental Design. New York: Van Nostrand Reinhold.
Lawrence, D.L., and S. Low (1990). The built environment and spatial form. AnnualReview of Anthropology, 19, 453–505.
Lawton, M.P. (1989). Behavior-relevant ecological factors. In K.W. Schaie, & C. Schooler(Eds.), Social Structure and Aging: Psychological Processes. Hillsdale, N.J.: LawrenceErlbaum Associates.
Lincoln, Y.S., and E.G. Guba (1985). Naturalistic Inquiry. Beverly Hills, Calif.: Sage.
Luhrman, T.M. (2000). Of Two Minds: An Anthropologist Looks at American Psychiatry.New York: Vintage.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 29 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Mazumdar, S., and G. Geis (2001). Case study method for research on disability. In B.N.Altman, & S. Barnartt (Eds.), Research in Social Science and Disability. New York:Elsevier.
Mazumdar, S. (2002). “Qualitative” research methods: An introduction and inquire intoIts scientific qualities. Journal of Asian Urban Studies, 3, 21–28.
McCormick, M., and M.M. Shepley (2003). How can consumers benefit from therapeuticenvironments? Journal of Environmental Psychology, 20, 4–15.
McLoughlin, B. (1995). Developing Psychodynamic Counselling. London: Sage.
Mitchell, R.R., and H.S. Friedman (1994). Sandplay: Past, Present, and Future. London:Routledge.
Miwa, Y., and K. Hanyu (2006). The Effects of Interior Design on Communication andImpressions of a Counselor in a Counseling Room. Environment and Behavior, 38, 484–502.
Moos, R.H. (1973). Conceptualization of human environments. American Psychologist, 28,652–665.
Osmond, H. (1957). Function as the basis of psychiatric ward design. Mental Hospital, 8,23–30.
Peled, A., and O. Ayalon (1988). The role of the spatial organization of the home in familytherapy: A case study. Journal of Environmental Psychology, 8, 87–106.
Pipes, R.B., and D.S. Davenport (1999). Introduction to Psychotherapy: Common ClinicalWisdom. 2nd ed. Boston: Allyn and Bacon.
Pressly, P.K., and M. Heesacker (2001). The physical environment and counseling: Areview of theory and research. Journal of Counseling and Development, 79, 148–160.
Saari, C. (2002). The Environment: Its Role in Psychosocial Functioning andPsychotherapy. New York: Columbia University Press.
Sachs, N.A. (1999). Psychiatric hospitals. In C.C. Marcus, & M. Barnes (Eds.), HealingGardens: Therapeutic Benefits and Design Recommendations. New York: John Wiley &Sons.
Satir, V. (1964). Conjoint Family Therapy: A Guide to Theory and Technique. Palo Alto,Calif.: Science and Behavior Books.
Scheflen, A.E. (1965). The institutionalized, the institution-prone and the institution.Psychiatric Quarterly, 39, 203–219.
_____ (1973). Communicational Structure: Analysis of a Psychotherapy Transaction.Bloomington: Indiana University Press.
Sherrod, D.R., and S. Cohen (1982). Density, personal control, and design. In S. Kaplan, &R. Kaplan (Eds.), Humanscape: Environments for People. Ann Arbor, Mich.: Ulrich’s Books.
Sommer, R. (1969). Personal Space: The Behavioral Basis of Design. Englewood Cliffs,

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 30 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Sommer, R. (1969). Personal Space: The Behavioral Basis of Design. Englewood Cliffs,N.J.:Prentice Hall.
Spivack, M. (1984). Institutional Settings: An Environmental Design Approach. New York:Human Sciences Press.
Stern, D. B. (1997). Unformulated Experience: From Dissociation to Imagination inPsychoanalysis. Hillsdale, N.J.: The Analytic Press.
Stevenson, C. (2000). Medicine and Magnificence: British Hospital and AsylumArchitecture, 1660–1815. New Haven: Yale University Press.
Stokols, D. (1979). A congruence analysis of stress. In I. Saranson, & C. Spielberger(Eds.), Stress and Anxiety, Vol. 6. New York: Hemisphere.
Stokols, D., H.C. Clitheroe Jr., and M. Zmuidzinas (2000). Modeling and managing changein people-environment transactions. In W.B. Walsh, K.H. Craik, and H.R. Price (Eds.),Person-Environment Psychology: New Directions and Perspectives. 2nd ed. Mahwah, N.J.:Erlbaum.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques andprocedures for developing grounded theory. London: Sage.
Sundstrom, E. (1986). Work places: The psychology of the physical environment in officesand factories. New York: Cambridge University Press.
Timko, C., Moos, R.H., & Finney, J.W. (2000). Models of matching patients and treatmentprograms. In B.W. Walsh, & K.H. Craik (Eds.), Person-environment psychology: Newdirections and perspectives. 2nd ed. Mahwah, NJ: Erlbaum.
Trost, J. (1986). Statistically nonrepresentative stratified sampling: A sampling techniquefor qualitative studies. Qualitative Sociology, 9, 54-57.
Ulrich, R.S. (1999). Effects of gardens on health outcomes: Theory and research. In C.C.Marcus, & M. Barnes (Eds.), Healing gardens: Therapeutic benefits and designrecommendations. New York: John Wiley & Sons.
Ulrich, R.S., Simons, R.F., & Miles, M.A. (2003). Effects of environmental simulations andtelevision on blood donor stress. Journal of Architectural and Planning Research, 20, 38-47.
Wachtel, P.L., & Messer, S.B. (1997). Theories of psychotherapy: Origins and evolution.American Psychological Association, Washington, DC.
Williams, S.M. (1994). Environment and mental health. John Wiley & Sons.
Winnicott, D.W. (1953). Transitional objects and transitional phenomena. InternationalJournal of Psycho-analysis, 34, 89-97.
_____. (1986). Holding and interpretation: Fragment of an analysis. New York: GrovePress.
Nicholas J. Watkins, PhD, is the director of research for Cannon Design in St. Louis. Heearned his doctorate in social and cultural factors in design from the University of Illinoisat Urbana-Champaign.

6/21/11 10:04 AMThe Design of Psychologists' Offices: A Qualitative Evaluation of Environment-Function Fit
Page 31 of 31http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20071101_watkins
Kathryn H. Anthony, PhD, is a professor in the School of Architecture, Department ofLandscape Architecture, and Gender and Women’s Studies Program at the University ofIllinois at Urbana-Champaign. She earned her doctorate in architecture from theUniversity of California at Berkeley.
© 2004 The American Institute of Architects | www.aia.org