metastatic spinal cord compression dr sally hall dr hannah gunn on behalf of mscc group
TRANSCRIPT

Metastatic Spinal Cord Compression
Dr Sally Hall
Dr Hannah Gunn
on behalf of MSCC group

Overview
Background to the MSCC audit March 2012 audit Recommendations and what might be
changing

Background
>100 cases per cancer network per year
Patients present acutely via different specialties
Diagnosis frequently delayed Time matters for neurological
recovery

Background
NICE Metastatic Spinal Cord Compression guidelines 2008Early detectionImagingTreatmentSupportive care & rehabCoordination of the service

Background Local audits NUTH/JCUH 2009 and 2011
using NICE standardsPatient education Chaotic pathway & delays (particularly for
patients from other trusts)Poor documentation & use of NCCC
pathwayPoor communication between specialtiesDifficulty capturing all patients

2012
New MSCC pathway document to be piloted soon across specialtieslocal then regionalpathway would move with the patientshould streamline patient journey named coordinators
MSCC group suggested a further audit whilst document being finalised

Case identification- March
16 patients with confirmed MSCC (bone mets/ vertebral collapse/ direct tumour involvement /invasion)
3 excluded: notes unavailable& insufficient information on Diadem/ PACS

Patient location 13 patients
9 referred to NUTH with ? MSCC from another hospital
0
0.5
1
1.5
2
2.5
3
3.5
North T
ynes
ide
Wan
sbec
k
Sunder
land
QEH
UHND
Darlin
gton
NCCC
RVI A&E G
P
Number of patients

Primary tumour site and metastatic disease
2
4
3
2
1
1
Breast
Lung
Prostate
Lymphoma
Myeloma
Extra-Skeletal EwS
3
6
6 New cancerdiagnosis
New diagnosis ofbone mets
Bone mets alreadyknown about

Did the patient exhibit signs and/or symptoms suggestive of spinal metastases?
Symptom Number of patients
Percentage
Pain in thoracic or cervical spine 7 54%
Progressive lumbar spinal pain 3 23%
Severe unremitting lower spinal pain 1 8%
Spinal pain aggravated by straining 0 0%
Localised spinal tenderness 4 31%
Nocturnal pain preventing sleep 0 0%
Neurological symptoms 13 92%
Neurological signs 9 69%

MSCC Coordinator
Neurosurgery = 5 patients Oncology = 8 patients
none had the old NCCC pathway document one NCCC ward no longer has copies (!)
Difficult to know when the coordinator was contacted, especially for patients being transferred from a peripheral hospital ranges from same day to 5 days telephone/ email/ MDT

MRI scanning
Whole spine imaging is the gold standard
Should be done to allow definitive treatment planning within 1 week of suspected MSCC for spinal pain or 24hours for neurological signs/symptoms suggestive of MSCC
92 % (12 patients) had whole spines done remaining patient underwent
CT
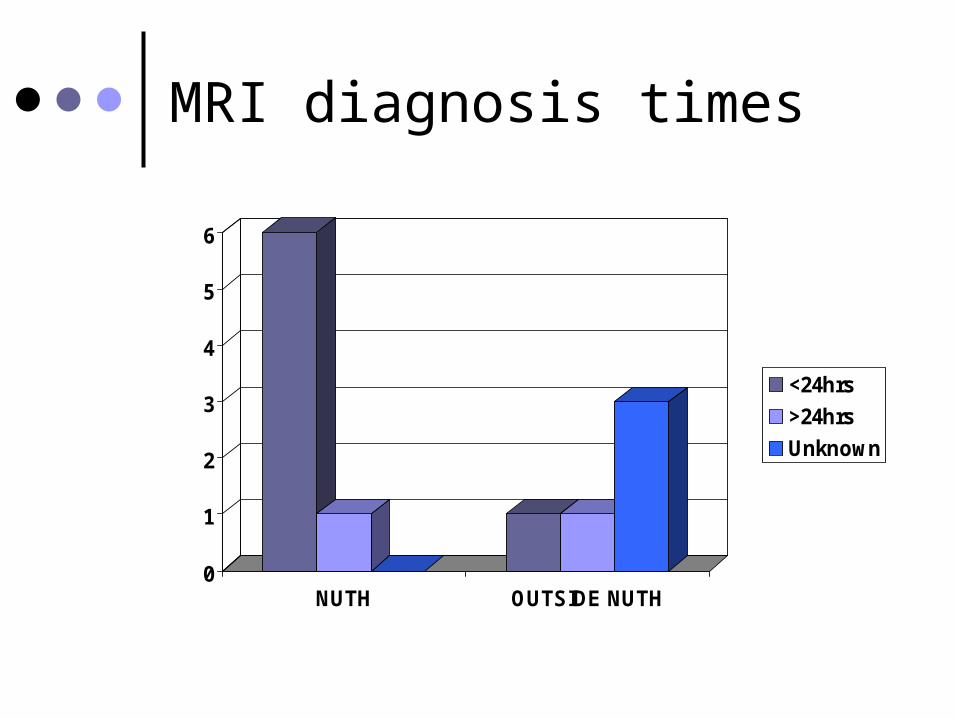
MRI diagnosis times
0
1
2
3
4
5
6
NUTH OUTSIDE NUTH
<24hrs
>24hrs
Unknown

Once MSCC confirmed…
All patients documented as receiving steroids but varying doses
VTE assessments documented in 53% (7 patients)
No documentation about being nursed flat/ stability of spine
Mobility on discharge not documented Discussions between Neurosurgery and
Oncology commented on in 46% (6 patients)

Definitive Treatment
One surgical candidate (subsequent radiotherapy)
everyone else treated with radiotherapy
? why delay from diagnosis to DXT treatment times 0
1
2
3
4
5
6
7
<24hrs unknown
numberofpatients
>48hrs

Summary
QUALITY STANDARD NCCC 2009 JCUH 2011 NCCC 2011 NCCC 2012
Whole spine MRI 100% 70% 80% 85% 92%
SPINAL PAIN
Definitive rx planning 1 week
100% unclear 18.5% 38% 63%
NEURO SX
Definitive rx planning 24hrs
100% unclear 51.6% 62% 54%

Limitations
• Retrospective for March• Unable to include 3 sets of patients
• 2 of these were surgical candidates• Number of patients that had surgery
suspiciously low ? not capturing all patients
• Referring hospital notes not always available

Recommendations & future planning
Introduction of new standardised MSCC pathway document
Should help improve standards and aid future audit
Role of MSCC coordinators Education locally, then regionally&
across specialties and grades