mental illness adult psychopathology definitions of mental health vs. illness vary: culture: great...
TRANSCRIPT

MENTAL ILLNESSMENTAL ILLNESS
ADULT PSYCHOPATHOLOGYADULT PSYCHOPATHOLOGY
Definitions of mental health vs. illness vary:Definitions of mental health vs. illness vary:• culture: great variabilityculture: great variability• SES (a rich man is eccentric, a poor one is SES (a rich man is eccentric, a poor one is
mad)mad)• age: more acceptance of ‘odd’ behaviours age: more acceptance of ‘odd’ behaviours
in the elderlyin the elderly• gender: different cultural expectations, gender: different cultural expectations,
less tolerance of deviance in womenless tolerance of deviance in women

ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)
Ideal vs. real mental health (e.g. text)Ideal vs. real mental health (e.g. text)• Difference between stress and coping Difference between stress and coping
mechanisms, which can sometimes be mechanisms, which can sometimes be maladaptive, and full blown mental illness.maladaptive, and full blown mental illness.
• Change is always stressful, individual Change is always stressful, individual variation in optimal levels of stress.variation in optimal levels of stress.
• Summation of stresses as we age: Summation of stresses as we age: depletion of coping resources vs. depletion of coping resources vs. development of better coping strategies.development of better coping strategies.
ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)
Important personal variables:Important personal variables:• past historypast history• personalitypersonality• social supportssocial supports• SESSES• locus of control (women, poor and elderly locus of control (women, poor and elderly
more external)more external)• longevity (higher incidence)longevity (higher incidence)

ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)
Bottom line criterion for mental illness:Bottom line criterion for mental illness:• inability to functioninability to function
Importance of label, stigmaImportance of label, stigma
Relative influence of nature vs. nurture Relative influence of nature vs. nurture
(heredity/environment):(heredity/environment):• the higher the genetic predisposition, the the higher the genetic predisposition, the
fewer environmental insults needed to fewer environmental insults needed to produce mental illness.produce mental illness.
ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)
Most common model of mental illness:Most common model of mental illness:• medical modelmedical model
Medical model:Medical model:• a series of culturally unacceptable a series of culturally unacceptable
behaviours is ‘packaged’ into a diagnostic behaviours is ‘packaged’ into a diagnostic category.category.
DSM:DSM:• no uniform, testable criteria.no uniform, testable criteria.

ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)Each category has:Each category has:• Symptoms (mix of behavioural and Symptoms (mix of behavioural and
physical)physical)• Underlying cause (etiology)Underlying cause (etiology)• Treatment (can be just palliative or geared Treatment (can be just palliative or geared
to eradicate the cause)to eradicate the cause)Approaches:Approaches:• biologicalbiological• psychologicalpsychological• combination of bothcombination of both

ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)
Biological approach:Biological approach:• organic causes (brain)organic causes (brain)• treatment: drugs, ECT, surgerytreatment: drugs, ECT, surgery
Psychological approach:Psychological approach:• causes: stress, emotions, personality, childhood causes: stress, emotions, personality, childhood
experiences, poor coping strategiesexperiences, poor coping strategies• treatment: psychotherapy (rare for the elderly)treatment: psychotherapy (rare for the elderly)
Combination approach:Combination approach:• causes: both organic and environmentalcauses: both organic and environmental• treatment: usually drugs and some level of treatment: usually drugs and some level of
psychotherapypsychotherapy

ADULT PSYCHOPATHOLOGY (Cont’d)ADULT PSYCHOPATHOLOGY (Cont’d)Etiology of mental illness:Etiology of mental illness:• organic, e.g. Alzheimer'sorganic, e.g. Alzheimer's• functional or psychic, e.g. phobiasfunctional or psychic, e.g. phobias• organic + environment, e.g. mostorganic + environment, e.g. most• ““problems in living” (Szasz)problems in living” (Szasz)
Treatments:Treatments:• drugsdrugs• ECTECT• psychotherapiespsychotherapies• out vs. inpatientout vs. inpatient

• strokestroke• heart attackheart attack• malnutritionmalnutrition• traumatrauma• tumorstumors• infectionsinfections• electrolite imbalanceelectrolite imbalance
• diabetesdiabetes• thyroid dysfunctionthyroid dysfunction• liver dysfunctionliver dysfunction• drugsdrugs• alcohol (Korsakoff alcohol (Korsakoff
syndrome)syndrome)• surgery (anesthesia) surgery (anesthesia)
Brain disorders (delirium in text – covers only acute disorders) can be acute or chronic.Acute: rapid onset, reversible with treatment.Chronic: slow and gradual onset, degenerative, irreversible.Acute Brain Disorders:Many possible causes:
Some symptoms:• confusion• disorganized thinking
• agitation• changes in sensation and perception
Chronic Brain DisordersChronic Brain Disorders
Schizophrenia: Schizophrenia: • onset between ages 13 and 30, chroniconset between ages 13 and 30, chronic• Delusions: Delusions:
• thought disorders, belief systemthought disorders, belief system
• Hallucinations: Hallucinations: • sensory perceptions not based on actual, real stimulisensory perceptions not based on actual, real stimuli
• Inappropriate AffectInappropriate Affect• Managed with drugs Managed with drugs
Unfortunately, the reversible illnesses are treated as irreversible in the elderly, therefore depriving them of a possible cure.

Depression:Depression:
Very high incidence all ages. Two types:Very high incidence all ages. Two types:
1.1. Unipolar: depression only, more common in Unipolar: depression only, more common in older adults.older adults.
2.2. Bipolar: alternating depression and mania, also Bipolar: alternating depression and mania, also called manic-depression. More common in the called manic-depression. More common in the young.young.
Depression can also be:Depression can also be:• Reactive: acute, short duration, due to events, Reactive: acute, short duration, due to events,
responds to psychotherapy alone, support.responds to psychotherapy alone, support.• Chronic: long term, resistant to psychotherapy, Chronic: long term, resistant to psychotherapy,
often need physical therapies, e.g. drugs, ECT.often need physical therapies, e.g. drugs, ECT.

Drugs: Drugs: • tricyclics, MAO inhibitors, lithium (for tricyclics, MAO inhibitors, lithium (for
bipolar, very toxic to liver and kidneys, bipolar, very toxic to liver and kidneys, increases blood pressure), SSRIs: increases blood pressure), SSRIs: selective serotonin reuptake inhibitors, selective serotonin reuptake inhibitors, e.g. Prozac, Zoloft, Paxil, etc.e.g. Prozac, Zoloft, Paxil, etc.
• Side effects of drugs leads to low Side effects of drugs leads to low compliance. Also danger of drug compliance. Also danger of drug interactions (potentiate or decrease interactions (potentiate or decrease effect when combined with other drugs) effect when combined with other drugs) often dangerous.often dangerous.

ECT: ECT: • electroconvulsive therapy, “shock”, electroconvulsive therapy, “shock”,
memory deficits, brain damage possible. memory deficits, brain damage possible. Nobody knows how it works.Nobody knows how it works.
Psychoactive drugs for the elderly:Psychoactive drugs for the elderly:• Elderly need lower doses!!Elderly need lower doses!!• More problematic, as dosages have to More problematic, as dosages have to
be more carefully adjusted, usually be more carefully adjusted, usually downward. Also problem of interaction downward. Also problem of interaction with other drugs taken for other with other drugs taken for other problems. Polypharmacy.problems. Polypharmacy.

Some Signs of Depression:Some Signs of Depression:• dysphoriadysphoria• insomniainsomnia• fatiguefatigue• inability to enjoy things that were likedinability to enjoy things that were liked• changes in appetitechanges in appetite• crying jagscrying jags• despairdespair• apathyapathy• pessimismpessimism• differences between young and old: young differences between young and old: young
may cover it up bettermay cover it up better• impaired daily functioningimpaired daily functioning• negative thoughts, suicidal ideationnegative thoughts, suicidal ideation

• People with chronic illnesses very People with chronic illnesses very vulnerable to depressionvulnerable to depression
• Some diseases of middle/old age can Some diseases of middle/old age can also cause depression:also cause depression:
• CV diseaseCV disease• brain disorders (Parkinson’s, MS, brain disorders (Parkinson’s, MS,
dementias, etc.)dementias, etc.)• metabolic disturbances (e.g. diabetes, metabolic disturbances (e.g. diabetes,
thyroid)thyroid)• cancercancer• post-operatory periodpost-operatory period• many drugs can many drugs can causecause depression and depression and
suicidesuicide

Gender Issues:Gender Issues:• Gender: women socialized to self-blame, Gender: women socialized to self-blame,
more prone.more prone.• Age: depletion syndrome of the elderly, Age: depletion syndrome of the elderly,
somewhat similar to depression. It somewhat similar to depression. It increases with age, depression proper increases with age, depression proper decreases.decreases.
Role of marital status:Role of marital status:• Before age 65: higher incidence for Before age 65: higher incidence for
single men and married women.single men and married women.• After age 65: reverseAfter age 65: reverse

Gender Issues (Cont’d):Gender Issues (Cont’d):• Marriage improves men’s mental health. It Marriage improves men’s mental health. It
negatively affects women’s mental health. This negatively affects women’s mental health. This is reversed after age 65.is reversed after age 65.
• Men more likely to show:Men more likely to show:• ‘‘acting out’acting out’• alcoholismalcoholism• drug abusedrug abuse• criminal behaviourcriminal behaviour• reluctance to seek helpreluctance to seek help
• but, because of social male stereotypes, more but, because of social male stereotypes, more tolerance for the above and less likely to be tolerance for the above and less likely to be labelled and stigmatized.labelled and stigmatized.

Gender Issues (Cont’d):Gender Issues (Cont’d):• Women more likely to show:Women more likely to show:
• anxietyanxiety• depressiondepression• self-blamingself-blaming• intense emotional expressionintense emotional expression
• Women more likely to acknowledge Women more likely to acknowledge problems and seek help, and more likely problems and seek help, and more likely to be labelled, stigmatized and given to be labelled, stigmatized and given psychotropic medication. Influence of psychotropic medication. Influence of feminine stereotypes, powerlessness.feminine stereotypes, powerlessness.

Psychotherapy for the elderly:Psychotherapy for the elderly:• Not common. Most therapists not trained Not common. Most therapists not trained
to deal with problems of the elderly.to deal with problems of the elderly.• Higher tolerance for deviant behaviour.Higher tolerance for deviant behaviour.• Therapists more interested in YAVIS: Therapists more interested in YAVIS:
(young, attractive, verbal, intelligent, (young, attractive, verbal, intelligent, successful)successful)
• Expense (private or public)Expense (private or public)• Many elderly suspicious or reluctantMany elderly suspicious or reluctant

Organic Brain Disorders:Organic Brain Disorders:• Alzheimer’sAlzheimer’s• Multi-infarct dementiaMulti-infarct dementia• Huntington’s choreaHuntington’s chorea• Parkinson'sParkinson's• Lewy body dementiaLewy body dementia

Alzheimer’s Disease:Alzheimer’s Disease:• Chronic, irreversible, degenerative Chronic, irreversible, degenerative
disease of brain.disease of brain.• No known cause, some genetic markers No known cause, some genetic markers
– iffy– iffy• Type of dementia – brain syndromeType of dementia – brain syndrome• Parts of brain involved:Parts of brain involved:
• amygdala (emotions)amygdala (emotions)• hippocampus (memory)hippocampus (memory)• cerebral cortex (reason, judgment)cerebral cortex (reason, judgment)

Alzheimer’s – Histological ChangesAlzheimer’s – Histological Changes
1.1. Amyloid plaques: clusters of protein bits Amyloid plaques: clusters of protein bits that accumulate, causing inflammation that accumulate, causing inflammation and damaging neurons.and damaging neurons.
2.2. Neurofibrillary tangles: dendrites change Neurofibrillary tangles: dendrites change structure and disintegrate, leading the structure and disintegrate, leading the neuron to wither and die.neuron to wither and die.

Alzheimer’s
Affects
Amygdala Hippocampus Cortex
Personality Memory ReasoningAppetites Works Back- JudgmentEnergy wards DecisionsDrivesex: Irritable Fussy
Chronic, Irreversible DeathUsual Cause: Pneumonia8 mo. – 20 years

4 Phases:4 Phases:
1.1. Early Changes:Early Changes:• IrritabilityIrritability• ““Something Wrong”Something Wrong”• MemoryMemory• Cover-Ups & CompensationsCover-Ups & Compensations
Hard to AssessHard to Assess• RetrospectiveRetrospective

4 Phases (Cont’d):4 Phases (Cont’d):2.2.
• Memory WorseMemory Worse• ParanoiaParanoia• Odd, Inappropriate Social BehaviorOdd, Inappropriate Social Behavior• Needs Help (eg. banking, bills)Needs Help (eg. banking, bills)• Personality ChangePersonality Change
3.3.• Unsafe to Leave Alone Unsafe to Leave Alone • Poor ConcentrationPoor Concentration• Memory GoneMemory Gone
4.4.• TerminalTerminal• No CoordinationNo Coordination• Swallowing difficult or impossibleSwallowing difficult or impossible• AgitationAgitation• Bed RiddenBed Ridden
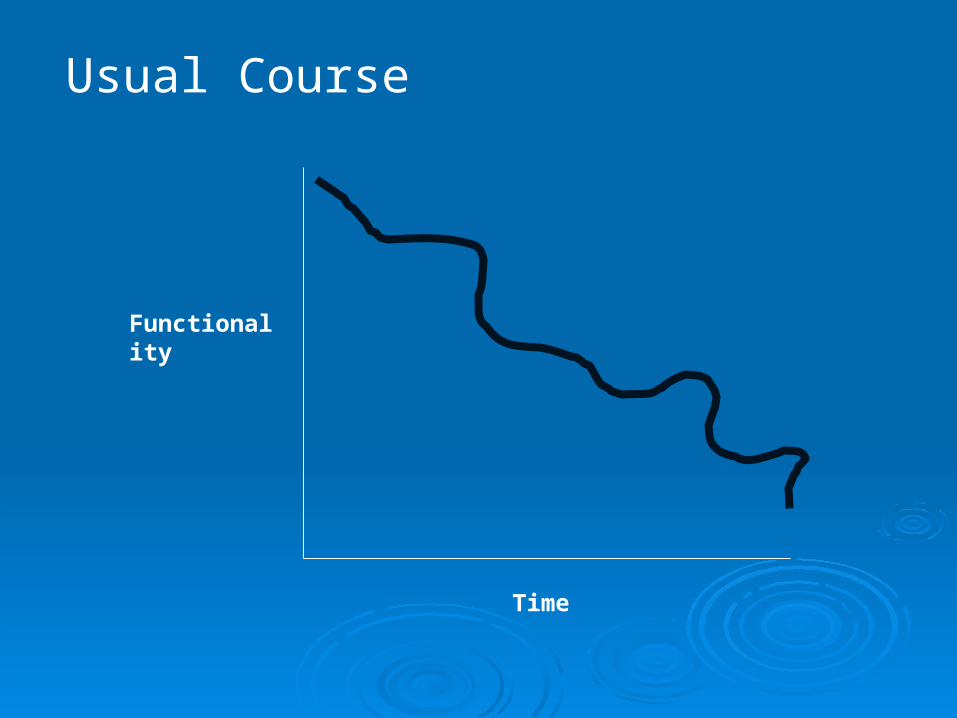
Usual Course
Functionality
Time


Assessment methods:Assessment methods:
1.1. Clinical interview (most common)Clinical interview (most common)
2.2. Self-report (reliability and validity?) e.g. Self-report (reliability and validity?) e.g. questionnairequestionnaire
3.3. Other’s report (relatives, neighbours)Other’s report (relatives, neighbours)
4.4. Psychophysiological (psychological Psychophysiological (psychological stimulus, physiological response) e.g. stimulus, physiological response) e.g. fearful stimulus-situation and EEG or fearful stimulus-situation and EEG or heart rateheart rate

Assessment methods:Assessment methods:
5.5. Direct observation in situ (e.g. nursing Direct observation in situ (e.g. nursing home dining room)home dining room)
6.6. Performance test (e.g. remembering list, Performance test (e.g. remembering list, drawing a picture after looking at it for 10 drawing a picture after looking at it for 10 seconds)seconds)
Critical areas:Critical areas:• cognitive functioningcognitive functioning• social cognitionsocial cognition• personalitypersonality
Must be preceded by medical exam to rule Must be preceded by medical exam to rule
out diseases or medication effects, and out diseases or medication effects, and
assessment of nutritional status.assessment of nutritional status.

• Genetics important only in early onset of Genetics important only in early onset of Alzheimer’s (age 30-60)Alzheimer’s (age 30-60)
• Increased evidence of some prevention Increased evidence of some prevention factors:factors:
• exerciseexercise• folatefolate• low cholesterollow cholesterol• low blood pressurelow blood pressure
MCI:MCI:• mild cognitive impairment, different from mild cognitive impairment, different from
Alzheimer’s and different from normal age-Alzheimer’s and different from normal age-related memory decline.related memory decline.
• Drugs may prevent progression to Alzheimer’sDrugs may prevent progression to Alzheimer’s

Multi-Infarct or Vascular Dementia:Multi-Infarct or Vascular Dementia:• Reduced blood flow to brain areas, due Reduced blood flow to brain areas, due
to either an arterial blockage (to either an arterial blockage (++85%) or a 85%) or a hemorrhage (hemorrhage (++15%)15%)
• Either ‘regular’ stroke or ‘mini’ stroke. Either ‘regular’ stroke or ‘mini’ stroke. The latter can go undetected, very brief The latter can go undetected, very brief symptoms: transient ischemic attack symptoms: transient ischemic attack (episode) TIA(episode) TIA
• E.g. brief fainting, acute brief headacheE.g. brief fainting, acute brief headache

Huntington’s ChoreaHuntington’s Chorea::Autosomal disorder, dominant gene. Test Autosomal disorder, dominant gene. Test
available. Expresses between ages 35 available. Expresses between ages 35 and 50. Physical and mental and 50. Physical and mental manifestations (see text)manifestations (see text)
• involuntary movements of limbsinvoluntary movements of limbs• difficulty with voluntary movementdifficulty with voluntary movement• hallucinationshallucinations• paranoiaparanoia• mood swingsmood swings• eventually unable to care for selfeventually unable to care for self

Parkinson’s diseaseParkinson’s disease::Characteristic: involuntary movements, Characteristic: involuntary movements,
cannot control but also cannot move cannot control but also cannot move some voluntary movements, rigidity.some voluntary movements, rigidity.
• hallucinationshallucinations• paranoiaparanoia• depressiondepression• mood swingsmood swings• eventually, cognitive declineeventually, cognitive decline• genetic test availablegenetic test available
L-dopa (medication)
• Neurons in the Neurons in the substantia nigrasubstantia nigra in the in the midbrain do not produce enough midbrain do not produce enough dopamine, an important dopamine, an important neurotransmitter.neurotransmitter.
• Initially physical symptoms only. Initially physical symptoms only. Eventually, up to 40% develop dementia, Eventually, up to 40% develop dementia, could be due to the illness or to the drugs could be due to the illness or to the drugs given. L-dopa, a synthetic dopamine, given. L-dopa, a synthetic dopamine, causes hallucinations and other causes hallucinations and other psychotic symptoms at certain dosages.psychotic symptoms at certain dosages.
• Lewy Body Dementia:Lewy Body Dementia:• abnormal brain structuresabnormal brain structures• progressive loss of memory, language, progressive loss of memory, language,
reasoningreasoning• faster progression than Alzheimer’sfaster progression than Alzheimer’s• more ups and downs than Alzheimer’s in more ups and downs than Alzheimer’s in
early stagesearly stages• psychotic symptoms as illness progressespsychotic symptoms as illness progresses

Substance abuse:Substance abuse:• In young adults, mostly by choice, though In young adults, mostly by choice, though
some by prescription medications.some by prescription medications.• In middle-aged (particularly women) and In middle-aged (particularly women) and
old adults, by prescribed medications old adults, by prescribed medications (tranquilizers, pain-killers, etc.)(tranquilizers, pain-killers, etc.)
• Very widespread in our societyVery widespread in our society• Males: alcohol most commonMales: alcohol most common• Females: sedatives, hypnotics, Females: sedatives, hypnotics,
psychotropic drugs most commonpsychotropic drugs most common