meier - palliative care 2020.ppt - nehcc · 1 palliative care 2020: matching care to patient and...
TRANSCRIPT

1
Palliative Care 2020: Matching Care to Patient and
Family NeedsFamily Needs
Diane E. Meier, MDDi tDirector
Center to Advance Palliative Care
www.getpalliativecare.org@dianeemeier
Disclosures
• I have no disclosures to report.
2
Objectives
1. How is palliative care important to f h l bl ?improving care of the most vulnerable?
2. How do we change the delivery system to improve access to quality palliative care for all persons with serious illness and their families?and their families?
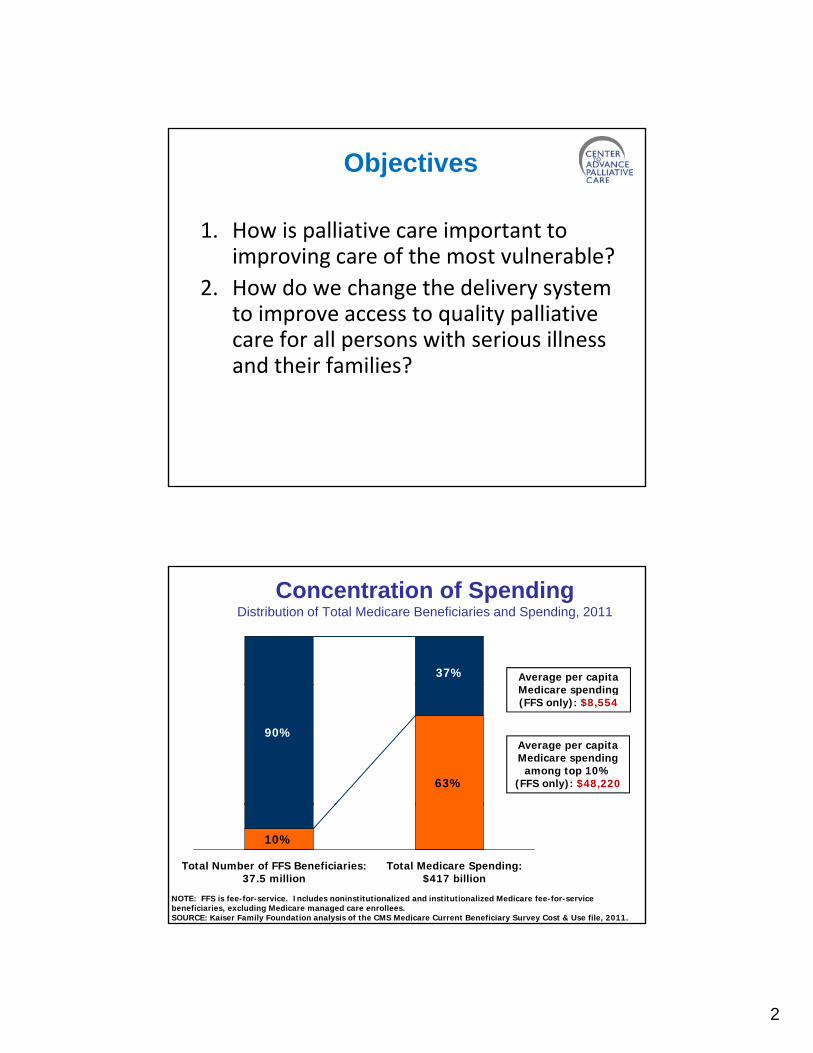
Concentration of SpendingDistribution of Total Medicare Beneficiaries and Spending, 2011
37% Average per capita
63%
90%
Medicare spending (FFS only): $8,554
Average per capita Medicare spending
among top 10% (FFS only): $48,220
10%
Total Number of FFS Beneficiaries: 37.5 million
Total Medicare Spending: $417 billion
NOTE: FFS is fee-for-service. Includes noninstitutionalized and institutionalized Medicare fee-for-service beneficiaries, excluding Medicare managed care enrollees. SOURCE: Kaiser Family Foundation analysis of the CMS Medicare Current Beneficiary Survey Cost & Use file, 2011.

3
Because of the concentration of risk (and spending)of risk (and spending), palliative care principles and practices are central to improving quality. Improved p g q y pquality reduces cost.
Mr.B• An 88 year old man with mild
dementia admitted via the ED for management of back pain due
to spinal stenosis and arthritisto spinal stenosis and arthritis.
• Pain is 8/10 on admission, for which he is taking a lot of acetaminophen.
• Admitted 4 times in 6 months for pain (2x), weight loss+falls, and altered mental status dueand altered mental status due to constipation.
• His family (83 year old wife) is overwhelmed.

4
Mr. B:• Mr. B: “I told the Dr. that I never
wanted to go back to the hospital again. It’s torture—you have no control and can’t do anything for y gyourself. And you get weaker and sicker. Every time I’m in the hospital it feels like I’ll never get out.”
• Mrs. B: “He hates being in the hospital, but what could I do? The p ,pain was terrible and I couldn’t reach the doctor. I couldn’t even move him myself, so I called the ambulance. It was the only thing I could do.”
Modified from and with thanks to Dave Casarett
Concentration of Risk
• Functional Limitation• Functional Limitation
• Dementia
• Frailty
S i ill ( )• Serious illness(es)
5
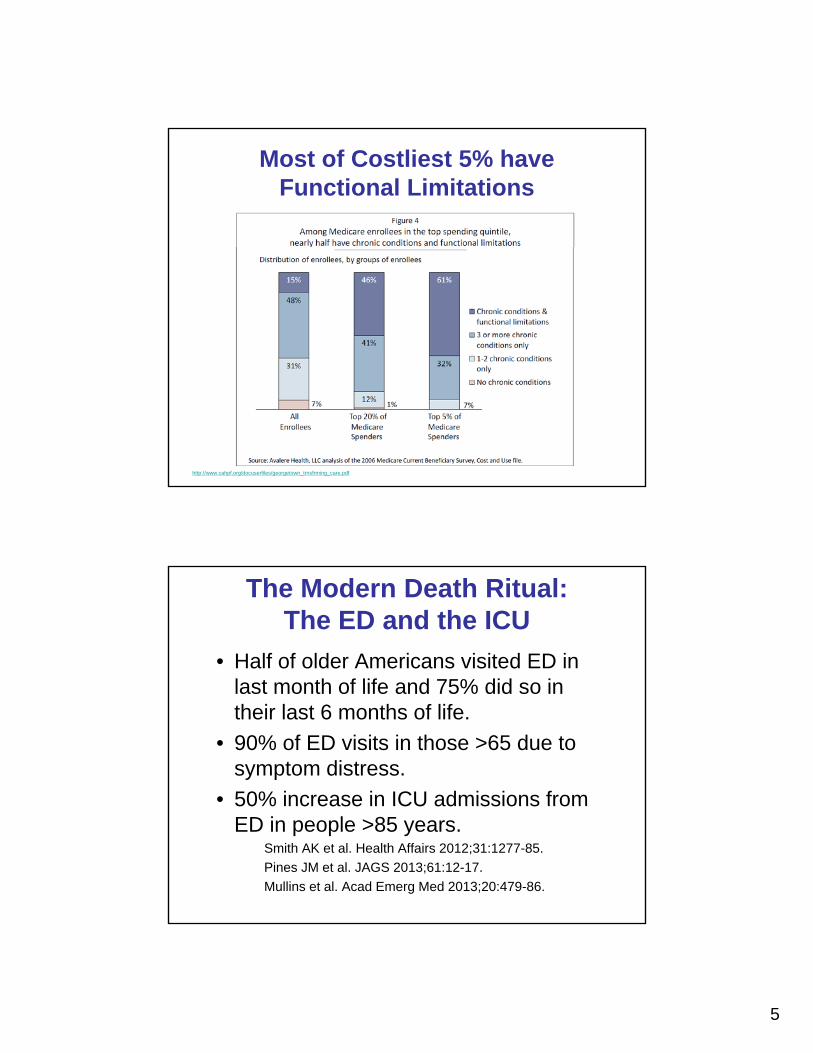
Most of Costliest 5% have Functional Limitations
http://www.cahpf.org/docuserfiles/georgetown_trnsfrming_care.pdf
The Modern Death Ritual: The ED and the ICU
• Half of older Americans visited ED in last month of life and 75% did so inlast month of life and 75% did so in their last 6 months of life.
• 90% of ED visits in those >65 due to symptom distress.
• 50% increase in ICU admissions from50% increase in ICU admissions from ED in people >85 years.
Smith AK et al. Health Affairs 2012;31:1277-85.
Pines JM et al. JAGS 2013;61:12-17.
Mullins et al. Acad Emerg Med 2013;20:479-86.

6
Dementia DrivesUtilization
Prospective
Cohort of Dementia No Dementia
community dwelling older adults
Callahan et al JAGS 2012;60:813-
Medicare SNF use 44.7% 11.4%
Medicaid NH use 21% 1.4%
Hospital use 76.2% 51.2%Callahan et al. JAGS 2012;60:813-20.
Home health use 55.7% 27.3%
Transitions 11.2 3.8
Dementia and Total Spend
• 2010: $215 billion/yr2010: $215 billion/yr
• By comparison: heart disease $102 billion; cancer $77 billion
• 2040 estimates> $375 billion/yr
Hurd MD et al. NEJM 2013;368:1326-34.
7
In case you are not already worried…The Future of Dementia Hospitalizations
and Long Term Services+Supports
10 fold growth in dementia related10 fold growth in dementia related hospitalizations projected between 2000 and 2050 to >7 million.
Zilberberg and Tija. Arch Int Med 2011;171:1850.
3 f ld i i d f f l LTSS3 fold increase in need for formal LTSS between now and 2050, from 9 to 27 million.
Lynn and Satyarthi. Arch Int Med 2011;171:1852.
•Highest risk, highest cost population: functional limitation
The 5%
population: functional limitation, frailty, cognitive impairment +/-serious illness(es)
•What are the roles of primary care teams in improving care of this population?

8
What is Palliative Care?• Specialized or generalist medical care for people with
serious illness and their families
Focused on improving quality of life as defined by• Focused on improving quality of life as defined by patients and families.
• Provided by an interdisciplinary team that works with patients, families, and other healthcare professionals to provide an added layer of support.
• Appropriate at any age, for any diagnosis, at any stage in i ill d id d t th ith ti da serious illness, and provided together with curative and
life-prolonging treatments.
Definition from public opinion survey conducted by ACS CAN and CAPC http://www.capc.org/tools‐for‐palliative‐care‐programs/marketing/public‐opinion‐research/2011‐public‐opinion‐research‐on‐palliative‐care.pdf
Conceptual Shift for Palliative Care
9
“Don’t ask what’s the matter with me. Ask what matters to me.”
Palliative Care Teams Address 3 Domains
1. Physical, emotional, and spiritual distress
2. Patient‐family‐professional communication about achievable goals for care and the decision‐making that follows
3. Coordinated, communicated, continuity3. Coordinated, communicated, continuity of care and support for social and practical needs of both patients and families across settings
Palliative care is specialized medical care for people with serious illnesses. This type of care is focused on providing
Palliative Care Language Endorsed by the Public
patients with relief from the symptoms, pain, and stress of a serious illness ‐ whatever the diagnosis.
The goal is to improve quality of life for both the patient and the family. Palliative care is provided by a team of doctors, nurses, and other specialists who work with a , , ppatient's other doctors to provide an extra layer of support. Palliative care is appropriate at any age and at any stage in a serious illness, and can be provided together with curative treatment.

10
Palliative Care Models Improve Value (Quality/Cost)
Quality improves Costs reducedQuality improves– Symptoms
– Quality of life
– Length of life
– Family satisfaction
– Family bereavement
Costs reduced– Hospital costs
decrease
– Need for hospital, ICU, ED decreased
– 30 day readmissions
outcomes
– MD satisfaction
– Care matched to patient centered goals
decreased
– Hospitality mortality decreased
The Future of Palliative Care
• Not enough to have access to palliative care in hospitalsp p
• Most illness occurs at home and in communities
• Home palliative care needed without regard to prognosis or goals of careregard to prognosis or goals of care
• Goal = insure access to palliative care across all settings and stages of illness

11
Access to Palliative Care Across the Continuum: The Future
Hospital
Consult ServiceConsult Service
Inpatient Unit
Outpatient Specialty Clinics
NH Services
Provider Home Visits
Clinics
Cancer Center
Outpatient PCP
Clinics
21

12
Palliative Care Improves Quality in Office Setting
Randomized trial simultaneous standard cancer care with palliative care co‐management from diagnosis versus control group receiving standard cancer care only:group receiving standard cancer care only:
– Improved quality of life– Reduced major depression– Reduced ‘aggressiveness’ (less chemo < 14d before death, more likely to get hospice, less likely to be hospitalized in last month)to be hospitalized in last month)
– Improved survival (11.6 mos. vs 8.9 mos., p<0.02)
Temel et al. Early palliative care for patients with non-small-cell lung cancer NEJM2010;363:733-42.
Palliative care in addition to usual oncology care allowed lung cancer patients to live almost 3 moslonger than those who got usual oncology care. Temel J, et al. NEJM 2010

13
Palliative Care at Home for the Chronically Ill
Improves Quality, Markedly Reduces CostRCT of Service Use Among Heart Failure, Chronic Obstructive Pulmonary Disease, or Cancer Patients While Enrolled in a Home
Palliative Care Intervention or Receiving Usual Home Care, 1999–2000
13.211.1
9.4
35.0
20
30
40
Usual Medicare home care Palliative care intervention
2.3
9.4
4.65.3
0.92.4
0.90
10
Home healthvisits
Physicianoffice visits
ER visits Hospital days SNF days
KP Study Brumley, R.D. et al. JAGS 2007
Palliative Care in the Nursing Home• Retrospective case control study comparing care
processes in 125 end stage dementia patients receiving palliative care consultations (2007-2009) to 125 historical controls (2006) receiving usual carehistorical controls (2006) receiving usual care
• Single facility (Hebrew Rehabilitation) in Boston• Data source: MDS• Primary outcome: a composite outcome based on
utilization patterns, depression, and pain and other clinical Indicators, and change on this composite score (and the individual outcomes) over a 1-year period.
• Results: Residents receiving palliative care• Results: Residents receiving palliative care consultation had fewer ED visits (p<.001) and less depression (P=.03). Change in the composite score indicated a significant difference over time between the 2 groups (p = .013).
Comart J et al. The Gerontologist 2012; dec 7. doi:10.1093/geront/gns154
14
RCT of Nurse-Led Telephonic Palliative Care Intervention
• N= 322 advanced cancer patients in rural NH+VT
• Improved quality of life and less depression (p=0.02)
• Trend towards reduced symptom intensity (p=0.06)
• No difference in utilization, (but v. low in both groups)
• Median survival: intervention group 14 months, control group 8.5 months, p = 0.14
Bakitas M et al. JAMA 2009;302(7):741-9
US Oncology: Pathways Include Palliative Care
Clinical pathways specify:• Number of regimens
Exact drugs to use• Exact drugs to use • Goals of care discussion early
– The Checklist Approach.– Advance medical directives and health
agent appointment “up front” as standard of care.
– Use of homecare and hospice as standard of care.
(In contrast, NCCN pathways allow 16 individual drugs in multiple combinations. No mention of non-chemo care until the end.)
15
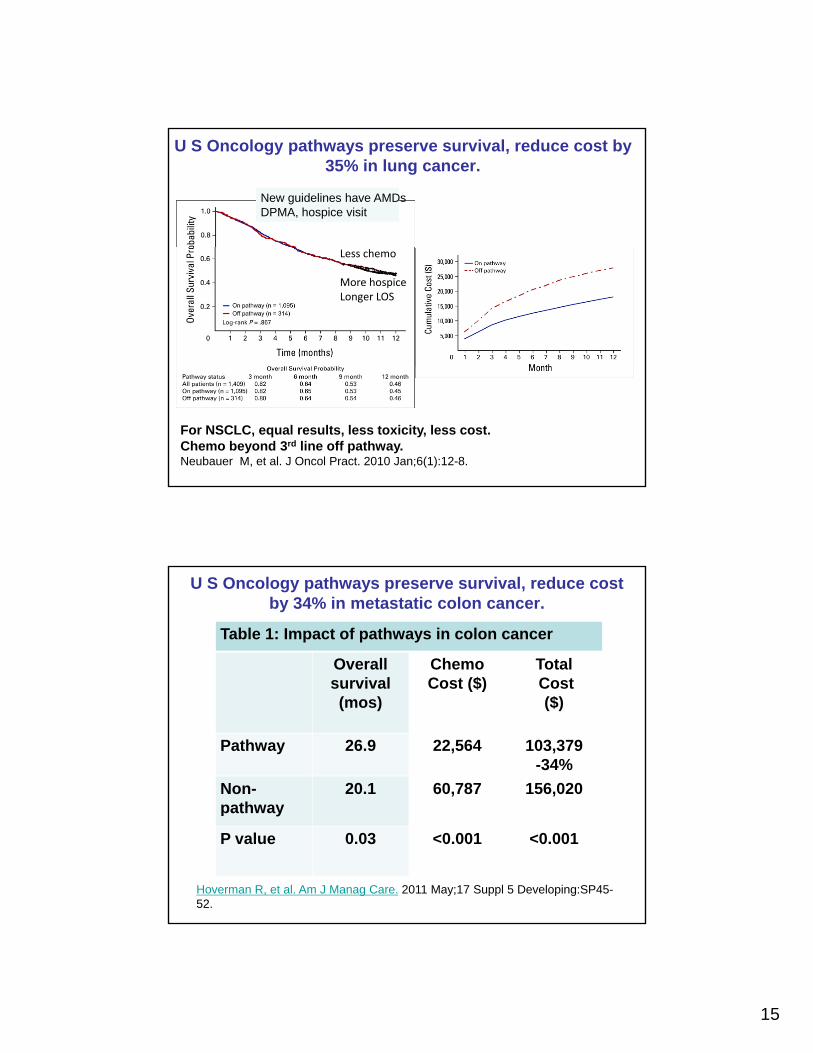
U S Oncology pathways preserve survival, reduce cost by 35% in lung cancer.
New guidelines have AMDsDPMA, hospice visit
Less chemo
More hospiceLonger LOS
For NSCLC, equal results, less toxicity, less cost.Chemo beyond 3rd line off pathway.Neubauer M, et al. J Oncol Pract. 2010 Jan;6(1):12-8.
U S Oncology pathways preserve survival, reduce cost by 34% in metastatic colon cancer.
Table 1: Impact of pathways in colon cancer
Overallsurvival
Chemo Cost ($)
TotalCostsurvival
(mos)Cost ($) Cost
($)
Pathway 26.9 22,564 103,379-34%
Non-path a
20.1 60,787 156,020
Hoverman R, et al. Am J Manag Care. 2011 May;17 Suppl 5 Developing:SP45-52.
pathway
P value 0.03 <0.001 <0.001

16
www.theatlantic.com 02.25.13 MA Full Risk PMPM contract with
HealthCare Partners/DaVita 15%+margin. >700K patients“Now instead of 30-40 patients/day, Dr. Dougher sees 6-
8.”
Consequences of Late Referral to Palliative Care
Serious Adverse Outcomes for Bereaved Caregivers:Caregivers:
Compared to care at home with hospice,
• Care in ICU associated with 5X family risk of Post Traumatic Stress Disorder; and
• Care in hospital associated with 8.8X family i k f l d i f di drisk of prolonged grief disorder
Wright A et al. Place of death: Correlation with quality of life of patients with cancer and predictors of bereaved caregivers mental health. JCO 2010; Sept 13 epub ahead of print
17
Effect of Palliative Care on Hospital Costs
18
How Palliative Care Reduces Cost
• Improved resource use
• Reduced bottlenecks in high cost units
• Improved throughput and consistency
The Conceptual Model:
Dedicated medical team =
Focus + Time =Focus + Time =
Decision Making / Clarity / Follow through

19
Key Characteristics of Effective Models 1: Targeting
SR
ES
OU
RC
ES
Demand Management DM/CM CCM-palliative care
NEEDS
Jones et al. JAGS 2004;52
20
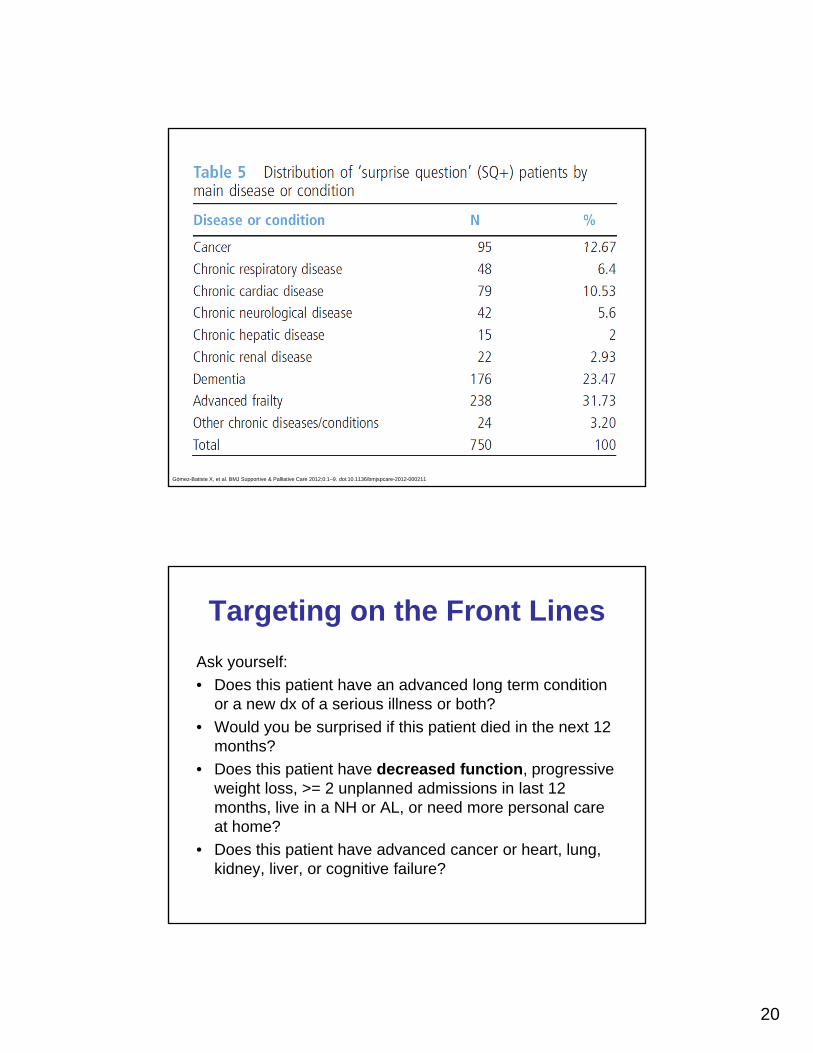
Gómez-Batiste X, et al. BMJ Supportive & Palliative Care 2012;0:1–9. doi:10.1136/bmjspcare-2012-000211
Ask yourself:
• Does this patient have an advanced long term condition
Targeting on the Front Lines
• Does this patient have an advanced long term condition or a new dx of a serious illness or both?
• Would you be surprised if this patient died in the next 12 months?
• Does this patient have decreased function, progressive weight loss, >= 2 unplanned admissions in last 12 months live in a NH or AL or need more personal caremonths, live in a NH or AL, or need more personal care at home?
• Does this patient have advanced cancer or heart, lung, kidney, liver, or cognitive failure?
21
Key Characteristic 2: Goal Setting
• “Don’t ask what’s the matter with me; ask h t tt t !”what matters to me!”
• Ask the person and family, “What is most important to you?”
• “Ultimately, good medicine is about doing right for the patient. For patients with MCC, severe disability, or limited life expectancy, any accounting of how well we’re succeeding in providing care must above all consider patients’ preferred outcomes.”
Reuben and Tinetti NEJM 2012;366:777-9.
Goals for Care
Survey of Senior Center and AL subjects, n=357, dementia excluded, no data on functiondementia excluded, no data on function
Asked to rank order what’s most important:
Overall, independence ranked highest (76% rank it most important) follo ed b pain and s mptom relieffollowed by pain and symptom relief, with staying alive last.
Fried et al. Arch Int Med 2011;171:1854

22
Impact of Goal Setting through Advance Care Planning
• Prospective data on >3000 Medicare beneficiaries p1998-2007 (linked HRS, claims, and NDI)
• Advance directives associated with lower Medicare spending, lower hospital death rate, and higher hospice use in medium-highhospice use in medium high Medicare spending regions of the U.S.
Nicholas et al. JAMA 2011;306:1447-53.
23
Key Characteristic 3: Can We Deliver on People’s Goals? Not When
Families are Home Alone
• 40 billion hours unpaid40 billion hours unpaid care/yr by 42 million caregivers worth $450 billion/yr
• Providing “skilled” care
• Increased morbidity/mortality/banmorbidity/mortality/bankruptcy
aarp.org/ppi
http://www.nextstepincare.org/
Optimistic Baby Boomers say “Get Ready, Kids!”
70% of those who have never received long term care say they can rely on family in time of need as they age, (compared to 55% of those who have received it).
The Scan Foundation/NORC/AP April 2013
To.pbs.org/15TQh2B http://www.apnorc.org/projects/Pages/long‐term‐care‐perceptions‐experiences‐and‐attitudes‐among‐americans‐40‐or‐older.aspx
24
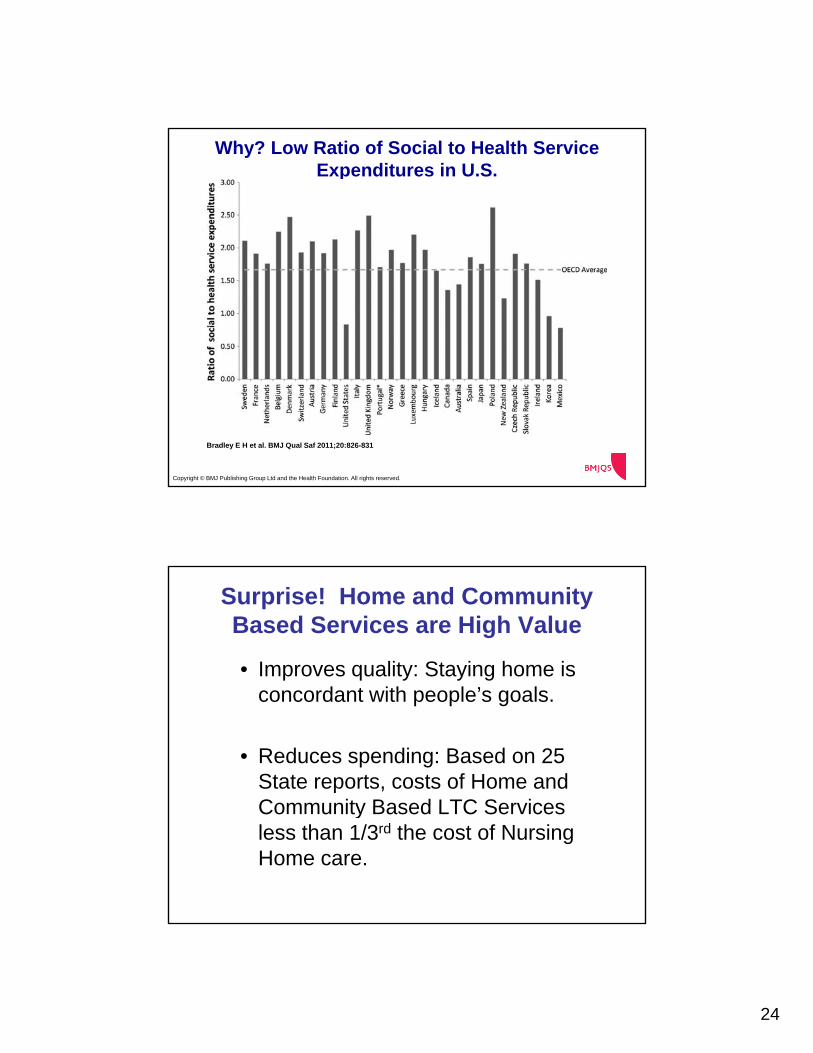
Why? Low Ratio of Social to Health Service Expenditures in U.S.
for Organization for Economic Co-operation and Development (OECD) countries, 2005.
Bradley E H et al. BMJ Qual Saf 2011;20:826-831
Copyright © BMJ Publishing Group Ltd and the Health Foundation. All rights reserved.
Surprise! Home and Community Based Services are High Value
• Improves quality: Staying home is concordant with people’s goals.
• Reduces spending: Based on 25 State reports, costs of Home and Community Based LTC ServicesCommunity Based LTC Services less than 1/3rd the cost of Nursing Home care.
25
Families Need Help if We Are to Honor People’s Goals
• Mobilizing long term services and supports i k t h l i l t h d tis key to helping people stay home and out of hospitals.
• Predictors of success: 24/7 phone access; high-touch consistent and personalized care relationships; focus on social andcare relationships; focus on social and behavioral health determinants; coordinated integration of social supports with medical services.
• This is our job.
Payers Are Already Bringing the Care Home
26
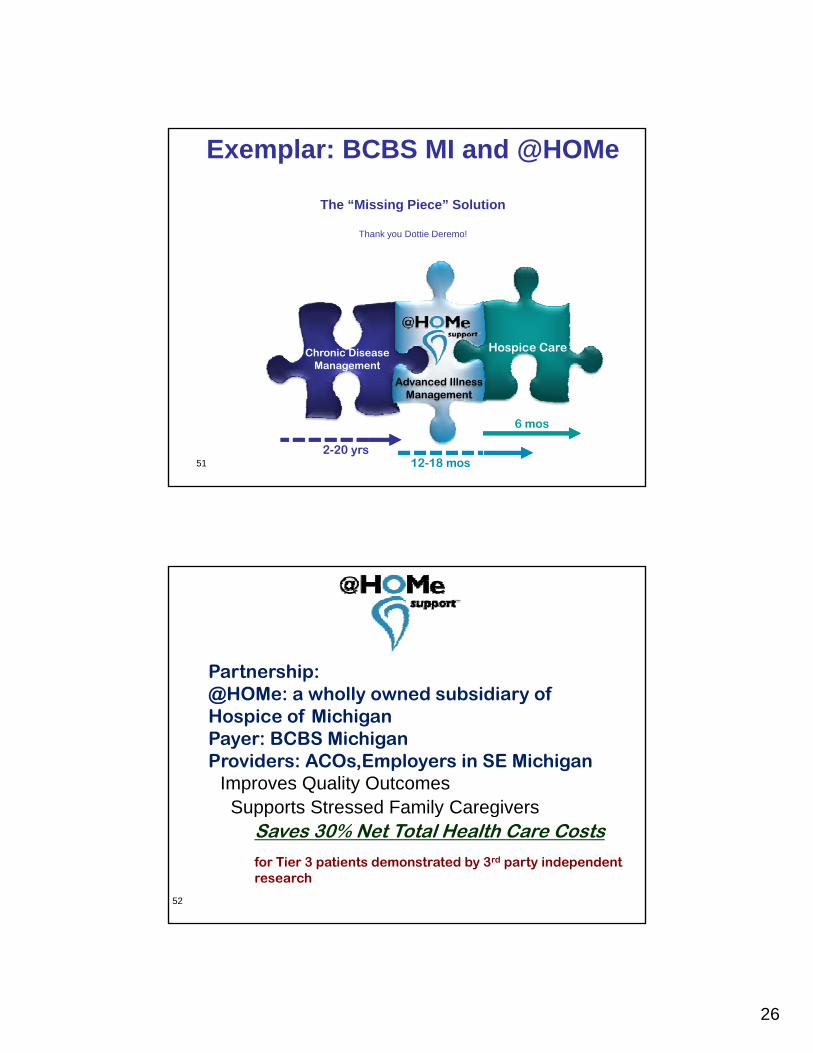
Exemplar: BCBS MI and @HOMe
The “Missing Piece” Solution
Thank you Dottie Deremo!
Chronic Disease Management
Hospice Care
51
Management
2-20 yrs12-18 mos
6 mos
Advanced Illness Management
Partnership:
Improves Quality Outcomes Supports Stressed Family Caregivers
@HOMe: a wholly owned subsidiary of Hospice of Michigan Payer: BCBS MichiganProviders: ACOs,Employers in SE Michigan
52
Supports Stressed Family Caregivers Saves 30% Net Total Health Care Costs
for Tier 3 patients demonstrated by 3rd party independent research
27
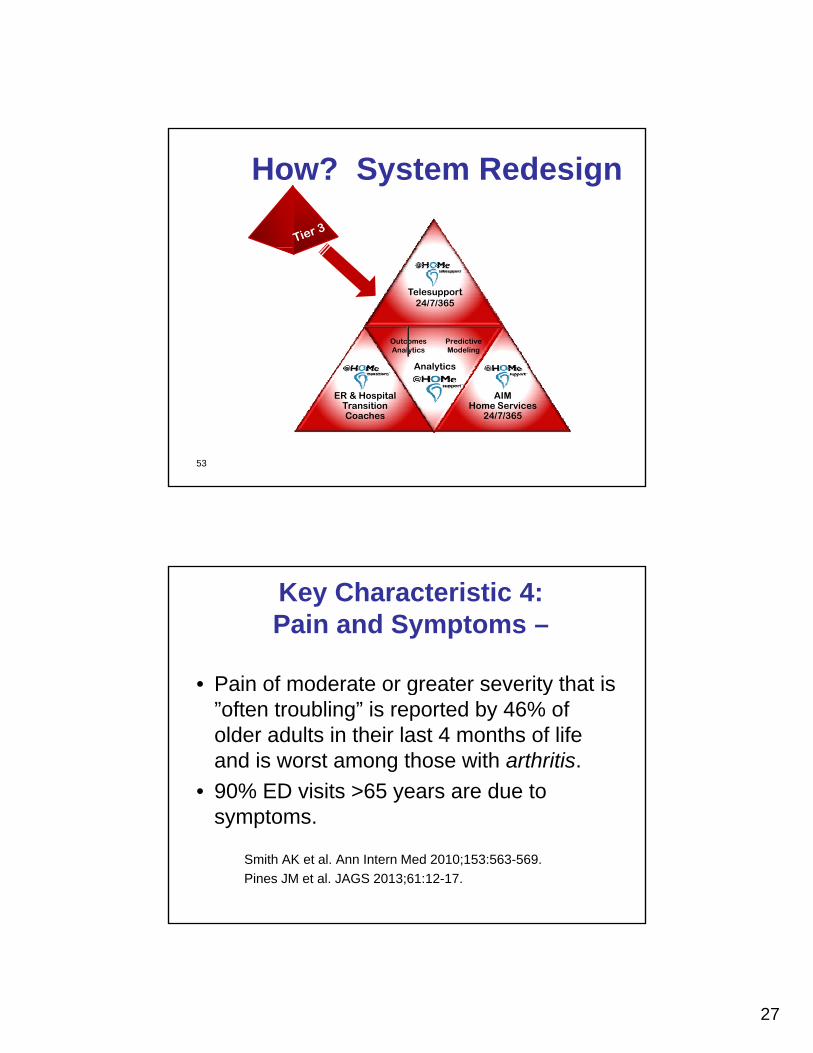
How? System Redesign
Telesupport 24/7/365
Analytics
Predictive Modeling
Outcomes Analytics
53
AIM Home Services
24/7/365
ER & Hospital Transition Coaches
Analytics
Key Characteristic 4: Pain and Symptoms –
• Pain of moderate or greater severity that is• Pain of moderate or greater severity that is ”often troubling” is reported by 46% of older adults in their last 4 months of life and is worst among those with arthritis.
• 90% ED visits >65 years are due to symptoms.
Smith AK et al. Ann Intern Med 2010;153:563-569.
Pines JM et al. JAGS 2013;61:12-17.
28
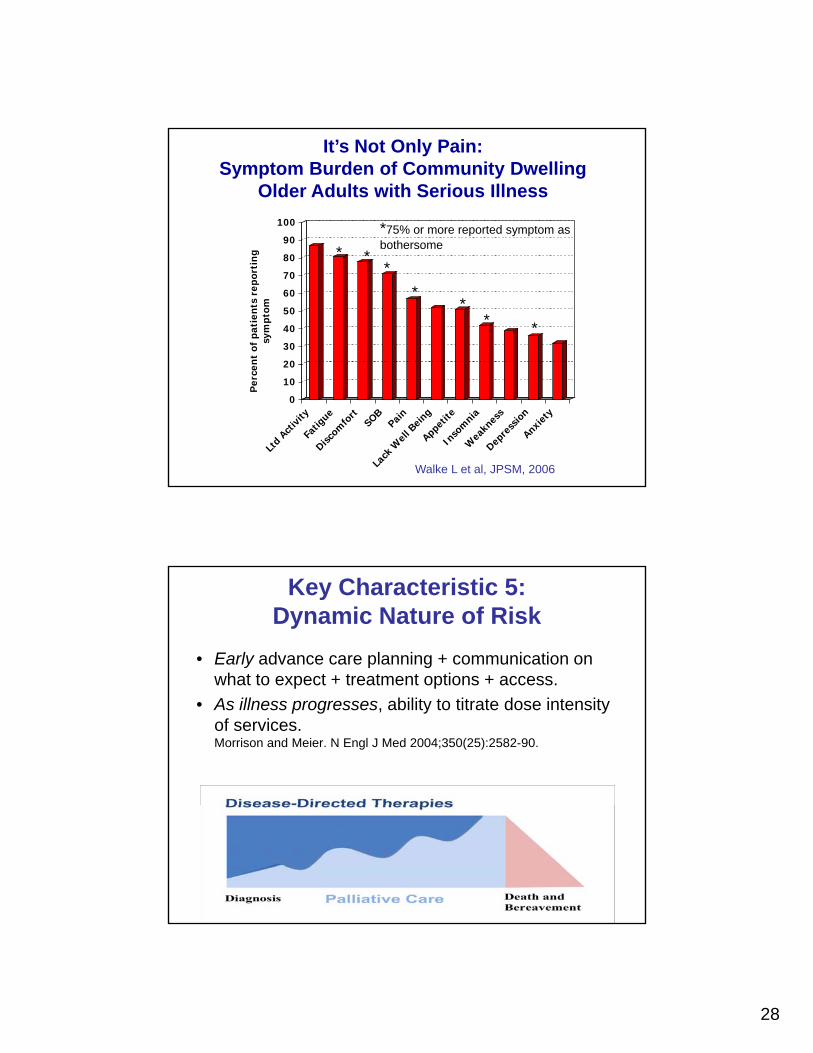
It’s Not Only Pain: Symptom Burden of Community Dwelling
Older Adults with Serious Illness
90
100
*
*75% or more reported symptom as bothersome
20
30
40
50
60
70
80en
t of
pat
ient
s re
port
ing
sym
ptom
* **
**
* *
bothersome
0
10
20
Per
ce
Ltd
Activi
ty
Fatig
ue
Discom
fort
SOBPain
Lack
Wel
l Bein
g
Appetite
Inso
mnia
Wea
knes
s
Depre
ssio
n
Anxiet
y
Walke L et al, JPSM, 2006
Key Characteristic 5: Dynamic Nature of Risk
• Early advance care planning + communication on what to expect + treatment options + access.what to expect treatment options access.
• As illness progresses, ability to titrate dose intensity of services.Morrison and Meier. N Engl J Med 2004;350(25):2582-90.
29
Integrate Palliative Care into New Delivery and Payment Models
Adding palliative care targeted to the highest risk populations to the specifications for ACOs, bundles, PCMHs is key to their
t i i lit dsuccess at improving quality and reducing cost.
Major Health Systems/ACOs Get It
Making multimillion dollar investments in palliative care integration across settings:
•Partners Health System/ Harvard Medical School•Partners Health System/ Harvard Medical School
•U. of Pittsburgh Health System
•Duke U. Health System
•North Shore‐LIJ Health System
•OSF Health System
•Iowa Health System
•Ohio Health System
•Sharp Health System
•Banner Health System…
30
Transforming 21st Century Care of Serious Illness Gomez-Batiste et al.2012
Change from: Change to:
Terminal ……………………………………Advanced Chronic
Prognosis weeks month Prognosis months to yearsPrognosis weeks-month…………………..Prognosis months to years
Cancer ……………………………………..All chronic progressive diseases
Disease……………………………………..Condition (frailty, fn’l dep, MCC)
Mortality…………………………………….Prevalence
Cure vs. Care………………………………Synchronous shared care
Disease OR palliation……………………..Disease AND palliation
Prognosis as criterion……………………..Need as criterionPrognosis as criterion……………………..Need as criterion
Reactive…………………………………….Screening, Preventive
Specialist……………………………………Palliative/Geriatric Care Everywhere
Institutional………………………………….Community
No regional planning……………………….Public health approach
Fragmented care……………………………Integrated care
(Present) and Future
“The future isThe future is here now. It’s just not very evenly distributed.”
William Gibson
The Economist, 2003